Effect of Autologous Serum Eyedrops on Ocular Surface Disease Caused by Preserved Glaucoma Eyedrops


Abstract
:1. Introduction
2. Experimental Section
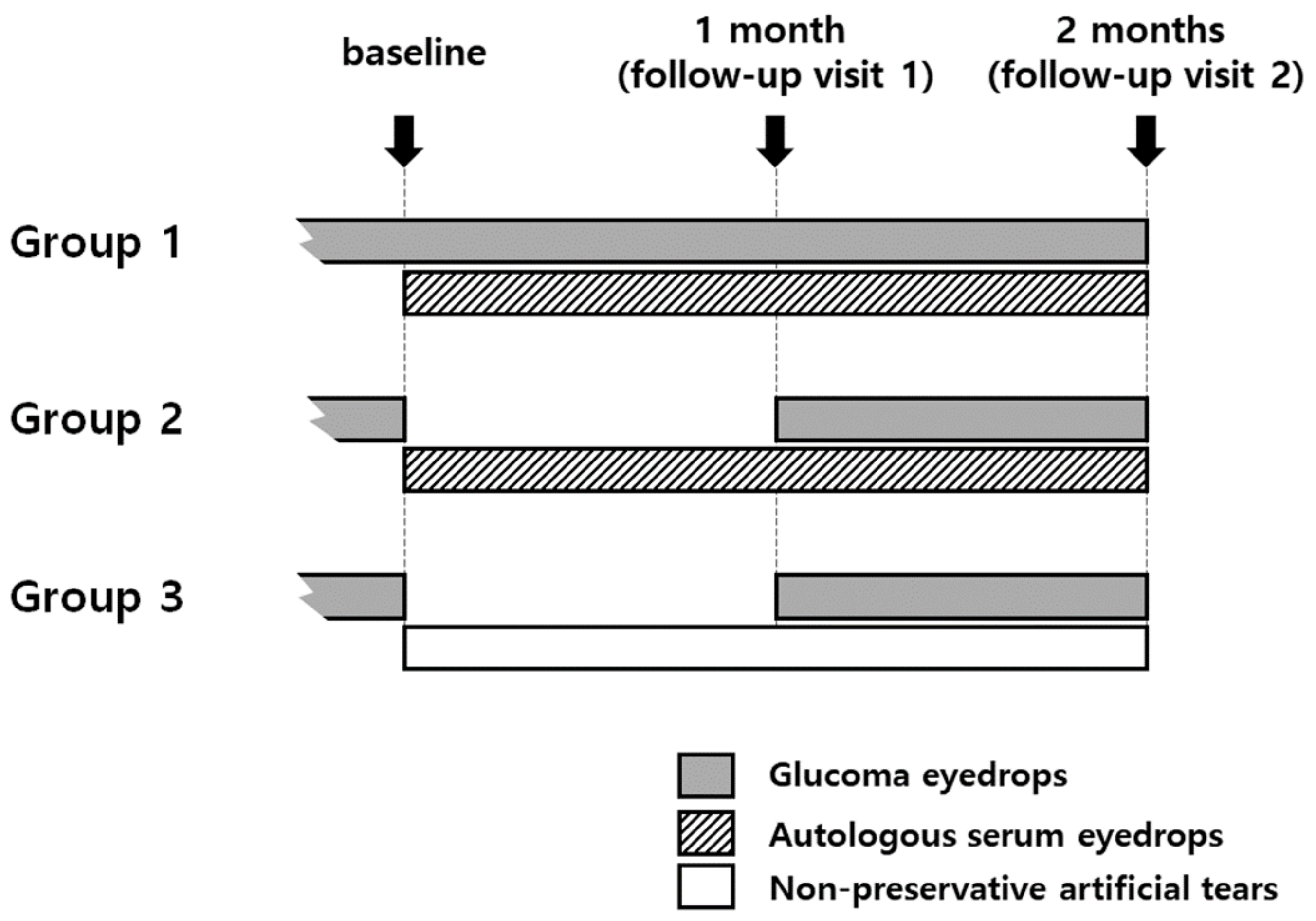
2.1. Patient Groups
2.2. Objective Measures
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Petrillo, F.; Pignataro, D.; Lavano, M.A.; Santella, B.; Folliero, V.; Zannella, C.; Astarita, C.; Gagliano, C.; Franci, G.; Avitabile, T.; et al. Current Evidence on the Ocular Surface Microbiota and Related Diseases. Microorganisms 2020, 8, 1033. [Google Scholar] [CrossRef]
- Anwar, Z.; Wellik, S.R.; Galor, A. Glaucoma therapy and ocular surface disease: Current literature and recommendations. Curr. Opin. Ophthalmol. 2013, 24, 136–143. [Google Scholar] [CrossRef]
- Aguayo Bonniard, A.; Yeung, J.Y.; Chan, C.C.; Birt, C.M. Ocular surface toxicity from glaucoma topical medications and associated preservatives such as benzalkonium chloride (BAK). Expert Opin. Drug Metab. Toxicol. 2016, 12, 1279–1289. [Google Scholar] [CrossRef]
- Pérez-Bartolomé, F.; Martínez-de-la-Casa, J.M.; Arriola-Villalobos, P.; Fernández-Pérez, C.; Polo, V.; García-Feijoó, J. Ocular Surface Disease in Patients under Topical Treatment for Glaucoma. Eur. J. Ophthalmol. 2017, 27, 694–704. [Google Scholar] [CrossRef]
- Asiedu, K.; Abu, S.L. The impact of topical intraocular pressure lowering medications on the ocular surface of glaucoma patients: A review. J. Curr. Ophthalmol. 2019, 31, 8–15. [Google Scholar] [CrossRef]
- Makashova, N.V.; Vasilieva, A.E.; Kolosova, O.Y. Effects of artificial tears on ocular surface in glaucomatous patients with long-term instillation of preserved antiglaucoma eye drops. Vestn. Oftalmol. 2018, 134, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Roberti, G.; Agnifili, L.; Berardo, F.; Riva, I.; Figus, M.; Manni, G.; Quaranta, L.; Oddone, F. Prospective, Randomized, Single Masked, Parallel Study Exploring the Effects of a Preservative-Free Ophthalmic Solution Containing Hyaluronic Acid 0.4% and Taurine 0.5% on the Ocular Surface of Glaucoma Patients Under Multiple Long-Term Topical Hypotensive Therapy. Adv. Ther. 2018, 35, 686–696. [Google Scholar] [PubMed]
- Uusitalo, H.; Egorov, E.; Kaarniranta, K.; Astakhov, Y.; Ropo, A. Benefits of switching from latanoprost to preservative-free tafluprost eye drops: A meta-analysis of two Phase IIIb clinical trials. Clin. Ophthalmol. 2016, 10, 445–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pisella, P.J.; Pouliquen, P.; Baudouin, C. Prevalence of ocular symptoms and signs with preserved and preservative free glaucoma medication. Br. J. Ophthalmol. 2002, 86, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Gazzard, G.; Konstantakopoulou, E.; Garway-Heath, D.; Garg, A.; Vickerstaff, V.; Hunter, R.; Ambler, G.; Bunce, C.; Wormald, R.; Nathwani, N.; et al. Selective laser trabeculoplasty versus drops for newly diagnosed ocular hypertension and glaucoma: The LiGHT RCT. Health Technol. Assess. 2019, 23, 1–102. [Google Scholar] [CrossRef]
- Marchand, M.; Harissi-Dagher, M.; Germain, M.; Thompson, P.; Robert, M.C. Serum drops for ocular surface disease: National survey of Canadian cornea specialists. Can. J. Ophthalmol. 2018, 53, 266–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, C.H.; Lee, H.J.; Park, H.Y.; Kim, H.; Kim, M.K.; Jeoung, J.W.; Oh, J.Y. Effects of topical autologous serum on the ocular surface in patients with toxic corneal epitheliopathy induced by anti-glaucoma drugs. Int. Ophthalmol. 2020, 40, 547–552. [Google Scholar] [CrossRef] [PubMed]
- Higuchi, A. Autologous Serum and Serum Components. Investig. Ophthalmol. Vis. Sci. 2018, 59, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Whitcher, J.P.; Shiboski, C.H.; Shiboski, S.C.; Heidenreich, A.M.; Kitagawa, K.; Zhang, S.; Hamann, S.; Larkin, G.; McNamara, N.A.; Greenspan, J.S.; et al. A simplified quantitative method for assessing keratoconjunctivitis sicca from the Sjögren’s Syndrome International Registry. Am. J. Ophthalmol. 2010, 149, 405–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arita, R.; Itoh, K.; Inoue, K.; Amano, S. Noncontact infrared meibography to document age-related changes of the meibomian glands in a normal population. Ophthalmology 2008, 115, 911–915. [Google Scholar] [CrossRef] [PubMed]
- Bron, A.J.; Benjamin, L.; Snibson, G.R. Meibomian gland disease. Classification and grading of lid changes. Eye 1991, 5, 395–411. [Google Scholar] [CrossRef] [PubMed]
- Rossi, G.C.; Pasinetti, G.M.; Scudeller, L.; Raimondi, M.; Lanteri, S.; Bianchi, P.E. Risk factors to develop ocular surface disease in treated glaucoma or ocular hypertension patients. Eur. J. Ophthalmol. 2013, 23, 296–302. [Google Scholar] [CrossRef]
- Leung, E.W.; Medeiros, F.A.; Weinreb, R.N. Prevalence of ocular surface disease in glaucoma patients. J. Glaucoma 2008, 17, 350–355. [Google Scholar] [CrossRef] [Green Version]
- Steven, D.W.; Alaghband, P.; Lim, K.S. Preservatives in glaucoma medication. Br. J. Ophthalmol. 2018, 102, 1497–1503. [Google Scholar] [CrossRef] [Green Version]
- Ohtani, S.; Shimizu, K.; Nejima, R.; Kagaya, F.; Aihara, M.; Iwasaki, T.; Shoji, N.; Miyata, K. Conjunctival Bacteria Flora of Glaucoma Patients During Long-Term Administration of Prostaglandin Analog Drops. Investig. Ophthalmol. Vis. Sci. 2017, 58, 3991–3996. [Google Scholar] [CrossRef] [Green Version]
- Actis, A.G.; Rolle, T. Ocular surface alterations and topical antiglaucomatous therapy: A review. Open Ophthalmol. J. 2014, 8, 67–72. [Google Scholar] [PubMed] [Green Version]
- Skalicky, S.E.; Goldberg, I.; McCluskey, P. Ocular surface disease and quality of life in patients with glaucoma. Am. J. Ophthalmol. 2012, 153, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Vadoothker, S.; Munir, W.M.; Saeedi, O. Ocular Surface Disease and Glaucoma Medications: A Clinical Approach. Eye Contact Lens 2019, 45, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Giannaccare, G.; Versura, P.; Buzzi, M.; Primavera, L.; Pellegrini, M.; Campos, E.C. Blood derived eye drops for the treatment of cornea and ocular surface diseases. Transfus. Apher. Sci. 2017, 56, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Van der Meer, P.F.; Seghatchian, J.; Marks, D.C. Quality standards, safety and efficacy of blood-derived serum eye drops: A review. Transfus. Apher. Sci. 2016, 54, 164–167. [Google Scholar] [CrossRef]
- Moon, J.; Ko, J.H.; Yoon, C.H.; Kim, M.K.; Oh, J.Y. Effects of 20% Human Serum on Corneal Epithelial Toxicity Induced by Benzalkonium Chloride: In vitro and clinical studies. Cornea 2018, 37, 617–623. [Google Scholar] [CrossRef]
- Mohammed, I.; Kulkarni, B.; Faraj, L.A.; Abbas, A.; Dua, H.S.; King, A.J. Profiling ocular surface responses to preserved and non-preserved topical glaucoma medications: A 2-year randomized evaluation study. Clin. Exp. Ophthalmol. 2020, 48, 973–982. [Google Scholar] [CrossRef]
- Arita, R.; Itoh, K.; Maeda, S.; Maeda, K.; Furuta, A.; Tomidokoro, A.; Aihara, M.; Amano, S. Effects of long-term topical anti-glaucoma medications on meibomian glands. Graefes Arch. Clin. Exp. Ophthalmol. 2012, 250, 1181–1185. [Google Scholar] [CrossRef]
- Kim, J.H.; Shin, Y.U.; Seong, M.; Cho, H.Y.; Kang, M.H. Eyelid Changes Related to Meibomian Gland Dysfunction in Early Middle-Aged Patients Using Topical Glaucoma Medications. Cornea 2018, 37, 421–425. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total | Group 1 | Group 2 | Group 3 | |
|---|---|---|---|---|
| Number of patients | 55 | 18 | 22 | 15 |
| Age (Mean ± SD 1, range) | 64.1 ± 10.9, 36 to 81 | 62.6 ± 10.7, 36 to 79 | 67.5 ± 10.3, 45 to 80 | 59.7 ± 11.8, 40 to 81 |
| Male (%) | 17 (30.9%) | 4 (22.2%) | 6 (27.3%) | 7 (46.7%) |
| Diagnosis | ||||
| POAG 2 | 16 (29.1%) | 5 (27.8%) | 7 (31.8%) | 4 (26.7%) |
| NTG 3 | 28 (50.9%) | 8 (44.4%) | 11 (50.0%) | 9 (60%) |
| NVG 4 | 3 (5.5%) | 1 (5.6%) | 2 (9.1%) | 0 |
| Uveitic glaucoma | 8 (14.5%) | 4 (22.2%) | 2 (9.1%) | 2 (13.3%) |
| Medication history | ||||
| monotherapy | 36 (65.5%) | 12 (66.7%) | 15 (68.2%) | 10 (66.7%) |
| combination | 19 (34.5%) | 6 (33.3%) | 7 (31.8%) | 5 (33.3%) |
| Medication duration | ||||
| <1 year | 11 (20.0%) | 3 (16.7%) | 5 (22.7%) | 9 (60.0%) |
| ≥1 year | 44 (80.0%) | 15 (83.3%) | 17 (77.3%) | 6 (40.0%) |
| Group 1 | Group 2 | Group 3 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD 4 | p-Value 5 | Mean ± SD | p-Value 5 | Mean ± SD | p-Value 5 | |||||||
| Initial | 1 m | 2 m | Initial | 1 m | 2 m | Initial | 1 m | 2 m | ||||
| Schirmer I | 4.2 ± 2.4 | 4.7 ± 3.3 | 5.7 ± 5.2 | 0.9815 | 3.7 ± 1.5 | 4.5 ± 3.0 | 5.4 ± 2.7 | 0.0702 | 4.7 ± 3.9 | 5.5 ± 3.0 | 5.5 ± 2.2 | 0.2510 |
| TBUT 1 | 3.2 ± 1.6 | 3.9 ± 1.9 | 5.6 ± 2.0 * | 0.0020 | 3.4 ± 2.0 | 3.6 ± 1.7 | 4.1 ± 1.7 * | 0.0195 | 2.8 ± 2.3 | 4.2 ± 2.7 | 3.1 ± 2.1 | 0.2744 |
| OSS 2 | 5.7 ± 2.5 | 4.2 ± 2.4 | 1.9 ± 1.3 * | <0.0001 | 5.5 ± 2.9 | 2.9 ± 1.2 * | 1.6 ± 1.3 * | <0.0001 | 5.1 ± 2.3 | 3.1 ± 1.8 | 4.5 ± 1.9 | 0.0480 |
| Meiboscore | 1.5 ± 0.9 | 1.5 ± 0.9 | 1.5 ± 0.9 | 1.000 | 1.5 ± 1.0 | 1.4 ± 1.0 | 1.4 ± 1.0 | 0.9774 | 1.3 ± 1.2 | 1. 5 ± 1.1 | 1.4 ± 1.2 | 0.8909 |
| Meibum quality | 1.2 ± 1.0 | 1.1 ± 1.0 | 0.6 ± 0.7 | 0.1098 | 1.3 ± 1.2 | 1.0 ± 0.8 | 0.8 ± 0.7 | 0.4023 | 1.1 ± 1.2 | 0.8 ± 0.9 | 1.1 ± 1.2 | 0.7812 |
| OSDI 3 | 51.9 ± 24.8 | 43.5 ± 19.6 | 30.0 ± 16.4 * | 0.0037 | 52.2 ± 22.5 | 35.3 ± 17.5 * | 28.9 ± 12.7 * | 0.0004 | 45.1 ± 16.4 | 35.8 ± 14.8 | 41.1 ± 16.6 | 0.0736 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
So, H.-R.; Park, H.Y.L.; Chung, S.-H.; Kim, H.-S.; Byun, Y.-S. Effect of Autologous Serum Eyedrops on Ocular Surface Disease Caused by Preserved Glaucoma Eyedrops. J. Clin. Med. 2020, 9, 3904. https://doi.org/10.3390/jcm9123904
So H-R, Park HYL, Chung S-H, Kim H-S, Byun Y-S. Effect of Autologous Serum Eyedrops on Ocular Surface Disease Caused by Preserved Glaucoma Eyedrops. Journal of Clinical Medicine. 2020; 9(12):3904. https://doi.org/10.3390/jcm9123904
Chicago/Turabian StyleSo, Ha-Rim, Hae Young Lopilly Park, So-Hyang Chung, Hyun-Seung Kim, and Yong-Soo Byun. 2020. "Effect of Autologous Serum Eyedrops on Ocular Surface Disease Caused by Preserved Glaucoma Eyedrops" Journal of Clinical Medicine 9, no. 12: 3904. https://doi.org/10.3390/jcm9123904