Uses of Inflammatory Markers for Differentiation of Intrahepatic Mass-Forming Cholangiocarcinoma from Liver Abscess: Case-Control Study


Abstract
:1. Introduction
2. Materials and Methods
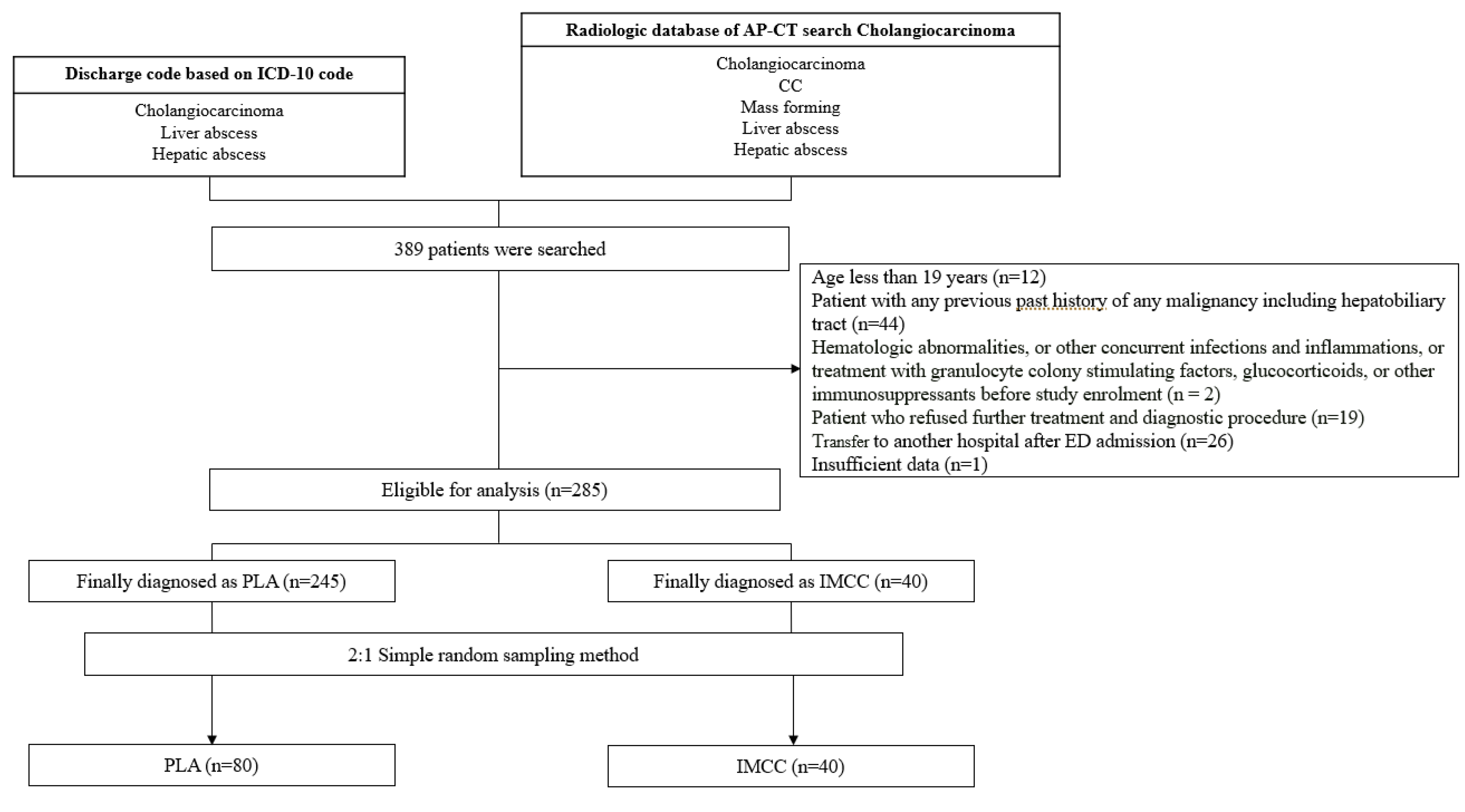
2.1. Study Setting and Population
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. General Characteristics
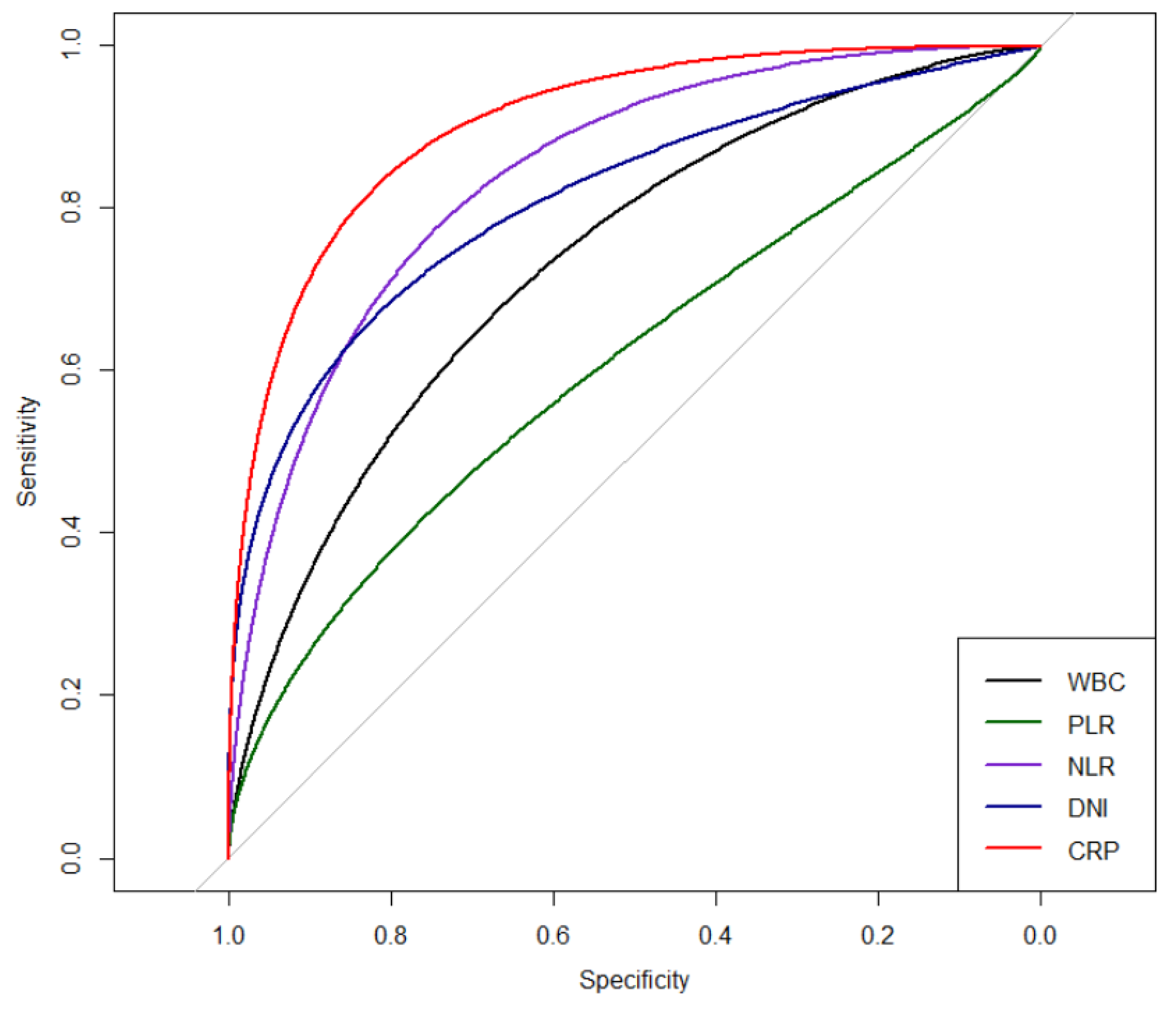
3.2. Comparison of Inflammatory Markers for Differential Prediction between PLA and IMCC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kim, J.E.; Kim, H.O.; Bae, K.; Cho, J.M.; Choi, H.C.; Choi, D.S. Differentiation of small intrahepatic mass-forming cholangiocarcinoma from small liver abscess by dual source dual-energy ct quantitative parameters. Eur. J. Radiol. 2017, 92, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Meddings, L.; Myers, R.P.; Hubbard, J.; Shaheen, A.A.; Laupland, K.B.; Dixon, E.; Coffin, C.; Kaplan, G.G. A population-based study of pyogenic liver abscesses in the united states: Incidence, mortality, and temporal trends. Am. J. Gastroenterol. 2010, 105, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Chen, C.H.; Chiu, K.L.; Lai, H.C.; Liao, K.F.; Ho, Y.J.; Hsu, W.H. Clinical outcome and prognostic factors of patients with pyogenic liver abscess requiring intensive care. Crit. Care Med. 2008, 36, 1184–1188. [Google Scholar] [CrossRef] [PubMed]
- Chia, D.W.J.; Kuan, W.S.; Ho, W.H.; Sim, T.B.; Chua, M.T. Early predictors for the diagnosis of liver abscess in the emergency department. Intern. Emerg. Med. 2019, 14, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Okabayashi, T.; Yamamoto, J.; Kosuge, T.; Shimada, K.; Yamasaki, S.; Takayama, T.; Makuuchi, M. A new staging system for mass-forming intrahepatic cholangiocarcinoma: Analysis of preoperative and postoperative variables. Cancer 2001, 92, 2374–2383. [Google Scholar] [CrossRef]
- Chung, Y.E.; Kim, M.J.; Park, Y.N.; Choi, J.Y.; Pyo, J.Y.; Kim, Y.C.; Cho, H.J.; Kim, K.A.; Choi, S.Y. Varying appearances of cholangiocarcinoma: Radiologic-pathologic correlation. Radiographics 2009, 29, 683–700. [Google Scholar] [CrossRef]
- Bachler, P.; Baladron, M.J.; Menias, C.; Beddings, I.; Loch, R.; Zalaquett, E.; Vargas, M.; Connolly, S.; Bhalla, S.; Huete, A. Multimodality imaging of liver infections: Differential diagnosis and potential pitfalls. Radiographics 2016, 36, 1001–1023. [Google Scholar] [CrossRef]
- Kuo, S.H.; Lee, Y.T.; Li, C.R.; Tseng, C.J.; Chao, W.N.; Wang, P.H.; Wong, R.H.; Chen, C.C.; Chen, S.C.; Lee, M.C. Mortality in emergency department sepsis score as a prognostic indicator in patients with pyogenic liver abscess. Am. J. Emerg. Med. 2013, 31, 916–921. [Google Scholar] [CrossRef]
- Jan, Y.Y.; Yeh, T.S.; Chen, M.F. Cholangiocarcinoma presenting as pyogenic liver abscess: Is its outcome influenced by concomitant hepatolithiasis? Am. J. Gastroenterol. 1998, 93, 253–255. [Google Scholar] [CrossRef]
- Smith, E.H. Complications of percutaneous abdominal fine-needle biopsy. Review. Radiology 1991, 178, 253–258. [Google Scholar] [CrossRef]
- Loew, R.; Dueber, C.; Schwarting, A.; Thelen, M. Subcutaneous implantation metastasis of a cholangiocarcinoma of the bile duct after percutaneous transhepatic biliary drainage (ptbd). Eur. Radiol. 1997, 7, 259–261. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Shen, Y.; Wang, H.; Ge, Q.; Fei, A.; Pan, S. Prognostic significance of neutrophil-to-lymphocyte ratio in patients with sepsis: A prospective observational study. Mediat. Inflamm. 2016, 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, Y.; Huang, X.; Zhang, W. Platelet-to-lymphocyte ratio as a prognostic predictor of mortality for sepsis: Interaction effect with disease severity—A retrospective study. BMJ Open 2019, 9, e022896. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.Y.; Kim, S.J.; Kim, Y.S.; Lee, J.W.; Park, E.J.; Lee, S.J.; Lee, K.J.; Cha, Y.S. Delta neutrophil index as an early predictive marker of severe acute pancreatitis in the emergency department. United Eur. Gastroenterol. J. 2019, 7, 488–495. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.J.; Park, E.J.; Lee, K.J.; Cha, Y.S. The delta neutrophil index is an early predictive marker of severe acute cholecystitis. Dig. Liver Dis. 2019, 51, 1593–1598. [Google Scholar] [CrossRef]
- Nahm, C.H.; Choi, J.W.; Lee, J. Delta neutrophil index in automated immature granulocyte counts for assessing disease severity of patients with sepsis. Ann. Clin. Lab. Sci. 2008, 38, 241–246. [Google Scholar]
- Li, C.; Li, G.; Miao, R.; Lu, X.; Zhong, S.; Sang, X.; Mao, Y.; Zhao, H. Primary liver cancer presenting as pyogenic liver abscess: Characteristics, diagnosis, and management. J. Surg. Oncol. 2012, 105, 687–691. [Google Scholar] [CrossRef]
- Blechacz, B.; Komuta, M.; Roskams, T.; Gores, G.J. Clinical diagnosis and staging of cholangiocarcinoma. Nat. Rev. Gastroenterol. Hepatol. 2011, 8, 512–522. [Google Scholar] [CrossRef] [Green Version]
- Brown, K.M.; Parmar, A.D.; Geller, D.A. Intrahepatic cholangiocarcinoma. Surg. Oncol. Clin. N. Am. 2014, 23, 231–246. [Google Scholar] [CrossRef] [Green Version]
- Thompson, D.; Pepys, M.B.; Wood, S.P. The physiological structure of human c-reactive protein and its complex with phosphocholine. Structure 1999, 7, 169–177. [Google Scholar] [CrossRef]
- Vanderschueren, S.; Deeren, D.; Knockaert, D.C.; Bobbaers, H.; Bossuyt, X.; Peetermans, W. Extremely elevated c-reactive protein. Eur. J. Intern. Med. 2006, 17, 430–433. [Google Scholar] [CrossRef] [PubMed]
- Le Gall, C.; Desideri-Vaillant, C.; Nicolas, X. Significations of extremely elevated c-reactive protein: About 91 cases in a french hospital center. Pathol. Biol. 2011, 59, 319–320. [Google Scholar] [CrossRef] [PubMed]
- Pepys, M.B.; Hirschfield, G.M. C-reactive protein: A critical update. J. Clin. Investig. 2003, 111, 1805–1812. [Google Scholar] [CrossRef] [PubMed]
- Póvoa, P.; Salluh, J.I. Biomarker-guided antibiotic therapy in adult critically ill patients: A critical review. Ann. Intensive Care 2012, 2, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Law, S.T.; Li, K.K. Role of c-reactive protein in response-guided therapy of pyogenic liver abscess. Eur. J. Gastroenterol. Hepatol. 2014, 26, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Gao, H.-N.; Yuan, W.-X.; Yang, M.-F.; Zhao, H.; Hu, J.-H.; Zhang, X.; Fan, J.; Ma, W.-H. Clinical significance of c-reactive protein values in antibiotic treatment for pyogenic liver abscess. World J. Gastroenterol. 2010, 16, 4871–4875. [Google Scholar] [CrossRef]
- Park, K.S.; Lee, S.H.; Yun, S.J.; Ryu, S.; Kim, K. Neutrophil-to-lymphocyte ratio as a feasible prognostic marker for pyogenic liver abscess in the emergency department. Eur. J. Trauma Emerg. Surg. 2019, 45, 343–351. [Google Scholar] [CrossRef]
- Kong, T.; Park, Y.S.; Lee, H.S.; Kim, S.; Lee, J.W.; You, J.S.; Chung, H.S.; Park, I.; Chung, S.P. The delta neutrophil index predicts the development of in-hospital hypotension in initially stable patients with pyogenic liver abscess. Sci. Rep. 2019, 9, 1–10. [Google Scholar] [CrossRef]
- Tan, D.W.; Fu, Y.; Su, Q.; Guan, M.J.; Kong, P.; Wang, S.Q.; Wang, H.L. Prognostic significance of neutrophil to lymphocyte ratio in oncologic outcomes of cholangiocarcinoma: A meta-analysis. Sci. Rep. 2016, 6, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Hu, G.; Liu, Q.; Ma, J.Y.; Liu, C.Y. Prognostic significance of platelet-to-lymphocyte ratio in cholangiocarcinoma: A meta-analysis. Biomed. Res. Int. 2018, 2018. [Google Scholar] [CrossRef] [Green Version]
- Mortelé, K.J.; Segatto, E.; Ros, P.R. The infected liver: Radiologic-pathologic correlation. Radiographics 2004, 24, 937–955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathieu, D.; Vasile, N.; Fagniez, P.L.; Segui, S.; Grably, D.; Lardé, D. Dynamic ct features of hepatic abscesses. Radiology 1985, 154, 749–752. [Google Scholar] [CrossRef] [PubMed]
- Shah, V.; Arora, A.; Tyagi, P.; Sharma, P.; Bansal, N.; Singla, V.; Bansal, R.K.; Gupta, V.; Kumar, A. Intrahepatic cholangiocarcinoma masquerading as liver abscess. J. Clin. Exp. Hepatol. 2015, 5, 89–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variables | Total (n= 120) | Liver Abscess (n = 80, 66.7%) | Cholangiocarcinoma (n = 40, 33.3%) | p Value |
|---|---|---|---|---|
| Male gender (%) | 70 (58.3) | 47 (58.8) | 23 (57.5) | 0.896 |
| Age | 63 (47–82) | 64 (48–82) | 62 (47–82) | 0.285 |
| Past medical history (%) | ||||
| Diabetes mellitus | 30 (25.0) | 18 (22.5) | 12 (30.0) | 0.371 |
| Hypertension | 49 (33.8) | 27 (33.8) | 22 (55.0) | 0.026 |
| Hepatitis | 10 (8.3) | 2 (2.5) | 8 (20.0) | 0.002* |
| Previous liver abscess | 2 (1.7) | 2 (2.5) | 0 (0.0) | 0.552* |
| Smoking (%) | 0.101 | |||
| Current smoker | 23 (19.2) | 11 (13.8) | 12 (30.0) | |
| Ex-smoker | 16 (13.3) | 11 (13.8) | 5 (12.5) | |
| Symptoms (%) | ||||
| Abdominal pain | 52 (43.3) | 35 (43.8) | 17 (42.5) | 0.86 |
| Fever | 71 (59.2) | 66 (82.5) | 5 (12.5) | <0.001 |
| Jaundice | 5 (4.2) | 0 (0.0) | 5 (12.5) | 0.003* |
| Weight loss | 4 (3.3) | 0 (0.0) | 4 (10.0) | 0.011* |
| Body mass index (Kg/m2) | 23.85(16.65–40.41) | 23.88(17.62–31.39) | 23.74(16.65–40.41) | 0.313 |
| Laboratory findings | ||||
| AST (U/L) | 55 (31–110) | 66 (34–113) | 40 (28–96) | 0.060 |
| ALT (U/L) | 45 (25–101) | 54 (36–104) | 29 (18–73) | 0.001 |
| ALP (U/L) | 144 (101–222) | 137 (89–214) | 149 (113–309) | 0.043 |
| γ-GT (U/L) | 118 (60–213) | 100 (56–170) | 136 (71–517) | 0.007 |
| T. bilirubin (mg/dl) | 1.20 (0.24–16.04) | 1.28 (0.29–4.43) | 0.61 (0.24–16.04) | 0.026 |
| CEA (ng/mL) | 2.00 (2.00–510.57) | 2.00 (2.00–14.80) | 2.66 (2.00–510.57) | 0.001 |
| CA 19-9 (U/mL) | 20.40 (9.14–163.85) | 10.70 (7.02–20.50) | 263.60 (40.70–7197.00) | <0.001 |
| AFP (ng/mL) | 2.00 (0.30–744.42) | 1.45 (0.30–5.48) | 3.34 (1.40–744.42) | <0.001 |
| Hemoglobin (g/dL) | 12.45 (4.80–19.30) | 12.35 (4.80–17.10) | 12.75 (8.60–19.30) | 0.140 |
| Platelet (E/L) | 209,500 (10,700–812,000) | 176,000 (10,700–812,000) | 261,000 (101,000–559,000) | 0.001 |
| Inflammatory markers | ||||
| White blood cell (E/L) | 10,620 (750–24,920) | 12,110 (750–24,920) | 7720 (4140–18,080) | <0.001 |
| PLR | 197.55 (6.05–912.50) | 218.13 (6.05–912.50) | 166.53 (71.38–750.00) | 0.016 |
| NLR | 8.31 (0.56–38.98) | 13.02 (0.56–3.98) | 3.20 (1.14–25.97) | <0.001 |
| DNI (%) | 0.65 (0.00–29.10) | 2.00 (0.00–29.10) | 0.00 (0.00–4.00) | <0.001 |
| CRP (mg/dl) | 13.45 (0.12–39.10) | 18.95 (0.29–39.10) | 1.23 (0.12–25.14) | <0.001 |
| Biopsy (%) | 41 (68.3) | 1 (5.0) | 40 (100.0) | <0.001 |
| Treatments (%) | ||||
| Antibiotics | 100 (83.3) | 80 (100.0) | 20(50.0) | <0.001 |
| PAD | 58 (48.3) | 58 (72.5) | 0(0.0) | <0.001 |
| Chemotherapy | 7 (5.8) | 0 (0.0) | 7(17.5) | <0.001* |
| Operation | 17 (14.2) | 3 (3.8) | 14(35.0) | <0.001* |
| In-hospital mortality (%) | 5 (4.2) | 4 (10.0) | 1(1.3) | 0.024* |
| Variables | Total (n = 120) | Liver Abscess (n = 80, 66.7%) | Cholangiocarcinoma (n = 40, 33.3%) | p Value |
|---|---|---|---|---|
| Location | ||||
| Right | 78 (65.0) | 58 (72.5) | 20 (50.0) | 0.015 |
| Left | 32 (26.7) | 16 (20.0) | 16 (40.0) | 0.020 |
| Both | 9 (7.6) | 6 (7.5) | 3 (7.7) | 0.970 |
| Size | 5.40 (1.50–21.00) | 5.30 (1.50–14.30) | 5.60 (2.30–21.00) | 0.181 |
| Number | 1.0 (0.0–6.0) | 1.0 (1.0–6.0) | 1.0 (0.0–5.0) | 0.301 |
| Type | ||||
| Solid | 32 (26.7) | 3 (3.8) | 29 (72.5) | <0.001 |
| Cystic | 71 (59.7) | 71 (88.8) | 0 (0.0) | <0.001 |
| Cyst-solid | 18 (15.1) | 7 (8.8) | 11 (28.2) | 0.005 |
| Stone | ||||
| GB | 11 (9.2) | 8 (10.0) | 3 (7.5) | 0.655 |
| IHD | 6 (5.0) | 5 (6.3) | 1 (2.5) | 0.374 |
| CBD | 6 (5.0) | 6 (7.5) | 0 (0.0) | 0.076 |
| Atrophy | ||||
| Right | 2 (1.7) | 1 (1.3) | 1 (2.5) | 0.614 |
| Left | 11 (9.2) | 5 (6.3) | 6 (15.0) | 0.117 |
| Both | 1 (0.8) | 0 (0.0) | 1 (2.5) | 0.156 |
| Markers | AUC | 95% CI | Sensitivity | Specificity | Cut-Off | p Value |
|---|---|---|---|---|---|---|
| Univariate | ||||||
| White blood cell | 0.755 | 0.660–0.851 | 0.800 | 0.700 | 8800.00 | <0.001 |
| PLR | 0.622 | 0.521–0.723 | 0.588 | 0.700 | 198.600 | <0.001 |
| NLR | 0.863 | 0.789–0.937 | 0.838 | 0.825 | 5.700 | <0.001 |
| DNI | 0.796 | 0.722–0.869 | 0.625 | 0.875 | 1.050 | <0.001 |
| CRP | 0.909 | 0.850–0.969 | 0.900 | 0.900 | 7.080 | <0.001 |
| Pairwise comparison of AUCs | ||||||
| Pairwise comparison of AUCs | difference | p-value* | ||||
| CRP | White blood cell | 0.154 | 0.003 | |||
| PLR | 0.287 | <0.001 | ||||
| NLR | 0.046 | 1.000 | ||||
| DNI | 0.113 | 0.042 | ||||
| Multivariate logistic regression | ||||||
| Markers | Odd ratio | 95% confidence interval | p-value | |||
| White blood cell /per 50 | 0.995 | 0.983–1.006 | 0.358 | |||
| PLR | 0.994 | 0.987–1.002 | 0.134 | |||
| NLR | 1.165 | 0.974–1.395 | 0.096 | |||
| DNI | 1.301 | 0.833–2.029 | 0.248 | |||
| CRP | 1.290 | 1.148–1.449 | <0.001 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.C.; Kim, S.J.; Yu, M.H.; Lee, K.J.; Cha, Y.S. Uses of Inflammatory Markers for Differentiation of Intrahepatic Mass-Forming Cholangiocarcinoma from Liver Abscess: Case-Control Study. J. Clin. Med. 2020, 9, 3194. https://doi.org/10.3390/jcm9103194
Lee SC, Kim SJ, Yu MH, Lee KJ, Cha YS. Uses of Inflammatory Markers for Differentiation of Intrahepatic Mass-Forming Cholangiocarcinoma from Liver Abscess: Case-Control Study. Journal of Clinical Medicine. 2020; 9(10):3194. https://doi.org/10.3390/jcm9103194
Chicago/Turabian StyleLee, Sun Chul, Sun Ju Kim, Min Heui Yu, Kyong Joo Lee, and Yong Sung Cha. 2020. "Uses of Inflammatory Markers for Differentiation of Intrahepatic Mass-Forming Cholangiocarcinoma from Liver Abscess: Case-Control Study" Journal of Clinical Medicine 9, no. 10: 3194. https://doi.org/10.3390/jcm9103194