Does the Implementation of a Quality Improvement Care Bundle Reduce the Incidence of Acute Kidney Injury in Patients Undergoing Emergency Laparotomy?

 , , ,
, , ,
Abstract
:1. Introduction
- All emergency surgical admissions risk assessed using the M(EWS) score [4]. Those with M(EWS) ≥4 reviewed by critical care outreach team.
- Broad spectrum antibiotics given to all patients with suspicion of peritoneal soiling or with sepsis.
- Once the decision is made for a laparotomy then next available theatre slot is used (or within 6 h) with senior clinical input (consultant anaesthetist and surgeon).
- Resuscitation commenced using goal-directed techniques and continued for a minimum of six hours post-operatively.
- All patients admitted to critical care when possible after surgery or held in a post anaesthetic care unit for at least six hours.
2. Methods
Statistical Analysis
3. Results
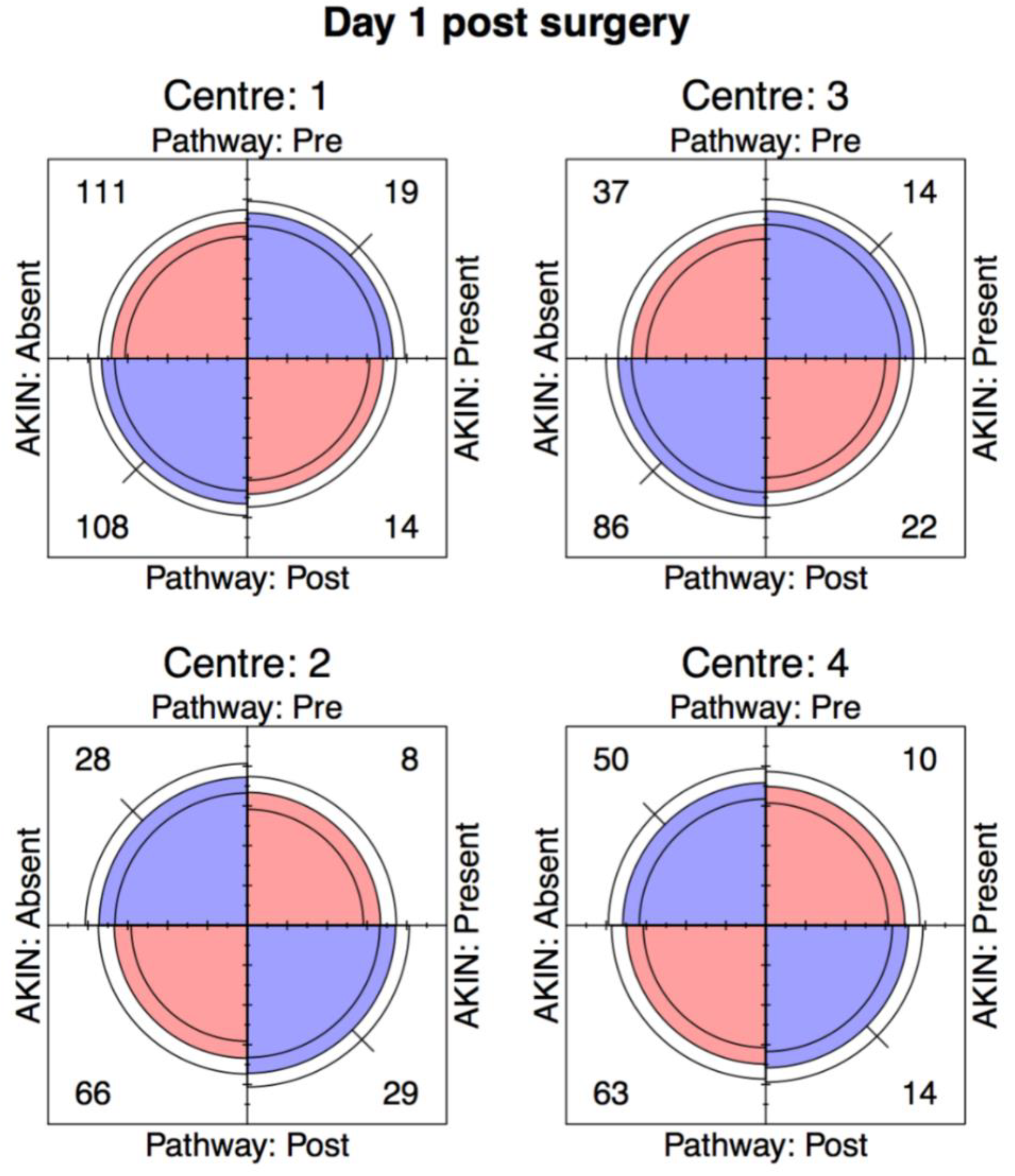
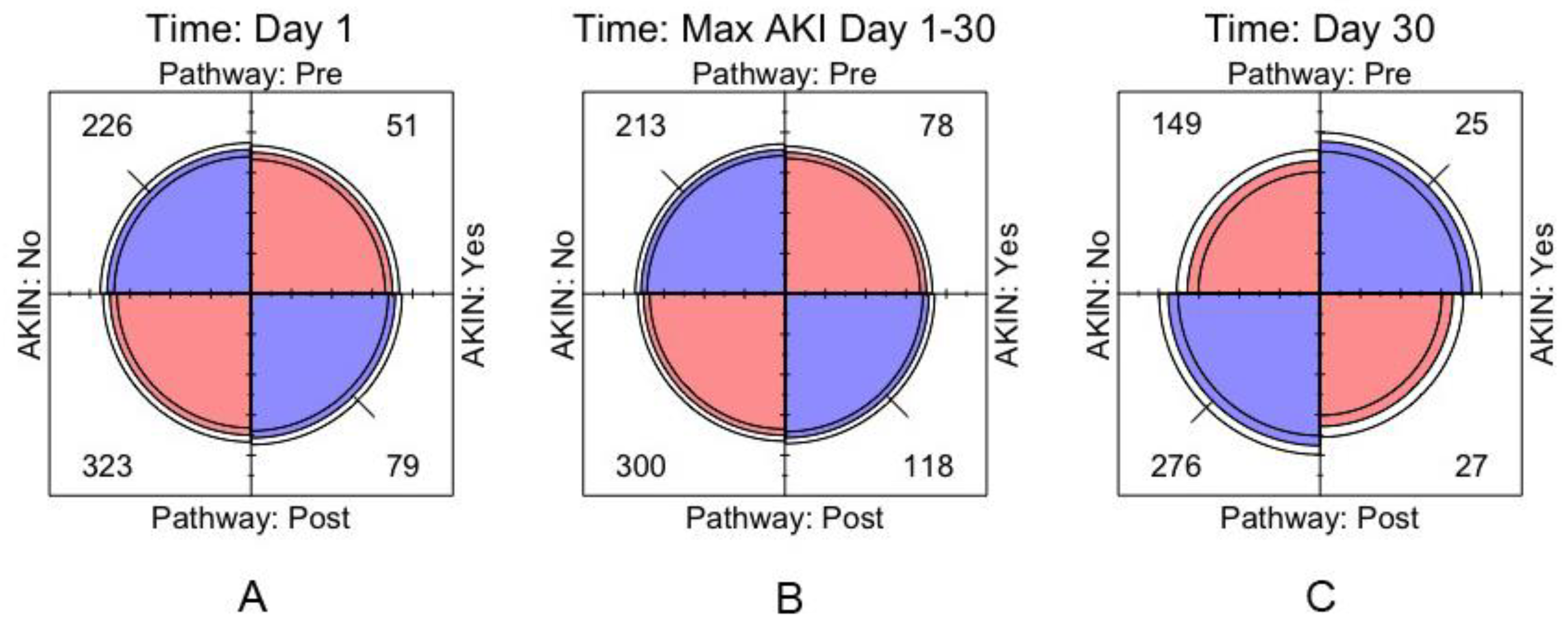
3.1. Day 1 AKI
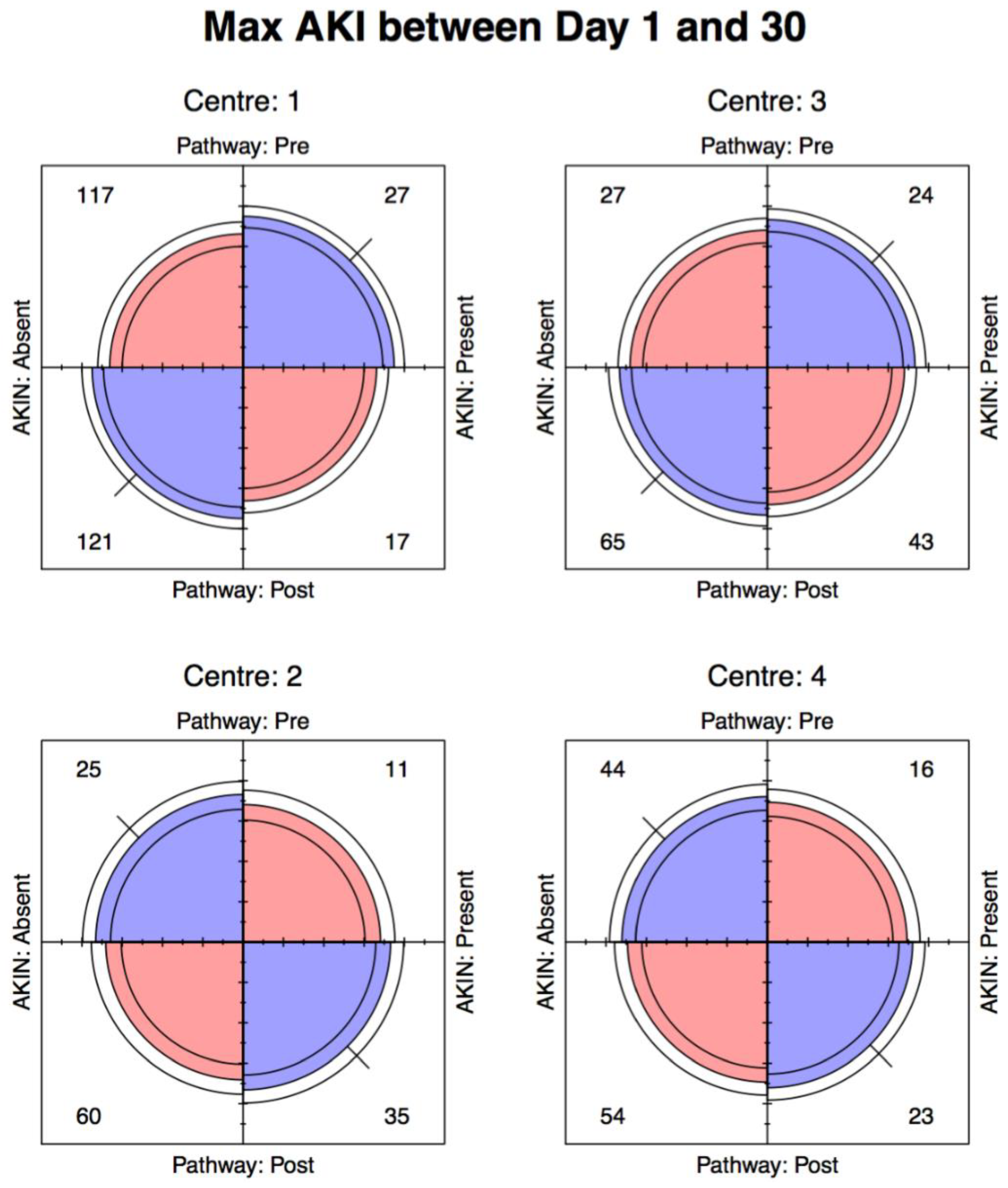
3.2. Maximum AKI Day 1–30
3.3. Day 30 AKI
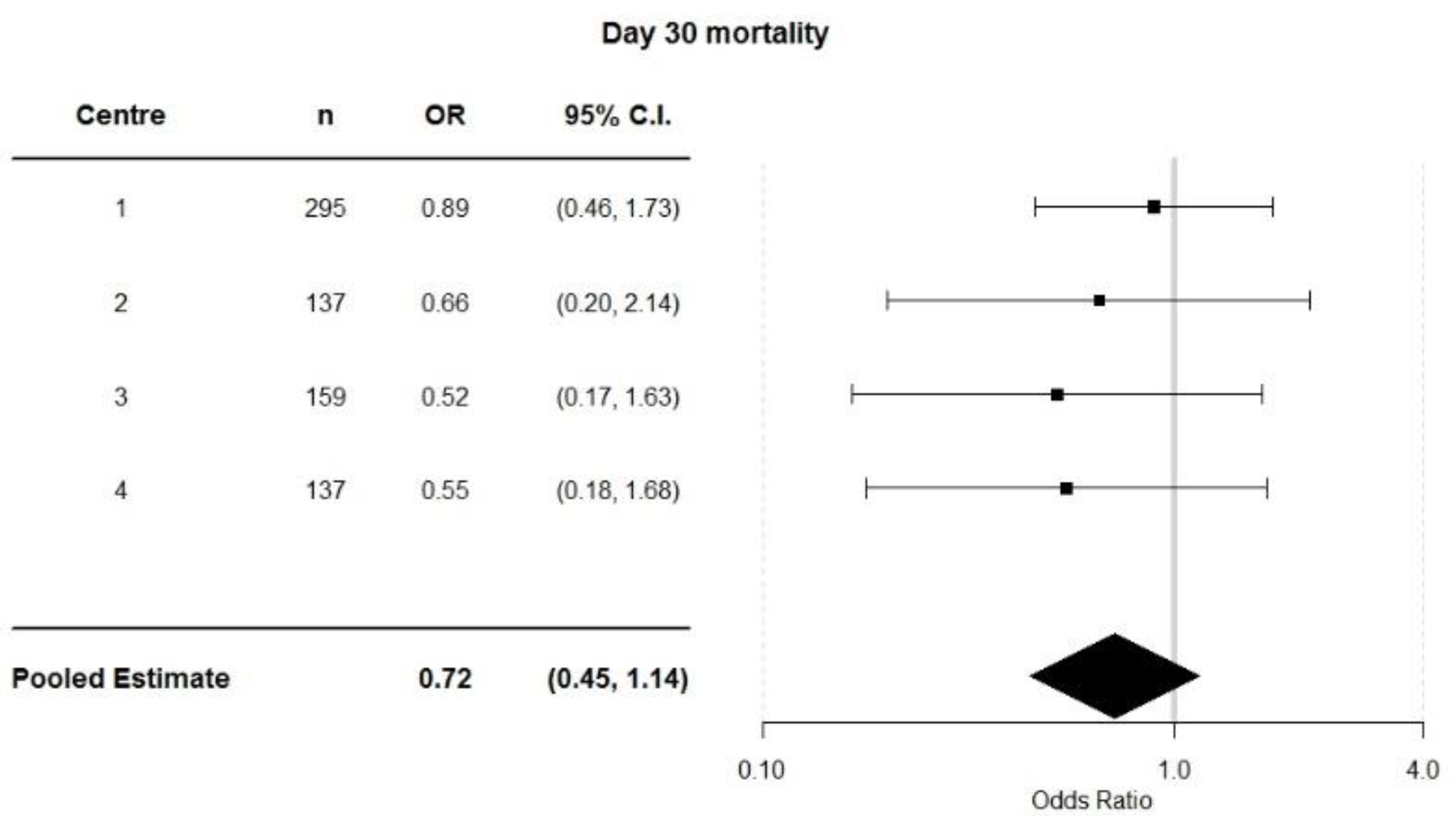
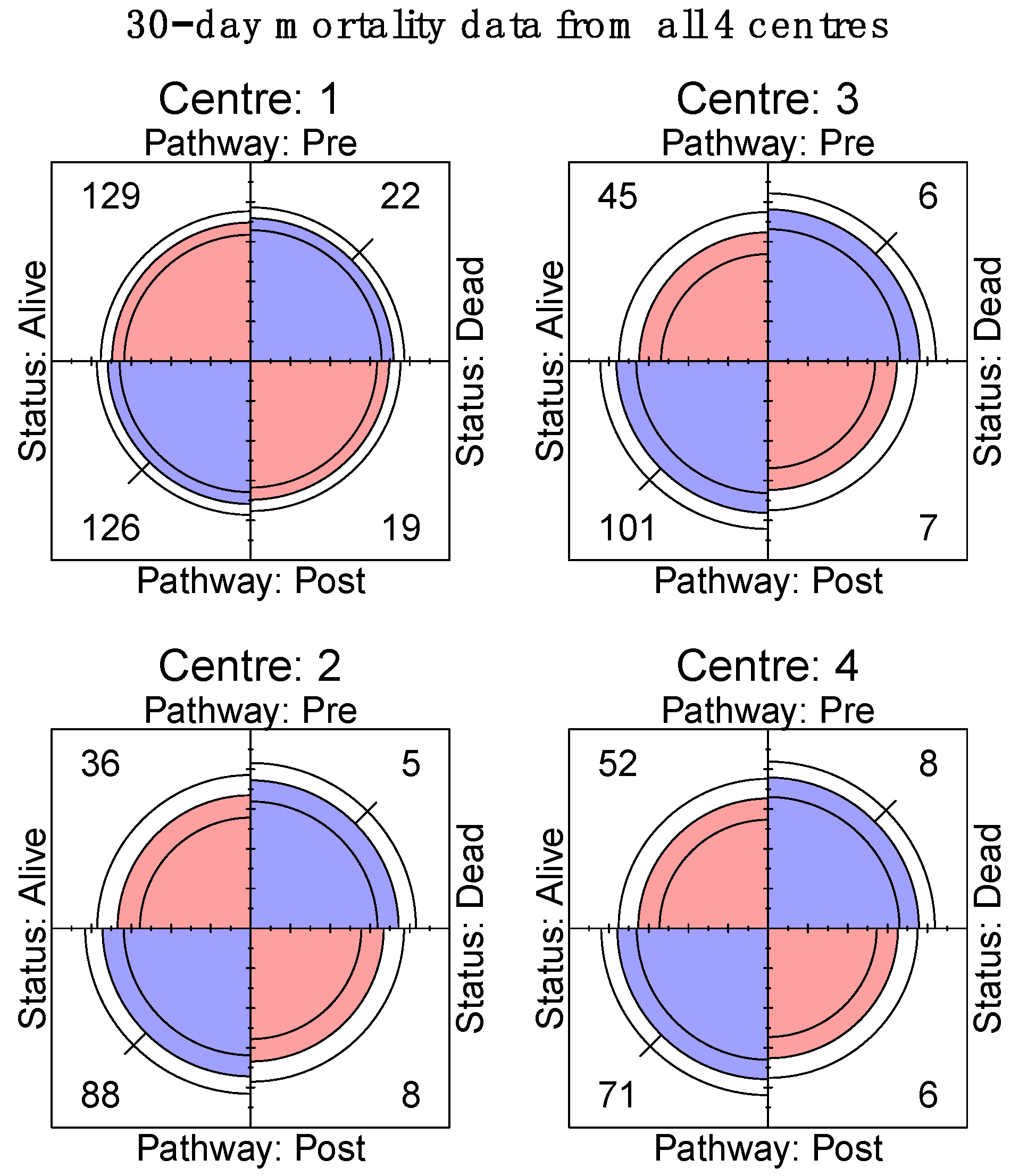
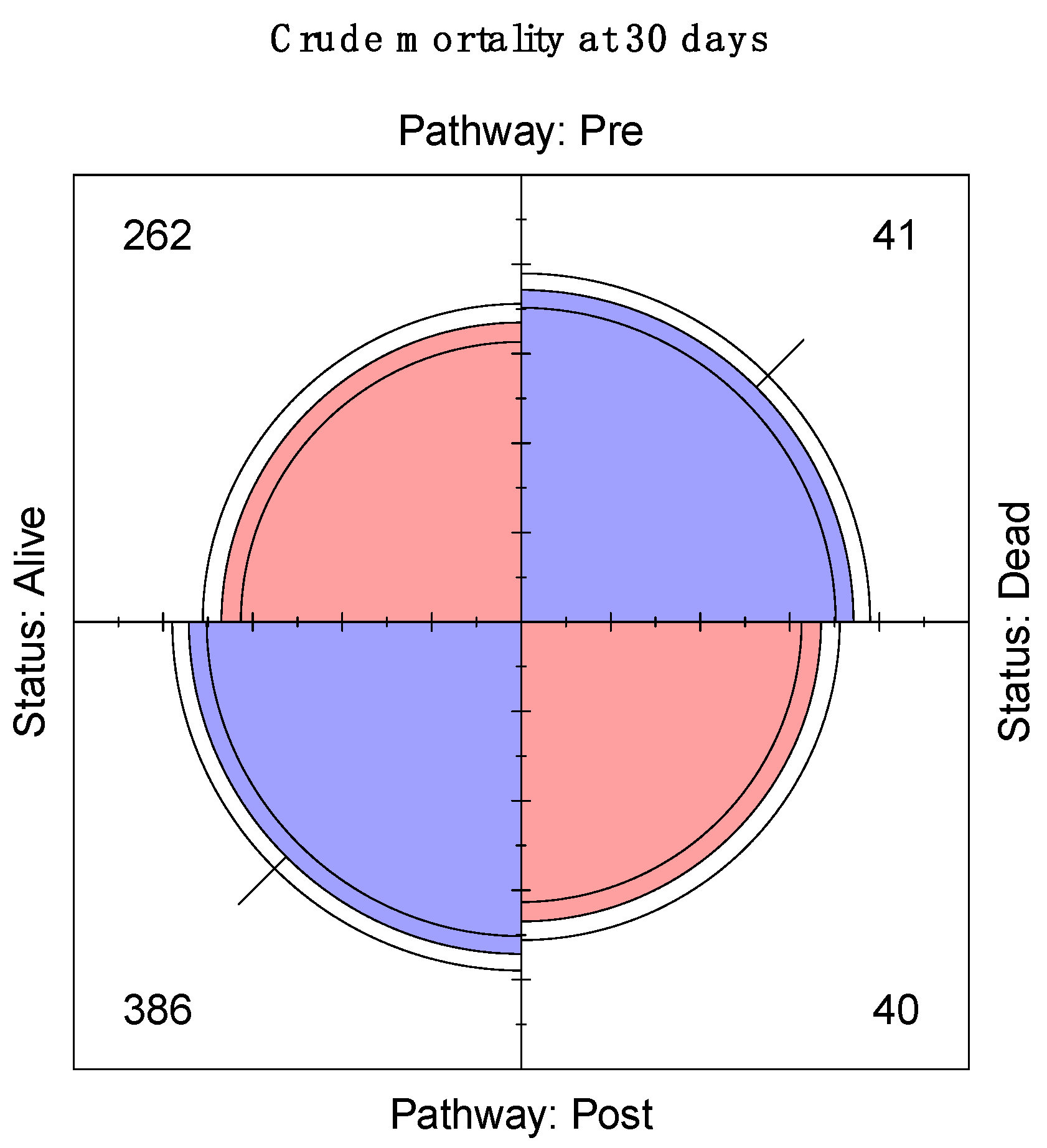
3.4. Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AKI | Acute kidney injury |
| ELPQuiC | Emergency laparotomy pathway quality improvement care bundle |
References
- Gustafsson, U.O.; Scott, M.J.; Schwenk, W.; Demartines, N.; Roulin, D.; Francis, N.; McNaught, C.E.; Macfie, J.; Liberman, A.S.; Soop, M.; et al. Guidelines for perioperative care in elective colonic surgery: Enhanced Recovery After Surgery (ERAS) Society recommendations. World J. Surg. 2013, 37, 259–284. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, A.; Lowe, M.C.; Parker, J.; Lewis, S.R.; Alderson, P.; Smith, A.F. Systematic review and meta-analysis of enhanced recoveryprogrammes in surgical patients. Br. J. Surg. 2014, 101, 172–188. [Google Scholar] [CrossRef] [PubMed]
- Huddart, S.; Peden, C.J.; Swart, M.; McCormick, B.; Dickinson, M.; Mohammed, M.A.; Quiney, N.; Group, E.L.C. Use of a pathway quality improvement care bundle to reduce mortality after emergency laparotomy. Br. J. Surg. 2015, 102, 57–66. [Google Scholar] [CrossRef]
- Subbe, C.P.; Kruger, M.; Rutherford, P.; Gemmel, L. Validation of a modified Early Warning Score in medical admissions. QJM 2001, 94, 521–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NELA Project Team. The First Patient Report of the National Emergency Laparotomy Audit; RCoA: London, UK, 2015. [Google Scholar]
- Al-Temimi, M.H.; Griffee, M.; Enniss, T.M.; Preston, R.; Vargo, D.; Overton, S.; Kimball, E.; Barton, R.; Nirula, R. When is death inevitable after emergency laparotomy? Analysis of the American College of Surgeons National Surgical Quality Improvement Program database. J. Am. Coll. Surg. 2012, 215, 503–511. [Google Scholar] [CrossRef]
- Vester-Andersen, M.; Lundstrøm, L.H.; Møller, M.H.; Waldau, T.; Rosenberg, J.; Møller, A.M. Mortality and postoperative care pathways after emergency gastrointestinal surgery in 2904 patients: A population-based cohort study. Br. J. Anaesth. 2014, 112, 860–870. [Google Scholar] [CrossRef]
- The Royal College of Surgeons of England. The Higher Risk General Surgical Patient: Towards Improved Care for a Forgotten Group; RCSENG: London, UK, 2011. [Google Scholar]
- Chang, C.H.; Fan, P.C.; Chang, M.Y.; Tian, Y.C.; Hung, C.C.; Fang, J.T.; Yang, C.W.; Chen, Y.C. Acute kidney injury enhances outcome prediction ability of sequential organ failure assessment score in critically ill patients. PLoS ONE 2014, 9, e109649. [Google Scholar] [CrossRef] [PubMed]
- Hoste, E.A.; Bagshaw, S.M.; Bellomo, R.; Cely, C.M.; Colman, R.; Cruz, D.N.; Edipidis, K.; Forni, L.G.; Gomersall, C.D.; Govil, D.; et al. Epidemiology of acute kidney injury in critically ill patients: The multinational AKI-EPI study. Intensive Care Med. 2015, 41, 1411–1423. [Google Scholar] [CrossRef] [PubMed]
- Howes, T.E.; Cook, T.M.; Corrigan, L.J.; Dalton, S.J.; Richards, S.K.; Peden, C.J. Postoperative morbidity survey, mortality and length of stay following emergency laparotomy. Anaesthesia 2015, 70, 1020–1027. [Google Scholar] [CrossRef]
- Linder, A.; Fjell, C.; Levin, A.; Walley, K.R.; Russell, J.A.; Boyd, J.H. Small acute increases in serum creatinine are associated with decreased long-term survival in the critically ill. Am. J. Respir. Crit. Care Med. 2014, 189, 1075–1081. [Google Scholar] [CrossRef] [PubMed]
- Doyle, J.F.; Forni, L.G. Acute kidney injury: Short-term and long-term effects. Crit. Care 2016, 20, 188. [Google Scholar] [CrossRef]
- Khwaja, A. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Nephron Clin. Pract. 2012, 120, 179–184. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, M.E.; Kirwan, C.J.; Pearse, R.M.; Prowle, J.R. Incidence and associations of acute kidney injury after major abdominal surgery. Intensive Care Med. 2016, 42, 521–530. [Google Scholar] [CrossRef]
- Quiney, N.H.S.; Peden, C.; Dickinson, M. Use of a care bundle to reduce mortality following emergency laparotomy. Br. J. Hosp. Med. 2015, 76, 358–362. [Google Scholar] [CrossRef]
- Prytherch, D.R.; Whiteley, M.S.; Higgins, B.; Weaver, P.C.; Prout, W.G.; Powell, S.J. POSSUM and Portsmouth POSSUM for predicting mortality. Physiological and Operative Severity Score for the enUmeration of Mortality and morbidity. Br. J. Surg. 1998, 85, 1217–1220. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; Van Lente, F. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef] [PubMed]
- The R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2015. [Google Scholar]
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2009. [Google Scholar]
- Gordon, M.L.T. Advanced Forest Plot Using ‘grid’ Graphics. Available online: https://cran.r-project.org/web/packages/forestplot/forestplot.pdf (accessed on 20 August 2019).
- Meyer, D.Z.A.; Hornik, A. Vcd: Visualizing Categorical Data. Available online: https://cran.r-project.org/web/packages/vcd/vcd.pdf (accessed on 20 August 2019).
- Pearse, R.M.; Harrison, D.A.; MacDonald, N.; Gillies, M.A.; Blunt, M.; Ackland, G.; Grocott, M.P.; Ahern, A.; Griggs, K.; Scott, R.; et al. Effect of a perioperative, cardiac output-guided hemodynamic therapy algorithm on outcomes following major gastrointestinal surgery: A randomized clinical trial and systematic review. JAMA 2014, 311, 2181–2190. [Google Scholar] [CrossRef] [PubMed]
- Grocott, M.P.; Dushianthan, A.; Hamilton, M.A.; Mythen, M.G.; Harrison, D.; Rowan, K. Perioperative increase in global blood flow to explicit defined goals and outcomes after surgery: A Cochrane Systematic Review. Br. J. Anaesth. 2013, 111, 535–548. [Google Scholar] [CrossRef]
- Russell, J.A.; Walley, K.R.; Singer, J.; Gordon, A.C.; Hébert, P.C.; Cooper, D.J.; Holmes, C.L.; Mehta, S.; Granton, J.T.; Storms, M.M.; et al. Investigators TV: Vasopressin versus Norepinephrine Infusion in Patients with Septic Shock. N. Eng. J. Med. 2008, 358, 877–887. [Google Scholar] [CrossRef]
- Sun, L.Y.; Wijeysundera, D.N.; Tait, G.A.; Beattie, W.S. Association of intraoperative hypotension with acute kidney injury after elective noncardiac surgery. Anesthesiology 2015, 123, 515–523. [Google Scholar] [CrossRef]
- Rhee, C.J.; Kibler, K.K.; Easley, R.B.; Andropoulos, D.B.; Czosnyka, M.; Smielewski, P.; Brady, K.M. Renovascular reactivity measured by near-infrared spectroscopy. J. Appl. Physiol. 2012, 113, 307–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bayliss, W.M. On the local reactions of the arterial wall to changes of internal pressure. J. Physiol. 1902, 28, 220–231. [Google Scholar] [CrossRef] [PubMed]
- Meersch, M.; Schmidt, C.; Hoffmeier, A.; Van Aken, H.; Wempe, C.; Gerss, J.; Zarbock, A. Prevention of cardiac surgery-associated AKI by implementing the KDIGO guidelines in high risk patients identified by biomarkers: The PrevAKI randomized controlled trial. Intensive Care Med. 2017, 43, 1551–1561. [Google Scholar] [CrossRef] [PubMed]
- Gocze, I.; Jauch, D.; Gotz, M.; Kennedy, P.; Jung, B.; Zeman, F.; Gnewuch, C.; Graf, B.M.; Gnann, W.; Banas, B.; et al. Biomarker-guided Intervention to Prevent Acute Kidney Injury After Major Surgery: The Prospective Randomized BigpAK Study. Ann. Surg. 2017, 267, 1013–1020. [Google Scholar] [CrossRef]
- Eknoyan, G.; Lameire, N.; Eckardt, K.; Kasiske, B.; Wheeler, D.; Levin, A.; Stevens, P.E.; Bilous, R.W.; Lamb, E.J.; Coresh, J.; et al. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. 2013, 3, 5–14. [Google Scholar]
- Bellomo, R.; Ronco, C.; Kellum, J.A.; Mehta, R.L.; Palevsky, P. Acute renal failure—Definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2007, 11, 411. [Google Scholar]
- Ye, M.; Dai, Q.; Zheng, J.; Jiang, X.; Wang, H.; Lou, S.; Yu, K. The significance of post-operative creatinine in predicting prognosis in cardiac surgery patients. Cell Biochem. Biophys. 2014, 70, 587–591. [Google Scholar] [CrossRef]
- Pearse, R. Enhanced Peri-Operative Care for High-risk patients (EPOCH) Trial: A stepped Wedge Cluster Randomised Trial of a Quality Improvement Intervention for Patients Undergoing Emergency Laparotomy; Queen Mary University of London: London, UK, 2014. [Google Scholar]
- Dellinger, R.P.; Levy, M.M.; Rhodes, A.; Annane, D.; Gerlach, H.; Opal, S.M.; Sevransky, J.E.; Sprung, C.L.; Douglas, I.S.; Jaeschke, R.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012. Crit. Care Med. 2013, 41, 580–637. [Google Scholar]
- Aggarwal, G.; Peden, C.J.; Mohammed, M.A.; Pullyblank, A.; Williams, B.; Stephens, T.; Kellett, S.; Kirkby-Bott, J.; Quiney, N.; Emergency Laparotomy, C. Evaluation of the Collaborative Use of an Evidence-Based Care Bundle in Emergency Laparotomy. JAMA Surg. 2019, 154, e190145. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Site 1 | Site 2 | Site 3 | Site 4 | All Patients | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Before ELPQuiC (n = 51) | After ELPQuiC (n = 109) | Before ELPQuiC (n = 144) | After ELPQuiC (n = 144) | Before ELPQuiC (n = 44) | After ELPQuiC (n = 97) | Before ELPQuiC (n = 60) | After ELPQuiC (n = 77) | Before ELPQuiC (n = 299) | After ELPQuiC (n = 427) | |
| Age (years) * | 66.6 (16.6) | 65.3 (17.7) | 65.1 (16.6) | 63.7 (17.5) | 65.7 (13.9) | 69.3 (14.0) | 66.2 (15.0) | 66.0 (15.5) | 65.6 (15.8) | 65.8 (16.5) |
| Sex | ||||||||||
| F | 38 (75) | 56 (51.4) | 73 (50.7) | 79 (54.9) | 19 (43) | 49 (51) | 31 (52) | 41 (53) | 161 (53.8) | 225 (52.7) |
| M | 13 (25) | 53 (48.6) | 71 (49.3) | 65 (45.1) | 25 (57) | 48 (49) | 29 (48) | 36 (47) | 138 (46.2) | 202 (47.3) |
| Outcomes at 30 days | ||||||||||
| alive | 42 (82) | 96 (88.1) | 123 (85.4) | 126 (87.5) | 39 (89) | 89 (92) | 53 (88) | 71 (92) | 257 (86.0) | 382 (89.5) |
| dead | 9 (18) | 13 (11.9) | 21 (14.6) | 18 (12.5) | 5 (11) | 8 (8) | 7 (12) | 6 (8) | 42 (14.0) | 45 (10.5) |
| Died in hospital | ||||||||||
| no | 41 (80) | 96 (88.1) | 122 (84.7) | 125 (86.8) | 37 (84) | 89 (92) | 52 (87) | 70 (91) | 252 (84.3) | 380 (89.0) |
| yes | 10 (20) | 13 (11.9) | 22 (15.3) | 19 (13.2) | 7 (16) | 8 (8) | 8 (13) | 7 (9) | 47 (15.7) | 47(11.0) |
| ASA fitness grade | ||||||||||
| I | 5 (10) | 14 (12.8) | 12 (8.3) | 16 (11.1) | 4 (9) | 8 (8) | 6 (10) | 7 (9) | 27 (9.0) | 45 (10.5) |
| II | 10 (20) | 36 (33.0) | 48 (33.3) | 52 (36.1) | 9 (21) | 32 (33) | 28 (47) | 27 (35) | 95 (31.8) | 147 (34.4) |
| III | 19 (37) | 40 (36.7) | 46 (31.9) | 44 (30.6) | 18 (41) | 40 (41) | 20 (33) | 32 (42) | 103 (34.5) | 156 (36.5) |
| IV | 16 (31) | 18 (16.5) | 31 (21.5) | 26 (18.1) | 12 (27) | 12 (12) | 5 (8) | 10 (13) | 64 (21.4) | 66 (15.5) |
| V | 1 (2) | 1 (0.9) | 7 (4.9) | 6 (4.2) | 1 (2) | 5 (5) | 1 (2) | 1 (1) | 10 (3.3) | 13 (3.0) |
| Length of hospital stay (days) † | 11 (7–24) | 11 (7–21) | 12 (7–23) | 10 (6–18) | 12 (8–21) | 12 (8–19) | 10 (7–21) | 13 (6–32) | 11 (7–23) | 11 (6–21) |
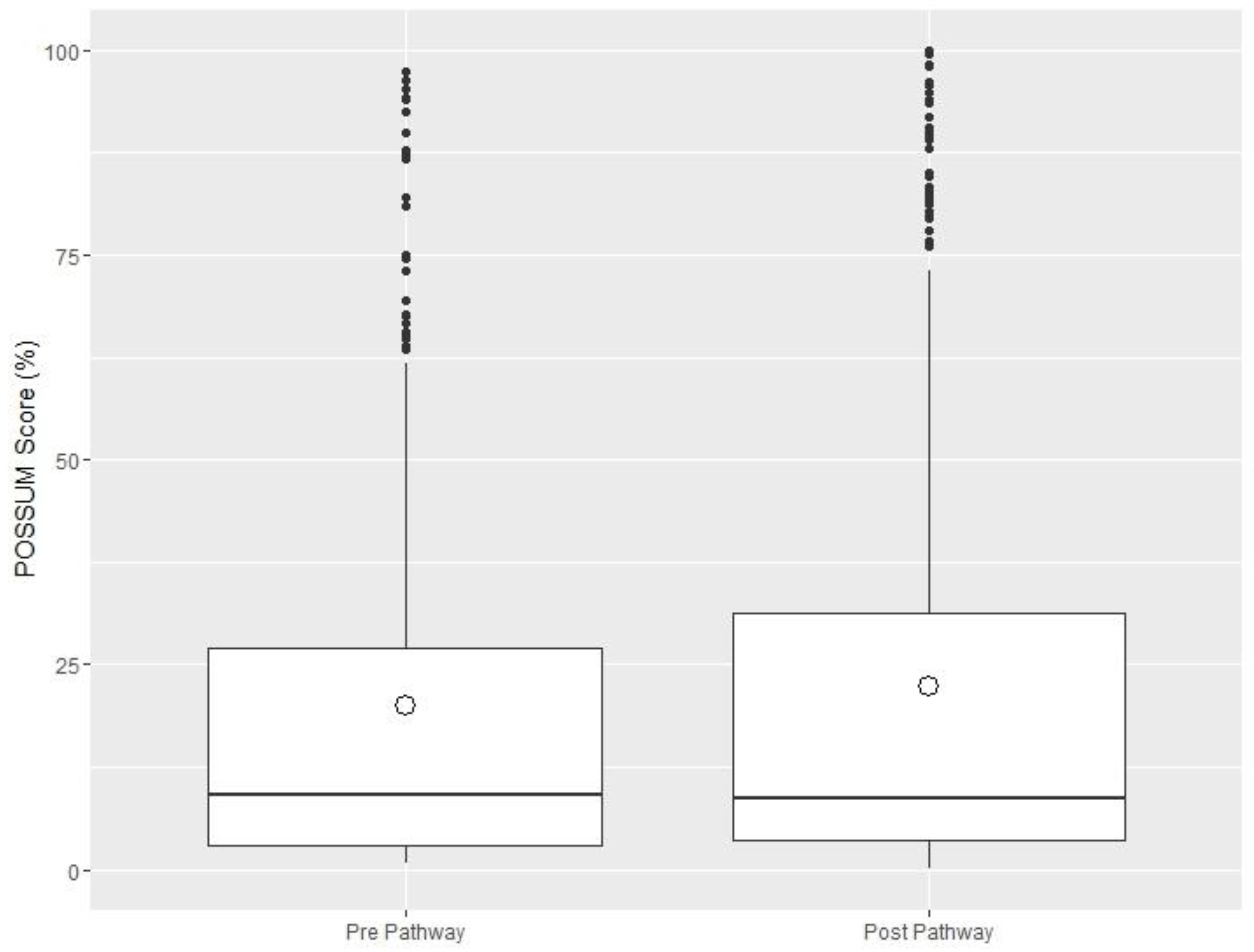
| P-POSSUM risk score * | 0.226 (0.282) | 0.251 (0.298) | 0.193 (0.234) | 0.267 (0.307) | 0.200 (0.207) | 0.179 (0.241) | 0.179 (0.237) | 0.159 (0.212) | 0.197 (0.239) | 0.223 (0.278) |
| P‡ | 0.730 | 0.140 | 0.764 | 0.755 | 0.395 | |||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doyle, J.F.; Sarnowski, A.; Saadat, F.; Samuels, T.L.; Huddart, S.; Quiney, N.; Dickinson, M.C.; McCormick, B.; deBrunner, R.; Preece, J.; et al. Does the Implementation of a Quality Improvement Care Bundle Reduce the Incidence of Acute Kidney Injury in Patients Undergoing Emergency Laparotomy? J. Clin. Med. 2019, 8, 1265. https://doi.org/10.3390/jcm8081265
Doyle JF, Sarnowski A, Saadat F, Samuels TL, Huddart S, Quiney N, Dickinson MC, McCormick B, deBrunner R, Preece J, et al. Does the Implementation of a Quality Improvement Care Bundle Reduce the Incidence of Acute Kidney Injury in Patients Undergoing Emergency Laparotomy? Journal of Clinical Medicine. 2019; 8(8):1265. https://doi.org/10.3390/jcm8081265
Chicago/Turabian StyleDoyle, James F., Alexander Sarnowski, Farzad Saadat, Theophilus L. Samuels, Sam Huddart, Nial Quiney, Matthew C. Dickinson, Bruce McCormick, Robert deBrunner, Jeremy Preece, and et al. 2019. "Does the Implementation of a Quality Improvement Care Bundle Reduce the Incidence of Acute Kidney Injury in Patients Undergoing Emergency Laparotomy?" Journal of Clinical Medicine 8, no. 8: 1265. https://doi.org/10.3390/jcm8081265