Relationship between Morbidity and Health Behavior in Chronic Diseases


Abstract
:1. Introduction
2. Experimental Section
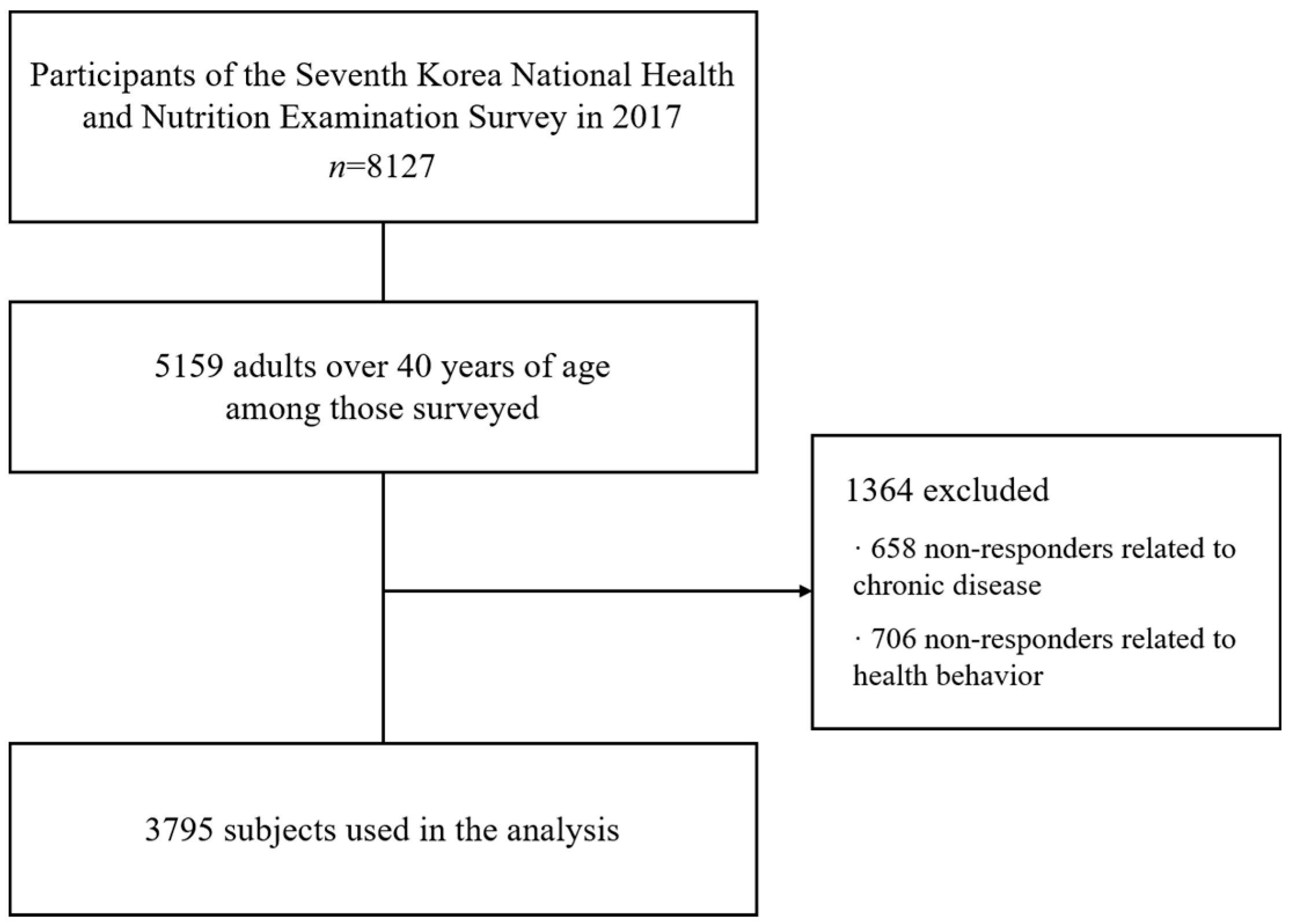
2.1. Data Source and Research Participants
2.2. Description of Variables
2.3. Statistical Analysis
3. Results
3.1. Participants’ Demographic Characteristics
3.2. Relationship between Demographic Characteristics and Chronic Diseases
3.3. Relationship between Health Behavior and Chronic Diseases
3.4. Factors Affecting Chronic Diseases
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Janowski, K.; Kurpas, D.; Kusz, J.; Mroczek, B.; Jedynak, T. Health-related behavior, profile of health locus of control and acceptance of illness in patients suffering from chronic somatic diseases. PLoS ONE 2013, 8, e63920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mullen, P.D.; Hersey, J.C.; Iverson, D.C. Health behavior models compared. Soc. Sci. Med. 1987, 24, 973–981. [Google Scholar] [CrossRef]
- Berrigan, D.; Dodd, K.; Troiano, R.P.; Krebs-Smith, S.M.; Barbash, R.B. Patterns of health behavior in U.S. adults. Prev. Med. 2003, 36, 615–623. [Google Scholar] [CrossRef]
- McGinnis, J.M.; Williams-Russo, P.; Knickman, J.R. The case for more active policy attention to health promotion. Health Aff. 2002, 21, 78–93. [Google Scholar] [CrossRef]
- Jarvandi, S.; Yan, Y.; Schootman, M. Income disparity and risk of death: The importance of health behaviors and other mediating factors. PLoS ONE 2012, 7, e49929. [Google Scholar] [CrossRef] [Green Version]
- Nettle, D. Why are there social gradients in preventative health behavior? A perspective from behavioral ecology. PLoS ONE 2010, 5, e13371. [Google Scholar] [CrossRef] [Green Version]
- Paudel, S.; Owen, A.J.; Owusu-Addo, E.; Smith, B.J. Physical activity participation and the risk of chronic diseases among South Asian adults: A systematic review and meta-analysis. Sci. Rep. 2019, 9, 9771. [Google Scholar] [CrossRef]
- Strong, K.; Mathers, C.; Leeder, S.; Beaglehole, R. Preventing chronic diseases: How many lives can we save? Lancet 2005, 366, 1578–1582. [Google Scholar] [CrossRef]
- Yach, D.; Hawkes, C.; Gould, C.L.; Hofman, K.J. The Global Burden of Chronic DiseasesOvercoming Impediments to Prevention and Control. JAMA 2004, 291, 2616–2622. [Google Scholar] [CrossRef]
- Bae, E.-J.; Park, N.-J.; Sohn, H.-S.; Kim, Y.-H. Handgrip strength and all-cause mortality in middle-aged and older Koreans. Int. J. Environ. Res. Public Health 2019, 16, 740. [Google Scholar] [CrossRef] [Green Version]
- Gansevoort, R.T.; Correa-Rotter, R.; Hemmelgarn, B.R.; Jafar, T.H.; Heerspink, H.J.L.; Mann, J.F.; Matsushita, K.; Wen, C.P. Chronic kidney disease and cardiovascular risk: Epidemiology, mechanisms, and prevention. Lancet 2013, 382, 339–352. [Google Scholar] [CrossRef]
- Halpin, H.A.; Morales-Suárez-Varela, M.M.; Martin-Moreno, J.M. Chronic Disease Prevention and the New Public Health. Public Health Rev. 2010, 32, 120–154. [Google Scholar] [CrossRef] [Green Version]
- Sturm, R. The effects of obesity, smoking, and drinking on medical problems and costs. Health Aff. 2002, 21, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Strine, T.W.; Chapman, D.P.; Balluz, L.S.; Moriarty, D.G.; Mokdad, A.H. The associations between life satisfaction and health-related quality of life, chronic illness, and health behaviors among US community-dwelling adults. J. Community Health 2008, 33, 40–50. [Google Scholar] [CrossRef]
- Harris, M. The role of primary health care in preventing the onset of chronic disease, with a particular focus on the lifestyle risk factors of obesity, tobacco and alcohol. Canberra Natl. Prev. Health Taskforce 2008, 1, 21. [Google Scholar]
- Steyn, K.; Damasceno, A. Lifestyle and related risk factors for chronic diseases. Dis. Mortal. Sub-Sahar. Afr. 2006, 2, 247–265. [Google Scholar]
- Reeves, M.J.; Rafferty, A.P. Healthy lifestyle characteristics among adults in the United States, 2000. Arch. Intern. Med. 2005, 165, 854–857. [Google Scholar] [CrossRef] [Green Version]
- Kang, Y.J.; Kang, M.-Y. Chronic diseases, health behaviors, and demographic characteristics as predictors of ill health retirement: Findings from the Korea Health Panel Survey (2008–2012). PLoS ONE 2016, 11, e0166921. [Google Scholar] [CrossRef]
- Winkleby, M.A.; Cubbin, C. Changing patterns in health behaviors and risk factors related to chronic diseases, 1990–2000. Am. J. Health Promot. 2004, 19, 19–27. [Google Scholar] [CrossRef]
- Speake, D.L.; Cowart, M.E.; Pellet, K. Health perceptions and lifestyles of the elderly. Res. Nurs. Health 1989, 12, 93–100. [Google Scholar] [CrossRef]
- Cho, Y.I.; Lee, S.-Y.D.; Arozullah, A.M.; Crittenden, K.S. Effects of health literacy on health status and health service utilization amongst the elderly. Soc. Sci. Med. 2008, 66, 1809–1816. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.W.; Ko, I.S.; Lee, K.J. Health promotion behaviors and quality of life among community-dwelling elderly in Korea: A cross-sectional survey. Int. J. Nurs. Stud. 2006, 43, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Winkleby, M.A.; Jatulis, D.E.; Frank, E.; Fortmann, S.P. Socioeconomic status and health: How education, income, and occupation contribute to risk factors for cardiovascular disease. Am. J. Public Health 1992, 82, 816–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Innes, H.; McAuley, A.; Alavi, M.; Valerio, H.; Goldberg, D.; Hutchinson, S.J. The contribution of health risk behaviors to excess mortality in American adults with chronic hepatitis C: A population cohort-study. Hepatology 2018, 67, 97–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, J.; Kim, S.; Ke, S.; Cho, B. The Association Chronic Liver Diseases with Health Related Behaviors in South Korea. Korean J. Fam. Med. 2010, 31, 302–307. [Google Scholar] [CrossRef]
- Caspersen, C.J.; Pereira, M.A.; Curran, K.M. Changes in physical activity patterns in the United States, by sex and cross-sectional age. Med. Sci. Sports Exerc. 2000, 32, 1601–1609. [Google Scholar] [CrossRef] [Green Version]
- Chang, O.; Choi, E.-K.; Kim, I.-R.; Nam, S.-J.; Lee, J.E.; Lee, S.K.; Im, Y.-H.; Park, Y.H.; Cho, J. Association between socioeconomic status and altered appearance distress, body image, and quality of life among breast cancer patients. Asian Pac. J. Cancer Prev. 2014, 15, 8607–8612. [Google Scholar] [CrossRef] [Green Version]
- Fine, L.J.; Philogene, G.S.; Gramling, R.; Coups, E.J.; Sinha, S. Prevalence of multiple chronic disease risk factors: 2001 National Health Interview Survey. Am. J. Prev. Med. 2004, 27, 18–24. [Google Scholar] [CrossRef]
- Lee, M.; Yoon, K. Catastrophic Health Expenditures and Its Inequality in Households with Cancer Patients: A Panel Study. Processes 2019, 7, 39. [Google Scholar] [CrossRef] [Green Version]
- McCann, B.A.; Ewing, R. Measuring the Health Effects of Sprawl: A National Analysis of Physical Activity, Obesity and Chronic Disease. Geography 2003. [Google Scholar] [CrossRef]
- Katzmarzyk, P.; Lear, S. Physical activity for obese individuals: A systematic review of effects on chronic disease risk factors. Obes. Rev. 2012, 13, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Mukamal, K.J.; Ding, E.L.; Djoussé, L. Alcohol consumption, physical activity, and chronic disease risk factors: A population-based cross-sectional survey. BMC Public Health 2006, 6, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, E.R.; Shin, A.; Kim, J.; Jee, S.H.; Sung, J. Leisure-time physical activity is associated with a reduced risk for metabolic syndrome. Ann. Epidemiol. 2009, 19, 784–792. [Google Scholar] [CrossRef] [PubMed]
- Choban, P.; Flancbaum, L. Nourishing the obese patient. Clin. Nutr. 2000, 19, 305–311. [Google Scholar] [CrossRef]
- Chan, M.; Lim, Y.; Ernest, A.; Tan, T. Nutritional assessment in an Asian nursing home and its association with mortality. J. Nutr. Health Aging 2010, 14, 23–28. [Google Scholar] [CrossRef]
- Kim, Y.-H.; Kim, S.M.; Han, K.-D.; Jung, J.-H.; Lee, S.-S.; Oh, S.W.; Park, H.S.; Rhee, E.-J.; Lee, W.-Y.; Yoo, S.J. Waist Circumference and All-Cause Mortality Independent of Body Mass Index in Korean Population from the National Health Insurance Health Checkup 2009–2015. J. Clin. Med. 2019, 8, 72. [Google Scholar] [CrossRef] [Green Version]
- Virtanen, M.; Oksanen, T.; Batty, G.D.; Ala-Mursula, L.; Salo, P.; Elovainio, M.; Pentti, J.; Lybäck, K.; Vahtera, J.; Kivimäki, M. Extending employment beyond the pensionable age: A cohort study of the influence of chronic diseases, health risk factors, and working conditions. PLoS ONE 2014, 9, e88695. [Google Scholar] [CrossRef] [Green Version]
- Park, M.; Park, Y.; Kim, S.; Park, S.; Seol, H.; Woo, S.; Cho, S.; Lim, D.-S. Introduction and effectiveness of The Seoul Metabolic Syndrome Management. Public Health Aff. 2017, 1, 25–39. [Google Scholar] [CrossRef] [Green Version]
- Zhao, C.; Wong, L.; Zhu, Q.; Yang, H. Prevalence and correlates of chronic diseases in an elderly population: A community-based survey in Haikou. PLoS ONE 2018, 13, e0199006. [Google Scholar] [CrossRef] [Green Version]
- Cockerham, W.C.; Hamby, B.W.; Oates, G.R. The social determinants of chronic disease. Am. J. Prev. Med. 2017, 52, S5–S12. [Google Scholar] [CrossRef] [Green Version]
- Martínez-García, M.; Salinas-Ortega, M.; Estrada-Arriaga, I.; Hernández-Lemus, E.; García-Herrera, R.; Vallejo, M. A systematic approach to analyze the social determinants of cardiovascular disease. PLoS ONE 2018, 13, e0190960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, L.A.; Tan, A.X.; Coyle, C.E.; Ndumele, C.; Rogan, E.; Canavan, M.; Curry, L.A.; Bradley, E.H. Leveraging the social determinants of health: What works? PLoS ONE 2016, 11, e0160217. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, S.B.; Kalantar-Zadeh, K.; Norris, K.C. Socioeconomic disparities in chronic kidney disease. Adv. Chronic Kidney Dis. 2015, 22, 6–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, B.; Kwon, S. Effect of private health insurance on health care utilization in a universal public insurance system: A case of South Korea. Health Policy 2013, 113, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Yoon, K.; Choi, M. Private health insurance and catastrophic health expenditures of households with cancer patients in South Korea. Eur. J. Cancer Care 2018, 27, e12867. [Google Scholar] [CrossRef]
- Mulcahy, A.W.; Eibner, C.; Finegold, K. Gaining coverage through Medicaid or private insurance increased prescription use and lowered out-of-pocket spending. Health Aff. 2016, 35, 1725–1733. [Google Scholar] [CrossRef] [Green Version]
- Culica, D.; Rohrer, J.; Ward, M.; Hilsenrath, P.; Pomrehn, P. Medical checkups: Who does not get them? Am. J. Public Health 2002, 92, 88–91. [Google Scholar] [CrossRef]
- Liu, Y.; Croft, J.B.; Wheaton, A.G.; Kanny, D.; Cunningham, T.J.; Lu, H.; Onufrak, S.; Malarcher, A.M.; Greenlund, K.J.; Giles, W.H. Clustering of Five Health-Related Behaviors for Chronic Disease Prevention Among Adults, United States, 2013. Prev. Chronic Dis. 2016, 13, E70. [Google Scholar] [CrossRef] [Green Version]
- Campbell, D.J.; Ronksley, P.E.; Manns, B.J.; Tonelli, M.; Sanmartin, C.; Weaver, R.G.; Hennessy, D.; King-Shier, K.; Campbell, T.; Hemmelgarn, B.R. The association of income with health behavior change and disease monitoring among patients with chronic disease. PLoS ONE 2014, 9, e94007. [Google Scholar] [CrossRef] [Green Version]
- Thande, N.K.; Hurstak, E.E.; Sciacca, R.E.; Giardina, E.G.V. Management of obesity: A challenge for medical training and practice. Obesity 2009, 17, 107–113. [Google Scholar] [CrossRef]
- Lee, M.; Yoon, K.; Lee, K.-S. Subjective health status of multimorbidity: Verifying the mediating effects of medical and assistive devices. Int. J. Equity Health 2018, 17, 164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, X.; Cahan, A. Wearable technologies and telehealth in Care Management for Chronic Illness. In Healthcare Information Management Systems; Springer: Cham, Switzerland, 2016; pp. 375–398. [Google Scholar]
- Kang, S.Y. The ICT Technology for Geriatric Diseases Healthcare. In Information Science and Applications (ICISA) 2016; Springer: Singapore, 2016; pp. 1495–1500. [Google Scholar]
- Bodenheimer, T.; Lorig, K.; Holman, H.; Grumbach, K. Patient self-management of chronic disease in primary care. JAMA 2002, 288, 2469–2475. [Google Scholar] [CrossRef] [PubMed]
- Chiauzzi, E.; Rodarte, C.; DasMahapatra, P. Patient-centered activity monitoring in the self-management of chronic health conditions. BMC Med. 2015, 13, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variable | Definition |
|---|---|
| Sex | 0 = Female |
| 1 = Male | |
| Age | 0 = Adult |
| 1 = Senior | |
| Education | 0 = ≤Middle school |
| 1 = ≥Middle school | |
| Income | 0 = <300 |
| 1 = ≥300 | |
| Type of insurance | 0 = National Health Insurance |
| 1 = Assistance | |
| Private insurance | 0 = No |
| 1 = Yes | |
| Chronic disease | 0 = No |
| 1 = Yes | |
| Medical checkup | 0 = No |
| 1 = Yes | |
| Drinking | 0 = Non-drinker |
| 1 = Drinker | |
| Smoking | 0 = Non-smoker |
| 1 = Smoker | |
| Exercise | 0 = No |
| 1 = Yes | |
| Obesity | 0 = Obesity |
| 1 = Normal | |
| Hypercholesterolemia | 0 = No |
| 1 = Yes |
| Characteristic | Type | N | % |
|---|---|---|---|
| Sex | Female | 2126 | 56.0 |
| Male | 1669 | 44.0 | |
| Age | 40–65 | 2544 | 67.0 |
| ≥65 | 1251 | 33.0 | |
| Education | <Middle school | 1526 | 40.2 |
| ≥Middle school | 2269 | 59.8 | |
| Income | <300 | 1688 | 44.5 |
| ≥300 | 2107 | 55.5 | |
| Type of insurance | National health insurance | 3632 | 95.7 |
| Assistance | 163 | 4.3 | |
| Private insurance | Y | 2814 | 74.2 |
| N | 981 | 25.8 | |
| Medical checkup | Y | 857 | 22.6 |
| N | 2938 | 77.4 | |
| Chronic disease | 0 | 2033 | 53.6 |
| 1 | 950 | 25.0 | |
| <2 | 812 | 21.4 |
| Characteristic | Type | Chronic Disease | p-Value | |||
|---|---|---|---|---|---|---|
| N | % | Y | % | |||
| Sex ** | Female | 1171 | 55.1 | 955 | 44.9 | 0.019 |
| Male | 862 | 51.6 | 807 | 48.4 | ||
| Age *** | 40–65 | 1674 | 65.8 | 870 | 34.2 | 0.001 |
| ≥65 | 359 | 28.7 | 892 | 71.3 | ||
| Education *** | <Middle school | 545 | 35.7 | 981 | 64.3 | 0.001 |
| ≥Middle school | 1488 | 65.6 | 781 | 34.4 | ||
| Income *** | <300 | 680 | 40.3 | 1008 | 59.7 | 0.001 |
| ≥300 | 1353 | 64.2 | 754 | 35.8 | ||
| Type of insurance *** | NHI | 1984 | 54.6 | 1648 | 45.4 | 0.001 |
| Assistance | 49 | 30.1 | 114 | 69.9 | ||
| Private insurance *** | Y | 1686 | 59.9 | 1128 | 40.1 | 0.001 |
| N | 347 | 35.4 | 634 | 64.6 | ||
| Characteristic | Type | Chronic Disease | p-Value | |||
|---|---|---|---|---|---|---|
| N | % | Y | % | |||
| Medical checkup | Y | 453 | 52.9 | 404 | 47.1 | 0.331 |
| N | 1580 | 53.8 | 1358 | 46.2 | ||
| Drinking *** | Y | 923 | 49.4 | 944 | 50.6 | 0.001 |
| N | 1110 | 57.6 | 818 | 42.4 | ||
| Smoking * | Y | 1696 | 53.0 | 1503 | 47.0 | 0.062 |
| N | 337 | 56.5 | 259 | 43.5 | ||
| Exercise *** | Y | 904 | 59.9 | 605 | 40.1 | 0.001 |
| N | 1129 | 49.4 | 1157 | 50.6 | ||
| Obesity *** | Y | 1132 | 47.3 | 1263 | 52.7 | 0.001 |
| N | 901 | 64.4 | 499 | 35.6 | ||
| Hypercholesterolemia *** | Y | 291 | 26.1 | 823 | 73.9 | 0.001 |
| N | 1742 | 65.0 | 939 | 35.0 | ||
| Dependent Variable | Independent Variable | Exp(B) | p-Value |
|---|---|---|---|
| Chronic disease | Sex *** | 1.498 | 0.001 |
| Age *** | 3.145 | 0.001 | |
| Education *** | 0.535 | 0.001 | |
| Income ** | 0.773 | 0.004 | |
| Type of insurance ** | 1.727 | 0.008 | |
| Private insurance ** | 0.803 | 0.036 | |
| Medical checkup ** | 0.782 | 0.009 | |
| Drinking | 1.101 | 0.252 | |
| Smoking | 1.061 | 0.606 | |
| Exercise * | 0.861 | 0.060 | |
| Obesity *** | 0.544 | 0.001 | |
| Hypercholesterolemia *** | 5.444 | 0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, M.; Park, S.; Lee, K.-S. Relationship between Morbidity and Health Behavior in Chronic Diseases. J. Clin. Med. 2020, 9, 121. https://doi.org/10.3390/jcm9010121
Lee M, Park S, Lee K-S. Relationship between Morbidity and Health Behavior in Chronic Diseases. Journal of Clinical Medicine. 2020; 9(1):121. https://doi.org/10.3390/jcm9010121
Chicago/Turabian StyleLee, Munjae, Sewon Park, and Kyu-Sung Lee. 2020. "Relationship between Morbidity and Health Behavior in Chronic Diseases" Journal of Clinical Medicine 9, no. 1: 121. https://doi.org/10.3390/jcm9010121