The Co-Morbidity between Bipolar and Panic Disorder in Fibromyalgia Syndrome

 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Subjects
2.2. Procedure
2.3. Psychiatric Diagnoses
2.3.1. Mood Disorders
2.3.2. Definition of the Bipolar Spectrum Disorders
2.3.3. Definition of Unipolar Spectrum Diagnoses
2.3.4. Panic Disorders
2.4. Temporal Relationship
2.5. Measures of Clinical Severity of Fibromyalgia
2.5.1. Fibromyalgia Impact Questionnaire (FIQ)
2.5.2. The Fibromyalgia Assessment Status (FAS)
2.5.3. Health Assessment Questionnaire (HAQ)
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Sample
3.2. Mood Spectrum Diagnosis
3.3. Panic Spectrum Diagnosis
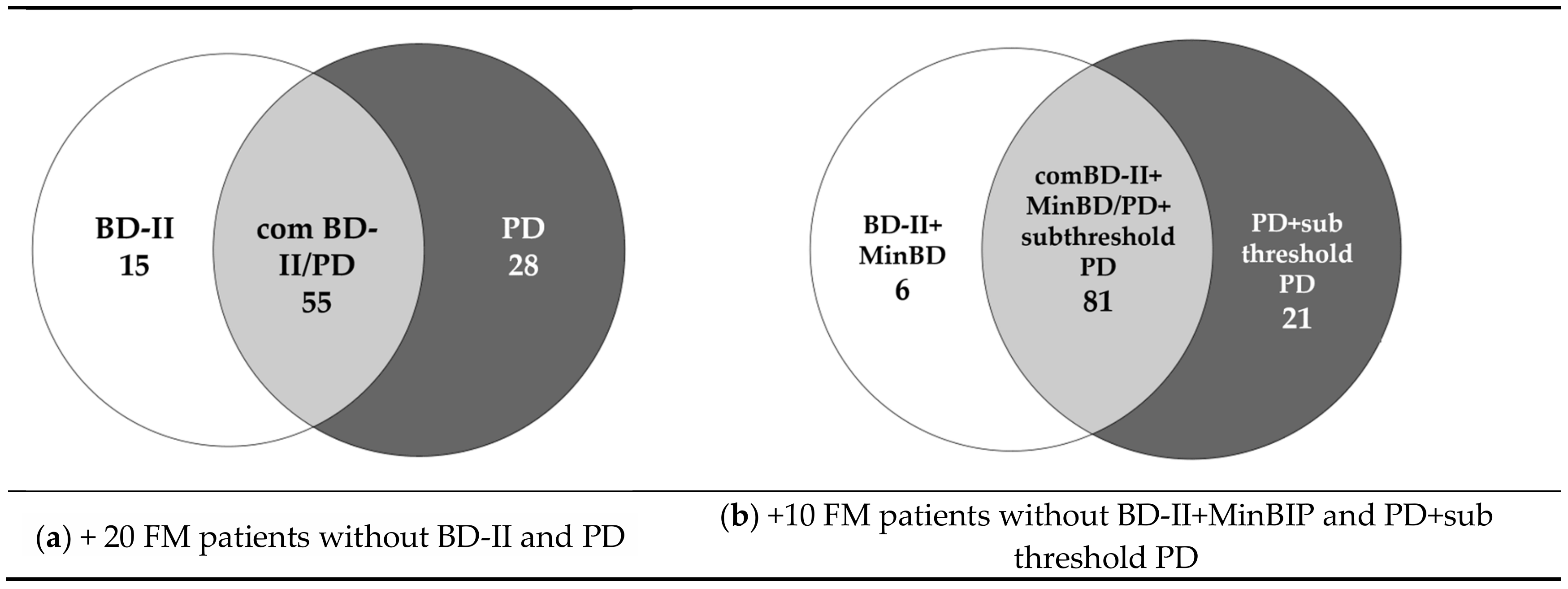
3.4. The Extent of BD/PD Comorbidity
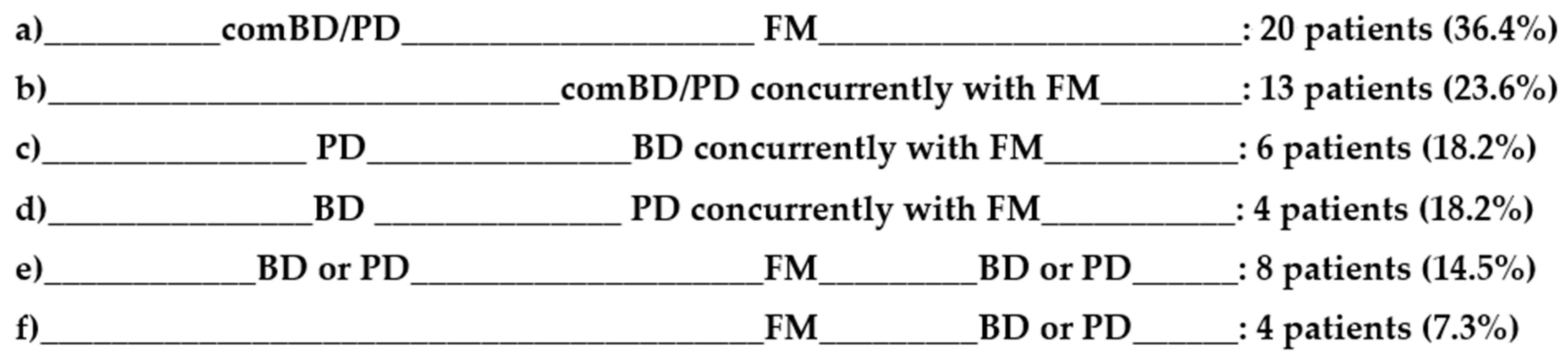
3.5. The Temporal Sequencing of Threshold BD, PD and FM
3.6. Comparison of Clinical Characteristics between the Threshold comBD/PD and no-comBD/PD
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Raphael, K.G.; Janal, M.N.; Nayak, S.; Schwartz, J.E.; Gallagher, R.M. Psychiatric comorbidities in a community sample of women with fibromyalgia. Pain 2006, 12, 117–125. [Google Scholar] [CrossRef]
- Thieme, K.; Turk, D.C.; Flor, H. Comorbid depression and anxiety in fibromyalgia syndrome: Relationship to somatic and psychosocial variables. Psychosom. Med. 2004, 66, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Gracely, R.H.; Ceko, M.; Bushnell, M.C. Fibromyalgia and depression. Pain Res. Treat. 2012, 2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguglia, A.; Salvi, V.; Maina, G.; Rossetto, I.; Aguglia, E. Fibromyalgia syndrome and depressive symptoms: Comorbidity and clinical correlates. J. Affect. Disord. 2011, 128, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Alciati, A.; Sarzi-Puttini, P.; Batticciotto, A.; Torta, R.; Gesuele, F.; Atzeni, F.; Angst, J. Overactive lifestyle in patients with fibromyalgia as a core feature of bipolar spectrum disorder. Clin. Exp. Rheumatol. 2012, 30 (Suppl. S74), 122–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kudlow, P.A.; Rosenblat, J.D.; Weissman, C.R.; Cha, D.S.; Kakar, R.; McIntyre, R.S.; Sharma, V. Prevalence of fibromyalgia and co-morbid bipolar disorder: A systematic review and meta-analysis. J. Affect. Disord. 2015, 188, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Arnold, L.M.; Hudson, J.I.; Hess, E.V.; Ware, A.E.; Fritz, D.A.; Auchenbach, M.B.; Starck, L.O.; Keck, P.E., Jr. Family study of fibromyalgia. Arthritis Rheumatol. 2004, 50, 944–952. [Google Scholar] [CrossRef]
- Carta, M.G.; Cardia, C.; Mannu, F.; Intilla, G.; Hardoy, M.C.; Anedda, C.; Ruggero, V.; Fornasier, D.; Cacace, E. The high frequency of manic symptoms in fibromyalgia does influence the choice of treatment? Clin. Pract. Epidemiol. Ment. Health 2006, 2, 36. [Google Scholar] [CrossRef] [Green Version]
- Arnold, L.M.; Hudson, J.I.; Keck, P.E.; Auchenbach, M.B.; Javaras, K.N.; Hess, E.V. Comorbidity of fibomyalgia and psychiatric disorders. J. Clin. Psychiatry 2006, 67, 1219–1225. [Google Scholar] [CrossRef]
- Arnold, L.M.; Leon, T.; Whalen, E.; Barrett, J. Relationships among pain and depressive and anxiety symptoms in clinical trials of pregabalin in fibromyalgia. Psychosomatics 2010, 51, 489–497. [Google Scholar] [CrossRef]
- Uguz, F.; Çiçek, E.; Salli, A.; Karahan, A.Y.; Albayrak, I.; Kaya, N.; Uğurlu, H. Axis I and Axis II psychiatric disorders in patients with fibromyalgia. Gen. Hosp. Psychiatry 2010, 32, 105–107. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Petukhova, M.; Sampson, N.A.; Zaslavsky, A.M.; Wittchen, H.U. Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. Int. J. Methods Psychiatr. Res. 2012, 21, 169–184. [Google Scholar] [CrossRef] [PubMed]
- Gormsen, L.; Rosenberg, R.; Bach, F.W.; Jensen, T.S. Depression, anxiety, health-related quality of life and pain in patients with chronic fibromyalgia and neuropathic pain. Eur. J. Pain 2010, 14, e1–e127. [Google Scholar] [CrossRef] [PubMed]
- Tander, B.; Cengiz, K.; Alayli, G.; Ilhanli, I.; Canbaz, S.; Canturk, F. A comparative evaluation of health related quality of life and depression in patients with fibromyalgia syndrome and rheumatoid arthritis. Rheumatol. Int. 2008, 28, 859–865. [Google Scholar] [CrossRef] [PubMed]
- Stasi, C.; Nisita, C.; Cortopassi, S.; Corretti, G.; Gambaccini, D.; De Bortoli, N.; Fani, B.; Simonetti, N.; Ricchiuti, A.; Dell’Osso, L.; et al. Subthreshold psychiatric psychopathology in functional gastrointestinal disorders: Can it be the bridge between gastroenterology and psychiatry? Gastroenterol. Res. Pract. 2017, 2017, 1953435. [Google Scholar] [CrossRef] [PubMed]
- Provencher, M.D.; Guimond, A.J.; Hawke, L.D. Comorbid anxiety in bipolar spectrum disorders: A neglected research and treatment issue? J. Affect. Disord. 2012, 137, 161–164. [Google Scholar] [CrossRef] [PubMed]
- Frank, E.; Cyranowski, J.M.; Rucci, P.; Shear, M.K.; Grochocinski, V.J.; Kostelnik, B.; Kupfer, D.J. Clinical significance of lifetime panic spectrum symptoms in the treatment of patients with bipolar I disorder. Arch. Gen. Psychiatry 2016, 59, 905–911. [Google Scholar] [CrossRef]
- Henry, C.; Van Den Bulke, D.; Bellivier, F.; Etain, B.; Rouillon, F.; Leboyer, M. Anxiety disorders in 318 bipolar patients: Prevalence and impact on illness severity and response to mood stabilizer. J. Clin. Psychiatry 2003, 64, 331–335. [Google Scholar] [CrossRef]
- Nabavi, B.; Mitchell, A.J.; Nutt, D.A. Lifetime prevalence of comorbidity between bipolar affective disorder and anxiety disorders: A meta-analysis of 52 interview-based studies of psychiatric population. EBioMedicine 2015, 2, 1405–1419. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.-W.; Dilsaver, S.C. Comorbidity of panic disorder in bipolar illness: Evidence from the epidemiologic catchment area survey. Am. J. psychiatry 1995, 152, 280–282. [Google Scholar]
- Pini, S.; Cassano, G.B.; Simonini, E.; Savino, M.; Russo, A.; Montgomery, S.A. Prevalence of anxiety disorders comorbidity in bipolar depression, unipolar depression and dysthymia. J. Affect. Disord. 1997, 42, 145–153. [Google Scholar] [CrossRef]
- Boylan, K.R.; Bieling, P.J.; Marriott, M.; Begin, H.; Young, L.T.; MacQueen, G.M. Impact of comorbid anxiety disorders on outcome in a cohort of patients with bipolar disorder. J. Clin. Psychiatry 2004, 65, 1106–1113. [Google Scholar] [CrossRef] [PubMed]
- Savino, M.; Perugi, G.; Simonini, E.; Soriani, A.; Cassano, G.B.; Akiskal, H.S. Affective comorbidity in panic disorder: Is there a bipolar connection? J. Affect. Disord. 1993, 28, 155–163. [Google Scholar] [CrossRef]
- Doughty, C.J.; Wells, J.E.; Joyce, P.R.; Olds, R.J.; Walsh, A.E.S. Bipolar-panic disorder comorbidity within bipolar disorder families: A study of siblings. Bipolar Disord. 2004, 6, 245–252. [Google Scholar] [CrossRef]
- Angst, J.; Gamma, A.; Bowden, C.L.; Azorin, J.M.; Perugi, G.; Vieta, E.; Young, A.H. Evidence-based definitions of bipolar-I and bipolar-II disorders among 5,635 patients with major depressive episodes in the Bridge Study: Validity and comorbidity. Eur. Arch. Psychiatry Clin. Neurosci. 2013, 263, 663–673. [Google Scholar] [CrossRef] [Green Version]
- MacKinnon, D.F.; McMahon, F.J.; Simpson, S.G.; McInnis, M.G.; DePaulo, J.R. Panic disorder with familial bipolar disorder. Biol. Psychiatry 1997, 42, 90–95. [Google Scholar] [CrossRef]
- MacKinnon, D.F.; Xu, J.; McMahon, F.J.; Simpson, S.G.; Stine, O.C.; Mclnnis, M.G.; DePaulo, J.R. Bipolar disorder and panic disorder in families: An analysis of chromosome 18 data. Am. J. Psychiatry 1998, 155, 829–831. [Google Scholar]
- McMahon, F.J.; Simpson, S.G.; McInnis, M.G.; Badner, J.A.; MacKinnon, D.F.; DePaulo, R. Linkage of bipolar disorder to chromosome 18q and the validity of bipolar II disorder. Arch. Gen. Psychiatry 2001, 58, 1025–1031. [Google Scholar] [CrossRef] [Green Version]
- Stine, O.C.; Xu, J.; Koskela, R.; McMahon, F.J.; Gschwend, M.; Friddle, C.; Clark, C.D.; McInnis, M.G.; Simpson, S.G.; Breschel, T.S.; et al. Evidence for linkage of bipolar disorder to chromosome 18 with a parent-of-origin effect. Am. J. Hum. Genet. 1995, 57, 1384–1394. [Google Scholar]
- MacKinnon, D.F.; Zandi, P.P.; Cooper, J.; Potash, J.B.; Simpson, S.G.; Gershon, E.; Nurnberger, J.; Reich, T.; DePaulo, J.R. Comorbid bipolar disorder and panic disorder in families with a high prevalence of bipolar disorder. Am. J. Psychiatry 2002, 159, 30–35. [Google Scholar] [CrossRef]
- Batelaan, N.M.; de Graaf, R.; Spijker, J.; Smit, J.H.; van Balkom, A.J.L.M.; Vollebergh, W.A.M.; Beekman, A.T. The course of panic attacks in individuals with panic disorder and subthreshold panic disorder: A population-based study. J. Affect. Disord. 2010, 121, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Pané-Farré, C.A.; Fenske, K.; Stender, J.P.; Meyer, C.; John, U.; Rumpf, H.J.; Hapke, U.; Hamm, A.O. Sub-threshold panic attacks and agoraphobic avoidance increase comorbidity of mental disorders: Results from an adult general population sample. J Anxiety Disord. 2013, 27, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P. The American college of rheumatology 1990 criteria for the classification of fibromyalgia. Report of the multicenter criteria committee. Arthritis Rheumatol. 1990, 33, 160–172. [Google Scholar] [CrossRef] [PubMed]
- First, M.B.; Spitzer, R.L.; Gibbon, M.; Williams, J. Structured Clinical Interview for DSM-IV-TR Axis I Disorders; American Psychiatric Press: Washington, DC, USA, 2001. [Google Scholar]
- Benazzi, F.; Akiskal, H.S. Refining the evaluation of bipolar II: Beyond the strict SCID-CV guidelines for hypomania. J. Affect. Disord. 2003, 73, 33–38. [Google Scholar] [CrossRef]
- Angst, J.; Gamma, A.; Benazzi, F.; Ajdacic, V.; Eich, D.; Rössler, W. Toward a re-definition of subthreshold bipolarity: Epidemiology and proposed criteria for bipolar-II, minor bipolar disorders and hypomania. J. Affect. Disord. 2003, 73, 133–146. [Google Scholar] [CrossRef]
- Judd, L.L.; Akiskal, H.S. The prevalence and disability of bipolar spectrum disorders in the US population: Re-analysis of the ECA database taking into account subthreshold cases. J. Affect. Disord. 2003, 73, 123–131. [Google Scholar] [CrossRef]
- Angst, J.; Adolfsson, R.; Benazzi, F.; Gamma, A.; Hantouche, E.; Meyer, T.D.; Skeppar, P.; Vieta, E.; Scott, J. The HCL-32: Towards a self-assessment tool for hypomanic symptoms in outpatients. J. Affect. Disord. 2005, 88, 217–233. [Google Scholar] [CrossRef]
- Meyer, T.D.; Schrader, J.; Ridley, M.; Lex, C. The Hypomania Checklist (HCL)—Systematic review of its properties to screen for bipolar disorders. Compr. Psychiatry 2014, 55, 1310–1321. [Google Scholar] [CrossRef]
- Burckhardt, C.S.; Clark, S.R.; Bennett, R.M. The fibromyalgia impact questionnaire: Development and validation. J. Rheumatol. 1991, 18, 728–733. [Google Scholar]
- Salaffi, F.; Sarzi-Puttini, P.; Girolimetti, R.; Gasparini, S.; Atzeni, F.; Grassi, W. Development and validation of the self-administered fibromyalgia assessment status: A disease-specific composite measure for evaluating treatment effect. Arthritis Res. Ther. 2009, 11, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Bruce, B.; Fries, J.F. The Stanford health assessment questionnaire: Dimensions and practical applications. Health Qual. Life Outcomes 2003, 1, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, R.C.; Wai, T.C.; Jin, R.; Ruscio, A.M.; Shear, K.; Walters, E.E. The epidemiology of panic attacks, panic disorder, and agoraphobia in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2006, 63, 415–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fasmer, O.B.; Oedegaard, K.J. Clinical characteristics of patients with major affective disorders and comorbid migraine. World J. Biol. Psychiatry 2001, 2, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Rotondo, A.; Mazzanti, C.; Dell’Osso, L.; Rucci, P.; Sullivan, P.; Bouanani, S.; Gonnelli, C.; Goldman, D.; Cassano, G.B. Catechol o-methyltransferase, serotonin transporter, and tryptophan hydroxylase gene polymorphisms in bipolar disorder patients with and without comorbid panic disorder. Am. J. Psychiatry 2002, 159, 23–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campos, S.B.; Miranda, D.M.; Souza, B.R.; Pereira, P.A.; Neves, F.S.; Tramontina, J.; Kapczinski, F.; Romano-Silva, M.A.; Correa, H. Association study of tryptophan hydroxylase 2 gene polymorphisms in bipolar disorder patients with panic disorder comorbidity. Psychiatr. Genet. 2011, 21, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Benson, C.; Mifflin, K.; Kerr, B.; Jesudasan, S.J.B.; Dursun, S.; Baker, G. Biogenic amines and the amino acids GABA and glutamate: Relationships with pain and depression. In Pain in Psychiatric Disorders; S. Karger AG: Basel, Switzerland, 2015; pp. 67–79. [Google Scholar]
- Harvey, M.; Gagné, B.; Labbé, M.; Barden, N. Polymorphisms in the neuronal isoform of tryptophan hydroxylase 2 are associated with bipolar disorder in French Canadian pedigrees. Psychiatr. Genet. 2007, 17, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Herpfer, I.; Lieb, K.P. Substance P receptor antagonists in psychiatry: Rationale for development and therapeutic potential. CNS Drugs 2005, 19, 275–293. [Google Scholar] [CrossRef]
- Perna, G.; Schruers, K.; Alciati, A.; Caldirola, D. Novel investigational therapeutics for panic disorder. Expert Opin. Investig. Drugs. 2015, 24, 491–505. [Google Scholar] [CrossRef]
- Muneer, A. The neurobiology of bipolar disorder: An integrated approach. Chonnam Med. J. 2016, 52, 18. [Google Scholar] [CrossRef]
- Perna, G.; Iannone, G.; Alciati, A.; Caldirola, D. Are anxiety disorders associated with accelerated aging? A focus on neuroprogression. Neural Plast. 2016, 2016. [Google Scholar] [CrossRef] [Green Version]
- Maes, M. Inflammatory and oxidative and nitrosative stress pathways underpinning chronic fatigue, somatization and psychosomatic symptoms. Curr. Opin. Psychiatry 2009, 22, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Bergink, V.; Larsen, J.T.; Hillegers, M.H.J.; Dahl, S.K.; Stevens, H.; Mortensen, P.B.; Petersen, L.; Munk-Olsen, T. Childhood adverse life events and parental psychopathology as risk factors for bipolar disorder. Transl. Psychiatry 2016, 6, e929. [Google Scholar] [CrossRef] [PubMed]
- Dell’Osso, M.C.; Conversano, C.; Lensi, E.; Granchi, F.; Consoli, G.; Faravelli, L.; Rotella, F.; Sarno, N.; Faravelli, C. Agorafobia: Un problema irrisolto. Ital. J. Psychopathol. 2008, 14, 51–57. [Google Scholar]
- Perna, G.; Alciati, A.; Prestia, D.; Torti, T.; Nemeroff, C.B. Is there a link between child abuse and neglect and anxiety disorders? Minerva Psichiatr. 2013, 54, 137–148. [Google Scholar]
- Alciati, A.; Atzeni, F.; Grassi, M.; Caldirola, D.; Riva, A.; Sarzi-Puttini, P.; Perna, G. Childhood adversities in patients with fibromyalgia: Are they related to comorbid lifetime major depression? Clin. Exp. Rheumatol. 2017, 35, 112–118. [Google Scholar]
- Angst, J.; Merikangas, J.A.K.R.; Meter, L.C.A.; Van Rössler, V.A.G.W. Bipolar spectrum in major depressive disorders. Eur. Arch. Psychiatry Clin. Neurosci. 2018, 268, 741–748. [Google Scholar] [CrossRef]
- Merikangas, K.R.; Jin, R.; He, J.; Kessler, R.C.; Lee, S.; Sampson, N.A.; Viana, M.C.; Andrade, L.H.; Hu, C.; Karam, E.G.; et al. Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative. Arch. Gen. Psychiatry 2011, 68, 241–251. [Google Scholar] [CrossRef]
- Nusslock, R.; Frank, E. Subthreshold bipolarity: Diagnostic issues and challenges. Bipolar Disord. 2011, 13, 587–603. [Google Scholar] [CrossRef]
- Piccinni, A.; Bazzichi, L.; Marazziti, D.; Veltri, A.; Bombardieri, S.; Conversano, C.; Ciapparelli, A.; Dell’Osso, L. Subthreshold mood symptoms in patients with fibromyalgia and rheumatoid arthritis. Clin. Exp. Rheumatol. 2011, 29 (Suppl. S69), S55–S59. [Google Scholar]
- Van Houdenhove, B.; Neerinckx, E.; Onghena, P.; Lysens, R.; Vertommen, H. Premorbid “overactive” lifestyle in chronic fatigue syndrome and fibromyalgia: An etiological factor or proof of good citizenship? J. Psychosom. Res. 2001, 51, 571–576. [Google Scholar] [CrossRef]
- Schmechel, D.E.; Edwards, C.L. Fibromyalgia, mood disorders, and intense creative energy: A1AT polymorphisms are not always silent. Neurotoxicology 2012, 33, 1454–1472. [Google Scholar] [CrossRef] [PubMed]
- Skapinakis, P.; Lewis, G.; Davies, S.; Brugha, T.; Prince, M.; Singleton, N. Panic disorder and subthreshold panic in the UK general population: Epidemiology, comorbidity and functional limitation. Eur. Psychiatry 2011, 26, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Kurtze, N.; Gundersen, K.T.; Svebak, S. The role of anxiety and depression in fatigue and patterns of pain among subgroups of fibromyalgia patients. Br. J. Med. Psychol. 1998, 71, 185–194. [Google Scholar] [CrossRef] [PubMed]
- White, K.P.; Nielson, W.R.; Harth, M.; Ostbye, T.; Speechley, M. Chronic widespread musculoskeletal pain with or without fibromyalgia: Psychological distress in a representative community adult sample. J. Rheumatol. 2002, 29, 588–594. [Google Scholar]
- Alok, R.; Das, S.K.; Agarwal, G.G.; Salwahan, L.; Srivastava, R. Relationship of severity of depression, anxiety and stress with severity of fibromyalgia. Clin. Exp. Rheumatol. 2011, 29, S70-2. [Google Scholar]
- Hadlandsmyth, K.; Dailey, D.L.; Rakel, B.A.; Zimmerman, M.B.; Vance, C.G.; Merriwether, E.N.; Chimenti, R.L.; Geasland, K.M.; Crofford, L.J.; Sluka, K.A. Somatic symptom presentations in women with fibromyalgia are differentially associated with elevated depression and anxiety. J. Health Psychol. 2020, 25, 819–829. [Google Scholar] [CrossRef]
- Walker, E.A.; Keegan, D.; Gardner, G.; Sullivan, M.; Katon, W.J.; Bernstein, D. Psychosocial factors in fibromyalgia compared with rheumatoid arthritis: I. Psychiatric diagnoses and functional disability. Psychosom. Med. 1997, 59, 565–571. [Google Scholar] [CrossRef]
- Wilson, H.D.; Robinson, J.P.; Turk, D.C. Toward the identification of symptom patterns in people with fibromyalgia. Arthritis Rheumatol. 2009, 61, 527–534. [Google Scholar] [CrossRef] [Green Version]
- Vincent, A.; Hoskin, T.L.; Whipple, M.O.; Clauw, D.J.; Barton, D.L.; Benzo, R.P.; Williams, D.A. OMERACT-based fibromyalgia symptom subgroups: An exploratory cluster analysis. Arthritis Res. Ther. 2014, 16, 463. [Google Scholar] [CrossRef] [Green Version]
- Salaffi, F.; Mozzani, F.; Draghessi, A.; Atzeni, F.; Catellani, R.; Ciapetti, A.; Di Carlo, M.; Sarzi-Puttini, P. Identifying the symptom and functional domains in patients with fibromyalgia: Results of a cross-sectional Internet-based survey in Italy. J. Pain Res. 2016, 9, 279–286. [Google Scholar] [CrossRef] [Green Version]
- Gorka, S.M.; Huggins, A.A.; Fitzgerald, D.A.; Nelson, B.D.; Phan, K.L.; Shankman, S.A. Neural response to reward anticipation in those with depression with and without panic disorder. J. Affect. Disord. 2014, 164, 50–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lueken, U.; Straube, B.; Yang, Y.; Hahn, T.; Beesdo-Baum, K.; Wittchen, H.U.; Konrad, C.; Ströhle, A.; Wittmann, A.; Gerlach, A.L.; et al. Separating depressive comorbidity from panic disorder: A combined functional magnetic resonance imaging and machine learning approach. J. Affect. Disord. 2015, 184, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Verburg, K.; Klaassen, T.; Pols, H.; Griez, E. Comorbid depressive disorder increases vulnerability to the 35% carbon dioxide (CO2) challenge in panic disorder patients. J. Affect. Disord. 1998, 49, 195–201. [Google Scholar] [CrossRef]
- Kilbane, E.J.; Gokbayrak, N.S.; Galynker, I.; Cohen, L.; Tross, S. A review of panic and suicide in bipolar disorder: Does comorbidity increase risk? J. Affect. Disord. 2009, 115, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lan, C.C.; Tseng, C.H.; Chen, J.H.; Lan, J.L.; Wang, Y.C.; Tsay, G.J.; Hsu, C.Y. Increased risk of a suicide event in patients with primary fibromyalgia and in fibromyalgia patients with concomitant comorbidities. Medicine (Baltimore) 2016, 95, e5187. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.K.Y.; Crane, C. Suicidality in chronic pain: A review of the prevalence, risk factors and psychological links. Psychol. Med. 2006, 36, 575–586. [Google Scholar] [CrossRef] [PubMed]
- Dreyer, L.; Kendall, S.; Danneskiold-Samsøe, B.; Bartels, E.M.; Bliddal, H. Mortality in a cohort of Danish patients with fibromyalgia: Increased frequency of suicide. Arthritis Rheumatol. 2010, 62, 3101–3108. [Google Scholar] [CrossRef]
- Preti, A.; Vrublevska, J.; Veroniki, A.A.; Huedo-Medina, T.B.; Kyriazis, O.; Fountoulakis, K.N. Prevalence and treatment of panic disorder in bipolar disorder: Systematic review and meta-analysis. Evid. Based Ment. Health 2018, 21, 53–60. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Bipolar Spectrum Disorders | Unipolar Spectrum Disorders | No Mood Disorders | χ2 or F | p-Value | ||||
|---|---|---|---|---|---|---|---|---|
| Major Bipolar Spectrum | Minor Bipolar Spectrum | Major Unipolar Spectrum | Minor Unipolar Spectrum | |||||
| BD-I | BD-II | MinBD | MDD | Dysthymia MinD or RBD | ||||
| Patients n (%) | 0 (0) | 70 (59.3) | 17 (14.4) | 0(0) | 0(0) | 31 (26.3) | ||
| Sex-females n (%) | 63 (90) | 15 (88.2) | 29 (93.5) | 0.460 | 0.794 | |||
| Age (years) | 46.5 ± 11.5 | 45.8 ± 12.7 | 43.6 ± 12.9 | 0.614 | 0.543 | |||
| Education (years) | 11.7 ± 2.9 | 11.4 ± 4.3 | 11.4 ± 4 | 0.121 | 0.886 | |||
| Marital Status Single Married Divorced/Widowed | 13 45 12 | 4 11 2 | 7 17 7 | 1.358 | 0.850 | |||
| Occupation Manager White-collar Blue-collar Unemployed | 6 34 20 11 | 3 5 8 1 | 3 13 7 8 | 7.647 | 0.265 | |||
| Age at Onset FM (years) | 35.6 ± 12.2 | 33 ± 16.5 | 34 ± 14 | 0.322 | 0.726 | |||
| Duration FM (months) | 128.1 ± 105 | 162 ± 157.6 | 110.2 ± 109 | 1.068 | 0.347 | |||
| Time to FM diagnosis | 102.2 ± 98.5 | 96.1 ± 122.6 | 72.4 ± 100 | 0.788 | 0.458 | |||
| HCL-32 total sc.(months) | 18.9 ± 4.1 | 16.9 ± 4.9 | 16.8 ± 4.6 | 2.744 | 0.69 | |||
| HCL-32 ≥ 14 Yes No | 57 5 | 13 3 | 20 6 | 3.998 | 0.135 | |||
| BMI | 24 ± 3.7 | 24.9 ± 3.9 | 23.9 ± 4 | 0.347 | 0.308 | |||
| Major Bipolar Spectrum | Minor Bipolar Spectrum | |||
|---|---|---|---|---|
| MDE with Hypomanic Features/BD-II | Minor Bipolar Disorder (MinBD): | |||
| n = 70 | n = 17 | |||
| DSM IV-TR | BD-II n = 34 | BD-NOS n = 36 | BD-NOS n = 10 | Cyclothymic Disorder n = 7 |
| ZurichCriteria | MDE+ Zurich Criteria Hypomanic Syndrome (BD-II) n = 50 | MDE+ Hypomanic Symptoms (BD-II) n = 20 | Minor Bipolar Disorder (MinBD) n = 17 | |
| Threshold PD | Sub-Threshold PD | No Threshold or Subthreshold PD | χ2 or F | p Value | ||
|---|---|---|---|---|---|---|
| PD | Recurrent PAs | Limited Symptoms PAs | ||||
| Patients n (%) | 83 (70.3) | 11 (9.3) | 8 (6.8) | 16 (13.6) | ||
| Sex-females n (%) | 77 (92.7) | 10 (91) | 7 (87.5) | 13 (81.2) | 2.209 | 0.530 |
| Age (years) | 45.7 ± 13 | 42.9 ± 10.1 | 43.2 ± 4.6 | 48.7 ± 10.6 | 0.629 | 0.598 |
| Education (years) | 11.4 ± 3.2 | 12.2 ± 3.8 | 12.4 ± 3 | 11.6 ± 4.2 | 0.318 | 0.812 |
| Marital status Single Married Divorced/Widowed | 15 55 13 | 4 3 4 | 3 4 1 | 2 11 3 | 8.410 | 0.210 |
| Occupation Manager White-collar Blue-collar Unemployed | 10 33 26 14 | 2 3 4 2 | 0 6 2 0 | 0 10 3 3 | 9.81 | 0.366 |
| Age at Onset of FM (years) | 34.2 ± 14.1 | 31.6 ± 8.5 | 34.2 ± 7.6 | 40.1 ± 12.5 | 1.112 | 0.348 |
| Duration of FM (months) | 136.9 ± 121.2 | 132.3 ± 112.6 | 107.2 ± 104.4 | 97.2 ± 78.8 | 0.608 | 0.611 |
| Time to FM diagnosis | 102.1 ± 105.1 | 111 ± 114 | 73.9 ± 102.3 | 50.4 ± 69.4 | 1.212 | 0.309 |
| BMI | 24.4 ± 3.9 | 22.6 ± 3.8 | 23.8 ± 4.1 | 24.2 ± 3.4 | 0.564 | 0.640 |
| COMORBID BD/PD | NoCOMORBID BD/PD | t or χ2 | p-Value | |
|---|---|---|---|---|
| Number of patients n (%) | 55 (46.6%) | 63 (53.4%) | ||
| Sex n (%) Male Female | 5 (9.1) 50 (90.9) | 6 (9.5) 57 (90.5) | 0.007 | 1.00 |
| Age (years) | 47.4 ± 11.9 | 44.2 ± 12.1 | 1.42 | 0.156 |
| Education (years) | 11.7 ± 3.1 | 11.5 ± 3.7 | 0.257 | 0.798 |
| Marital status n (%) Single Married Divorced/widowed | 9 (16.4) 37 (67.2) 9 (16.4) | 15 (23.9) 36 (57.1) 12(19) | 1.406 | 0.495 |
| Occupation n (%) Manager White-collar Blue-collar Unemployed | 8 (14.5) 17 (31) 24 (43.5) 6 (11) | 11(17.5) 18 (28.6) 28 (44.4) 6 (9.5) | 0.269 | 0.966 |
| Age at Onset of FM (years) | 36.7 ± 12.4 | 33.1 ± 13.7 | 1.440 | 0.153 |
| Duration of FM (months) | 124.9 ± 101.3 | 133 ± 125.4 | −0.377 | 0.707 |
| Time to FM diagnosis (months) | 100.82 ± 93.5 | 87.98 ± 110.1 | 0.643 | 0.522 |
| BMI | 24.2 ± 3.6 | 24 ± 4 | 0.231 | 0.818 |
| VAS pain | 8.1 ± 0.9 | 8.2 ± 1.3 | −0.210 | 0.834 |
| FIQ | 78 ± 10.3 | 76 ± 12.7 | 0.849 | 0.398 |
| FAS | 7.6 ± 1.2 | 7.6 ± 1.05 | −0.272 | 0.786 |
| HAQ | 1.1 ± 0.4 | 1.02 ± 0.4 | 0.165 | 0.311 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alciati, A.; Atzeni, F.; Caldirola, D.; Perna, G.; Sarzi-Puttini, P. The Co-Morbidity between Bipolar and Panic Disorder in Fibromyalgia Syndrome. J. Clin. Med. 2020, 9, 3619. https://doi.org/10.3390/jcm9113619
Alciati A, Atzeni F, Caldirola D, Perna G, Sarzi-Puttini P. The Co-Morbidity between Bipolar and Panic Disorder in Fibromyalgia Syndrome. Journal of Clinical Medicine. 2020; 9(11):3619. https://doi.org/10.3390/jcm9113619
Chicago/Turabian StyleAlciati, Alessandra, Fabiola Atzeni, Daniela Caldirola, Giampaolo Perna, and Piercarlo Sarzi-Puttini. 2020. "The Co-Morbidity between Bipolar and Panic Disorder in Fibromyalgia Syndrome" Journal of Clinical Medicine 9, no. 11: 3619. https://doi.org/10.3390/jcm9113619