Association between Extracorporeal Membrane Oxygenation (ECMO) and Mortality in the Patients with Cardiac Arrest: A Nation-Wide Population-Based Study with Propensity Score Matched Analysis


Abstract
:1. Introduction
2. Methods
2.1. Data Source
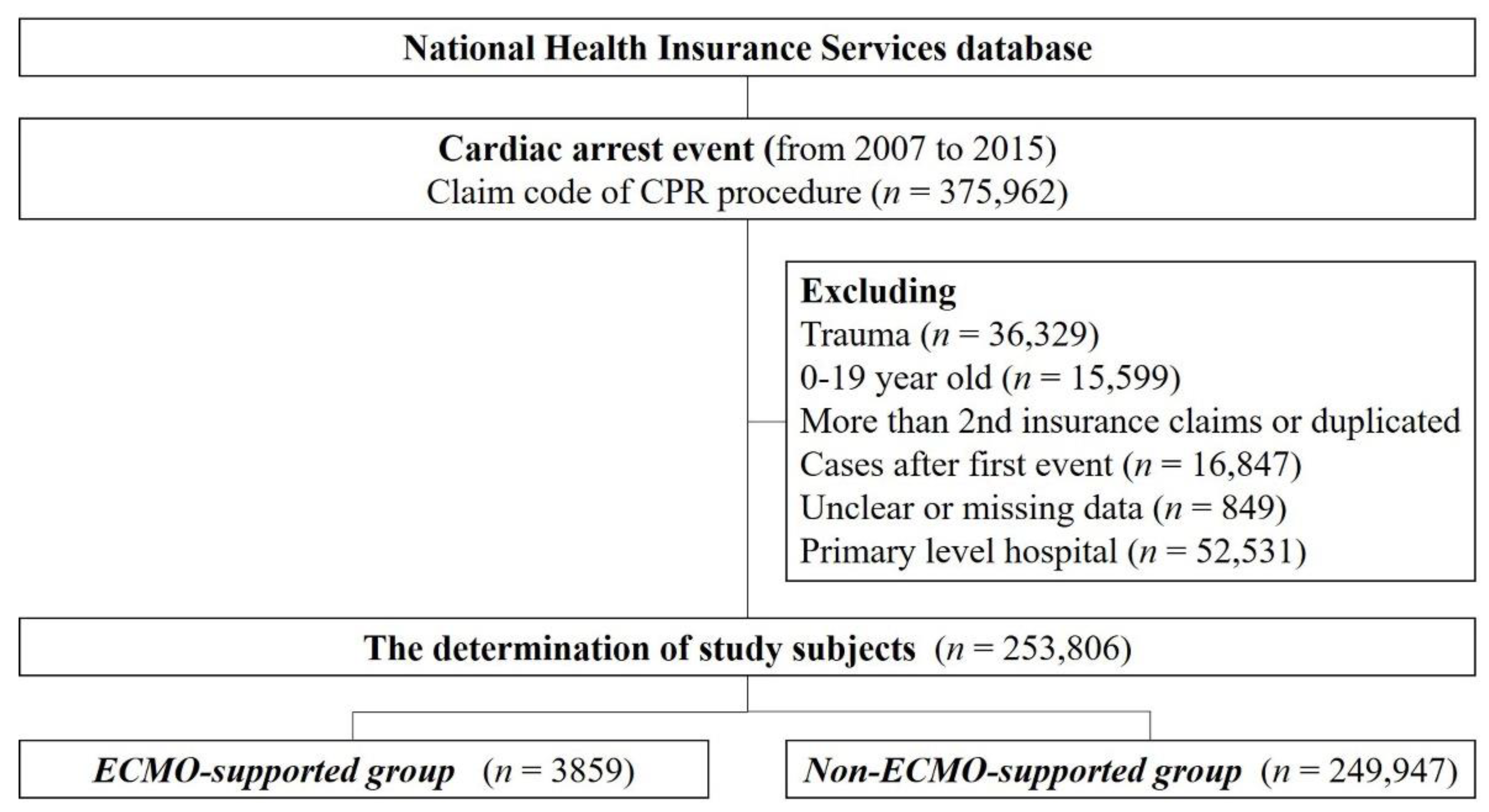
2.2. Study Population
2.3. Definition of Variables
2.4. Study Outcome
2.5. Statistical Analysis
3. Results
3.1. Comparison of Demographic Characteristics, Hospital-Related Factors, and Pre-Existing Diseases, before PS-Matching
3.2. Comparison of Provided Treatments in both Groups after PS-Matching
3.3. Adjusted Odds Ratio of ECMO for 30-Days, 6-Month, and One-Year Mortality
3.4. Comparison of Length of Stay, Hospital Costs, and Disposition after PS Matching
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
Appendix A

{kind=link}
| Before PS Matched Analysis | After PS Matched Analysis | |||||
|---|---|---|---|---|---|---|
| Total | Non-ECMO | ECMO | Total | mNon-ECMO | mECMO | |
| 30-day death | 211,815 (83.5) | 208,932 (83.6) | 2883 (74.7) | 5954 (77.8) | 3081 (80.5) | 2873 (75.1) |
| 6-month death | 228,967 (90.2) | 225,840 (90.4) | 3127 (81.0) | 6471 (84.6) | 3354 (87.7) | 3117 (81.5) |
| 1-year death | 231,356 (91.2) | 228,202 (91.3) | 3154 (81.7) | 6539 (85.5) | 3395 (88.7) | 3144 (82.2) |
Appendix B
| Survivors N = 705 (18.3) | Non-Survivors N = 3154 (81.7) | p-Value | |
|---|---|---|---|
| Age, years | 55.05 ± 14.38 (705) | 60.85 ± 14.83 (3155) | <0.0001 |
| Age group, n (%) | |||
| 20–39 yrs | 107 (15.18) | 325 (10.30) | <0.0001 |
| 40–64 yrs | 394 (55.89) | 1374 (43.58) | |
| 65–74 yrs | 143 (20.28) | 860 (27.26) | |
| 75–84 yrs | 58 (8.23) | 529 (16.77) | |
| 85~yrs | 3 (0.43) | 66 (2.09) | |
| Male | 504 (71.5) | 2120 (67.2) | 0.0271 |
| Insurance type, n (%) | |||
| National Health insurance | 683 (96.9) | 2986 (94.6) | 0.0073 |
| Medical aid | 20 (2.8) | 167 (5.3) | |
| Urbanization level, n (%) | |||
| Urban | 627 (88.9) | 2824 (89.6) | <0.0001 |
| Rural | 57 (8.09) | 321 (10.17) | |
| Level of Hospital, n (%) | |||
| Tertiary | 480 (68.09) | 2090 (66.24) | 0.5822 |
| Secondary | 225 (31.91) | 1064 (33.72) | |
| Volume of hospital (Beds), n (%) | |||
| <300 | 35 (4.96) | 120 (3.84) | 0.0021 |
| 300–499 | 79 (11.21) | 384 (12.17) | |
| 500–799 | 277 (39.29) | 1454 (46.09) | |
| >800 | 314 (44.54) | 1196 (37.91) | |
| Admission route (ER), n (%) | 494 (70.07) | 2283 (72.39) | 0.2146 |
| Charlson comorbidity index <2 | 419 (59.43) | 1528 (48.43) | <0.0001 |
| Preexisting disease, n (%) | |||
| Cancer | 56 (7.94) | 322 (10.21) | 0.0676 |
| Ischemic Stroke | 57 (8.09) | 390 (12.36) | 0.0013 |
| Hemorrhagic Stroke | 7 (0.99) | 39 (1.24) | 0.5905 |
| Myocardial infarction | 41 (5.82) | 218 (6.91) | 0.2939 |
| Angina | 143 (20.28) | 709 (22.47) | 0.2052 |
| Heart failure | 48 (6.81) | 347 (11.00) | 0.0009 |
| Arrhythmia | 54 (7.66) | 293 (9.29) | 0.172 |
| Hypertension | 318 (45.11) | 1689 (53.53) | <0.0001 |
| Hypertension + medication | 276 (39.15) | 1372 (43.49) | 0.0353 |
| Diabetes Mellitus | 189 (26.81) | 1115 (35.34) | <0.0001 |
| Diabetes Mellitus + medication | 128 (18.16) | 736 (23.33) | 0.0029 |
| Lipidemia | 246 (34.89) | 1156 (36.64) | 0.3833 |
| Chronic Pulmonary disease | 130 (18.44) | 676 (21.43) | 0.0778 |
| Chronic Renal Failure | 21 (2.98) | 223 (7.07) | <0.0001 |
| Hemodialysis | 12 (1.70) | 122 (3.87) | 0.0045 |
References
- Mosier, J.M.; Kelsey, M.; Raz, Y.; Gunnerson, K.J.; Meyer, R.; Hypes, C.D.; Malo, J.; Whitmore, S.P.; Spaite, D.W. Extracorporeal membrane oxygenation (ECMO) for critically ill adults in the emergency department: History, current applications, and future directions. Crit. Care 2015, 19, 431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abrams, D.; Garan, A.R.; Abdelbary, A.; Bacchetta, M.; Bartlett, R.H.; Beck, J.; Belohlavek, J.; Chen, Y.S.; Fan, E.; Ferguson, N.D.; et al. Position paper for the organization of ECMO programs for cardiac failure in adults. Intensive Care Med. 2018, 44, 717–729. [Google Scholar] [CrossRef] [PubMed]
- Richardson, A.S.; Schmidt, M.; Bailey, M.; Pellegrino, V.A.; Rycus, P.T.; Pilcher, D.V. ECMO Cardio-Pulmonary Resuscitation (ECPR), trends in survival from an international multicentre cohort study over 12-years. Resuscitation 2017, 112, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Lorusso, R.; Barili, F.; Mauro, M.D.; Gelsomino, S.; Parise, O.; Rycus, P.T.; Maessen, J.; Mueller, T.; Muellenbach, R.; Belohlavek, J.; et al. In-Hospital Neurologic Complications in Adult Patients Undergoing Venoarterial Extracorporeal Membrane Oxygenation: Results From the Extracorporeal Life Support Organization Registry. Crit. Care Med. 2016, 44, e964–e972. [Google Scholar] [CrossRef]
- Karagiannidis, C.; Brodie, D.; Strassmann, S.; Stoelben, E.; Philipp, A.; Bein, T.; Muller, T.; Windisch, W. Extracorporeal membrane oxygenation: Evolving epidemiology and mortality. Intensive Care Med. 2016, 42, 889–896. [Google Scholar] [CrossRef]
- Barbaro, R.P.; Odetola, F.O.; Kidwell, K.M.; Paden, M.L.; Bartlett, R.H.; Davis, M.M.; Annich, G.M. Association of hospital-level volume of extracorporeal membrane oxygenation cases and mortality. Analysis of the extracorporeal life support organization registry. Am. J. Respir. Crit. Care Med. 2015, 191, 894–901. [Google Scholar] [CrossRef] [Green Version]
- Sasson, C.; Rogers, M.A.; Dahl, J.; Kellermann, A.L. Predictors of survival from out-of-hospital cardiac arrest: A systematic review and meta-analysis. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 63–81. [Google Scholar] [CrossRef] [Green Version]
- Goldberger, Z.D.; Chan, P.S.; Berg, R.A.; Kronick, S.L.; Cooke, C.R.; Lu, M.; Banerjee, M.; Hayward, R.A.; Krumholz, H.M.; Nallamothu, B.K. Duration of resuscitation efforts and survival after in-hospital cardiac arrest: An observational study. Lancet 2012, 380, 1473–1481. [Google Scholar] [CrossRef] [Green Version]
- Meaney, P.A.; Nadkarni, V.M.; Kern, K.B.; Indik, J.H.; Halperin, H.R.; Berg, R.A. Rhythms and outcomes of adult in-hospital cardiac arrest. Crit. Care Med. 2010, 38, 101–108. [Google Scholar] [CrossRef]
- Wang, C.H.; Chen, Y.S.; Ma, M.H. Extracorporeal life support. Curr. Opin. Crit. Care 2013, 19, 202–207. [Google Scholar] [CrossRef]
- Ortega-Deballon, I.; Hornby, L.; Shemie, S.D.; Bhanji, F.; Guadagno, E. Extracorporeal resuscitation for refractory out-of-hospital cardiac arrest in adults: A systematic review of international practices and outcomes. Resuscitation 2016, 101, 12–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.J.; Jung, J.S.; Park, J.H.; Park, J.S.; Hong, Y.S.; Lee, S.W. An optimal transition time to extracorporeal cardiopulmonary resuscitation for predicting good neurological outcome in patients with out-of-hospital cardiac arrest: A propensity-matched study. Crit. Care 2014, 18, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Arrigo, S.; Cacciola, S.; Dennis, M.; Jung, C.; Kagawa, E.; Antonelli, M.; Sandroni, C. Predictors of favourable outcome after in-hospital cardiac arrest treated with extracorporeal cardiopulmonary resuscitation: A systematic review and meta-analysis. Resuscitation 2017, 121, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Bednarczyk, J.M.; White, C.W.; Ducas, R.A.; Golian, M.; Nepomuceno, R.; Hiebert, B.; Manji, R.A.; Singal, R.K.; Hussain, F.; Freed, D.H. Resuscitative extracorporeal membrane oxygenation for in hospital cardiac arrest: A Canadian observational experience. Resuscitation 2014, 85, 1713–1719. [Google Scholar] [CrossRef] [PubMed]
- Cardarelli, M.G.; Young, A.J.; Griffith, B. Use of extracorporeal membrane oxygenation for adults in cardiac arrest (E-CPR): A meta-analysis of observational studies. ASAIO J. 2009, 55, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Ouweneel, D.M.; Schotborgh, J.V.; Limpens, J.; Sjauw, K.D.; Engstrom, A.E.; Lagrand, W.K.; Cherpanath, T.G.V.; Driessen, A.H.G.; de Mol, B.; Henriques, J.P.S. Extracorporeal life support during cardiac arrest and cardiogenic shock: A systematic review and meta-analysis. Intensive Care Med. 2016, 42, 1922–1934. [Google Scholar] [CrossRef] [Green Version]
- Twohig, C.J.; Singer, B.; Grier, G.; Finney, S.J. A systematic literature review and meta-analysis of the effectiveness of extracorporeal-CPR versus conventional-CPR for adult patients in cardiac arrest. J. Intensive Care Soc. 2019, 20, 347–357. [Google Scholar] [CrossRef]
- Kim, S.J.; Kim, H.J.; Lee, H.Y.; Ahn, H.S.; Lee, S.W. Comparing extracorporeal cardiopulmonary resuscitation with conventional cardiopulmonary resuscitation: A meta-analysis. Resuscitation 2016. [Google Scholar] [CrossRef]
- Kehrl, T.; Kaczorowski, D.J. Extracorporeal Life Support for Cardiopulmonary Resuscitation for Adults: Evolving Evidence. Asaio J. 2016, 62, 364–369. [Google Scholar] [CrossRef]
- Lazzeri, C.; Bernardo, P.; Sori, A.; Innocenti, L.; Stefano, P.; Peris, A.; Gensini, G.F.; Valente, S. Venous-arterial extracorporeal membrane oxygenation for refractory cardiac arrest: A clinical challenge. Eur. Heart J. Acute Cardiovasc. Care 2013, 2, 118–126. [Google Scholar] [CrossRef] [Green Version]
- Holmberg, M.J.; Geri, G.; Wiberg, S.; Guerguerian, A.M.; Donnino, M.W.; Nolan, J.P.; Deakin, C.D.; Andersen, L.W. Extracorporeal cardiopulmonary resuscitation for cardiac arrest: A systematic review. Resuscitation 2018, 131, 91–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, K.H.; Nam, C.M.; Lee, E.J.; Choi, Y.; Yoo, K.B.; Lee, S.H.; Park, E.C. Effects of individual and neighborhood socioeconomic status on the risk of all-cause mortality in chronic obstructive pulmonary disease: A nationwide population-based cohort study, 2002–2013. Respir Med. 2016, 114, 9–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Health Insurance System of Korea. National Health Insurance Service; National Health Insurance System of Korea: Seoul, Korea, 2007. [Google Scholar]
- Choi, Y.; Kwon, I.H.; Jeong, J.; Chung, J.; Roh, Y. Incidence of Adult In-Hospital Cardiac Arrest Using National Representative Patient Sample in Korea. Healthc. Inform. Res. 2016, 22, 277–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tay, C.K.; Cho, Y.H.; Park, J.; Yang, J.H.; Chung, C.R.; Sung, K.; Cho, J.; Kang, D.; Park, H.; Suh, G.Y. Extracorporeal membrane oxygenation in Korea-Trends and impact of hospital volume on outcome: Analysis of national insurance data 2009–2014. J. Crit. Care 2019, 49, 1–6. [Google Scholar] [CrossRef]
- Sundararajan, V.; Quan, H.; Halfon, P.; Fushimi, K.; Luthi, J.C.; Burnand, B.; Ghali, W.A. Cross-national comparative performance of three versions of the ICD-10 Charlson index. Med. Care 2007, 45, 1210–1215. [Google Scholar] [CrossRef]
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; Bhutta, Z.A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef] [Green Version]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef] [Green Version]
- Shin, T.G.; Jo, I.J.; Sim, M.S.; Song, Y.B.; Yang, J.H.; Hahn, J.Y.; Choi, S.H.; Gwon, H.C.; Jeon, E.S.; Sung, K.; et al. Two-year survival and neurological outcome of in-hospital cardiac arrest patients rescued by extracorporeal cardiopulmonary resuscitation. Int. J. Cardiol. 2013, 168, 3424–3430. [Google Scholar] [CrossRef]
- Chen, Y.S.; Lin, J.W.; Yu, H.Y.; Ko, W.J.; Jerng, J.S.; Chang, W.T.; Chen, W.J.; Huang, S.C.; Chi, N.H.; Wang, C.H.; et al. Cardiopulmonary resuscitation with assisted extracorporeal life-support versus conventional cardiopulmonary resuscitation in adults with in-hospital cardiac arrest: An observational study and propensity analysis. Lancet 2008, 372, 554–561. [Google Scholar] [CrossRef]
- Wang, C.H.; Chou, N.K.; Becker, L.B.; Lin, J.W.; Yu, H.Y.; Chi, N.H.; Hunag, S.C.; Ko, W.J.; Wang, S.S.; Tseng, L.J.; et al. Improved outcome of extracorporeal cardiopulmonary resuscitation for out-of-hospital cardiac arrest--a comparison with that for extracorporeal rescue for in-hospital cardiac arrest. Resuscitation 2014, 85, 1219–1224. [Google Scholar] [CrossRef]
- Maekawa, K.; Tanno, K.; Hase, M.; Mori, K.; Asai, Y. Extracorporeal cardiopulmonary resuscitation for patients with out-of-hospital cardiac arrest of cardiac origin: A propensity-matched study and predictor analysis. Crit. Care Med. 2013, 41, 1186–1196. [Google Scholar] [CrossRef] [PubMed]
- Blumenstein, J.; Leick, J.; Liebetrau, C.; Kempfert, J.; Gaede, L.; Gross, S.; Krug, M.; Berkowitsch, A.; Nef, H.; Rolf, A.; et al. Extracorporeal life support in cardiovascular patients with observed refractory in-hospital cardiac arrest is associated with favourable short and long-term outcomes: A propensity-matched analysis. Eur. Heart J. Acute Cardiovasc. Care 2015. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.K.; Meng, H.; Qadeer, A.; Parikh, P.B. Impact of Extracorporeal Membrane Oxygenation on Mortality in Adults with Cardiac Arrest. Am. J. Cardiol. 2019, 124, 1857–1861. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.J.; Patel, N.; Bhardwaj, B.; Golwala, H.; Kumar, V.; Atti, V.; Arora, S.; Patel, S.; Patel, N.; Hernandez, G.A.; et al. Trends in utilization of mechanical circulatory support in patients hospitalized after out-of-hospital cardiac arrest. Resuscitation 2018, 127, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Sandroni, C.; Dell’anna, A.M.; Tujjar, O.; Geri, G.; Cariou, A.; Taccone, F.S. Acute kidney injury after cardiac arrest: A systematic review and meta-analysis of clinical studies. Minerva Anestesiol. 2016, 82, 989–999. [Google Scholar]
- Askenazi, D.J.; Selewski, D.T.; Paden, M.L.; Cooper, D.S.; Bridges, B.C.; Zappitelli, M.; Fleming, G.M. Renal replacement therapy in critically ill patients receiving extracorporeal membrane oxygenation. Clin. J. Am. Soc. Nephrol. 2012, 7, 1328–1336. [Google Scholar] [CrossRef] [Green Version]
- Cheng, R.; Hachamovitch, R.; Kittleson, M.; Patel, J.; Arabia, F.; Moriguchi, J.; Esmailian, F.; Azarbal, B. Complications of extracorporeal membrane oxygenation for treatment of cardiogenic shock and cardiac arrest: A meta-analysis of 1,866 adult patients. Ann. Thorac. Surg. 2014, 97, 610–616. [Google Scholar] [CrossRef]
- Clarke, S.O.; Schellenbaum, G.D.; Rea, T.D. Socioeconomic status and survival from out-of-hospital cardiac arrest. Acad. Emerg. Med. Off. J. Soc. Acad. Emerg. Med. 2005, 12, 941–947. [Google Scholar] [CrossRef]
- Uray, T.; Mayr, F.B.; Fitzgibbon, J.; Rittenberger, J.C.; Callaway, C.W.; Drabek, T.; Fabio, A.; Angus, D.C.; Kochanek, P.M.; Dezfulian, C. Socioeconomic factors associated with outcome after cardiac arrest in patients under the age of 65. Resuscitation 2015, 93, 14–19. [Google Scholar] [CrossRef] [Green Version]
- Brooks, S.C.; Anderson, M.L.; Bruder, E.; Daya, M.R.; Gaffney, A.; Otto, C.W.; Singer, A.J.; Thiagarajan, R.R.; Travers, A.H. Part 6: Alternative Techniques and Ancillary Devices for Cardiopulmonary Resuscitation: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015, 132 (Suppl. 2), S436–S443. [Google Scholar] [CrossRef] [Green Version]
- Bharmal, M.I.; Venturini, J.M.; Chua, R.F.M.; Sharp, W.W.; Beiser, D.G.; Tabit, C.E.; Hirai, T.; Rosenberg, J.R.; Friant, J.; Blair, J.E.A.; et al. Cost-utility of extracorporeal cardiopulmonary resuscitation in patients with cardiac arrest. Resuscitation 2019, 136, 126–130. [Google Scholar] [CrossRef] [PubMed]
- Gravesteijn, B.Y.; Schluep, M.; Voormolen, D.C.; van der Burgh, A.C.; Dos Reis Miranda, D.; Hoeks, S.E.; Endeman, H. Cost-effectiveness of extracorporeal cardiopulmonary resuscitation after in-hospital cardiac arrest: A Markov decision model. Resuscitation 2019, 143, 150–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dennis, M.; Zmudzki, F.; Burns, B.; Scott, S.; Gattas, D.; Reynolds, C.; Buscher, H.; Forrest, P. Cost effectiveness and quality of life analysis of extracorporeal cardiopulmonary resuscitation (ECPR) for refractory cardiac arrest. Resuscitation 2019, 139, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, T.; Uehara, H.; Miyagi, N.; Shimajiri, M.; Nakamura, K.; Chinen, T.; Hatano, S.; Nago, C.; Chiba, S.; Nakane, H.; et al. Impact of first documented rhythm on cost-effectiveness of extracorporeal cardiopulmonary resuscitation. Resuscitation 2019, 140, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Sanaiha, Y.; Bailey, K.; Downey, P.; Seo, Y.J.; Aguayo, E.; Dobaria, V.; Shemin, R.J.; Benharash, P. Trends in mortality and resource utilization for extracorporeal membrane oxygenation in the United States: 2008–2014. Surgery 2019, 165, 381–388. [Google Scholar] [CrossRef]
- Goto, T.; Morita, S.; Kitamura, T.; Natsukawa, T.; Sawano, H.; Hayashi, Y.; Kai, T. Impact of extracorporeal cardiopulmonary resuscitation on outcomes of elderly patients who had out-of-hospital cardiac arrests: A single-centre retrospective analysis. BMJ Open 2018, 8, e019811. [Google Scholar] [CrossRef] [Green Version]
- Tseng, L.J.; Yu, H.Y.; Wang, C.H.; Chi, N.H.; Huang, S.C.; Chou, H.W.; Shih, H.C.; Chou, N.K.; Chen, Y.S. Impact of Age-Adjusted Charlson Comorbidity on Hospital Survival and Short-Term Outcome of Patients with Extracorporeal Cardiopulmonary Resuscitation. J. Clin. Med. 2018, 7, 313. [Google Scholar] [CrossRef] [Green Version]
- Maxwell, B.G.; Powers, A.J.; Sheikh, A.Y.; Lee, P.H.; Lobato, R.L.; Wong, J.K. Resource use trends in extracorporeal membrane oxygenation in adults: An analysis of the Nationwide Inpatient Sample 1998–2009. J. Thorac. Cardiovasc. Surg. 2014, 148, 416–421. [Google Scholar] [CrossRef] [Green Version]

| Before Propensity Score-Matched Analysis | After Propensity Score-Matched Analysis | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Total | Non-ECMO * | ECMO | p-Value | ASD * | Total | Non-ECMO | ECMO | ASD * | |
| Age, years | <0.0001 a | 0.4492 | 0.0077 | ||||||
| Mean ± SD † | 66.4 ± 14.8 | 66.5 ± 14.8 | 59.8 ± 14.9 | 59.7 ± 15.0 | 59.7 ± 15.1 | 59.8 ± 14.9 | |||
| Median (IQR ‡) | 69.0 (56.0–78.0) | 69.0 (56.0–78.0) | 61.0 (50.0–72.0) | 61.0 (50.0–72.0) | 61.0 (49.0–72.0) | 61.0 (50.0–72.0) | |||
| Sex, n (%) | <0.0001 b | 0.1372 | 0.0141 | ||||||
| Female | 97,569 (38.4) | 96,334 (38.5) | 1235 (32.0) | 2421 (31.6) | 1198 (31.3) | 1223 (31.9) | |||
| Male | 156,237 (61.6) | 153,613 (61.5) | 2624 (68.0) | 5231 (68.4) | 2628 (68.7) | 2603 (68.0) | |||
| Insurance type, n (%) | <0.0001 b | 0.3019 | 0.0148 | ||||||
| National health insurance | 219,883 (86.7) | 216,214 (86.5) | 3669 (95.2) | 7290 (95.3) | 3651 (95.4) | 3639 (95.1) | |||
| Medical aid | 33,811 (13.3) | 33,624 (13.5) | 187 (4.9) | 362 (4.7) | 175 (4.6) | 187 (4.9) | |||
| Urbanization level, n (%) | <0.0001 b | 0.0740 | 0.0168 | ||||||
| Urban | 222,381 (87.9) | 218,930 (87.8) | 3451 (90.1) | 6915 (90.4) | 3467 (90.6) | 3448 (90.1) | |||
| Rural | 30,769 (12.2) | 30,391 (12.2) | 378 (9.9) | 737 (9.6) | 359 (9.4) | 378 (9.9) | |||
| Level of Hospital, n (%) | <0.0001 c | 0.5684 | 0.0033 | ||||||
| Tertiary | 100,823 (39.7) | 98,253 (39.3) | 2570 (66.6) | 5098 (66.6) | 2546 (66.5) | 2552 (66.7) | |||
| Secondary | 152,983 (60.3) | 151,694 (60.7) | 1289 (33.4) | 2554 (33.4) | 1280 (33.5) | 1274 (33.3) | |||
| Volume of hospital (Beds), n (%) | <0.0001 c | 0.6228 | 0.0555 | ||||||
| <300 | 46,143 (18.2) | 45,988 (18.4) | 155 (4.0) | 281 (3.7) | 129 (3.4) | 152 (3.9) | |||
| 300–499 | 54,905 (21.6) | 54,442 (21.8) | 463 (12.0) | 902 (11.8) | 443 (11.6) | 459 (12.0) | |||
| 500–799 | 99,652 (39.3) | 97,921 (39.2) | 1731 (44.9) | 3488 (45.6) | 1769 (46.2) | 1719 (44.9) | |||
| >800 | 53,106 (20.9) | 51,596 (20.6) | 1510 (39.1) | 2981 (38.9) | 1485 (38.8) | 1496 (39.1) | |||
| Admission route (ER §), n (%) | 197,414 (77.8) | 194,637 (77.9) | 2777 (71.9) | <0.0001 b | 0.1366 | 5627 (73.5) | 2871 (75.0) | 2756 (72.0) | 0.0682 |
| Total, n (%) | 253,806 (100) | 249,947 (100) | 3859 (100) | 7652 (100) | 3826 (100) | 3826 (100) | |||
| Before Propensity Score Matched Analysis | After Propensity Score Matched Analysis | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| n (%) | Total | Non-ECMO | ECMO | p-Value | ASD * | Total | Non-ECMO | ECMO | ASD * |
| Cancer | 50,084 (19.7) | 49,706 (19.9) | 378 (9.8) | <0.0001 a | 0.2868 | 750 (9.8) | 374 (9.8) | 376 (9.8) | 0.0018 |
| Ischemic Stroke | 46,543 (18.3) | 46,096 (18.4) | 447 (11.6) | <0.0001 a | 0.1929 | 876 (11.5) | 430 (11.2) | 446 (11.7) | 0.0131 |
| Hemorrhagic Stroke | 7904 (3.1) | 7858 (3.1) | 46 (1.2) | <0.0001 a | 0.1343 | 90 (1.2) | 44 (1.2) | 46 (1.2) | 0.0048 |
| Myocardial infarction | 10,420 (4.1) | 10,161 (4.1) | 259 (6.7) | <0.0001 a | 0.1174 | 492 (6.4) | 234 (6.1) | 258 (6.7) | 0.0256 |
| Angina | 40,540 (15.9) | 39,688 (15.9) | 852 (22.1) | <0.0001 a | 0.1586 | 1609 (21.0) | 764 (19.9) | 845 (22.1) | 0.0520 |
| Heart failure | 29,198 (11.5) | 28,803 (11.5) | 395 (10.2) | 0.0127 a | 0.0414 | 695 (9.1) | 304 (7.9) | 391 (10.2) | 0.0792 |
| Arrhythmia | 25,676 (10.1) | 25,329 (10.1) | 347 (8.9) | 0.0192 a | 0.0388 | 626 (8.2) | 283 (7.4) | 343 (8.9) | 0.0572 |
| HTN † + medication | 104,358 (41.1) | 102,711 (41.1) | 1647 (42.7) | 0.0479 a | 0.0322 | 3255 (42.5) | 1617 (42.3) | 1638 (42.8) | 0.0111 |
| DM ‡ + medication | 51,998 (20.5) | 51,134 (20.5) | 864 (22.4) | 0.0036 a | 0.0471 | 1708 (22.3) | 849 (22.2) | 859 (22.5) | 0.0063 |
| Lipidemia | 71,182 (28.1) | 69,781 (27.9) | 1401 (36.3) | <0.0001 a | 0.1803 | 2708 (35.4) | 1316 (34.4) | 1392 (36.4) | 0.0416 |
| Chronic Pulmonary disease | 77,667 (30.6) | 76,861 (30.8) | 806 (20.9) | <0.0001 a | 0.2269 | 1559 (20.4) | 762 (19.9) | 797 (20.8) | 0.0227 |
| Chronic Renal Failure | 24,519 (9.7) | 24,275 (9.7) | 244 (6.3) | <0.0001 a | 0.125 | 458 (5.9) | 215 (5.6) | 243 (6.4) | 0.0309 |
| N (%) | Total | mNon-ECMO | mECMO | p-Value |
|---|---|---|---|---|
| Defibrillation | 3692 (48.3) | 1279 (33.4) | 2413 (63.1) | <0.0001 a |
| Epinephrine | 7411 (96.9) | 3631 (94.9) | 3780 (98.8) | <0.0001 a |
| Mean ± SD | 9.2 ± 21.6 | 5.6 ± 8.1 | 12.6 ± 28.8 | <0.0001 b |
| Median (IQR) | 4.0 (2.0–11.0) | 2.0 (1.0–7.0) | 6.0 (2.0–16.0) | <0.0001 b |
| Amiodarone | 3025 (39.5) | 830 (21.7) | 2195 (57.4) | <0.0001 a |
| Atropine | 5391 (70.5) | 2505 (65.5) | 2886 (75.4) | <0.0001 a |
| Mean ± SD | 3.9 ± 5.6 | 3.6 ± 5.8 4.1 ± 5.4 | 4.1 ± 5.4 | 0.0075 b |
| Median (IQR) | 2.0 (1.0–4.0) | 2.0 (1.0–4.0) | 2.0 (1.0–5.0) | |
| CAG * | 2803 (36.6) | 433 (11.3) | 2370 (61.9) | <0.0001 a |
| PCI † | 1933 (25.3) | 257 (6.7) | 1676 (43.8) | <0.0001 a |
| CABG ‡ | 157 (2.1) | 30 (0.8) | 127 (3.3) | <0.0001 a |
| ICD || | 44 (0.6) | 16 (0.4) | 28 (0.7) | 0.0641 a |
| Pacing | 930 (12.2) | 186 (4.9) | 744 (19.5) | <0.0001 a |
| ETCO2 # | 802 (10.5) | 322 (8.4) | 480 (12.6) | <0.0001 a |
| CRRT ** | 2079 (27.2) | 435 (11.4) | 1644 (42.9) | <0.0001 a |
| Hemodialysis | 269 (3.5) | 103 (2.7) | 166 (4.3) | <0.0001 a |
| Brain CT | 1837 (24.0) | 987 (25.8) | 850 (22.2) | 0.0002 a |
| Brain MRI | 507 (6.6) | 257 (6.7) | 250 (6.5) | 0.7481 a |
| EEG ¶ | 933 (12.2) | 285 (7.5) | 648 (16.9) | <0.0001 a |
| Therapeutic hypothermia | 354 (4.6) | 74 (1.9) | 280 (7.3) | <0.0001 a |
| Crude Analysis | Multivariable Analysis * | Propensity Score Matching | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95%CI) | p-Value | |
| 30-day death | ||||||
| Non-ECMO | ref | <0.0001 | ref | <0.0001 | ref | <0.0001 |
| ECMO | 0.58 (0.54, 0.62) | 0.73 (0.68, 0.79) | 0.76 (0.68, 0.85) | |||
| 6-month death | ||||||
| Non-ECMO | ref | <0.0001 | ref | <0.0001 | ref | <0.0001 |
| ECMO | 0.46 (0.42, 0.49) | 0.661 (0.61, 0.72) | 0.69 (0.61, 0.79) | |||
| One-year death | ||||||
| Non-ECMO | ref | <0.0001 | ref | <0.0001 | ref | <0.0001 |
| ECMO | 0.43 (0.39, 0.46) | 0.63 (0.58, 0.69) | 0.66 (0.58, 0.75) | |||
| Total | mNon-ECMO | mECMO | p-Value | |
|---|---|---|---|---|
| Hospitalization days | <0.0001 a | |||
| Mean ± SD * | 11.1 ± 15.9 | 9.8 ± 15.4 | 12.4 ± 16.4 | |
| Median (IQR †) | 4.0 (1.0–15.0) | 3.0 (1.0–13.0) | 6.0 (2.0–17.0) | |
| ICU ‡ days | 0.0954 a | |||
| Mean ± SD * | 9.2 ± 19.9 | 10.0 ± 29.8 | 8.8 ± 11.2 | |
| Median (IQR †) | 4.0 (2.0–12.0) | 4.0 (2.0–12.0) | 4.0 (2.0–12.0) | |
| Post-hospitalization ICU days | 0.1129 b | |||
| Mean ± SD * | 23.8 ± 47.1 | 27.4 ± 53.3 | 21.4 ± 31.4 | |
| Median (IQR †) | 11.0 (4.0–27.0) | 10.0 (3.0–25.0) | 11.0 (4.0–29.0) | |
| Hospital cost/person | ||||
| Short-term Hospital cost * | <0.0001 a | |||
| Mean ± SD * | $12,017 ± 13,428 | $5016 ± 7031 | $19,018 ± 14,601 | |
| Median (IQR †) | $7877 (2069–17,091) | $2157 (518–6904) | $15,117 (8853–248,757) | |
| Long-term Hospital cost | <0.0001 a | |||
| Mean ± SD * | $26,519 ± 29,592 | $21,252 ± 25,548 | $30,400 ± 31,714 | |
| Median (IQR †) | $17,111 (6285–35,533) | $12,780 (5063–29,686) | $20,324 (8324–42,500) | |
| Post-hospitalization disposition, n (%) | 0.1299 c | |||
| Continuing Admission | 869 (11.4) | 396 (10.4) | 473 (12.4) | |
| Readmission | 57 (0.7) | 25 (0.7) | 32 (0.8) | |
| Outpatient clinic | 965 (12.6) | 501 (13.1) | 464 (12.1) | |
| No follow-up | 5761 (75.3) | 2904 (75.9) | 2857 (74.7) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.J.; Han, K.S.; Lee, E.J.; Lee, S.J.; Lee, J.S.; Lee, S.W. Association between Extracorporeal Membrane Oxygenation (ECMO) and Mortality in the Patients with Cardiac Arrest: A Nation-Wide Population-Based Study with Propensity Score Matched Analysis. J. Clin. Med. 2020, 9, 3703. https://doi.org/10.3390/jcm9113703
Kim SJ, Han KS, Lee EJ, Lee SJ, Lee JS, Lee SW. Association between Extracorporeal Membrane Oxygenation (ECMO) and Mortality in the Patients with Cardiac Arrest: A Nation-Wide Population-Based Study with Propensity Score Matched Analysis. Journal of Clinical Medicine. 2020; 9(11):3703. https://doi.org/10.3390/jcm9113703
Chicago/Turabian StyleKim, Su Jin, Kap Su Han, Eui Jung Lee, Si Jin Lee, Ji Sung Lee, and Sung Woo Lee. 2020. "Association between Extracorporeal Membrane Oxygenation (ECMO) and Mortality in the Patients with Cardiac Arrest: A Nation-Wide Population-Based Study with Propensity Score Matched Analysis" Journal of Clinical Medicine 9, no. 11: 3703. https://doi.org/10.3390/jcm9113703