The Genetics of Pituitary Adenomas



Section on Endocrinology and Genetics, Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), National Institutes of Health, Bethesda, MD 20892, USA
*
Author to whom correspondence should be addressed.
J. Clin. Med. 2020, 9(1), 30; https://doi.org/10.3390/jcm9010030
Submission received: 4 November 2019
/
Revised: 12 December 2019
/
Accepted: 15 December 2019
/
Published: 21 December 2019
(This article belongs to the Special Issue Advances in the Diagnosis and Therapy of Pituitary Disorders)
Abstract
:The genetic landscape of pituitary adenomas (PAs) is diverse and many of the identified cases remain of unclear pathogenetic mechanism. Germline genetic defects account for a small percentage of all patients and may present in the context of relevant family history. Defects in AIP (mutated in Familial Isolated Pituitary Adenoma syndrome or FIPA), MEN1 (coding for menin, mutated in Multiple Endocrine Neoplasia type 1 or MEN 1), PRKAR1A (mutated in Carney complex), GPR101 (involved in X-Linked Acrogigantism or X-LAG), and SDHx (mutated in the so called “3 P association” of PAs with pheochromocytomas and paragangliomas or 3PAs) account for the most common familial syndromes associated with PAs. Tumor genetic defects in USP8, GNAS, USP48 and BRAF are some of the commonly encountered tissue-specific changes and may explain a larger percentage of the developed tumors. Somatic (at the tumor level) genomic changes, copy number variations (CNVs), epigenetic modifications, and differential expression of miRNAs, add to the variable genetic background of PAs.
1. Introduction
Pituitary adenomas (PAs) are common lesions in the adult population presenting in 15–20% of cadavers or radiologic findings and constitute approximately 10% of all intracranial tumors [1,2]. PAs are rarer in the pediatric population identified in 0.2% of children undergoing brain imaging [3]. Although most of the identified PAs are incidental findings without the need for intervention, some may present as clinically significant because they secrete hormones or cause symptoms from compression or invasion of surrounding tissues [4].
The etiology of PAs is diverse, and more than half of them do not have an identified genetic cause. In certain cases, however, germline or somatic genetic defects are associated with the formation of PAs. Additional genetic changes found in PAs, such as copy number variations (CNVs), methylation changes and miRNA abnormalities have also been investigated as being potentially involved in the pathogenesis, presentation and behavior of these tumors, especially with regard to aggressiveness and response to treatment.
This review focuses on the current knowledge of the genetic findings in PAs at the germline (Table 1 and Table 2) and somatic (Table 3) level. Additional information on the genomic profile of PAs can derive from expression studies, methylation analyses and miRNA changes, which are briefly mentioned in the current review.
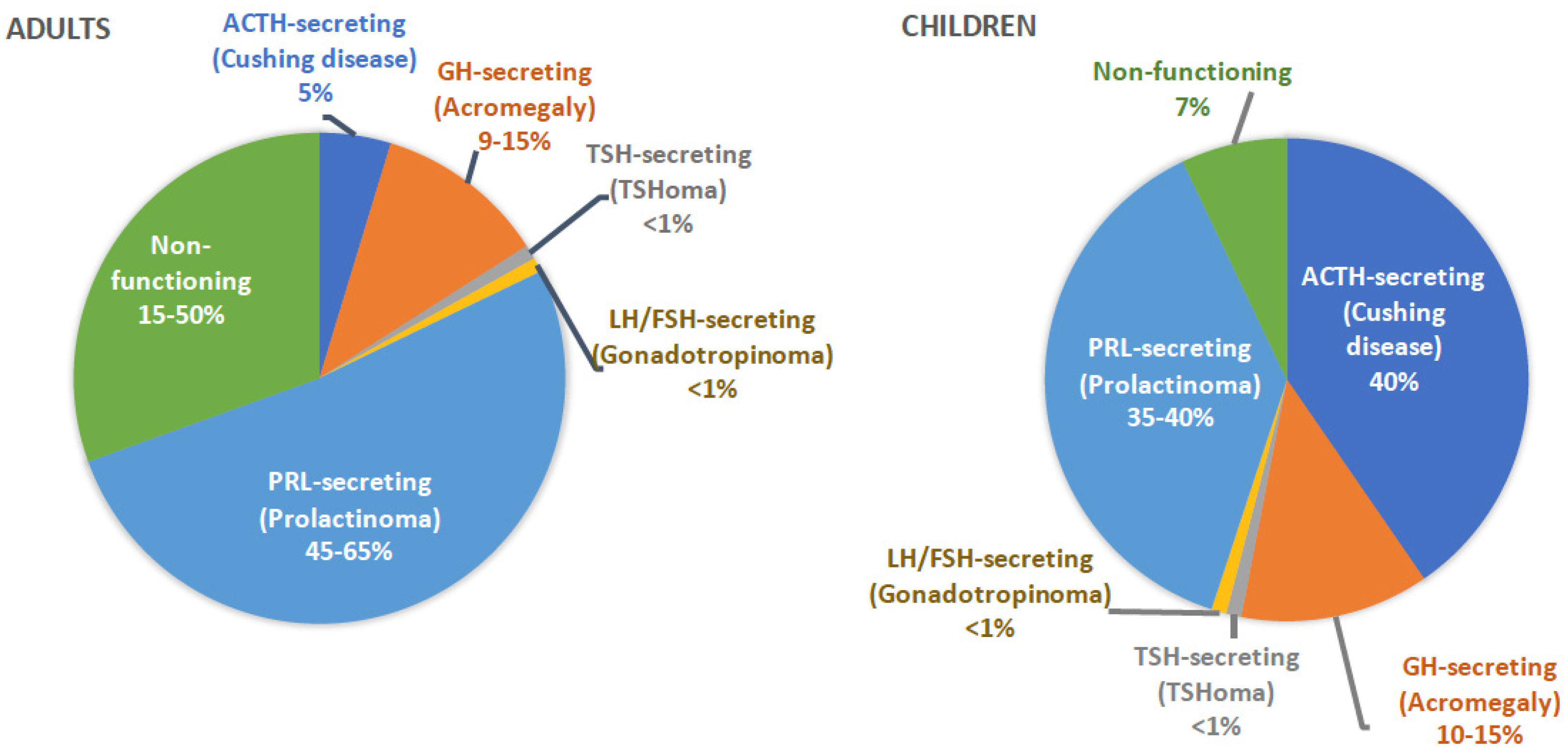
PAs can be classified based on their functional status (Figure 1). In adults, most PAs are prolactin (PRL)-secreting, while non-functioning adenomas represent the second most common type. In children, depending on the study population, ACTH- and PRL-secreting adenomas are the most commonly encountered subtypes [5]. PAs may also be classified as sporadic (95% of cases), when relevant family history is not present, or familial (5% of cases), when additional family members with similar or relevant disorders are identified [6].
2. Germline Defect and Associated Syndromes
2.1. Familial Isolated Pituitary Adenomas (FIPA)
The term Familial Isolated Pituitary Adenoma (FIPA) is used to describe families with at least two members with pituitary adenomas, with or without other abnormalities [7]. FIPA accounts for 2–4% of all patients with PAs [7]. Tumors within a family can be homologous (of the same subtype) or heterologous (of different subtypes) [7].
Aryl hydrocarbon receptor interacting protein (AIP) gene mutations were described as a cause of FIPA in 2006, and they are currently thought to account for almost 15% of all FIPA cases; this number is even higher (up to 75%) when families with GH-secreting adenomas are selected [8,9]. AIP gene defects are less common in sporadic pituitary adenomas identified in up to 8% of all cases [10,11]. However, when younger patients (<30 years old) with macroadenomas, or children and adolescents <18 years old are selected, up to 20.5% of cases with sporadic PAs may harbor an AIP mutation [12,13,14,15]. The exact mechanism of the pituitary tumorigenesis with AIP mutations is not clear. Some evidence suggests that there is interaction of AIP in the synthesis of cAMP, and decreased AIP activity leads to aberrant cAMP levels, which then affect several pathways involving cell proliferation [16].
Patients with AIP mutations commonly present with GH-secreting adenomas; the second most common presentation is that of GH/PRL co-secreting adenomas. It has been often described that PAs with AIP mutations have a more aggressive presentation compared to AIP-negative tumors: patients often present in younger age, with larger tumors, higher chance of invasion of surrounding tissues, higher risk for apoplexy, and less chance for control with one intervention, especially in the pediatric population [17,18,19,20,21,22].
2.2. Multiple Endocrine Neoplasia Syndromes
Multiple endocrine neoplasia (MEN) syndromes are autosomal dominant disorders that present with combination of tumors in at least two endocrine systems [23].
MEN 1 (OMIM#131100) is caused by mutations in the tumor suppressor gene MEN1 [24] Patients with MEN1 present with anterior pituitary adenomas in approximately 40% of all cases [25,26]. Although pituitary adenomas commonly present in the third to fourth decade of life, they have been described in children as young as 5 years of age [26,27,28,29,30]. Notably, PAs may be the first manifestation of MEN1 syndrome, and evaluation for other related comorbidities may be indicated [25,26,31]. Most of the PAs in MEN1 are PRL-secreting (42–62%) or non-functioning tumors (15–42%), but GH- (6.5–9%) and ACTH-secreting (3–4%) adenomas have also been described in Table 1 [25,26].
Interestingly, PAs in MEN1 have higher chance of co-secreting multiple hormones compared to MEN1-negative patients, in up to 39% of cases [27]. PAs in MEN1 are considered more aggressive and at higher risk for resistance to treatment, especially in children with large prolactinomas [32]. Somatic MEN1 gene mutations are not commonly found in sporadic pituitary tumors [33,34].
MEN2A (OMIM#171400) and MEN2B (OMIM#162300) syndromes, caused by RET gene mutations, have rarely been associated with PAs [35]. RET gene codes for a transmembrane receptor with tyrosine kinase activity that acts as proto-oncogene [36]. To date, only few case reports have described patients with MEN2A/2B and PAs: GH-secreting (n = 1), ACTH-secreting (n = 1) and non-functioning (n = 1) adenomas [37,38,39]. Furthermore, RET gene mutations do not commonly present in patients with isolated sporadic or familial PAs, suggesting that it is a rare cause of pituitary adenomas [40,41,42].
MEN4 (OMIM#610755) is caused by CDKN1B gene mutations, which codes for a cyclin-dependent kinase (p27) that regulates cell cycle and progression from G1 to S phase of mitosis [43]. MEN4 is a rare genetic syndrome, accounting for approximately 1.5–3% of patients clinically classified as MEN1, without genetic defects in MEN1 gene [44,45]. Of the reported index cases to date, five patients have been diagnosed with PAs (two with GH-secreting, two with ACTH-secreting, and one with non-functioning adenoma) [44,45,46,47,48,49]. CDKN1B gene mutations in FIPA have been a rare entity and are described in approximately 2% of AIP-negative FIPA kindreds [50]. To date, only one patient with isolated sporadic GH-secreting PA has been described in the literature [51].
2.3. Carney Complex
Carney complex (CNC) describes the constellation of myxomas, spotty skin pigmentation, and endocrine overactivity [52,53]. Germline mutations of the PRKAR1A gene are responsible for more than 70% of cases of CNC (OMIM#160980), whereas few patients may harbor defects at another locus on chromosome 2p16 [54,55]. PRKAR1A codes for the type 1 alpha regulatory subunit of the protein kinase A (PKA) tetramer. Inactivating mutations of PRKAR1A lead to dissociation of the regulatory from the catalytic subunit, resulting in aberrant activity of PKA and phosphorylation of downstream targets, leading to cell proliferation and tumor formation [53].
Amongst the common endocrine abnormalities described in CNC are pituitary hyperplasia and PAs that are often associated with GH and/or PRL excess [56]. Although definite adenomas are present in 15% of patients, abnormal GH response to various stimuli, such as glucose or TRH, is present in almost 75% of patients [57,58]. Pituitary involvement in CNC is thought to be a progressive disorder with normal pituitary tissue progressing to somato(mammo)troph hyperplasia and subsequently, to distinct tumor formation [58]. Thus, multiple adenomas may be present synchronous or metachronous in the same patient [59]. Once diagnosed, GH excess is usually slowly progressive and although transsphenoidal resection of PAs may be attempted, there is high risk for recurrence. Medical therapy is often offered to the patients and sometimes, partial or complete hypophysectomy may be needed for control of disease [58,59].
Although CNC was thought to be associated almost exclusively with GH and /or PRL excess, most recently, two patients with Cushing disease (CD) have also been described, showing that other pituitary cell lineages may be rarely affected [60,61]. Somatic PRKAR1A gene changes are not reported in sporadic PAs [62,63].
2.4. McCune-Albright Syndrome (MAS)
The classic presentation of MAS (OMIM#174800) includes the triad of polyostotic fibrous dysplasia (FD), café-au-lait pigmentation and precocious puberty [64]. The disease is the result of postzygotic activating mutations of the GNAS1 gene product, the cAMP-regulating protein Gsalpha (Gsα) [65]. It is now well recognized that additional endocrine overactivity disorders, other than precocious puberty, are part of the condition, including GH excess. GH excess in MAS presents in almost 21% of patients and may contribute to worsening of FD, vision and hearing loss, and macrocephaly [66]. For that reason, prompt medical therapy is recommended in all patients, while surgical intervention is not frequently attempted due to thick bones, the potential for worsening of skull FD, as well as the need for partial or total hypophysectomy [64].
2.5. X-Linked Acrogigantism (X-LAG)
X-LAG (OMIM#300942) has been recently described in patients with early onset GH excess [67]. X-LAG is caused by germline or somatic mosaic microduplications of Xq26.3, involving a G-protein-coupled receptor gene (GPR101) [68,69].
In a large study of 143 pediatric patients with gigantism, 10% of patients had microduplication of Xq26.3, two in familial cases and ten in sporadic adenomas [70]. Compared to patients without an identified genetic etiology, patients presented younger than the remaining patients, were more likely to co-secrete PRL, and had less risk of invasion of surrounding tissues [70]. In a cohort of 18 patients with X-LAG, mean age at diagnosis was 41 months and most patients had a macroadenoma identified on MRI, although no giant adenoma (by criteria of diameter more than 4 cm) was reported [67]. X-LAG is generally recognized as an aggressive disease given the difficulty to control GH excess. Most of the patients require multiple interventions (surgical and medical), and sometimes, subtotal or total hypophysectomy may be necessary. Radiation therapy is not generally helpful [67,71].
2.6. 3 P Association (3PAs)
The three P association or 3PAs is another recently identified condition involving the combination of pituitary adenomas, pheochromocytomas (PHEO) and/or paragangliomas (PGL) [72]. Xekouki et al. described that up to 75% of familial cases with 3PAs harbor pathogenic variants in the SDHx (SDHB and SDHD) genes [72]. Succinate dehydrogenase is part of the mitochondrial complex II and plays a significant role in energy production through the Krebs cycle and the respiratory chain through electron transfer [73]. Additional studies have further contributed in the genetic spectrum of the disease, by identifying additional genetic causes of the association (SDHA, SDHAF2, VHL, MEN1, RET and MAX) [74,75,76,77,78]. The presenting pituitary tumors are more commonly PRL- or GH-secreting or non-functioning adenomas, but they are thought to be more aggressive in presentation and more likely to be resistant to standard therapy [77].
2.7. DICER1
DICER1 codes for a small RNA processing endoribonuclease that cleaves double stranded RNA into small interfering RNAs and mature miRNAs [79]. DICER1 or pleuropulmonary syndrome (OMIM#601200) is an autosomal dominant pleuropulmonary blastoma, familial tumor and dysplasia syndrome, which involves various tumors, such as pleuropulmonary blastomas, cystic nephromas, Sertoli-Leydig cell tumors, multinodular goiter and other [80].
A rare but almost pathognomonic manifestation of DICER1 syndrome is pituitary blastoma (PitB). PitBs differ from PAs in terms of their histological characteristics (since these are embryonic tumors) but given the potential for hormone production, they should be considered in the context of pituitary tumors. ACTH-secreting PitBs, although extremely rare, are almost always associated with DICER1 mutations [81,82]. They are always diagnosed in infants and toddlers, less than 24 months of age [82]. Their management involves, in most cases, surgical removal, while at least one of the patients was treated with TMZ and radiation therapy. Four of the eleven reported patients died from complications of their disease, while at least two patients experienced recurrence [82]. Since PitBs are a rare association of DICER1 syndrome, routine screening with imaging or biochemical studies is not currently recommended for patients with DICER1 syndrome [83].
Recently, a case of isolated PRL-secreting adenoma in a 50-year old patient has been reported. Although histologic evaluation of the identified sellar tumor was not available, and the patient did not respond to medical therapy, this report expands the potential implications of DICER1 in adult-onset pituitary tumorigenesis [84].
2.8. Tuberous Sclerosis (TSC)
TSC is an autosomal dominant syndrome caused by genetic defects of TSC1 (OMIM#191100) or TSC2 (OMIM#613254) genes, which code for hamartin and tuberin respectively. TSC1/TSC2 mediate PI3K/Akt activation and lead to inhibition of the mTOR pathway [85].
2.9. Less Common Germline Genetic Defects Potentially Associated with PAs
NF1 (OMIM#613675) is an autosomal dominant syndrome caused by mutations or deletions in the NF1 gene, reported in 1:3500 births [85]. NF1 codes for neurofibromin which acts as a Ras-GTPase-activating protein; neurofibromin deficiency leads to constitutive activation of Ras-dependent pathways, namely Ras/Raf/MEK and Ras/PI3K/TSC/mTOR [85]. GH excess presents in 5.5–10.9% of patients with NF1 and optic pathway gliomas (OPGs), and it is thought to result from suppression of the hypothalamic somatostatin tone, while GHRH overactivity from OPGs has also been postulated in certain cases [90,91]. As a result, there is diffuse pituitary hyperplasia and no distinct adenoma is usually identified. Only one patient with a GH-secreting adenoma has been reported to date [92]. However, NF1 should remain in the differential diagnosis when evaluating a patient with acromegaly/gigantism.
Recently, Hernandez-Ramirez et al. described four potentially pathogenic variants in the CABLES1 gene in patients with CD. CABLES1 interacts with cyclin-dependent kinase 3 and genetic defects lead to impaired inhibition of cell growth [93]. CNVs and methylation defects of other cyclin-dependent kinases (CDK2A and CDKN2C, coding for p16 and p18) have been reported in studies of PAs [94,95]. Additionally, a somatic mutation in DKC1 gene, coding for dyskeratin, associated with X-Linked dyskeratosis congenita when present in germline, has been described in a patient with a non-functioning pituitary adenoma. The mutation is potentially associated with decreased p27 levels or defects in rRNA modification [96].
Finally, few patients with diagnosis of PA and additional genetic syndromes have been reported in the literature, for example, a patient with Beckwith-Wiedemann syndrome (loss of methylation of imprinting critical region 2 on chromosome 11p) and ACTH-secreting adenoma, two family members with Cantu syndrome (ABCC9) and non-functioning adenomas, a patient with autosomal dominant polycystic kidney disease (PKD1) and acromegaly, and a patient with X-linked adrenal hypoplasia (due to a DAX1 defect) and ACTH-secreting adenoma [97,98,99,100]. The etiologic association of the pathogenesis of PA with the identified germline genetic defect is not confirmed in most of them, however, potential relationship cannot be excluded.
3. Somatic Changes
As mentioned above, somatic changes of genes involved in identified syndromes when present in germline may be identified exclusively in the tumor level in certain cases. For example, GNAS mutations are present in up to 50% of GH-secreting adenomas. Below we present genetic defects reported mainly in the tumor level of PAs.
3.1. Ubiquitin Specific Peptidase 8 (USP8)
USP8 is involved in the deubiquitination process of epidermal growth factor receptor (EGFR). Gain-of-function USP8 gene defects lead to increased EGFR levels. In corticotroph cells, this defect results in high POMC expression and ACTH secretion [101,102]. Somatic defects of USP8 represent the most frequent genetic defect in CD, present in approximately 20–60% of all ACTH-secreting adenomas [101,102,103,104,105,106]. However, they are uncommon in other PAs. Of note, all USP8 somatic mutations associated with CD are located in the 14-3-3 binding motif (between amino acids 713 and 720) [101,102].
The prognosis of patients with somatic USP8 mutations differs in various studies. Some reports of increased risk for recurrence of patients with somatic USP8 mutations have not been replicated by others [104,106,107]. However, the potentially aggressive behavior of this genetic defect is evident in the patient with germline USP8 defect, described recently by Cohen et al. [108]. The patient had severe recurrent CD difficult to control with surgical and medical therapies [108].
3.2. USP48 and BRAF
With the understanding of the importance of USP8 in corticotropinomas, further studies for other genes related to the MAPK pathway have been published. Recently, USP48 and BRAF have been reported as additional target genes, with somatic variants of BRAF gene in 16% of patients and of USP48 gene in 23% of USP8-negative corticotropinomas [109]. Of interest, variants in these genes were not detected in other pituitary tumors, suggesting a specific defect in the POMC regulation [109].
3.3. GNAS
Somatic GNAS mutations are common in sporadic GH-secreting adenomas presenting in up to 50% of these tumors [110,111]. Mutations are usually located at codons 201 and 227, and lead to activation of the Gsa subunit of GNAS, leading to increased adenylate cyclase activity, similarly to the defect seen in patients with MAS. Because of paternal imprinting of GNAS in the pituitary gland, mutations need to occur at the maternal allele to result in pituitary tumorigenesis [112]. A limited number of ACTH-secreting adenomas with somatic GNAS gene defects has been reported, showing that there may be a rare association with CD [113,114].
3.4. The Phosphoinositide 3-Kinase (PI3K)/AKT Pathway
The PI3K/AKT pathway regulates several cellular functions, including cell survival, growth, proliferation and metabolism [115]. Gene defects, including pathogenic variants and amplifications, in PIK3CA have been isolated in several cancers [116]. Studies in PAs identified a potential role in pituitary tumorigenesis as well with a frequency of somatic defects in 2.3–12.1% of all tumors, with higher incidence in invasive PAs [117,118].
3.5. The p53 Tumor Suppressor Gene
TP53 codes for a tumor suppressor protein that has important implication in human carcinogenesis. Although p53 expression in pituitary tumors is associated with more aggressive behavior, several studies have failed to show a significant role of genetic defects of TP53 in pituitary tumorigenesis [119,120,121]. Few cases of atypical PAs and pituitary carcinomas with somatic TP53 defects have only been reported to date [122,123,124].
3.6. Copy Number Variations (CNVS) at the Chromosomal Level
Several studies have investigated the presence of CNVs in PAs. Although no recurrent CNV has been clearly noted, CNVs in chromosomes 1p and 11p have been reported in several occasions [125,126].
Recently, Bi et al. described a different profile of genomic aberrations: in a cohort of 42 PAs, a group of “disrupted” tumors, defined as large CNVs encompassing on average 39% of the tumor genome, were noted. These tumors were more likely to be functional adenomas, without evidence of more aggressive behavior [127,128]. Similar results were further described by other groups in GH-secreting tumors [129,130]. Our group also supported these studies by identifying a subgroup of patients with CD that harbored large genomic aberrations, involving up to 59% of the tumor genome. These tumors were associated with larger size and higher risk for cavernous sinus invasion [131].
4. Other Genomic and/or Molecular Events Associated with Various Features of PAs
4.1. Epigenetic Modifications of Pituitary Adenomas
The understanding of pathogenesis, differentiation and presentation of PAs has been further advanced through studies of epigenetic modifications.
Genome-wide methylation analyses of PAs have identified changes in methylation profile between normal pituitary tissue and PAs and attempted to clarify the differences between various subtypes of PAs [132,133]. Although the results have not been always consistent, changes in the methylation pattern of tumor suppressor and cell-cycle regulating genes (such as CASP8, tp73, RASSF1, Rb, p16, p18, SFN and other) or genes involved in the behavior of the tumors and their potential to invade tissues, like cell adhesion genes have been described [95,133,134,135,136]. Methylation changes also correlate with certain tumor characteristics, such as their size, functional status, and invasion of surrounding tissues, but again, results have not been replicated in all studies [94,133,135,137,138,139].
Growth factors have also been studied in relation to pituitary development and tumorigenesis [140]. FGFR2, and specifically, the predominat isoform FGFR2-IIIb) is downregulated in half of the pituitary adenomas, possibly due to increased promoter methylation, with potential implication for the expression of certain cyclin dependent kinases (such as p21 and p27) [141]. Furthermore, FGFR2 interacts with melanoma-associated antigen-3 (MAGE-A3) complex which further regulates p53 expression and leads to disordered cell cycle regulation [142]. FGFR4, on the other hand, is overexpressed in PAs, with potential implication in tumorigenesis [143].
Histone modifications and chromatin changes may also explain some of the PA characteristics, leading to altered expression of important cell-cycle genes (like Rb, p21 and p27) [142]. Examples of histone modifications and chromatin remodeling include the case of Ikaros, where expression of a certain isoform results in histone 3 acetylation and activation of the Bcl-XL promoter, leading to increased survival of pituitary cells [144,145].
4.2. miRNAs
miRNAs are small non-coding RNAs that are involved in cell cycle regulation and cancer pathogenesis via control of expression of various genes [146,147]. Over the last 10 years, studies on differentially expressed miRNAs in PAs compared to normal pituitary tissues have identified miRNAs with potential interest. For example, downregulation of miR-326, miR-432, miR-570, and miR-603, has been described in GH-secreting adenomas. These miRNAs potentially target the HMGA2 and E2F1 genes and their downregulation leads to increased expression and results in increased cell proliferation [148]. Several additional miRNAs, either upregulated or downregulated targeting genes affecting cell proliferation, apoptosis, invasion and even response to therapy, have been described, with potential implications for diagnostic, prognostic and therapeutic purposes [149,150,151].
5. Conclusions
The genomic landscape of PAs remains complex. Germline and somatic genetic defects contribute to our understanding of their pathogenesis, but do not explain the majority of them. Additional information derived from other gene regulation mechanisms should be considered in combination to describe the full picture of pituitary tumorigenesis.
Author Contributions
C.T. and C.A.S. contributed equally to this manuscript. All authors have read and agree to the published version of the manuscript.
Funding
The work was supported by the Intramural Research Program, Eunice Kennedy Shriver National Institute of Child Health & Human Development (NICHD), National Institutes of Health.
Conflicts of Interest
Stratakis holds patents on technologies involving PRKAR1A and related genes, and his laboratory has received research funding support by Pfizer Inc, unrelated to this project.
References
- Lim, C.T.; Korbonits, M. Update on the Clinicopathology of Pituitary Adenomas. Endocr. Pract. 2018, 24, 473–488. [Google Scholar] [CrossRef]
- Ezzat, S.; Asa, S.L.; Couldwell, W.T.; Barr, C.E.; Dodge, W.E.; Vance, M.L.; McCutcheon, I.E. The prevalence of pituitary adenomas: A systematic review. Cancer 2004, 101, 613–619. [Google Scholar] [CrossRef]
- Souteiro, P.; Maia, R.; Santos-Silva, R.; Figueiredo, R.; Costa, C.; Belo, S.; Castro-Correia, C.; Carvalho, D.; Fontoura, M. Pituitary incidentalomas in paediatric age are different from those described in adulthood. Pituitary 2019, 22, 124–128. [Google Scholar] [CrossRef]
- Freda, P.U.; Beckers, A.M.; Katznelson, L.; Molitch, M.E.; Montori, V.M.; Post, K.D.; Vance, M.L.; Endocrine, S. Pituitary incidentaloma: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 894–904. [Google Scholar] [CrossRef]
- Perry, A.; Graffeo, C.S.; Marcellino, C.; Pollock, B.E.; Wetjen, N.M.; Meyer, F.B. Pediatric Pituitary Adenoma: Case Series, Review of the Literature, and a Skull Base Treatment Paradigm. J. Neurol. Surg. B Skull Base 2018, 79, 91–114. [Google Scholar] [CrossRef]
- Daly, A.F.; Rixhon, M.; Adam, C.; Dempegioti, A.; Tichomirowa, M.A.; Beckers, A. High prevalence of pituitary adenomas: A cross-sectional study in the province of Liege, Belgium. J. Clin. Endocrinol. Metab. 2006, 91, 4769–4775. [Google Scholar] [CrossRef]
- Stiles, C.E.; Korbonits, M. Familial Isolated Pituitary Adenoma. In Endotext; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., Dungan, K., Grossman, A., Hershman, J.M., Kaltsas, G., Koch, C., Kopp, P., et al., Eds.; South Dartmouth: Dartmouth, MA, USA, 2000. [Google Scholar]
- Vierimaa, O.; Georgitsi, M.; Lehtonen, R.; Vahteristo, P.; Kokko, A.; Raitila, A.; Tuppurainen, K.; Ebeling, T.M.; Salmela, P.I.; Paschke, R.; et al. Pituitary adenoma predisposition caused by germline mutations in the AIP gene. Science 2006, 312, 1228–1230. [Google Scholar] [CrossRef]
- Daly, A.F.; Vanbellinghen, J.F.; Khoo, S.K.; Jaffrain-Rea, M.L.; Naves, L.A.; Guitelman, M.A.; Murat, A.; Emy, P.; Gimenez-Roqueplo, A.P.; Tamburrano, G.; et al. Aryl hydrocarbon receptor-interacting protein gene mutations in familial isolated pituitary adenomas: Analysis in 73 families. J. Clin. Endocrinol. Metab. 2007, 92, 1891–1896. [Google Scholar] [CrossRef]
- Iwata, T.; Yamada, S.; Mizusawa, N.; Golam, H.M.; Sano, T.; Yoshimoto, K. The aryl hydrocarbon receptor-interacting protein gene is rarely mutated in sporadic GH-secreting adenomas. Clin. Endocrinol. (Oxf.) 2007, 66, 499–502. [Google Scholar] [CrossRef]
- Hernandez-Ramirez, L.C.; Gabrovska, P.; Denes, J.; Stals, K.; Trivellin, G.; Tilley, D.; Ferrau, F.; Evanson, J.; Ellard, S.; Grossman, A.B.; et al. Landscape of Familial Isolated and Young-Onset Pituitary Adenomas: Prospective Diagnosis in AIP Mutation Carriers. J. Clin. Endocrinol. Metab. 2015, 100, E1242–E1254. [Google Scholar] [CrossRef] [Green Version]
- Schofl, C.; Honegger, J.; Droste, M.; Grussendorf, M.; Finke, R.; Plockinger, U.; Berg, C.; Willenberg, H.S.; Lammert, A.; Klingmuller, D.; et al. Frequency of AIP gene mutations in young patients with acromegaly: A registry-based study. J. Clin. Endocrinol. Metab. 2014, 99, E2789–E2793. [Google Scholar] [CrossRef] [Green Version]
- Georgitsi, M.; De Menis, E.; Cannavo, S.; Makinen, M.J.; Tuppurainen, K.; Pauletto, P.; Curto, L.; Weil, R.J.; Paschke, R.; Zielinski, G.; et al. Aryl hydrocarbon receptor interacting protein (AIP) gene mutation analysis in children and adolescents with sporadic pituitary adenomas. Clin. Endocrinol. (Oxf.) 2008, 69, 621–627. [Google Scholar] [CrossRef]
- Daly, A.; Cano, D.A.; Venegas, E.; Petrossians, P.; Dios, E.; Castermans, E.; Flores-Martinez, A.; Bours, V.; Beckers, A.; Soto, A. AIP and MEN1 mutations and AIP immunohistochemistry in pituitary adenomas in a tertiary referral center. Endocr. Connect. 2019, 8, 338–348. [Google Scholar] [CrossRef] [Green Version]
- Tichomirowa, M.A.; Barlier, A.; Daly, A.F.; Jaffrain-Rea, M.L.; Ronchi, C.; Yaneva, M.; Urban, J.D.; Petrossians, P.; Elenkova, A.; Tabarin, A.; et al. High prevalence of AIP gene mutations following focused screening in young patients with sporadic pituitary macroadenomas. Eur. J. Endocrinol. 2011, 165, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Tuominen, I.; Heliovaara, E.; Raitila, A.; Rautiainen, M.R.; Mehine, M.; Katainen, R.; Donner, I.; Aittomaki, V.; Lehtonen, H.J.; Ahlsten, M.; et al. AIP inactivation leads to pituitary tumorigenesis through defective Galphai-cAMP signaling. Oncogene 2015, 34, 1174–1184. [Google Scholar] [CrossRef]
- Daly, A.F.; Tichomirowa, M.A.; Petrossians, P.; Heliovaara, E.; Jaffrain-Rea, M.L.; Barlier, A.; Naves, L.A.; Ebeling, T.; Karhu, A.; Raappana, A.; et al. Clinical characteristics and therapeutic responses in patients with germ-line AIP mutations and pituitary adenomas: An international collaborative study. J. Clin. Endocrinol. Metab. 2010, 95, E373–E383. [Google Scholar] [CrossRef] [Green Version]
- Caimari, F.; Hernandez-Ramirez, L.C.; Dang, M.N.; Gabrovska, P.; Iacovazzo, D.; Stals, K.; Ellard, S.; Korbonits, M.; International, F.C. Risk category system to identify pituitary adenoma patients with AIP mutations. J. Med. Genet. 2018, 55, 254–260. [Google Scholar] [CrossRef] [Green Version]
- Naves, L.A.; Jaffrain-Rea, M.L.; Vencio, S.A.; Jacomini, C.Z.; Casulari, L.A.; Daly, A.F.; Beckers, A. Aggressive prolactinoma in a child related to germline mutation in the ARYL hydrocarbon receptor interacting protein (AIP) gene. Arq. Bras. Endocrinol. Metabol. 2010, 54, 761–767. [Google Scholar] [CrossRef] [Green Version]
- Joshi, K.; Daly, A.F.; Beckers, A.; Zacharin, M. Resistant Paediatric Somatotropinomas due to AIP Mutations: Role of Pegvisomant. Horm. Res. Paediatr. 2018, 90, 196–202. [Google Scholar] [CrossRef]
- Personnier, C.; Cazabat, L.; Bertherat, J.; Gaillard, S.; Souberbielle, J.C.; Habrand, J.L.; Dufour, C.; Clauser, E.; SainteRose, C.; Polak, M. Clinical features and treatment of pediatric somatotropinoma: Case study of an aggressive tumor due to a new AIP mutation and extensive literature review. Horm. Res. Paediatr. 2011, 75, 392–402. [Google Scholar] [CrossRef]
- Dutta, P.; Reddy, K.S.; Rai, A.; Madugundu, A.K.; Solanki, H.S.; Bhansali, A.; Radotra, B.D.; Kumar, N.; Collier, D.; Iacovazzo, D.; et al. Surgery, Octreotide, Temozolomide, Bevacizumab, Radiotherapy, and Pegvisomant Treatment of an AIP MutationPositive Child. J. Clin. Endocrinol. Metab. 2019, 104, 3539–3544. [Google Scholar] [CrossRef] [Green Version]
- Falchetti, A.; Marini, F.; Luzi, E.; Tonelli, F.; Brandi, M.L. Multiple endocrine neoplasms. Best Pract. Res. Clin. Rheumatol. 2008, 22, 149–163. [Google Scholar] [CrossRef]
- Chandrasekharappa, S.C.; Guru, S.C.; Manickam, P.; Olufemi, S.E.; Collins, F.S.; Emmert-Buck, M.R.; Debelenko, L.V.; Zhuang, Z.; Lubensky, I.A.; Liotta, L.A.; et al. Positional cloning of the gene for multiple endocrine neoplasia-type 1. Science 1997, 276, 404–407. [Google Scholar] [CrossRef]
- De Laat, J.M.; Dekkers, O.M.; Pieterman, C.R.; Kluijfhout, W.P.; Hermus, A.R.; Pereira, A.M.; van der Horst-Schrivers, A.N.; Drent, M.L.; Bisschop, P.H.; Havekes, B.; et al. Long-Term Natural Course of Pituitary Tumors in Patients With MEN1: Results From the DutchMEN1 Study Group (DMSG). J. Clin. Endocrinol. Metab. 2015, 100, 3288–3296. [Google Scholar] [CrossRef] [Green Version]
- Verges, B.; Boureille, F.; Goudet, P.; Murat, A.; Beckers, A.; Sassolas, G.; Cougard, P.; Chambe, B.; Montvernay, C.; Calender, A. Pituitary disease in MEN type 1 (MEN1): Data from the France-Belgium MEN1 multicenter study. J. Clin. Endocrinol. Metab. 2002, 87, 457–465. [Google Scholar] [CrossRef]
- Trouillas, J.; Labat-Moleur, F.; Sturm, N.; Kujas, M.; Heymann, M.F.; Figarella-Branger, D.; Patey, M.; Mazucca, M.; Decullier, E.; Verges, B.; et al. Pituitary tumors and hyperplasia in multiple endocrine neoplasia type 1 syndrome (MEN1): A case-control study in a series of 77 patients versus 2509 non-MEN1 patients. Am. J. Surg. Pathol. 2008, 32, 534–543. [Google Scholar] [CrossRef]
- Giusti, F.; Cianferotti, L.; Boaretto, F.; Cetani, F.; Cioppi, F.; Colao, A.; Davi, M.V.; Faggiano, A.; Fanciulli, G.; Ferolla, P.; et al. Multiple endocrine neoplasia syndrome type 1: Institution, management, and data analysis of a nationwide multicenter patient database. Endocrine 2017, 58, 349–359. [Google Scholar] [CrossRef] [Green Version]
- Rix, M.; Hertel, N.T.; Nielsen, F.C.; Jacobsen, B.B.; Hoejberg, A.S.; Brixen, K.; Hangaard, J.; Kroustrup, J.P. Cushing’s disease in childhood as the first manifestation of multiple endocrine neoplasia syndrome type 1. Eur. J. Endocrinol. 2004, 151, 709–715. [Google Scholar] [CrossRef] [Green Version]
- Stratakis, C.A.; Schussheim, D.H.; Freedman, S.M.; Keil, M.F.; Pack, S.D.; Agarwal, S.K.; Skarulis, M.C.; Weil, R.J.; Lubensky, I.A.; Zhuang, Z.; et al. Pituitary macroadenoma in a 5-year-old: An early expression of multiple endocrine neoplasia type 1. J. Clin. Endocrinol. Metab. 2000, 85, 4776–4780. [Google Scholar] [CrossRef]
- Makri, A.; Bonella, M.B.; Keil, M.F.; Hernandez-Ramirez, L.; Paluch, G.; Tirosh, A.; Saldarriaga, C.; Chittiboina, P.; Marx, S.J.; Stratakis, C.A.; et al. Children with MEN1 gene mutations may present first (and at a young age) with Cushing disease. Clin. Endocrinol. (Oxf.) 2018, 89, 437–443. [Google Scholar] [CrossRef]
- Salenave, S.; Ancelle, D.; Bahougne, T.; Raverot, G.; Kamenicky, P.; Bouligand, J.; Guiochon-Mantel, A.; Linglart, A.; Souchon, P.F.; Nicolino, M.; et al. Macroprolactinomas in children and adolescents: Factors associated with the response to treatment in 77 patients. J. Clin. Endocrinol. Metab. 2015, 100, 1177–1186. [Google Scholar] [CrossRef] [Green Version]
- Wenbin, C.; Asai, A.; Teramoto, A.; Sanno, N.; Kirino, T. Mutations of the MEN1 tumor suppressor gene in sporadic pituitary tumors. Cancer Lett. 1999, 142, 43–47. [Google Scholar] [CrossRef]
- Zhuang, Z.; Ezzat, S.Z.; Vortmeyer, A.O.; Weil, R.; Oldfield, E.H.; Park, W.S.; Pack, S.; Huang, S.; Agarwal, S.K.; Guru, S.C.; et al. Mutations of the MEN1 tumor suppressor gene in pituitary tumors. Cancer Res. 1997, 57, 5446–5451. [Google Scholar]
- Mulligan, L.M.; Kwok, J.B.; Healey, C.S.; Elsdon, M.J.; Eng, C.; Gardner, E.; Love, D.R.; Mole, S.E.; Moore, J.K.; Papi, L.; et al. Germ-line mutations of the RET proto-oncogene in multiple endocrine neoplasia type 2A. Nature 1993, 363, 458–460. [Google Scholar] [CrossRef]
- Traugott, A.L.; Moley, J.F. The RET Protooncogene. Cancer Treat Res. 2010, 153, 303–319. [Google Scholar]
- Saito, T.; Miura, D.; Taguchi, M.; Takeshita, A.; Miyakawa, M.; Takeuchi, Y. Coincidence of multiple endocrine neoplasia type 2A with acromegaly. Am. J. Med. Sci. 2010, 340, 329–331. [Google Scholar] [CrossRef]
- Heinlen, J.E.; Buethe, D.D.; Culkin, D.J.; Slobodov, G. Multiple endocrine neoplasia 2a presenting with pheochromocytoma and pituitary macroadenoma. ISRN Oncol. 2011, 2011, 732452. [Google Scholar] [CrossRef] [Green Version]
- Ezzat, T.; Paramesawaran, R.; Phillips, B.; Sadler, G. MEN 2 syndrome masquerading as MEN 1. Ann. R Coll. Surg. Engl. 2012, 94, e206–e207. [Google Scholar] [CrossRef] [Green Version]
- Heliovaara, E.; Tuupanen, S.; Ahlsten, M.; Hodgson, S.; de Menis, E.; Kuismin, O.; Izatt, L.; McKinlay Gardner, R.J.; Gundogdu, S.; Lucassen, A.; et al. No evidence of RET germline mutations in familial pituitary adenoma. J. Mol. Endocrinol. 2011, 46, 1–8. [Google Scholar] [CrossRef]
- Komminoth, P.; Roth, J.; Muletta-Feurer, S.; Saremaslani, P.; Seelentag, W.K.; Heitz, P.U. RET proto-oncogene point mutations in sporadic neuroendocrine tumors. J. Clin. Endocrinol. Metab. 1996, 81, 2041–2046. [Google Scholar]
- Yoshimoto, K.; Tanaka, C.; Moritani, M.; Shimizu, E.; Yamaoka, T.; Yamada, S.; Sano, T.; Itakura, M. Infrequent detectable somatic mutations of the RET and glial cell line-derived neurotrophic factor (GDNF) genes in human pituitary adenomas. Endocr. J. 1999, 46, 199–207. [Google Scholar] [CrossRef] [Green Version]
- Sherr, C.J.; Roberts, J.M. CDK inhibitors: Positive and negative regulators of G1-phase progression. Genes Dev. 1999, 13, 1501–1512. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, S.K.; Mateo, C.M.; Marx, S.J. Rare germline mutations in cyclin-dependent kinase inhibitor genes in multiple endocrine neoplasia type 1 and related states. J. Clin. Endocrinol. Metab. 2009, 94, 1826–1834. [Google Scholar] [CrossRef] [Green Version]
- Georgitsi, M.; Raitila, A.; Karhu, A.; van der Luijt, R.B.; Aalfs, C.M.; Sane, T.; Vierimaa, O.; Makinen, M.J.; Tuppurainen, K.; Paschke, R.; et al. Germline CDKN1B/p27Kip1 mutation in multiple endocrine neoplasia. J. Clin. Endocrinol. Metab. 2007, 92, 3321–3325. [Google Scholar] [CrossRef] [Green Version]
- Occhi, G.; Regazzo, D.; Trivellin, G.; Boaretto, F.; Ciato, D.; Bobisse, S.; Ferasin, S.; Cetani, F.; Pardi, E.; Korbonits, M.; et al. A novel mutation in the upstream open reading frame of the CDKN1B gene causes a MEN4 phenotype. PLoS Genet. 2013, 9, e1003350. [Google Scholar] [CrossRef]
- Pellegata, N.S.; Quintanilla-Martinez, L.; Siggelkow, H.; Samson, E.; Bink, K.; Hofler, H.; Fend, F.; Graw, J.; Atkinson, M.J. Germ-line mutations in p27Kip1 cause a multiple endocrine neoplasia syndrome in rats and humans. Proc. Natl. Acad. Sci. USA 2006, 103, 15558–15563. [Google Scholar] [CrossRef] [Green Version]
- Molatore, S.; Marinoni, I.; Lee, M.; Pulz, E.; Ambrosio, M.R.; degli Uberti, E.C.; Zatelli, M.C.; Pellegata, N.S. A novel germline CDKN1B mutation causing multiple endocrine tumors: Clinical, genetic and functional characterization. Hum. Mutat. 2010, 31, E1825–E1835. [Google Scholar] [CrossRef] [Green Version]
- Frederiksen, A.; Rossing, M.; Hermann, P.; Ejersted, C.; Thakker, R.V.; Frost, M. Clinical Features of Multiple Endocrine Neoplasia Type 4: Novel Pathogenic Variant and Review of Published Cases. J. Clin. Endocrinol. Metab. 2019, 104, 3637–3646. [Google Scholar] [CrossRef]
- Tichomirowa, M.A.; Lee, M.; Barlier, A.; Daly, A.F.; Marinoni, I.; Jaffrain-Rea, M.L.; Naves, L.A.; Rodien, P.; Rohmer, V.; Faucz, F.R.; et al. Cyclin-dependent kinase inhibitor 1B (CDKN1B) gene variants in AIP mutation-negative familial isolated pituitary adenoma kindreds. Endocr. Relat. Cancer 2012, 19, 233–241. [Google Scholar] [CrossRef] [Green Version]
- Sambugaro, S.; Di Ruvo, M.; Ambrosio, M.R.; Pellegata, N.S.; Bellio, M.; Guerra, A.; Buratto, M.; Foschini, M.P.; Tagliati, F.; degli Uberti, E.; et al. Early onset acromegaly associated with a novel deletion in CDKN1B 5’UTR region. Endocrine 2015, 49, 58–64. [Google Scholar] [CrossRef]
- Stratakis, C.A. Carney complex: A familial lentiginosis predisposing to a variety of tumors. Rev. Endocr. Metab. Disord. 2016, 17, 367–371. [Google Scholar] [CrossRef]
- Salpea, P.; Stratakis, C.A. Carney complex and McCune Albright syndrome: An overview of clinical manifestations and human molecular genetics. Mol. Cell. Endocrinol. 2014, 386, 85–91. [Google Scholar] [CrossRef] [Green Version]
- Kirschner, L.S.; Carney, J.A.; Pack, S.D.; Taymans, S.E.; Giatzakis, C.; Cho, Y.S.; Cho-Chung, Y.S.; Stratakis, C.A. Mutations of the gene encoding the protein kinase A type I-alpha regulatory subunit in patients with the Carney complex. Nat. Genet. 2000, 26, 89–92. [Google Scholar] [CrossRef]
- Stratakis, C.A.; Carney, J.A.; Lin, J.P.; Papanicolaou, D.A.; Karl, M.; Kastner, D.L.; Pras, E.; Chrousos, G.P. Carney complex, a familial multiple neoplasia and lentiginosis syndrome. Analysis of 11 kindreds and linkage to the short arm of chromosome 2. J. Clin. Investig. 1996, 97, 699–705. [Google Scholar] [CrossRef] [Green Version]
- Courcoutsakis, N.A.; Tatsi, C.; Patronas, N.J.; Lee, C.C.; Prassopoulos, P.K.; Stratakis, C.A. The complex of myxomas, spotty skin pigmentation and endocrine overactivity (Carney complex): Imaging findings with clinical and pathological correlation. Insights Imaging 2013, 4, 119–133. [Google Scholar] [CrossRef] [Green Version]
- Pack, S.D.; Kirschner, L.S.; Pak, E.; Zhuang, Z.; Carney, J.A.; Stratakis, C.A. Genetic and histologic studies of somatomammotropic pituitary tumors in patients with the “complex of spotty skin pigmentation, myxomas, endocrine overactivity and schwannomas” (Carney complex). J. Clin. Endocrinol. Metab. 2000, 85, 3860–3865. [Google Scholar]
- Boikos, S.A.; Stratakis, C.A. Pituitary pathology in patients with Carney Complex: Growth-hormone producing hyperplasia or tumors and their association with other abnormalities. Pituitary 2006, 9, 203–209. [Google Scholar] [CrossRef]
- Lonser, R.R.; Mehta, G.U.; Kindzelski, B.A.; Ray-Chaudhury, A.; Vortmeyer, A.O.; Dickerman, R.; Oldfield, E.H. Surgical Management of Carney Complex-Associated Pituitary Pathology. Neurosurgery 2017, 80, 780–786. [Google Scholar] [CrossRef]
- Kiefer, F.W.; Winhofer, Y.; Iacovazzo, D.; Korbonits, M.; Wolfsberger, S.; Knosp, E.; Trautinger, F.; Hoftberger, R.; Krebs, M.; Luger, A.; et al. PRKAR1A mutation causing pituitary-dependent Cushing disease in a patient with Carney complex. Eur. J. Endocrinol. 2017, 177, K7–K12. [Google Scholar] [CrossRef] [Green Version]
- Hernandez-Ramirez, L.C.; Tatsi, C.; Lodish, M.B.; Faucz, F.R.; Pankratz, N.; Chittiboina, P.; Lane, J.; Kay, D.M.; Valdes, N.; Dimopoulos, A.; et al. Corticotropinoma as a Component of Carney Complex. J. Endocr. Soc. 2017, 1, 918–925. [Google Scholar] [CrossRef] [Green Version]
- Kaltsas, G.A.; Kola, B.; Borboli, N.; Morris, D.G.; Gueorguiev, M.; Swords, F.M.; Czirjak, S.; Kirschner, L.S.; Stratakis, C.A.; Korbonits, M.; et al. Sequence analysis of the PRKAR1A gene in sporadic somatotroph and other pituitary tumours. Clin. Endocrinol. (Oxf.) 2002, 57, 443–448. [Google Scholar] [CrossRef] [PubMed]
- Yamasaki, H.; Mizusawa, N.; Nagahiro, S.; Yamada, S.; Sano, T.; Itakura, M.; Yoshimoto, K. GH-secreting pituitary adenomas infrequently contain inactivating mutations of PRKAR1A and LOH of 17q23-24. Clin. Endocrinol. (Oxf.) 2003, 58, 464–470. [Google Scholar] [CrossRef] [Green Version]
- Dumitrescu, C.E.; Collins, M.T. McCune-Albright syndrome. Orphanet J. Rare Dis. 2008, 3, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinstein, L.S.; Shenker, A.; Gejman, P.V.; Merino, M.J.; Friedman, E.; Spiegel, A.M. Activating mutations of the stimulatory G protein in the McCune-Albright syndrome. N. Engl. J. Med. 1991, 325, 1688–1695. [Google Scholar] [CrossRef]
- Akintoye, S.O.; Chebli, C.; Booher, S.; Feuillan, P.; Kushner, H.; Leroith, D.; Cherman, N.; Bianco, P.; Wientroub, S.; Robey, P.G.; et al. Characterization of gsp-mediated growth hormone excess in the context of McCune-Albright syndrome. J. Clin. Endocrinol. Metab. 2002, 87, 5104–5112. [Google Scholar] [CrossRef] [Green Version]
- Beckers, A.; Lodish, M.B.; Trivellin, G.; Rostomyan, L.; Lee, M.; Faucz, F.R.; Yuan, B.; Choong, C.S.; Caberg, J.H.; Verrua, E.; et al. X-linked acrogigantism syndrome: Clinical profile and therapeutic responses. Endocr. Relat. Cancer 2015, 22, 353–367. [Google Scholar] [CrossRef]
- Trivellin, G.; Daly, A.F.; Faucz, F.R.; Yuan, B.; Rostomyan, L.; Larco, D.O.; Schernthaner-Reiter, M.H.; Szarek, E.; Leal, L.F.; Caberg, J.H.; et al. Gigantism and acromegaly due to Xq26 microduplications and GPR101 mutation. N. Engl. J. Med. 2014, 371, 2363–2374. [Google Scholar] [CrossRef]
- Daly, A.F.; Yuan, B.; Fina, F.; Caberg, J.H.; Trivellin, G.; Rostomyan, L.; de Herder, W.W.; Naves, L.A.; Metzger, D.; Cuny, T.; et al. Somatic mosaicism underlies X-linked acrogigantism syndrome in sporadic male subjects. Endocr. Relat. Cancer 2016, 23, 221–233. [Google Scholar] [CrossRef] [Green Version]
- Rostomyan, L.; Daly, A.F.; Petrossians, P.; Nachev, E.; Lila, A.R.; Lecoq, A.L.; Lecumberri, B.; Trivellin, G.; Salvatori, R.; Moraitis, A.G.; et al. Clinical and genetic characterization of pituitary gigantism: An international collaborative study in 208 patients. Endocr. Relat. Cancer 2015, 22, 745–757. [Google Scholar] [CrossRef]
- Naves, L.A.; Daly, A.F.; Dias, L.A.; Yuan, B.; Zakir, J.C.; Barra, G.B.; Palmeira, L.; Villa, C.; Trivellin, G.; Junior, A.J.; et al. Aggressive tumor growth and clinical evolution in a patient with X-linked acro-gigantism syndrome. Endocrine 2016, 51, 236–244. [Google Scholar] [CrossRef]
- Xekouki, P.; Szarek, E.; Bullova, P.; Giubellino, A.; Quezado, M.; Mastroyannis, S.A.; Mastorakos, P.; Wassif, C.A.; Raygada, M.; Rentia, N.; et al. Pituitary adenoma with paraganglioma/pheochromocytoma (3PAs) and succinate dehydrogenase defects in humans and mice. J. Clin. Endocrinol. Metab. 2015, 100, E710–E719. [Google Scholar] [CrossRef]
- Moosavi, B.; Berry, E.A.; Zhu, X.L.; Yang, W.C.; Yang, G.F. The assembly of succinate dehydrogenase: A key enzyme in bioenergetics. Cell. Mol. Life Sci. 2019, 76, 4023–4042. [Google Scholar] [CrossRef]
- Dwight, T.; Mann, K.; Benn, D.E.; Robinson, B.G.; McKelvie, P.; Gill, A.J.; Winship, I.; Clifton-Bligh, R.J. Familial SDHA mutation associated with pituitary adenoma and pheochromocytoma/paraganglioma. J. Clin. Endocrinol. Metab. 2013, 98, E1103–E1108. [Google Scholar] [CrossRef] [Green Version]
- Denes, J.; Swords, F.; Rattenberry, E.; Stals, K.; Owens, M.; Cranston, T.; Xekouki, P.; Moran, L.; Kumar, A.; Wassif, C.; et al. Heterogeneous genetic background of the association of pheochromocytoma/paraganglioma and pituitary adenoma: Results from a large patient cohort. J. Clin. Endocrinol. Metab. 2015, 100, E531–E541. [Google Scholar] [CrossRef]
- Roszko, K.L.; Blouch, E.; Blake, M.; Powers, J.F.; Tischler, A.S.; Hodin, R.; Sadow, P.; Lawson, E.A. Case Report of a Prolactinoma in a Patient With a Novel MAX Mutation and Bilateral Pheochromocytomas. J. Endocr. Soc. 2017, 1, 1401–1407. [Google Scholar] [CrossRef] [Green Version]
- Guerrero-Perez, F.; Fajardo, C.; Torres Vela, E.; Gimenez-Palop, O.; Lisbona Gil, A.; Martin, T.; Gonzalez, N.; Diez, J.J.; Iglesias, P.; Robledo, M.; et al. 3P association (3PAs): Pituitary adenoma and pheochromocytoma/paraganglioma. A heterogeneous clinical syndrome associated with different gene mutations. Eur. J. Intern. Med. 2019, 69, 14–19. [Google Scholar] [CrossRef]
- Daly, A.F.; Castermans, E.; Oudijk, L.; Guitelman, M.A.; Beckers, P.; Potorac, I.; Neggers, S.; Sacre, N.; van der Lely, A.J.; Bours, V.; et al. Pheochromocytomas and pituitary adenomas in three patients with MAX exon deletions. Endocr. Relat. Cancer 2018, 25, L37–L42. [Google Scholar] [CrossRef] [Green Version]
- Solarski, M.; Rotondo, F.; Foulkes, W.D.; Priest, J.R.; Syro, L.V.; Butz, H.; Cusimano, M.D.; Kovacs, K. DICER1 gene mutations in endocrine tumors. Endocr. Relat. Cancer 2018, 25, R197–R208. [Google Scholar] [CrossRef]
- Foulkes, W.D.; Priest, J.R.; Duchaine, T.F. DICER1: Mutations, microRNAs and mechanisms. Nat. Rev. Cancer 2014, 14, 662–672. [Google Scholar] [CrossRef]
- De Kock, L.; Sabbaghian, N.; Plourde, F.; Srivastava, A.; Weber, E.; Bouron-Dal Soglio, D.; Hamel, N.; Choi, J.H.; Park, S.H.; Deal, C.L.; et al. Pituitary blastoma: A pathognomonic feature of germ-line DICER1 mutations. Acta Neuropathol. 2014, 128, 111–122. [Google Scholar] [CrossRef]
- Tatsi, C.; Stratakis, C.A. Neonatal Cushing Syndrome: A Rare but Potentially Devastating Disease. Clin. Perinatol. 2018, 45, 103–118. [Google Scholar] [CrossRef]
- Schultz, K.A.P.; Williams, G.M.; Kamihara, J.; Stewart, D.R.; Harris, A.K.; Bauer, A.J.; Turner, J.; Shah, R.; Schneider, K.; Schneider, K.W.; et al. DICER1 and Associated Conditions: Identification of At-risk Individuals and Recommended Surveillance Strategies. Clin. Cancer Res. 2018, 24, 2251–2261. [Google Scholar] [CrossRef] [Green Version]
- Cotton, E.; Ray, D. DICER1 mutation and pituitary prolactinoma. Endocrinol. Diabetes Metab. Case Rep. 2018, 2018. [Google Scholar] [CrossRef]
- Rosner, M.; Hanneder, M.; Siegel, N.; Valli, A.; Fuchs, C.; Hengstschlager, M. The mTOR pathway and its role in human genetic diseases. Mutat. Res. 2008, 659, 284–292. [Google Scholar] [CrossRef]
- Tigas, S.; Carroll, P.V.; Jones, R.; Bingham, E.; Russell-Jones, D.; Powell, M.; Scobie, I.N. Simultaneous Cushing’s disease and tuberous sclerosis; a potential role for TSC in pituitary ontogeny. Clin. Endocrinol. (Oxf.) 2005, 63, 694–695. [Google Scholar] [CrossRef]
- Nandagopal, R.; Vortmeyer, A.; Oldfield, E.H.; Keil, M.F.; Stratakis, C.A. Cushing’s syndrome due to a pituitary corticotropinoma in a child with tuberous sclerosis: An association or a coincidence? Clin. Endocrinol. (Oxf.) 2007, 67, 639–641. [Google Scholar] [CrossRef]
- Dworakowska, D.; Grossman, A.B. Are neuroendocrine tumours a feature of tuberous sclerosis? A systematic review. Endocr. Relat. Cancer 2009, 16, 45–58. [Google Scholar] [CrossRef] [Green Version]
- Regazzo, D.; Gardiman, M.P.; Theodoropoulou, M.; Scaroni, C.; Occhi, G.; Ceccato, F. Silent gonadotroph pituitary neuroendocrine tumor in a patient with tuberous sclerosis complex: Evaluation of a possible molecular link. Endocrinol. Diabetes Metab. Case Rep. 2018, 2018. [Google Scholar] [CrossRef] [Green Version]
- Cambiaso, P.; Galassi, S.; Palmiero, M.; Mastronuzzi, A.; Del Bufalo, F.; Capolino, R.; Cacchione, A.; Buonuomo, P.S.; Gonfiantini, M.V.; Bartuli, A.; et al. Growth hormone excess in children with neurofibromatosis type-1 and optic glioma. Am. J. Med. Genet. A 2017, 173, 2353–2358. [Google Scholar] [CrossRef]
- Sani, I.; Albanese, A. Endocrine Long-Term Follow-Up of Children with Neurofibromatosis Type 1 and Optic Pathway Glioma. Horm. Res. Paediatr. 2017, 87, 179–188. [Google Scholar] [CrossRef]
- Hozumi, K.; Fukuoka, H.; Odake, Y.; Takeuchi, T.; Uehara, T.; Sato, T.; Inoshita, N.; Yoshida, K.; Matsumoto, R.; Bando, H.; et al. Acromegaly caused by a somatotroph adenoma in patient with neurofibromatosis type 1. Endocr. J. 2019, 66, 853–857. [Google Scholar] [CrossRef] [Green Version]
- Hernandez-Ramirez, L.C.; Gam, R.; Valdes, N.; Lodish, M.B.; Pankratz, N.; Balsalobre, A.; Gauthier, Y.; Faucz, F.R.; Trivellin, G.; Chittiboina, P.; et al. Loss-of-function mutations in the CABLES1 gene are a novel cause of Cushing’s disease. Endocr. Relat. Cancer 2017, 24, 379–392. [Google Scholar] [CrossRef] [Green Version]
- Seemann, N.; Kuhn, D.; Wrocklage, C.; Keyvani, K.; Hackl, W.; Buchfelder, M.; Fahlbusch, R.; Paulus, W. CDKN2A/p16 inactivation is related to pituitary adenoma type and size. J. Pathol. 2001, 193, 491–497. [Google Scholar] [CrossRef]
- Kirsch, M.; Morz, M.; Pinzer, T.; Schackert, H.K.; Schackert, G. Frequent loss of the CDKN2C (p18INK4c) gene product in pituitary adenomas. Genes Chromosomes Cancer 2009, 48, 143–154. [Google Scholar] [CrossRef]
- Bellodi, C.; Krasnykh, O.; Haynes, N.; Theodoropoulou, M.; Peng, G.; Montanaro, L.; Ruggero, D. Loss of function of the tumor suppressor DKC1 perturbs p27 translation control and contributes to pituitary tumorigenesis. Cancer Res. 2010, 70, 6026–6035. [Google Scholar] [CrossRef] [Green Version]
- Brioude, F.; Nicolas, C.; Marey, I.; Gaillard, S.; Bernier, M.; Das Neves, C.; Le Bouc, Y.; Touraine, P.; Netchine, I. Hypercortisolism due to a Pituitary Adenoma Associated with Beckwith-Wiedemann Syndrome. Horm. Res. Paediatr. 2016, 86, 206–211. [Google Scholar] [CrossRef]
- Marques, P.; Spencer, R.; Morrison, P.J.; Carr, I.M.; Dang, M.N.; Bonthron, D.T.; Hunter, S.; Korbonits, M. Cantu syndrome with coexisting familial pituitary adenoma. Endocrine 2018, 59, 677–684. [Google Scholar] [CrossRef] [Green Version]
- Syro, L.V.; Sundsbak, J.L.; Scheithauer, B.W.; Toledo, R.A.; Camargo, M.; Heyer, C.M.; Sekiya, T.; Uribe, H.; Escobar, J.I.; Vasquez, M.; et al. Somatotroph pituitary adenoma with acromegaly and autosomal dominant polycystic kidney disease: SSTR5 polymorphism and PKD1 mutation. Pituitary 2012, 15, 342–349. [Google Scholar] [CrossRef] [Green Version]
- De Menis, E.; Roncaroli, F.; Calvari, V.; Chiarini, V.; Pauletto, P.; Camerino, G.; Cremonini, N. Corticotroph adenoma of the pituitary in a patient with X-linked adrenal hypoplasia congenita due to a novel mutation of the DAX-1 gene. Eur. J. Endocrinol. 2005, 153, 211–215. [Google Scholar] [CrossRef]
- Reincke, M.; Sbiera, S.; Hayakawa, A.; Theodoropoulou, M.; Osswald, A.; Beuschlein, F.; Meitinger, T.; Mizuno-Yamasaki, E.; Kawaguchi, K.; Saeki, Y.; et al. Mutations in the deubiquitinase gene USP8 cause Cushing’s disease. Nat. Genet. 2015, 47, 31–38. [Google Scholar] [CrossRef]
- Ma, Z.Y.; Song, Z.J.; Chen, J.H.; Wang, Y.F.; Li, S.Q.; Zhou, L.F.; Mao, Y.; Li, Y.M.; Hu, R.G.; Zhang, Z.Y.; et al. Recurrent gain-of-function USP8 mutations in Cushing’s disease. Cell Res. 2015, 25, 306–317. [Google Scholar] [CrossRef]
- Perez-Rivas, L.G.; Theodoropoulou, M.; Ferrau, F.; Nusser, C.; Kawaguchi, K.; Stratakis, C.A.; Faucz, F.R.; Wildemberg, L.E.; Assie, G.; Beschorner, R.; et al. The Gene of the Ubiquitin-Specific Protease 8 Is Frequently Mutated in Adenomas Causing Cushing’s Disease. J. Clin. Endocrinol. Metab. 2015, 100, E997–E1004. [Google Scholar] [CrossRef]
- Faucz, F.R.; Tirosh, A.; Tatsi, C.; Berthon, A.; Hernandez-Ramirez, L.C.; Settas, N.; Angelousi, A.; Correa, R.; Papadakis, G.Z.; Chittiboina, P.; et al. Somatic USP8 Gene Mutations Are a Common Cause of Pediatric Cushing Disease. J. Clin. Endocrinol. Metab. 2017, 102, 2836–2843. [Google Scholar] [CrossRef]
- Ballmann, C.; Thiel, A.; Korah, H.E.; Reis, A.C.; Saeger, W.; Stepanow, S.; Kohrer, K.; Reifenberger, G.; Knobbe-Thomsen, C.B.; Knappe, U.J.; et al. USP8 Mutations in Pituitary Cushing Adenomas-Targeted Analysis by Next-Generation Sequencing. J. Endocr. Soc. 2018, 2, 266–278. [Google Scholar] [CrossRef] [Green Version]
- Losa, M.; Mortini, P.; Pagnano, A.; Detomas, M.; Cassarino, M.F.; Pecori Giraldi, F. Clinical characteristics and surgical outcome in USP8-mutated human adrenocorticotropic hormone-secreting pituitary adenomas. Endocrine 2019, 63, 240–246. [Google Scholar] [CrossRef]
- Albani, A.; Perez-Rivas, L.G.; Dimopoulou, C.; Zopp, S.; Colon-Bolea, P.; Roeber, S.; Honegger, J.; Flitsch, J.; Rachinger, W.; Buchfelder, M.; et al. The USP8 mutational status may predict long-term remission in patients with Cushing’s disease. Clin. Endocrinol. (Oxf.) 2018, 89, 454–458. [Google Scholar] [CrossRef]
- Cohen, M.; Persky, R.; Stegemann, R.; Hernandez-Ramirez, L.C.; Zeltser, D.; Lodish, M.B.; Chen, A.; Keil, M.F.; Tatsi, C.; Faucz, F.; et al. Germline USP8 mutation associated with pediatric Cushing disease and other clinical features: A new syndrome. J. Clin. Endocrinol. Metab. 2019, 104, 4676–4682. [Google Scholar] [CrossRef]
- Chen, J.; Jian, X.; Deng, S.; Ma, Z.; Shou, X.; Shen, Y.; Zhang, Q.; Song, Z.; Li, Z.; Peng, H.; et al. Identification of recurrent USP48 and BRAF mutations in Cushing’s disease. Nat. Commun. 2018, 9, 3171. [Google Scholar] [CrossRef] [Green Version]
- Ronchi, C.L.; Peverelli, E.; Herterich, S.; Weigand, I.; Mantovani, G.; Schwarzmayr, T.; Sbiera, S.; Allolio, B.; Honegger, J.; Appenzeller, S.; et al. Landscape of somatic mutations in sporadic GH-secreting pituitary adenomas. Eur. J. Endocrinol. 2016, 174, 363–372. [Google Scholar] [CrossRef] [Green Version]
- Freda, P.U.; Chung, W.K.; Matsuoka, N.; Walsh, J.E.; Kanibir, M.N.; Kleinman, G.; Wang, Y.; Bruce, J.N.; Post, K.D. Analysis of GNAS mutations in 60 growth hormone secreting pituitary tumors: Correlation with clinical and pathological characteristics and surgical outcome based on highly sensitive GH and IGF-I criteria for remission. Pituitary 2007, 10, 275–282. [Google Scholar] [CrossRef]
- Hayward, B.E.; Barlier, A.; Korbonits, M.; Grossman, A.B.; Jacquet, P.; Enjalbert, A.; Bonthron, D.T. Imprinting of the Gsα gene GNAS1 in the pathogenesis of acromegaly. J. Clin. Investig. 2001, 107, R31–R36. [Google Scholar] [CrossRef] [Green Version]
- Riminucci, M.; Collins, M.T.; Lala, R.; Corsi, A.; Matarazzo, P.; Gehron Robey, P.; Bianco, P. An R201H activating mutation of the GNAS1 (Gsalpha) gene in a corticotroph pituitary adenoma. Mol. Pathol. 2002, 55, 58–60. [Google Scholar] [CrossRef]
- Williamson, E.A.; Ince, P.G.; Harrison, D.; Kendall-Taylor, P.; Harris, P.E. G-protein mutations in human pituitary adrenocorticotrophic hormone-secreting adenomas. Eur. J. Clin. Investig. 1995, 25, 128–131. [Google Scholar] [CrossRef]
- Manning, B.D.; Cantley, L.C. AKT/PKB signaling: Navigating downstream. Cell 2007, 129, 1261–1274. [Google Scholar] [CrossRef] [Green Version]
- Karakas, B.; Bachman, K.E.; Park, B.H. Mutation of the PIK3CA oncogene in human cancers. Br. J. Cancer 2006, 94, 455–459. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.; Jiang, X.; Shen, Y.; Li, M.; Ma, H.; Xing, M.; Lu, Y. Frequent mutations and amplifications of the PIK3CA gene in pituitary tumors. Endocr. Relat. Cancer 2009, 16, 301–310. [Google Scholar] [CrossRef] [Green Version]
- Murat, C.B.; Braga, P.B.; Fortes, M.A.; Bronstein, M.D.; Correa-Giannella, M.L.; Giorgi, R.R. Mutation and genomic amplification of the PIK3CA proto-oncogene in pituitary adenomas. Braz. J. Med. Biol. Res. 2012, 45, 851–855. [Google Scholar] [CrossRef] [Green Version]
- Raverot, G.; Burman, P.; McCormack, A.; Heaney, A.; Petersenn, S.; Popovic, V.; Trouillas, J.; Dekkers, O.M.; European Society of Endocrinology. European Society of Endocrinology Clinical Practice Guidelines for the management of aggressive pituitary tumours and carcinomas. Eur. J. Endocrinol. 2018, 178, G1–G24. [Google Scholar] [CrossRef]
- Levy, A.; Hall, L.; Yeudall, W.A.; Lightman, S.L. P53 gene mutations in pituitary adenomas: Rare events. Clin. Endocrinol. (Oxf.) 1994, 41, 809–814. [Google Scholar] [CrossRef]
- Herman, V.; Drazin, N.Z.; Gonsky, R.; Melmed, S. Molecular screening of pituitary adenomas for gene mutations and rearrangements. J. Clin. Endocrinol. Metab. 1993, 77, 50–55. [Google Scholar]
- Kawashima, S.T.; Usui, T.; Sano, T.; Iogawa, H.; Hagiwara, H.; Tamanaha, T.; Tagami, T.; Naruse, M.; Hojo, M.; Takahashi, J.A.; et al. P53 gene mutation in an atypical corticotroph adenoma with Cushing’s disease. Clin. Endocrinol. (Oxf.) 2009, 70, 656–657. [Google Scholar] [CrossRef]
- Guo, F.; Wang, G.; Wang, F.; Xu, D.; Liu, X. Identification of Novel Genes Involved in the Pathogenesis of an ACTH-Secreting Pituitary Carcinoma: A Case Report and Literature Review. Front. Oncol. 2018, 8, 510. [Google Scholar] [CrossRef]
- Tanizaki, Y.; Jin, L.; Scheithauer, B.W.; Kovacs, K.; Roncaroli, F.; Lloyd, R.V. P53 gene mutations in pituitary carcinomas. Endocr. Pathol. 2007, 18, 217–222. [Google Scholar] [CrossRef]
- Szymas, J.; Schluens, K.; Liebert, W.; Petersen, I. Genomic instability in pituitary adenomas. Pituitary 2002, 5, 211–219. [Google Scholar] [CrossRef]
- Pack, S.D.; Qin, L.X.; Pak, E.; Wang, Y.; Ault, D.O.; Mannan, P.; Jaikumar, S.; Stratakis, C.A.; Oldfield, E.H.; Zhuang, Z.; et al. Common genetic changes in hereditary and sporadic pituitary adenomas detected by comparative genomic hybridization. Genes Chromosomes Cancer 2005, 43, 72–82. [Google Scholar] [CrossRef]
- Bi, W.L.; Greenwald, N.F.; Ramkissoon, S.H.; Abedalthagafi, M.; Coy, S.M.; Ligon, K.L.; Mei, Y.; MacConaill, L.; Ducar, M.; Min, L.; et al. Clinical Identification of Oncogenic Drivers and Copy-Number Alterations in Pituitary Tumors. Endocrinology 2017, 158, 2284–2291. [Google Scholar] [CrossRef]
- Bi, W.L.; Horowitz, P.; Greenwald, N.F.; Abedalthagafi, M.; Agarwalla, P.K.; Gibson, W.J.; Mei, Y.; Schumacher, S.E.; Ben-David, U.; Chevalier, A.; et al. Landscape of Genomic Alterations in Pituitary Adenomas. Clin. Cancer Res. 2017, 23, 1841–1851. [Google Scholar] [CrossRef] [Green Version]
- Song, Z.J.; Reitman, Z.J.; Ma, Z.Y.; Chen, J.H.; Zhang, Q.L.; Shou, X.F.; Huang, C.X.; Wang, Y.F.; Li, S.Q.; Mao, Y.; et al. The genome-wide mutational landscape of pituitary adenomas. Cell Res. 2016, 26, 1255–1259. [Google Scholar] [CrossRef] [Green Version]
- Hage, M.; Viengchareun, S.; Brunet, E.; Villa, C.; Pineau, D.; Bouligand, J.; Teglas, J.P.; Adam, C.; Parker, F.; Lombes, M.; et al. Genomic Alterations and Complex Subclonal Architecture in Sporadic GH-Secreting Pituitary Adenomas. J. Clin. Endocrinol. Metab. 2018, 103, 1929–1939. [Google Scholar] [CrossRef]
- Tatsi, C.; Pankratz, N.; Lane, J.; Faucz, F.R.; Hernandez-Ramirez, L.C.; Keil, M.; Trivellin, G.; Chittiboina, P.; Mills, J.L.; Stratakis, C.A.; et al. Large Genomic Aberrations in Corticotropinomas Are Associated With Greater Aggressiveness. J. Clin. Endocrinol. Metab. 2019, 104, 1792–1801. [Google Scholar] [CrossRef] [Green Version]
- Duong, C.V.; Emes, R.D.; Wessely, F.; Yacqub-Usman, K.; Clayton, R.N.; Farrell, W.E. Quantitative, genome-wide analysis of the DNA methylome in sporadic pituitary adenomas. Endocr. Relat. Cancer 2012, 19, 805–816. [Google Scholar] [CrossRef] [Green Version]
- Kober, P.; Boresowicz, J.; Rusetska, N.; Maksymowicz, M.; Goryca, K.; Kunicki, J.; Bonicki, W.; Siedlecki, J.A.; Bujko, M. DNA methylation profiling in nonfunctioning pituitary adenomas. Mol. Cell Endocrinol. 2018, 473, 194–204. [Google Scholar] [CrossRef]
- Garcia-Martinez, A.; Sottile, J.; Sanchez-Tejada, L.; Fajardo, C.; Camara, R.; Lamas, C.; Barbera, V.M.; Pico, A. DNA Methylation of Tumor Suppressor Genes in Pituitary Neuroendocrine Tumors. J. Clin. Endocrinol. Metab. 2019, 104, 1272–1282. [Google Scholar] [CrossRef]
- Gu, Y.; Zhou, X.; Hu, F.; Yu, Y.; Xie, T.; Huang, Y.; Zhao, X.; Zhang, X. Differential DNA methylome profiling of nonfunctioning pituitary adenomas suggesting tumour invasion is correlated with cell adhesion. J. Neurooncol. 2016, 129, 23–31. [Google Scholar] [CrossRef]
- Yoshino, A.; Katayama, Y.; Ogino, A.; Watanabe, T.; Yachi, K.; Ohta, T.; Komine, C.; Yokoyama, T.; Fukushima, T. Promoter hypermethylation profile of cell cycle regulator genes in pituitary adenomas. J. Neurooncol. 2007, 83, 153–162. [Google Scholar] [CrossRef]
- Ling, C.; Pease, M.; Shi, L.; Punj, V.; Shiroishi, M.S.; Commins, D.; Weisenberger, D.J.; Wang, K.; Zada, G. A pilot genome-scale profiling of DNA methylation in sporadic pituitary macroadenomas: Association with tumor invasion and histopathological subtype. PLoS ONE 2014, 9, e96178. [Google Scholar] [CrossRef]
- Pease, M.; Ling, C.; Mack, W.J.; Wang, K.; Zada, G. The role of epigenetic modification in tumorigenesis and progression of pituitary adenomas: A systematic review of the literature. PLoS ONE 2013, 8, e82619. [Google Scholar] [CrossRef] [Green Version]
- Buslei, R.; Kreutzer, J.; Hofmann, B.; Schmidt, V.; Siebzehnrubl, F.; Hahnen, E.; Eyupoglu, I.Y.; Fahlbusch, R.; Blumcke, I. Abundant hypermethylation of SOCS-1 in clinically silent pituitary adenomas. Acta Neuropathol. 2006, 111, 264–271. [Google Scholar] [CrossRef]
- Vandeva, S.; Jaffrain-Rea, M.L.; Daly, A.F.; Tichomirowa, M.; Zacharieva, S.; Beckers, A. The genetics of pituitary adenomas. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 461–476. [Google Scholar] [CrossRef]
- Zhu, X.; Lee, K.; Asa, S.L.; Ezzat, S. Epigenetic silencing through DNA and histone methylation of fibroblast growth factor receptor 2 in neoplastic pituitary cells. Am. J. Pathol. 2007, 170, 1618–1628. [Google Scholar] [CrossRef] [Green Version]
- Zhu, X.; Mao, X.; Hurren, R.; Schimmer, A.D.; Ezzat, S.; Asa, S.L. Deoxyribonucleic acid methyltransferase 3B promotes epigenetic silencing through histone 3 chromatin modifications in pituitary cells. J. Clin. Endocrinol. Metab. 2008, 93, 3610–3617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbass, S.A.; Asa, S.L.; Ezzat, S. Altered expression of fibroblast growth factor receptors in human pituitary adenomas. J. Clin. Endocrinol. Metab. 1997, 82, 1160–1166. [Google Scholar] [CrossRef] [PubMed]
- Ezzat, S.; Zhu, X.; Loeper, S.; Fischer, S.; Asa, S.L. Tumor-derived Ikaros 6 acetylates the Bcl-XL promoter to up-regulate a survival signal in pituitary cells. Mol. Endocrinol. 2006, 20, 2976–2986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ezzat, S. Epigenetic control in pituitary tumors. Endocr. J. 2008, 55, 951–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karp, X.; Ambros, V. Developmental biology. Encountering microRNAs in cell fate signaling. Science 2005, 310, 1288–1289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, T.; Yang, Z.; Gao, H. Advancements in the study of miRNA regulation during the cell cycle in human pituitary adenomas. J. Neurooncol. 2017, 134, 253–258. [Google Scholar] [CrossRef]
- D’Angelo, D.; Palmieri, D.; Mussnich, P.; Roche, M.; Wierinckx, A.; Raverot, G.; Fedele, M.; Croce, C.M.; Trouillas, J.; Fusco, A. Altered microRNA expression profile in human pituitary GH adenomas: Down-regulation of miRNA targeting HMGA1, HMGA2, and E2F1. J. Clin. Endocrinol. Metab. 2012, 97, E1128–E1138. [Google Scholar] [CrossRef]
- Nemeth, K.; Darvasi, O.; Liko, I.; Szucs, N.; Czirjak, S.; Reiniger, L.; Szabo, B.; Krokker, L.; Pallinger, E.; Igaz, P.; et al. Comprehensive analysis of circulating microRNAs in plasma of patients with pituitary adenomas. J. Clin. Endocrinol. Metab. 2019. [Google Scholar] [CrossRef]
- Cui, M.; Zhang, M.; Liu, H.F.; Wang, J.P. Effects of microRNA-21 targeting PITX2 on proliferation and apoptosis of pituitary tumor cells. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 2995–3004. [Google Scholar]
- Roche, M.; Wierinckx, A.; Croze, S.; Rey, C.; Legras-Lachuer, C.; Morel, A.P.; Fusco, A.; Raverot, G.; Trouillas, J.; Lachuer, J. Deregulation of miR-183 and KIAA0101 in Aggressive and Malignant Pituitary Tumors. Front. Med. (Lausanne) 2015, 2, 54. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Types and frequency of PAs based on their functional status in adult and pediatric patients.
Figure 1.
Types and frequency of PAs based on their functional status in adult and pediatric patients.


{kind=link}
Table 1.
Familial syndromes associated with pituitary adenomas (PAs). GH: growth hormone, PRL: prolactin, ACTH: Corticotropin hormone.
Table 1.
Familial syndromes associated with pituitary adenomas (PAs). GH: growth hormone, PRL: prolactin, ACTH: Corticotropin hormone.
| Familial Syndrome | Gene | Chromosomal Locus | Suggested Mechanism of Pituitary Tumorigenesis | Most Common Functional Status | Frequency of PAs |
|---|---|---|---|---|---|
| Familial Isolated Pituitary Adenomas | AIP (15–30% of cases) | 11q13.2 | Interaction in cAMP synthesis | GH | 100% |
| Multiple Endocrine Neoplasia type 1 | MEN1 | 11q13.1 | Tumor suppressor; Involved in cell proliferation, genome stability and gene transcription | PRL or non-functioning | 40% |
| Multiple Endocrine Neoplasia type 2A/2B | RET | 10q11.21 | Proto-oncogene; Transmembrane receptor with tyrosine kinase activity | Rare | Rare |
| Multiple Endocrine Neoplasia type 4 | CDKN1B | 12p13.1 | Tumor suppressor; Cell cycle regulation | Rare | Rare |
| McCune-Albright | GNAS | 20q13.32 | cAMP-regulating protein Gsa; activation leads to increased cAMP levels and activation of protein kinase A (PKA) | GH excess | Up to 20% |
| Carney complex | PRKAR1A | 17q24.2 | Alpha regulatory subunit of PKA; inactivation of PRKAR1A leads to dissociation of the regulatory from the catalytic subunit and aberrant PKA activity | GH | 15% |
| DICER1 | DICER1 | 14q32.13 | RNA processing endoribonuclease that cleaves double stranded RNA into small interfering RNAs and mature miRNAs | ACTH | Rare |
| 3 P association | SDHx, VHL, MEN1, RET and MAX | 5p15.33 (SDHA) 1p36.13 (SDHB) 11q23.1 (SDHD) 11q12.2 (SDHAF2) 3p25.3 (VHL) 11q13.1 (MEN1) 11q13.1 (RET) 14q23.3 (MAX) | Several functions depending on identified gene. SDHx: participate in the mitochondrial complex II, energy production through the Krebs cycle and respiratory chain through electron transfer. VHL: tumor suppressor; oxygen sensing and interaction with hypoxia-inducible factors. MAX: Myc associated factor X; involved in cell proliferation, differentiation and apoptosis | PRL or GH | 100% |
| Tuberous sclerosis | TSC1, TSC2 | 9q34.13 (TSC1) 16p13.3 (TSC2) | Mediate PI3K/Akt activation and lead to inhibition of mTOR pathway | ACTH | Rare |
| X-Linked Acrogigantism | GPR101 | Xq26.3 | G-protein-coupled receptor; defects lead to constitutive activation of the cAMP-PKA pathway | GH | 85% |
| Neurofibromatosis type 1 | NF1 | 17q11.2 | Ras-GTPase-activating protein involved in Ras-dependent pathways (Ras/Raf/MEK and Ras/PI3K/TSC/mTOR) | GH | Rare |
Table 2.
Clinical presentation of patients with familial syndromes involving PAs. MEN: Multiple Endocrine Neoplasia, GH: growth hormone, ACTH: Corticotropin hormone.
Table 2.
Clinical presentation of patients with familial syndromes involving PAs. MEN: Multiple Endocrine Neoplasia, GH: growth hormone, ACTH: Corticotropin hormone.
| Familial Syndrome | Gene | Presentation |
|---|---|---|
| Familial Isolated Pituitary Adenomas | AIP (15–30% of cases) | Presence of at least two family members with pituitary adenomas, either of the same functional status (homologous) or of different (heterologous), without extra-pituitary findings. |
| Multiple Endocrine Neoplasia type 1 | MEN1 | Autosomal dominant syndrome presenting with multiple endocrine neoplasias, including anterior pituitary adenomas, hyperparathyroidism, enteropancreatic tumors, neuroendocrine tumors and others. |
| Multiple Endocrine Neoplasia type 2A/2B | RET | Autosomal dominant syndromes presenting with medullary thyroid carcinoma (MEN2A/B), pheochromocytoma (MEN2A/B), hyperparathyroidism (MEN2A), mucosal ganglioneuromas (MEN2B), and rare occurrence of anterior pituitary adenomas. |
| Multiple Endocrine Neoplasia type 4 | CDKN1B | Autosomal dominant MEN1-like syndrome, without genetic confirmation of MEN1 gene defect. |
| McCune-Albright | GNAS | Classic triad of polyostotic fibrous dysplasia, café-au-lait macules, and precocious puberty. Additional features include GH excess, hyperthyroidism, neonatal Cushing syndrome, and hypophosphatemia. |
| Carney complex | PRKAR1A | Autosomal dominant syndrome presenting with the constellation of cardiac and skin myxomas, spotty skin pigmentation, endocrine overactivity, including anterior pituitary adenomas and ACTH-independent Cushing syndrome, breast and testicular tumors, thyroid nodules, psammomatous melanotic schwannomas, and osteochondromyxomas. |
| DICER1 | DICER1 | Autosomal dominant syndrome presenting with pleuropulmonary blastomas, cystic nephromas, Sertoli-Leydig cell tumors, multinodular goiter, pituitary blastomas and other tumors. |
| 3 P association | SDHx, VHL, MEN1, RET and MAX | Combination of pituitary adenomas, pheochromocytomas and/or paragangliomas. |
| Tuberous sclerosis | TSC1, TSC2 | Autosomal dominant syndrome characterized by hamartomas, epilepsy, mental retardation, and rare occurrence of pituitary neuroendocrine tumors |
| X-Linked Acrogigantism | GPR101 | GH excess with onset of symptoms in most cases younger than 2 years of age. |
| Neurofibromatosis type 1 | NF1 | Autosomal dominant syndrome presenting with neurofibromas, skin findings (café-au-lait macules and freckling), Lisch (iris) nodules, optic pathway gliomas with consequent precocious puberty and GH excess, and other rare tumors. |
Table 3.
Commonest somatic genetic defects associated with PAs. GH: growth hormone, PKA: protein kinase A, EGFR: Epidermal growth factor receptor, ACTH: Corticotropin hormone.
Table 3.
Commonest somatic genetic defects associated with PAs. GH: growth hormone, PKA: protein kinase A, EGFR: Epidermal growth factor receptor, ACTH: Corticotropin hormone.
| Gene | Chromosomal Locus | Suggested Mechanism of Pituitary Tumorigenesis | Most Common Functional Status |
|---|---|---|---|
| GNAS | 20q13.32 | cAMP-regulating protein Gsa; activation leads to increased cAMP levels and activation of protein kinase A (PKA) | GH |
| USP8 | 15q21.2 | Involved in deubiquitination of EGFR; gain of functions mutations cause increase EGFR, and POMC expression | ACTH |
| AIP | 11q13.2 | Interaction in cAMP synthesis | GH |
| USP48 | 1p36.12 | Deubiquitination; activation of MAPK and increased POMC expression | ACTH |
| BRAF | 7q34 | Proto-oncogene with tyrosine kinase activity; activation of MAPK and increased POMC expression | ACTH |
| PIK3CA | 3q26.32 | Involved in PI3K/AKT pathway which regulates several cellular functions, including cell survival, growth, proliferation and metabolism | Non-functioning |
| TP53 | 17p13.1 | Tumor suppressor; involved in cell cycle, apoptosis and genomic stability | ACTH(also associated with atypical adenomas and pituitary carcinomas) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Tatsi, C.; Stratakis, C.A. The Genetics of Pituitary Adenomas. J. Clin. Med. 2020, 9, 30. https://doi.org/10.3390/jcm9010030
AMA Style
Tatsi C, Stratakis CA. The Genetics of Pituitary Adenomas. Journal of Clinical Medicine. 2020; 9(1):30. https://doi.org/10.3390/jcm9010030
Chicago/Turabian StyleTatsi, Christina, and Constantine A. Stratakis. 2020. "The Genetics of Pituitary Adenomas" Journal of Clinical Medicine 9, no. 1: 30. https://doi.org/10.3390/jcm9010030
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.