Prevalence of Early Chronic Kidney Disease and Main Associated Factors in Spanish Population: Populational Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
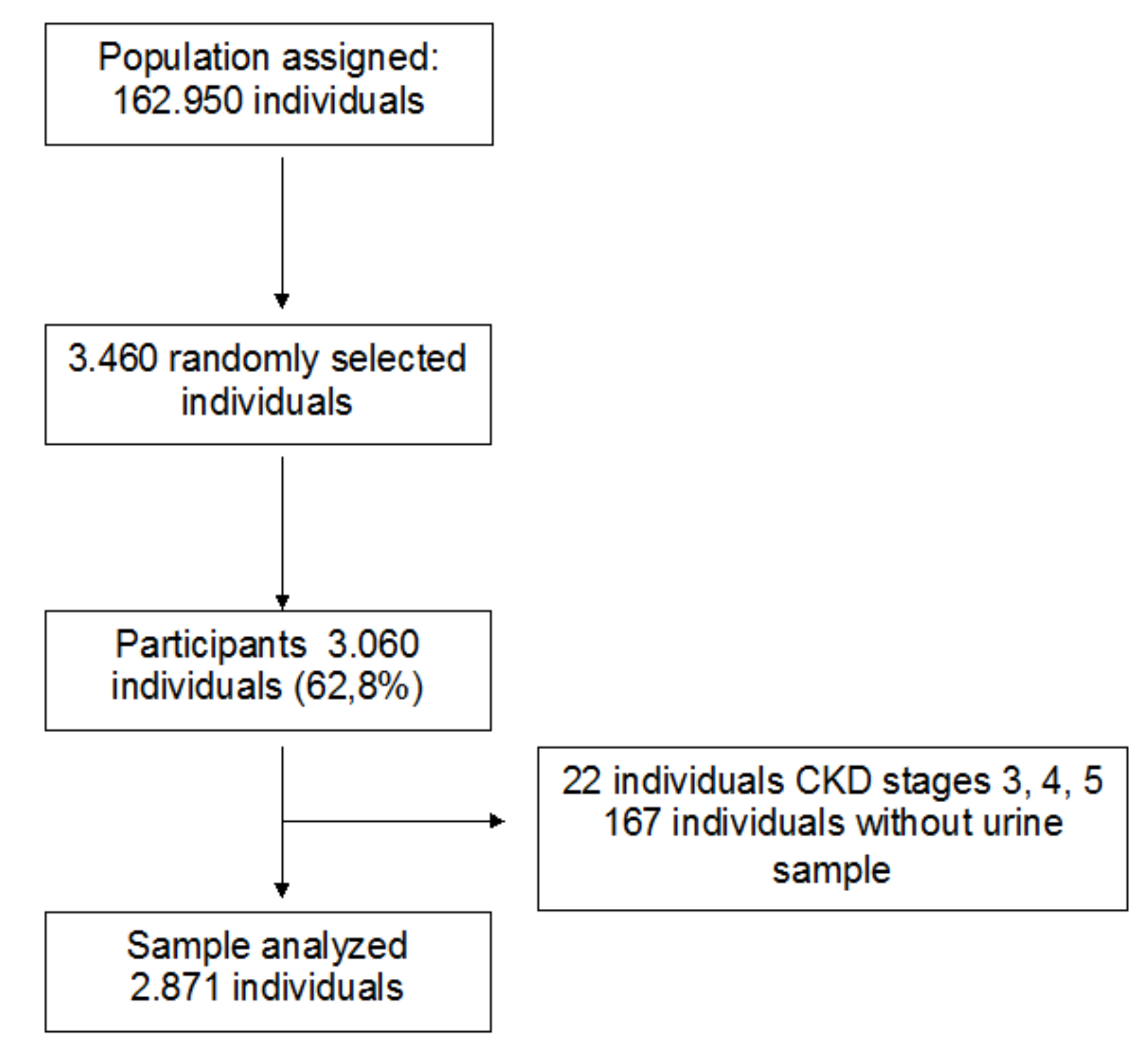
2.1. Study Design and Population
2.2. Study Variables
2.2.1. Sociodemographic Variables: Age, Gender
- Age: Age in years in subjects between 18 and 75 years
- Gender: Males and females
2.2.2. Anamnesis
- Presence of comorbidities. This was determined by review of the clinical history: arterial hypertension (AHT), type 2 diabetes mellitus (DM2), hypercholesterolemia and hypertriglyceridemia.
- Alcohol intake. The consumption of alcohol was recorded as standard drink units (SDU), and intake during the week and the weekends was differentiated. The length of consumption in years was also recorded. One SDU is equivalent to 10 g of alcohol. Consumption per week ≥ 21 SDU in men and ≥ 14 SDU in women was considered to be of risk.
- Tobacco consumption: This included never smokers, ex-smokers (more than 1 years without smoking) and active smokers.
2.3. Physical Examination
2.4. Analytical Determinations.
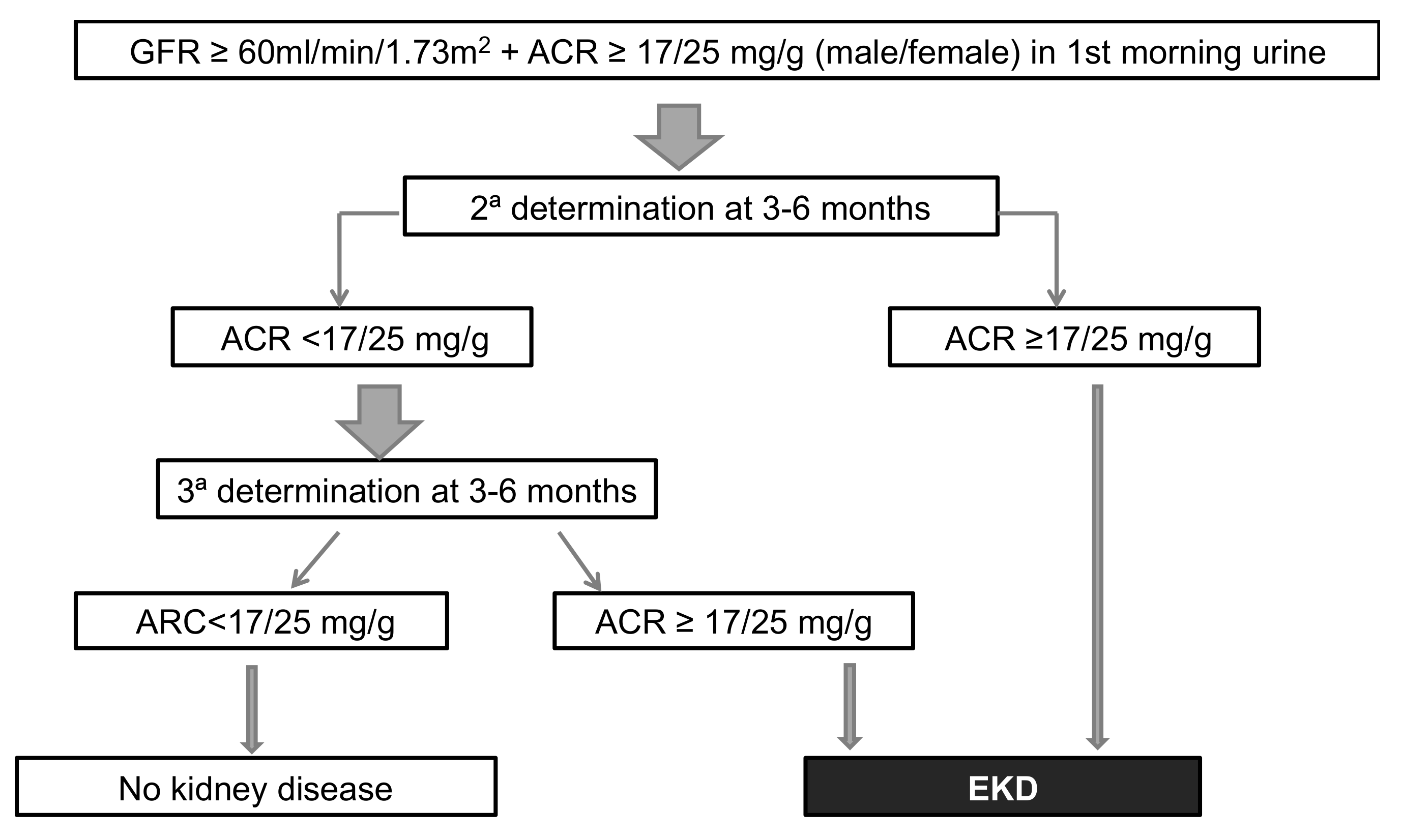
2.5. Diagnosis of EKD
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Sample
3.2. Prevalence of EKD
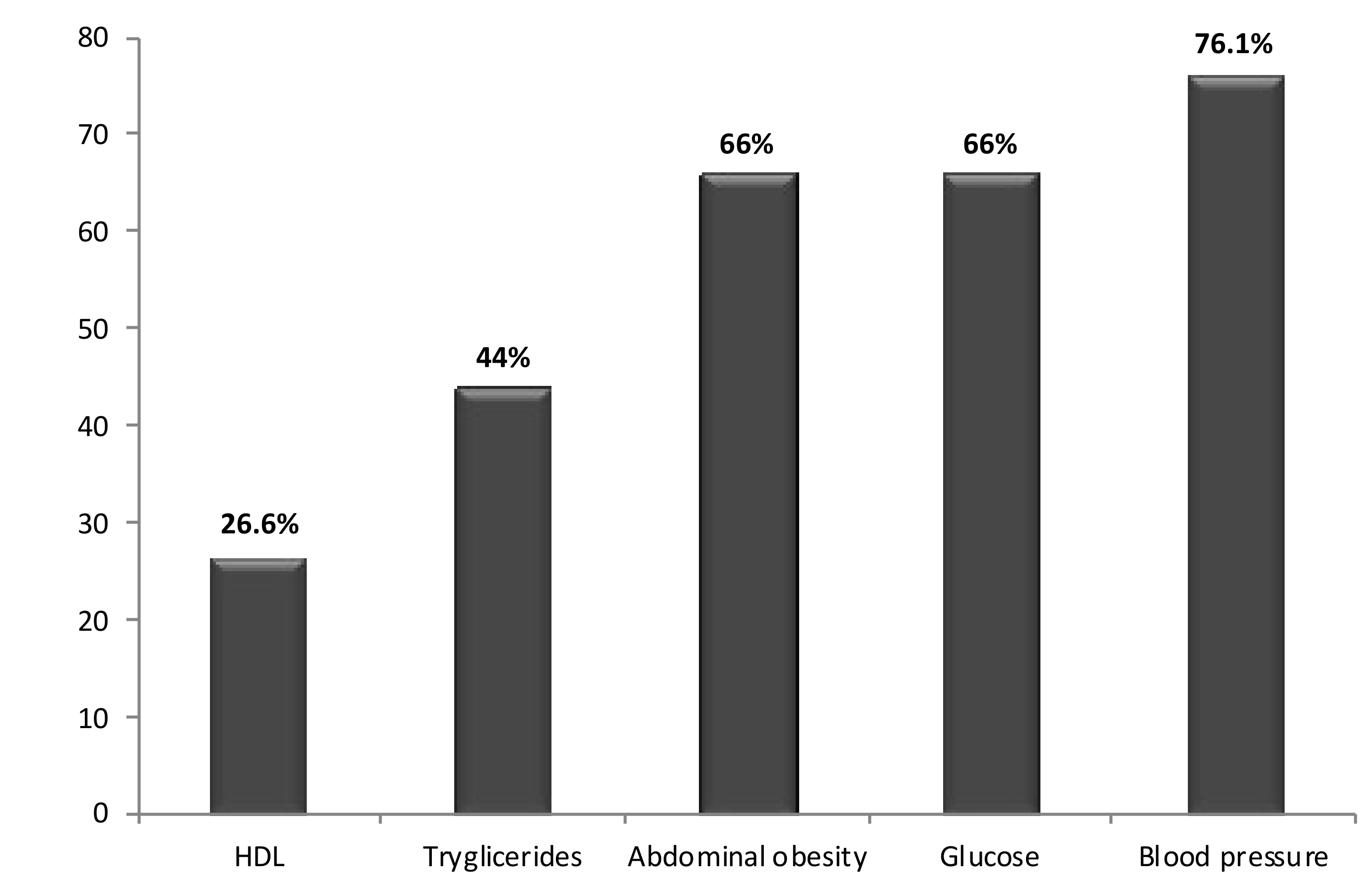
3.3. Principal Associated Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Schoolwerth, A.C.; Engelgau, M.M.; Hostetter, T.H.; Rufo, K.H.; Chianchiano, D.; McClellan, W.M.; Warnock, D.G.; Vinicor, F. Chronic kidney disease: A public health problem that needs a public health action plan. Prev. Chronic. Dis. 2006, 3, A57. [Google Scholar] [PubMed]
- Levey, A.S.; Atkins, R.; Coresh, J.; Cohen, E.P.; Collins, A.J.; Eckardt, K.U.; Nahas, M.E.; Jaber, B.L.; Jadoul, M.; Levin, A.; et al. Chronic kidney disease as a global public health problem: Approaches and initiatives—A position statement from Kidney Disease Improving Global Outcomes. Kidney Int. 2007, 72, 247–259. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Martínez-Castelao, A.; Górriz, J.L.; Bover, J.; Segura-de la Morena, J.; Cebollada, J.; Escalada, J.; Esmatjes, E.; Fácila, L.; Gamarra, J.; Gràcia, S.; et al. Consensus document for the detection and management of chronic kidney disease. Atención Primaria 2014, 46, 501–519. [Google Scholar] [CrossRef] [PubMed]
- Landecho, M.F.; Colina, I.; Huerta, A.; Fortuño, A.; Zalba, G.; Beloqui, O. Connection between the early phases of kidney disease and the metabolic syndrome. Rev. Esp. Cardiol. 2011, 64, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Coresh, J.; Astor, B.C.; Greene, T.; Eknoyan, G.; Levey, A.S. Prevalence of chronic kidney disease and decreased kidney function in the adult US population: Third National Health and Nutrition Examination Survey. Am. J. Kidney Dis. 2003, 41, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Coresh, J.; Selvin, E.; Stevens, L.A.; Manzi, J.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Levey, A.S. Prevalence of chronic kidney disease in the United States. JAMA 2007, 298, 2038–2047. [Google Scholar] [CrossRef] [PubMed]
- Chadban, S.J.; Briganti, E.M.; Kerr, P.G.; Dunstan, D.W.; Welborn, T.A.; Zimmet, P.Z.; Atkins, R.C. Prevalence of kidney damage in Australian adults: The Aus Diab kidney study. J. Am. Soc. Nephrol. 2003, 14, S131–S138. [Google Scholar] [CrossRef] [PubMed]
- Magnason, R.L.; Indridason, O.S.; Sigvaldason, H.; Sigfusson, N.; Palsson, R. Prevalence and progression of CRF in Iceland: A population-based study. Am. J. Kidney Dis. 2002, 40, 955–963. [Google Scholar] [CrossRef] [PubMed]
- Nwankwo, E.; Bello, A.K.; El Nahas, A.M. Chronic kidney disease: Stemming the global tide. Am. J. Kidney Dis. 2005, 45, 201–208. [Google Scholar] [CrossRef]
- Jafar, T.H.; Schmid, C.H.; Levey, A.S. Serum creatinine as marker of kidney function in South Asians: A study of reduced GFR in adults in Pakistan. J. Am. Soc. Nephrol. 2005, 16, 1413–1419. [Google Scholar] [CrossRef] [PubMed]
- Amato, D.; Alvarez-Aguilar, C.; Castañeda-Limones, R.; Rodriguez, E.; Avila-Diaz, M.; Arreola, F.; Gomez, A.; Ballesteros, H.; Becerril, R.; Paniagua, R. Prevalence of chronic kidney disease in an urban Mexican population. Kidney Int. Suppl. 2005, 97, S11–S17. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Wildman, R.P.; Gu, D.; Kusek, J.W.; Spruill, M.; Reynolds, K.; Liu, D.; Hamm, L.L.; Whelton, P.K.; He, J. Prevalence of decreased kidney function in Chinese adults aged 35 to 74 years. Kidney Int. 2005, 68, 2837–2845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viktorsdottir, O.; Palsson, R.; Andresdottir, M.B.; Aspelund, T.; Gudnason, V.; Indridason, O.S. Prevalence of chronic kidney disease based on estimated glomerular filtration rate and proteinuria in Icelandic adults. Nephrol. Dial. Transplant. 2005, 20, 1799–1807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, C.C.; Hwang, S.J.; Wen, C.P.; Chang, H.Y.; Chen, T.; Shiu, R.S.; Horng, S.S.; Chang, Y.K.; Yamg, W.C. High prevalence and low awareness of CKD in Taiwan: A study on the relationship between serum creatinine and awareness from a nationally representative survey. Am. J. Kidney Dis. 2006, 48, 727–738. [Google Scholar] [CrossRef] [PubMed]
- Hallan, S.I.; Coresh, J.; Astor, B.C.; Asberg, A.; Powe, N.R.; Romundstad, S.; Hallan, H.A.; Lydersen, S.; Holmen, J. International comparison of the relationship of chronic kidney disease prevalence and ESRD risk. J. Am. Soc. Nephrol. 2006, 17, 2275–2284. [Google Scholar] [CrossRef] [PubMed]
- Djukanović, L.; Ležaić, V.; Dimković, N.; Peković, G.P.; Bukvić, D.; Bajčetić, S.; Pavlović, J.; Bontić, A.; Momćilović, D.; Stojanović, M. Early detection of chronic kidney disease: Collaboration of belgrade nephrologists and primary care physicians. Nefrologia 2012, 32, 59–66. [Google Scholar] [PubMed]
- Bonet, J.; Vila, J.; Alsina, M.J.; Ancochea, L.; Romero, R.; Baetulo, G. Prevalencia de microalbuminuria en la población general de un área mediterránea española y su asociación con otros factores de riesgo cardiovascular. Med. Clin. 2001, 116, 573–574. [Google Scholar] [CrossRef]
- Otero, A.; de Francisco, A.; Gayoso, P.; García, F. Prevalence of chronic renal disease in Spain: Results of the EPIRCE study. Nefrologia 2010, 30, 78–86. [Google Scholar]
- Chen, F.; Yang, W.; Weng, J.; Jia, W.; Ji, L.; Xiao, J.; Shan, Z.; Liu, J.; Tian, H.; Ji, Q.; et al. Albuminuria: Prevalence, associated risk factors and relationship with cardiovascular disease. J. Diabetes Investig. 2014, 5, 464–471. [Google Scholar] [CrossRef]
- Montañes, R.; Gràcia, S.; Pérez, D.; Martínez, A.; Bover, J. Documento de Consenso. Recomendaciones sobre la valoración de la proteinuria en el diagnóstico y seguimiento de la enfermedad renal crónica. Nefrologia 2011, 31, 331–345. [Google Scholar]
- American Diabetes Association. Standards of Medical Care in Diabetes-2010. Diabetes Care 2010, 33, S11–S61. [Google Scholar] [CrossRef] [PubMed]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L., Jr.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.T., Jr.; et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003, 42, 1206–1252. [Google Scholar] [CrossRef] [PubMed]
- The CARI guidelines. Urine protein as diagnostic test: Testing for proteinuria. Nephrology 2004, 9, S3–S7. [Google Scholar]
- Burden, R.; Tomson, C.; Joint Specialty Committee on Renal Disease; Renal Association. Identification, management and referral of adults with chronic kidney disease: Concise guidelines. Clin. Med. 2005, 5, 635–642. [Google Scholar] [CrossRef] [PubMed]
- Scottish Intercollegiate Guidelines Network. Diagnosis and Management of Chronic Kidney Disease—A National Clinical Guideline; Scottish Intercoll Guidel Network: Edinburgh, UK, 2008; pp. 1–57. [Google Scholar]
- Levey, A.S.; Lesley, A.I. Definition and Staging of Chronic Kidney Disease in Adults. Available online: http://www.uptodate.com/contents/definition-and-staging-of-chronic-kidne disease-in-adults (accessed on 5 April 2017).
- Bernelot Moens, S.J.; Verweij, S.L.; van der Valk, F.M.; van Capelleveen, J.C.; Kroon, J.; Versloot, M.; Verbeme, H.J.; Marquering, H.A.; Duivenvoorden, R.; Vogt, L.; et al. Arterial and Cellular Inflammation in Patients with CKD. J. Am. Soc. Nephrol. 2017, 28, 1278–1285. [Google Scholar] [CrossRef] [PubMed]
- Caballería, L.; Pera, G.; Arteaga, I.; Rodríguez, L.; Alumà, A.; Morillas, R.M.; de la Ossa, N.; Díaz, A.; Expósito, C.; Miranda, D.; et al. High Prevalence of Liver Fibrosis Among European Adults With Unknown Liver Disease: A Population-Based Study. Clin. Gastroenterol. Hepatol. 2018, 16, 1138–1145. [Google Scholar] [CrossRef]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of Diet in Renal Disease Study Group. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef]
- Levey, A.S.; Greene, T.; Kusek, J.W.; Beck, G.J.; MDRD Study Group. A simplified equation to predict glomerular filtration rate from serum creatinine. J. Am. Soc. Nephrol. 2000, 11, A155. [Google Scholar]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Coresh, J. Conceptual Model of CKD: Applications and Implications. Am. J. Kidney Dis. 2009, 53, S4–S16. [Google Scholar] [CrossRef] [PubMed]
- Brück, K.; Stel, V.S.; Gambaro, G.; Hallan, S.; Völzke, H.; Ärnlöv, J.; Kastarinen, M.; Guessous, I.; Vinhas, J.; Stengel, B.; et al. CKD Prevalence Varies across the European General Population. J. Am. Soc. Nephrol. 2016, 27, 2135–2147. [Google Scholar] [CrossRef] [PubMed]
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.D. Global Prevalence of Chronic Kidney Disease—A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef] [PubMed]
- Gorostidi, M.; Sánchez-Martínez, M.; Ruilope, L.M.; Graciani, A.; de la Cruz, J.J.; Santamaría, R.; Del Pino, M.D.; Guallar-Castillón, P.; de Álvaro, F.; Rodríguez-Artalejo, F.; et al. Chronic kidney disease in Spain: Prevalence and impact of accumulation of cardiovascular risk factors. Nefrologia 2018, 38, 606–615. [Google Scholar] [CrossRef] [PubMed]
- Gheewala, P.A.; Zaidi, S.T.R.; Jose, M.D.; Bereznicki, L.; Peterson, G.M.; Castelino, R.L. Effectiveness of targeted screening for chronic kidney disease in the community setting: A systematic review. J. Nephrol. 2018, 31, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Inker, L.A.; Perrone, R.D. Assessment of Kidney Function; Stems, R.H., Ed.; UpToDate: Waltham, MA, USA, 2018; Available online: https://www.uptodate.com/contents/assessment-of-kidney-function (accessed on 18 February 2019).
- Heathcote, K.L.; Wilson, M.P.; Quest, D.W.; Wilson, T.W. Prevalence and duration of exercise induced albuminuria in healthy people. Clin. Invest. Med. 2009, 32, E261–E265. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; de Jong, P.E.; Coresh, J.; El Nahas, M.; Astor, B.C.; Matsushita, K.; Gansevoort, R.T.; Kasiske, B.L.; Eckardt, K.U. The definition, classification, and prognosis of chronic kidney disease: A KDIGO Controversies Conference report. Kidney Int. 2011, 80, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Chronic Kidney Disease Prognosis Consortium; Matsushita, K.; van der Velde, M.; Astor, B.C.; Woodward, M.; Levey, A.S.; de Jong, P.E.; Coresh, J.; Gansevoort, R.T. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: A collaborative meta-analysis. Lancet 2010, 375, 2073–2081. [Google Scholar] [PubMed]
- Hallan, S.I.; Matsushita, K.; Sang, Y.; Mahmoodi, B.K.; Black, C.; Ishani, A.; Kleefstra, N.; Naimark, D.; Roderick, P.; Tonelli, M.; et al. Age and the Association of Kidney Measures with Mortality and End-Stage Renal Disease. JAMA 2012, 308, 2349–2360. [Google Scholar] [CrossRef]
- Ji, E.; Kim, Y.S. Prevalence of chronic kidney disease defined by using CKD-EPI equation and albumin-to-creatinine ratio in the Korean adult population. Korean J. Intern. Med. 2016, 31, 1120–1130. [Google Scholar] [CrossRef] [Green Version]
- Drion, I.; Cobbaert, C.; Groenier, K.H.; Weykamp, C.; Bilo, H.J.; Wetzels, J.F.; Kleefstra, N. Clinical evaluation of analytical variations in serum creatinine measurements: Why laboratories should abandon Jaffe techniques. BMC Nephrol. 2012, 13, 133. [Google Scholar] [CrossRef] [PubMed]
- Bachmann, L.M.; Nilsson, G.; Bruns, D.E.; McQueen, M.J.; Lieske, J.C.; Zakowski, J.J.; Miller, W.G. State of the art for measurement of urine albumin: Comparison of routine measurement procedures to isotope dilution tandem mass spectrometry. Clin. Chem. 2014, 60, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Coresh, J.; Byrd-Holt, D.; Astor, B.C.; Briggs, J.P.; Eggers, P.W.; Lacher, D.A.; Hostetter, T.H. Chronic kidney disease awareness, prevalence, and trends among U.S. adults, 1999 to 2000. J. Am. Soc. Nephrol. 2005, 16, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Warram, J.H.; Gearin, G.; Laffel, L.; Krolewski, A.S. Effect of duration of type I diabetes on the prevalence of stages of diabetic nephropathy defined by urinary albumin/creatinine ratio. J. Am. Soc. Nephrol. 1996, 7, 930–937. [Google Scholar]
- Taal, M.; Tomson, C. Clinical practice guidelines for the care of patients with chronic kidney disease. In UK Renal Association Clinical Practice Guidelines, 4th ed.; The Renal Association: Bristol, UK, 2007; Available online: www.renal.org/guidelines (accessed on 12 November 2018).
- Johnson, D.W.; Atai, E.; Chan, M.; Phoon, R.K.; Scott, C.; Toussaint, N.D.; Turner, G.L.; Usherwood, T.; Wiggins, K.J.; KHA-CARI. KHA-CARI guideline: Early chronic kidney disease: Detection, prevention and management. Nephrology 2013, 18, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Fox, C.S.; Larson, M.G.; Leip, E.P.; Culleton, B.; Wilson, P.W.F.; Levy, D. Predictors of new-onset kidney disease in a community-based population. JAMA 2004, 291, 844–850. [Google Scholar] [CrossRef] [PubMed]
- Flegal, K.M.; Kruszon-Moran, D.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Trends in Obesity Among Adults in the United States, 2005 to 2014. JAMA 2016, 315, 2284–2291. [Google Scholar] [CrossRef] [Green Version]
- Aranceta-Bartrina, J.; Perez-Rodrigo, C.; Alberdi-Aresti, G.; Ramos-Carrera, N.; Lazaro-Masedo, S. Prevalencia de obesidad general y obesidad abdominal en la poblacion adulta española (25-64 años) 2014-2015: Estudio ENPE. Rev. Esp. Cardiol. 2016, 69, 579–587. [Google Scholar] [CrossRef]
- Maric, C.; Hall, J.E. Obesity, Metabolic Syndrome and Diabetic Nephropathy. NIH Public Access. 2011, 170, 28–35. [Google Scholar] [Green Version]
- Musso, G.; Gambino, R.; Tabibian, J.H.; Ekstedt, M.; Kechagias, S.; Hamaguchi, M.; Hultcrantz, R.; Hagström, H.; Yoon, S.K.; Charatcharoenwitthaya, P.; et al. Association of non-alcoholic fatty liver disease with chronic kidney disease: A systematic review and meta-analysis. PLoS Med. 2014, 11, e1001680. [Google Scholar] [CrossRef]
- Targher, G.; Chonchol, M.B.; Byrne, C.D. CKD and Nonalcoholic Fatty Liver Disease. Am. J. Kidney Dis. 2014, 64, 638–652. [Google Scholar] [CrossRef] [PubMed]
- Escasany, E.; Izquierdo-Lahuerta, A.; Medina-Gomez, G. Underlying Mechanisms of Renal Lipotoxicity in Obesity. Nephron 2019, 143, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Mende, C.; Einhorn, D. Fatty kidney disease: A new renal and endocrine clinical entity? Describing the role of the kidney in obesity, metabolic syndrome, and type 2 diabetes. Endocr. Pract. 2019, 25, 854–858. [Google Scholar] [CrossRef] [PubMed]
- Silva Junior, G.; Bentes, A.; Daher, E.; Matos, S. Obesity and kidney disease. J. Bras. Nefrol. 2017, 39, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.C.; Lai, Y.J.; Lin, Y.C.; Peng, C.C.; Chen, K.C.; Chuang, M.T.; Wu, M.S.; Chang, T.H. Effect of weight loss on the estimated glomerular filtration rates of obese patients at risk of chronic kidney disease: The RIGOR-TMU study. J. Cachexia Sarcopenia Muscle 2019, 10, 756–766. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Poncelas, A.; Garre-Olmo, J.; Franch-Nadal, J.; Diez-Espino, J.; Mundet-Tuduri, X.; Barrot-De la Puente, J.; Coll-de Tuero, G.; RedGDPS Study Group. Prevalence of chronic kidney disease in patients with type 2 diabetes in Spain: PERCEDIME2 study. BMC Nephrol. 2013, 14, 46. [Google Scholar] [CrossRef] [PubMed]
- Murphy, D.; McCulloch, C.E.; Lin, F.; Banerjee, T.; Bragg-Gresham, J.L.; Eberhardt, M.S.; Morgenstern, H.; Pavkov, M.E.; Saran, R.; Powe, N.R.; et al. Trends in Prevalence of Chronic Kidney Disease in the United States. Ann. Intern. Med. 2016, 165, 473–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | EKD | Total | |||||
|---|---|---|---|---|---|---|---|
| No | Yes | ||||||
| n | % | n | % | n | % | p | |
| Gender | <0.001 | ||||||
| Males | 1137 | 93.0% | 85 | 7.0% | 1222 | 43.0% | |
| Females | 1625 | 98.5% | 24 | 1.5% | 1649 | 57.0% | |
| Age | <0.001 | ||||||
| 19–44 | 562 | 98.8% | 7 | 1.2% | 569 | 19.8% | |
| 45–54 | 674 | 97.8% | 15 | 2.2% | 689 | 24.0% | |
| 5–64 | 928 | 96.% | 38 | 3.9% | 966 | 33.6% | |
| 65–75 | 598 | 92.4% | 49 | 7.6% | 647 | 22.5% | |
| Mean, (±SD) | 55 | 12 | 61 | 9 | 55 | 12 | <0.001 |
| Tobacco | <0.001 | ||||||
| Non smoker | 1339 | 98.0% | 28 | 2.0% | 1367 | 47.6% | |
| Former smoker | 778 | 93.4% | 55 | 6.6% | 833 | 29.0% | |
| Current smoker | 633 | 96.3% | 24 | 3.7% | 657 | 22.9% | |
| Alcohol | <0.001 | ||||||
| Never drinker | 1392 | 97.1% | 42 | 2.9% | 1434 | 50.0% | |
| Moderate drinker 1 | 1123 | 96.1% | 45 | 3.9% | 1168 | 40.6% | |
| Risk drinker | 244 | 91.7% | 22 | 8.3% | 266 | 9.2% | |
| Obesity | <0.001 | ||||||
| Normoweight (BMI < 25 kg/m2) | 741 | 98.8% | 9 | 1.2% | 750 | 26.2% | |
| Overweight (25 ≤ BMI < 30 kg/m2) | 1153 | 96.8% | 38 | 3.2% | 1191 | 41.6% | |
| Obese (BMI ≥ 30 kg/m2) | 859 | 93.3% | 62 | 6.7% | 921 | 32.2% | |
| Abdominal obesity 2 | 0.001 | ||||||
| No | 1373 | 97.4% | 36 | 2.6% | 1409 | 49.5% | |
| Yes | 1368 | 95.1% | 71 | 4.9% | 1439 | 50.5% | |
| Arterial hypertension | <0.001 | ||||||
| No | 2049 | 97.9% | 44 | 2.1% | 2093 | 72.9% | |
| Yes | 713 | 91.6% | 65 | 8.4% | 778 | 27.1% | |
| Blood pressure (≥130/85 mmHg) | <0.001 | ||||||
| No | 1548 | 98.3% | 26 | 1.7% | 1574 | 55.0% | |
| Yes | 1205 | 93.6% | 83 | 6.4% | 1288 | 45.0% | |
| Type-2 diabetes | <0.001 | ||||||
| No | 2504 | 97.6% | 62 | 2.4% | 2566 | 89.4% | |
| Yes | 258 | 84.6% | 47 | 15.4% | 305 | 10.6% | |
| Glucose (≥100 mg/dL) | <0.001 | ||||||
| No | 1776 | 98.0% | 37 | 2.0% | 1813 | 63.7% | |
| Yes | 963 | 93.0% | 72 | 7.0% | 1035 | 36.3% | |
| HDL < 40/50 mg/dL (Male/Female) | 0.086 | ||||||
| No | 2184 | 96.5% | 80 | 3.5% | 2264 | 79.9% | |
| Yes | 542 | 94.9% | 29 | 5.1% | 571 | 20.1% | |
| Triglycerides (≥150 mg/dL) | <0.001 | ||||||
| No | 2076 | 97.1% | 61 | 2.9% | 2137 | 75.3% | |
| Yes | 653 | 93.2% | 48 | 6.8% | 701 | 24.7% | |
| OR | IC95% | p | ||
|---|---|---|---|---|
| Age (per year) | 1.04 | 1.02 | 1.70 | 0.001 |
| Male gender | 3.35 | 1.98 | 5.68 | 0.001 |
| Smoker | 1.67 | 1.02 | 2.73 | 0.042 |
| Overweight (25 ≤ BMI < 30 kg/m2) | 1.35 | 0.63 | 2.87 | 0.440 |
| Obesity (BMI ≥ 30 Kg/m2) | 2.48 | 1.18 | 5.20 | 0.016 |
| Blood pressure (≥130/85 mmHg) | 2.29 | 1.41 | 3.70 | 0.001 |
| Fasting glucose (≥100 mg/dL) | 1.73 | 1.12 | 2.67 | 0.013 |
| Triglycerides (≥150 mg/dL) | 1.51 | 1.00 | 2.29 | 0.053 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Expósito, C.; Pera, G.; Rodríguez, L.; Arteaga, I.; Martínez, A.; Alumà, A.; Doladé, M.; Torán, P.; Caballeria, L. Prevalence of Early Chronic Kidney Disease and Main Associated Factors in Spanish Population: Populational Study. J. Clin. Med. 2019, 8, 1384. https://doi.org/10.3390/jcm8091384
Expósito C, Pera G, Rodríguez L, Arteaga I, Martínez A, Alumà A, Doladé M, Torán P, Caballeria L. Prevalence of Early Chronic Kidney Disease and Main Associated Factors in Spanish Population: Populational Study. Journal of Clinical Medicine. 2019; 8(9):1384. https://doi.org/10.3390/jcm8091384
Chicago/Turabian StyleExpósito, Carmen, Guillem Pera, Lluís Rodríguez, Ingrid Arteaga, Alba Martínez, Alba Alumà, María Doladé, Pere Torán, and Llorenç Caballeria. 2019. "Prevalence of Early Chronic Kidney Disease and Main Associated Factors in Spanish Population: Populational Study" Journal of Clinical Medicine 8, no. 9: 1384. https://doi.org/10.3390/jcm8091384