Blood Flow Restriction Increases the Neural Activation of the Knee Extensors During Very Low-Intensity Leg Extension Exercise in Cardiovascular Patients: A Pilot Study

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Participants
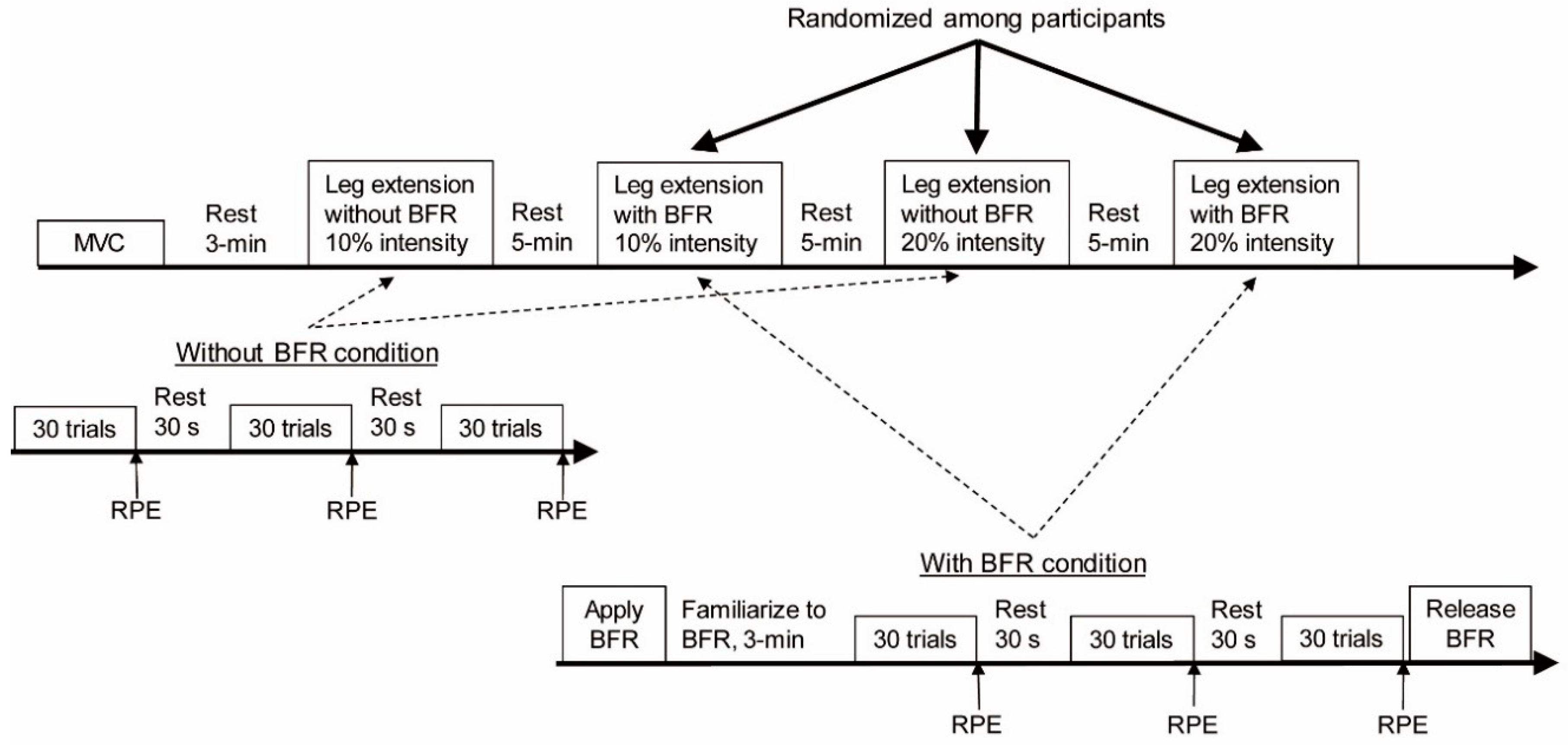
2.2. Experimental Protocol
2.3. Blood Flow Restriction
2.4. Data Collection
2.5. Data Analysis
2.6. Statistics
3. Results
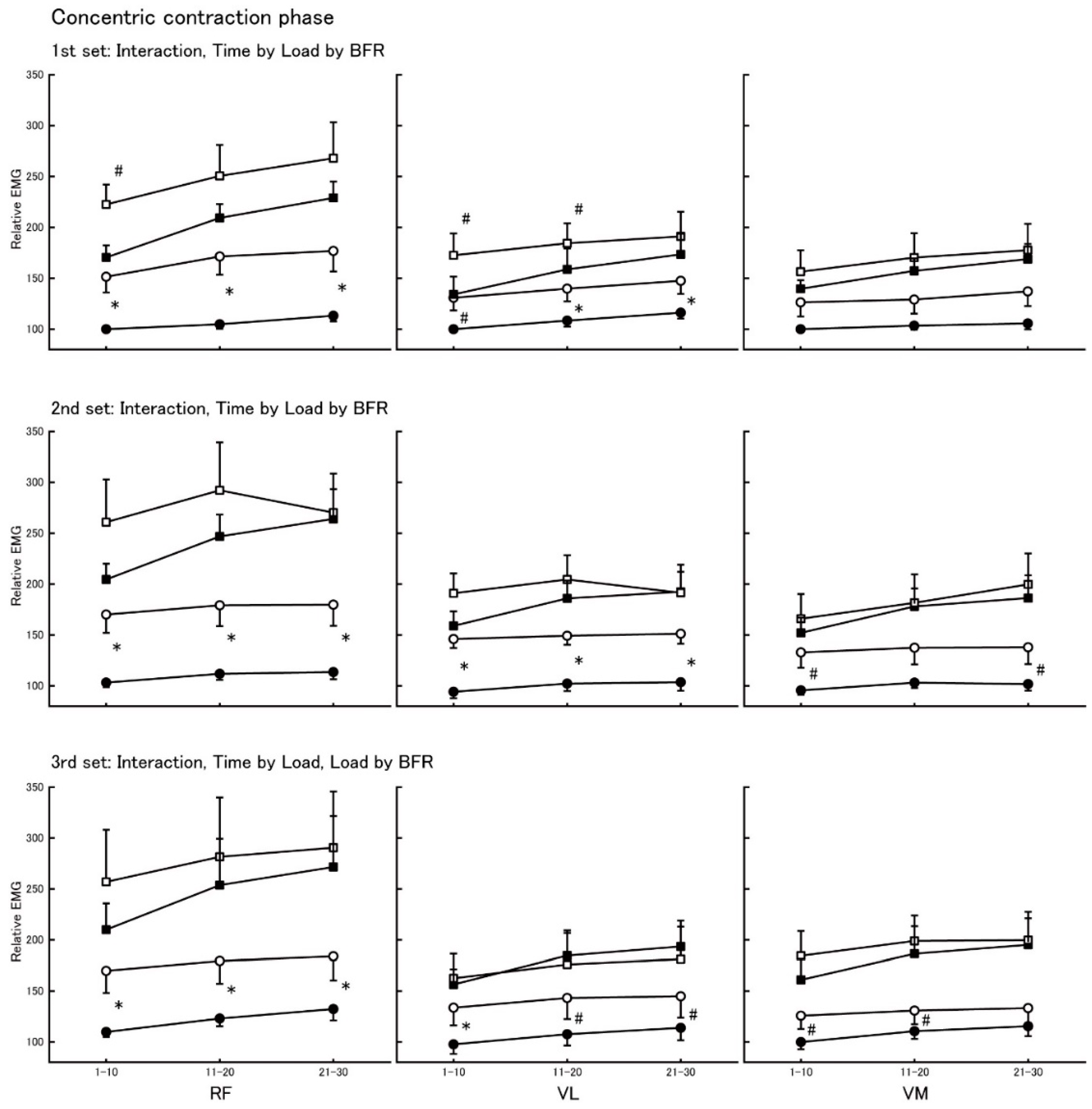
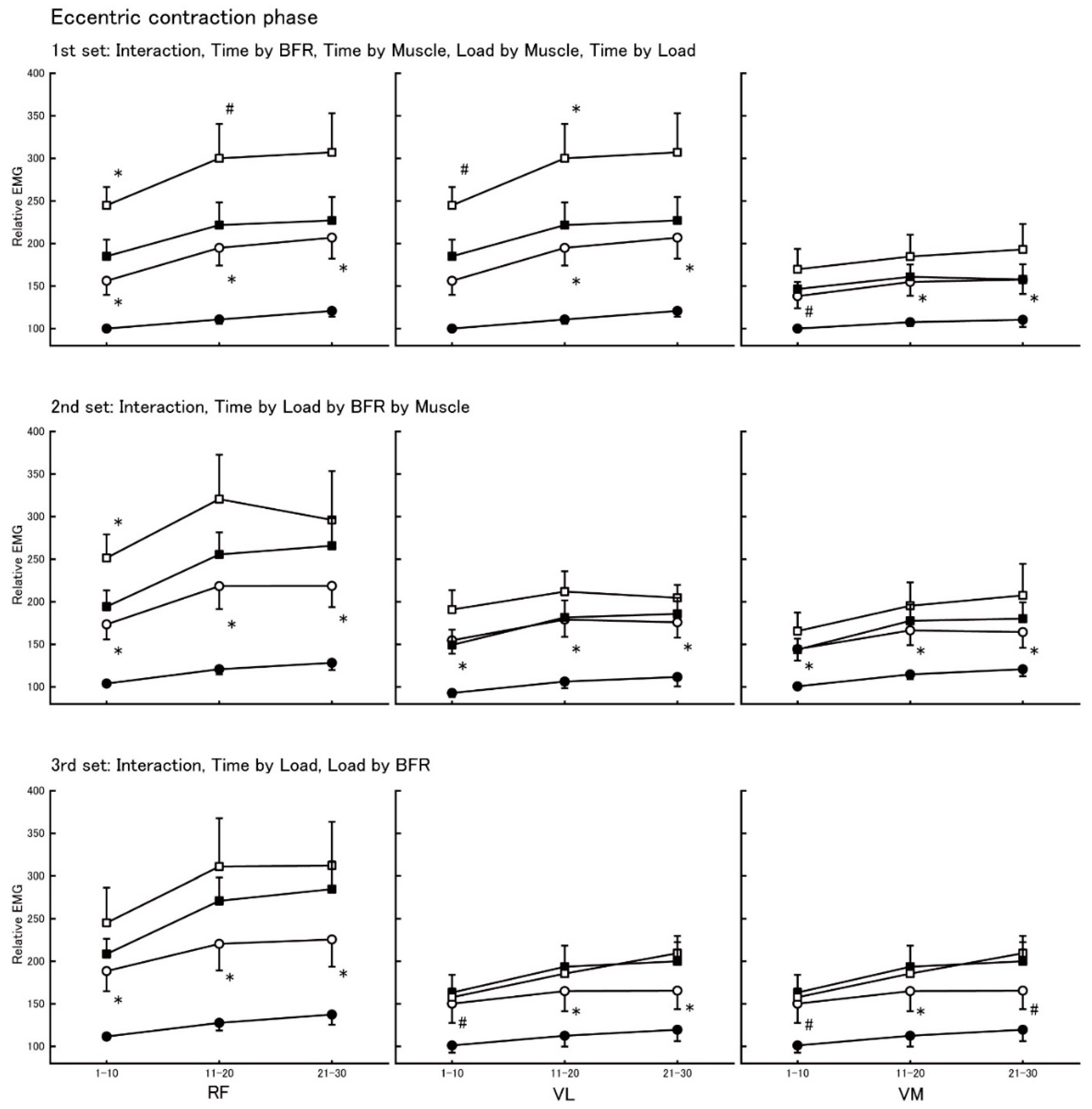
3.1. Electromyographic Activity During Concentric and Eccentric Contractions
3.2. Relative Electromyographic Changes in the Concentric Contraction Phase
3.3. Relative Electromyographic Changes in the Eccentric Contraction Phase
3.4. Subjective Exercise Intensity
3.5. Correlations Between Age and Relative EMG and RPE in the BFR Condition
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Price, K.J.; Gordon, B.A.; Bird, S.R.; Benson, A.C. A review of guidelines for cardiac rehabilitation exercise programmes: Is there an international consensus? Eur. J. Prev. Cardiol. 2016, 23, 1715–1733. [Google Scholar] [CrossRef]
- Williams, M.A.; Haskell, W.L.; Ades, P.A.; Amsterdam, E.A.; Bittner, V.; Franklin, B.A.; Gulanick, M.; Laing, S.T.; Stewart, K.J.; American Heart Association Council on Clinical Cardiology; et al. Resistance exercise in individuals with and without cardiovascular disease: 2007 update: A scientific statement from the american heart association council on clinical cardiology and council on nutrition, physical activity, and metabolism. Circulation 2007, 116, 572–584. [Google Scholar] [CrossRef] [PubMed]
- Atkins, J.M.; A Matthews, O.; Blomqvist, C.G.; Mullins, C.B. Incidence of arrhythmias induced by isometric and dynamic exercise. Br. Heart J. 1976, 38, 465–471. [Google Scholar] [CrossRef] [PubMed]
- JCS Joint Working Group. Guidelines for rehabilitation in patients with cardiovascular disease (JCS 2012). Circ. J. 2014, 78, 2022–2093. [Google Scholar] [CrossRef]
- Baechle, T.R.; Earle, R.W. Resistance training. In Essentials of Strength Training and Conditioning, 3rd ed.; Human Kinetics: Champaign, IL, USA, 2008; pp. 381–412. [Google Scholar]
- Nakajima, T.; Yasuda, T.; Sato, Y.; Morita, T.; Yamasoba, T. Effects of exercise and anti-aging. Anti-Aging Med. 2011, 8, 92–102. [Google Scholar] [CrossRef]
- Takarada, Y.; Takazawa, H.; Sato, Y.; Takebayashi, S.; Tanaka, Y.; Ishii, N. Effects of resistance exercise combined with moderate vascular occlusion on muscular function in humans. J. Appl. Physiol. 2000, 88, 2097–2106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearson, S.J.; Hussain, S.R. A review on the mechanisms of blood-flow restriction resistance training-induced muscle hypertrophy. Sports Med. 2015, 45, 187–200. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, T.; Kurano, M.; Sakagami, F.; Iida, H.; Fukumura, K.; Fukuda, T.; Takano, H.; Madarame, H.; Yasuda, T.; Nagata, T.; et al. Effects of low-intensity KAATSU resistance training on skeletal muscle size/strength and endurance capacity in patients with ischemic heart disease. Int. J. KAATSU Train. Res. 2010, 6, 1–7. [Google Scholar] [CrossRef]
- Yasuda, T.; Loenneke, J.P.; Thiebaud, R.S.; Abe, T. Effects of Blood Flow Restricted Low-Intensity Concentric or Eccentric Training on Muscle Size and Strength. PLOS ONE 2012, 7, e52843. [Google Scholar] [CrossRef]
- Landers, J. Maximum based on reps. Natl. Strength Cond. Assoc. 1984, 60, 60. [Google Scholar]
- Iida, H.; Kurano, M.; Takano, H.; Kubota, N.; Morita, T.; Meguro, K.; Sato, Y.; Abe, T.; Yamazaki, Y.; Uno, K.; et al. Hemodynamic and neurohumoral responses to the restriction of femoral blood flow by KAATSU in healthy subjects. Graefe’s Arch. Clin. Exp. Ophthalmol. 2007, 100, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, T.; Brechue, W.F.; Fujita, T.; Sato, Y.; Abe, T. Muscle Activation During Low-Intensity Muscle Contractions With Varying Levels of External Limb Compression. J. Sports Sci. Med. 2008, 7, 467–474. [Google Scholar] [PubMed]
- Yasuda, T.; Brechue, W.F.; Fujita, T.; Shirakawa, J.; Sato, Y.; Abe, T. Muscle activation during low-intensity muscle contractions with restricted blood flow. J. Sports Sci. 2009, 27, 479–489. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, T.; Fukumura, K.; Fukuda, T.; Iida, H.; Imuta, H.; Sato, Y.; Yamasoba, T.; Nakajima, T. Effects of low-intensity, elastic band resistance exercise combined with blood flow restriction on muscle activation. Scand. J. Med. Sci. Sports 2014, 24, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, E.L.; Barroso, R.; Silva-Batista, C.; Laurentino, G.C.; Loenneke, J.P.; Roschel, H.; Ugrinowitsch, C.; Tricoli, V. Blood flow restriction increases metabolic stress but decreases muscle activation during high-load resistance exercise. Muscle Nerve 2018, 57, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Wernbom, M.; Järrebring, R.; A Andreasson, M.; Augustsson, J. Acute Effects of Blood Flow Restriction on Muscle Activity and Endurance During Fatiguing Dynamic Knee Extensions at Low Load. J. Strength Cond. Res. 2009, 23, 2389–2395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keller-Ross, M.L.; Larson, M.; Johnson, B.D. Skeletal Muscle Fatigability in Heart Failure. Front. Physiol. 2019, 10, 10. [Google Scholar] [CrossRef] [PubMed]
- Bigland, B.; Lippold, O.C.J. The relation between force, velocity and integrated electrical activity in human muscles. J. Physiol. 1954, 123, 214–224. [Google Scholar] [CrossRef] [PubMed]
- Dalton, P.A.; Stokes, M.J. Acoustic myography reflects force changes during dynamic concentric and eccentric contractions of the human biceps brachii muscle. Graefe’s Arch. Clin. Exp. Ophthalmol. 1991, 63, 412–416. [Google Scholar] [CrossRef]
- Roots, H.; Offer, G.W.; Ranatunga, K.W. Comparison of the tension responses to ramp shortening and lengthening in intact mammalian muscle fibres: crossbridge and non-crossbridge contributions. J. Muscle Res. Cell Motil. 2007, 28, 123–139. [Google Scholar] [CrossRef] [PubMed]
- Pasquet, B.; Carpentier, A.; Duchateau, J. Specific modulation of motor unit discharge for a similar change in fascicle length during shortening and lengthening contractions in humans. J. Physiol. 2006, 577, 753–765. [Google Scholar] [CrossRef] [PubMed]
- Bigland-Ritchie, B.; Cafarelli, E.; Vøllestad, N.K. Fatigue of submaximal static contractions. Acta Physiol. Scand. Suppl. 1986, 556, 137–148. [Google Scholar] [PubMed]
- Moritani, T.; Muro, M.; Nagata, A. Intramuscular and surface electromyogram changes during muscle fatigue. J. Appl. Physiol. 1986, 60, 1179–1185. [Google Scholar] [CrossRef] [PubMed]
- Takarada, Y.; Nakamura, Y.; Aruga, S.; Onda, T.; Miyazaki, S.; Ishii, N. Rapid increase in plasma growth hormone after low-intensity resistance exercise with vascular occlusion. J. Appl. Physiol. 2000, 88, 61–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasuda, T.; Fukumura, K.; Uchida, Y.; Koshi, H.; Iida, H.; Masamune, K.; Yamasoba, T.; Sato, Y.; Nakajima, T. Effects of low-load, elastic band resistance training combined with blood flow restriction on muscle size and arterial stiffness in older adults. J. Gerontol. A. Biol. Sci. Med. Sci. 2015, 70, 950–958. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patient No, Sex | Age (years) | Height (cm) | Weight (kg) | LVEF | Drugs | Diagnosis | Days after Diagnosis |
|---|---|---|---|---|---|---|---|
| No 1, Male | 42 | 168.0 | 57.5 | 66% | ACEI, β-blocker | Post MVP | 482 |
| No 2, Male | 25 | 168.0 | 61.3 | 53% | Post AVR | 105 | |
| No 3, Male | 44 | 172.0 | 77.5 | 52% | ARB, β-blocker | Post AVR, TAP | 482 |
| No 4, Male | 66 | 170.7 | 68.0 | 20% | Post AVR, TAP | 476 | |
| No 5, Male | 70 | 171.4 | 67.5 | 46% | CCB, ACEI, β-blocker | Post BO | 293 |
| No 6, Male | 46 | 170.0 | 67.0 | 63% | Post AVR, TAP | 187 | |
| No 7, Female | 43 | 158.0 | 49.2 | 37% | β-blocker | CHF, MR, AR | 1018 |
| 10% Intensity | 20% Intensity | |||||||
|---|---|---|---|---|---|---|---|---|
| Without BFR | With BFR | Without BFR | With BFR | |||||
| CON | ECC | CON | ECC | CON | ECC | CON | ECC | |
| RF | 10.9 (1.8) | 7.7 (1.0) | 15.4 (2.2) | 12.6 (1.8) | 18.4 (2.5) | 13.5 (1.6) | 19.5 (2.3) | 15.8 (2.0) |
| VL | 15.1 (2.1) | 10.2 (1.1) | 20.3 (2.6) | 15.5 (2.2) | 23.6 (3.2) | 16.5 (2.3) | 25.2 (3.2) | 18.3 (1.9) |
| VM | 12.6 (1.6) | 9.3 (1.3) | 15.6 (2.0) | 12.4 (1.7) | 20.2 (3.0) | 14.3 (2.2) | 20.2 (3.0) | 15.8 (2.3) |
| AVG | 11.8 (2.0) * | 8.5 (1.1) | 16.2 (2.4) * | 12.7 (1.9) | 20.3 (3.2) * | 14.2 (2.1) | 21.6 (3.2) * | 16.6 (2.3) |
| 10% Intensity | 20% Intensity | |||
|---|---|---|---|---|
| Without BFR | With BFR | Without BFR | With BFR | |
| RPE | 10.7 (0.2) | 12.6 (0.5) † | 14.2 (0.4) †† | 15.7 (0.7) ††† |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishizaka, H.; Uematsu, A.; Mizushima, Y.; Nozawa, N.; Katayanagi, S.; Matsumoto, K.; Nishikawa, K.; Takahashi, R.; Arakawa, T.; Sawaguchi, T.; et al. Blood Flow Restriction Increases the Neural Activation of the Knee Extensors During Very Low-Intensity Leg Extension Exercise in Cardiovascular Patients: A Pilot Study. J. Clin. Med. 2019, 8, 1252. https://doi.org/10.3390/jcm8081252
Ishizaka H, Uematsu A, Mizushima Y, Nozawa N, Katayanagi S, Matsumoto K, Nishikawa K, Takahashi R, Arakawa T, Sawaguchi T, et al. Blood Flow Restriction Increases the Neural Activation of the Knee Extensors During Very Low-Intensity Leg Extension Exercise in Cardiovascular Patients: A Pilot Study. Journal of Clinical Medicine. 2019; 8(8):1252. https://doi.org/10.3390/jcm8081252
Chicago/Turabian StyleIshizaka, Hayato, Azusa Uematsu, Yuta Mizushima, Naohiro Nozawa, Satoshi Katayanagi, Kazuhisa Matsumoto, Kaori Nishikawa, Reiko Takahashi, Tomoe Arakawa, Tatsuya Sawaguchi, and et al. 2019. "Blood Flow Restriction Increases the Neural Activation of the Knee Extensors During Very Low-Intensity Leg Extension Exercise in Cardiovascular Patients: A Pilot Study" Journal of Clinical Medicine 8, no. 8: 1252. https://doi.org/10.3390/jcm8081252