A History of Trauma is Associated with Aggression, Depression, Non-Suicidal Self-Injury Behavior, and Suicide Ideation in First-Episode Psychosis

Abstract
:1. Introduction
1.1. Impact of Trauma on Non-Psychosis Populations
1.2. Impact of Trauma on Psychosis Populations
1.3. Impact of Trauma on Treatment Engagement for Psychosis Populations
1.4. Hypotheses
2. Methods
2.1. Participants
2.2. Measures
- No aggression.
- Verbal aggression: yelling, screaming, cussing, argumentative.
- Verbal aggression with threat: threatening harm towards self or others, but no weapon or action.
- Verbal Aggression with threat/weapon: verbally threatening other with weapon, but no action.
- Aggression against property: slamming doors, ripping clothing, throwing objects, breaking small objects, fire setting.
- Aggression against property accompanied by threat: destroying large items with threat to do more.
- Autoaggression: banging head, pounding walls, banging fists, pulling hair out.
- Autoaggression (Self-harmarm with injury): punching wall (e.g., breaking hand), cutting/burning self (NSSIB), and aborted suicide attempts.
- Physical aggression: pushing others, shaking others, hitting, kicking, scratching, and pinning down.
- Physical aggression (with threat or injury): hitting and kicking people with threat to do more, suicide attempts; causing injury, potentially or actually lethal.
2.3. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of Sample
3.2. Impact of Trauma on Clinical Characteristics
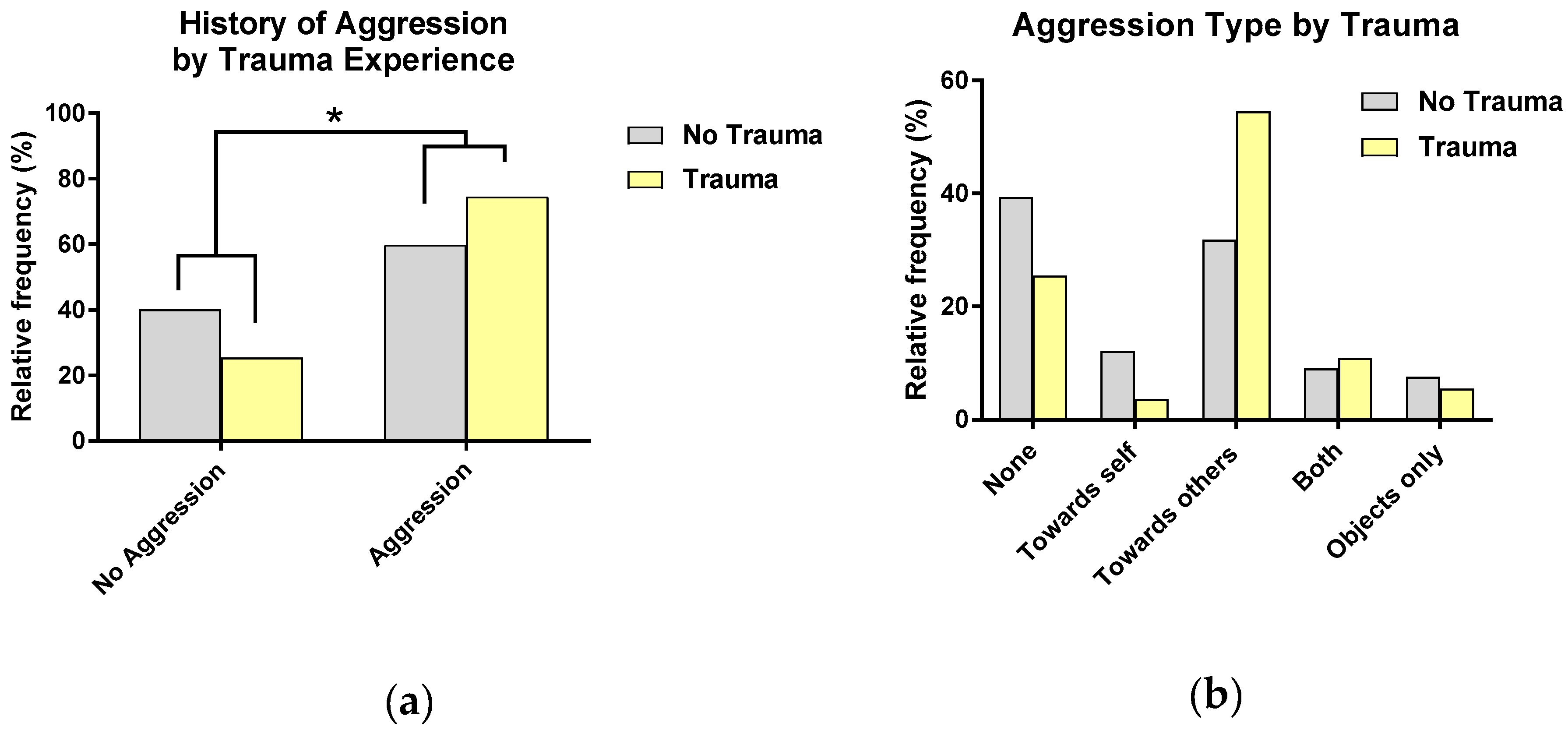
3.2.1. Aggression
3.2.2. Symptom Severity
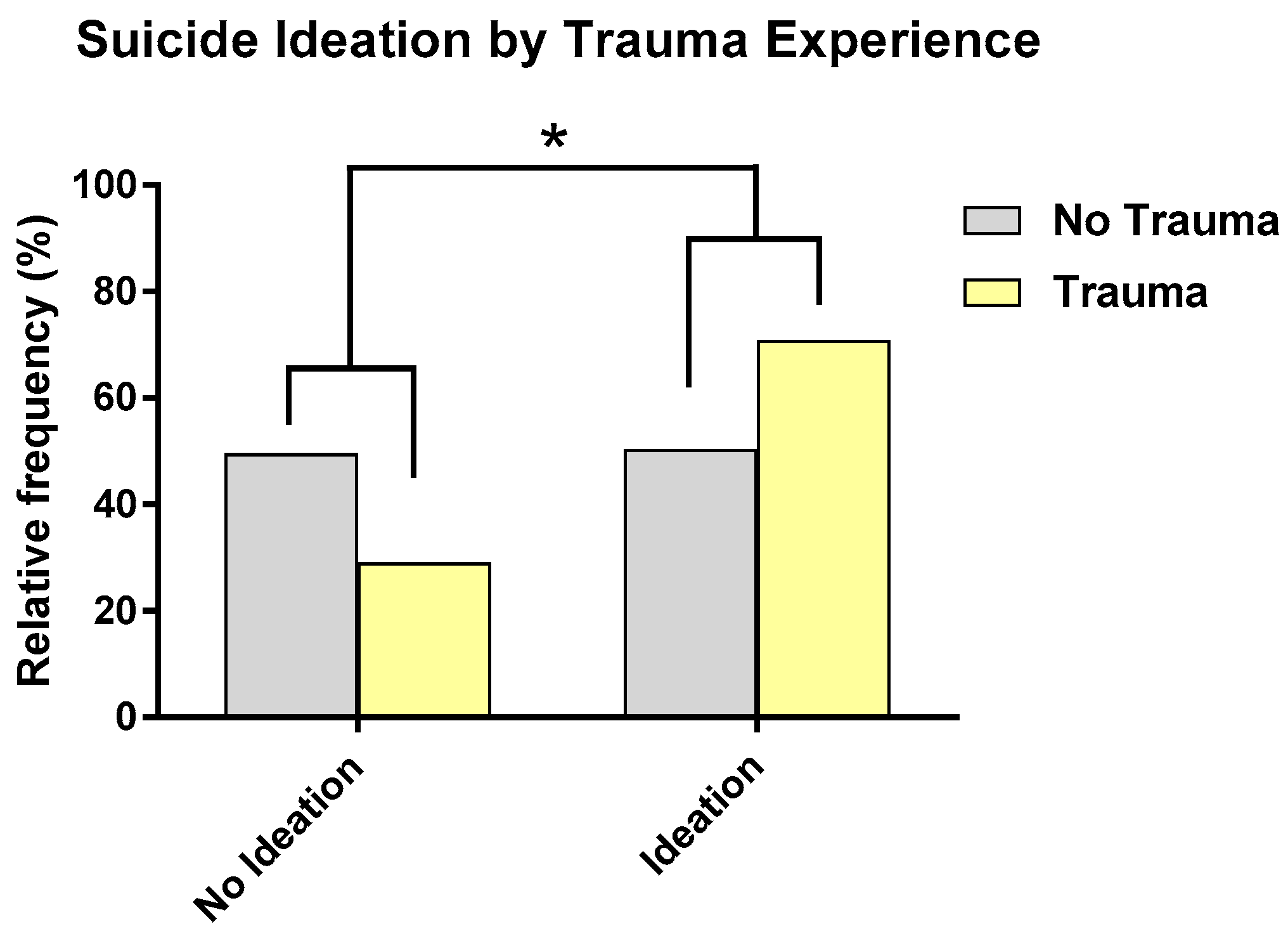
3.2.3. Suicide Ideation and Behavior
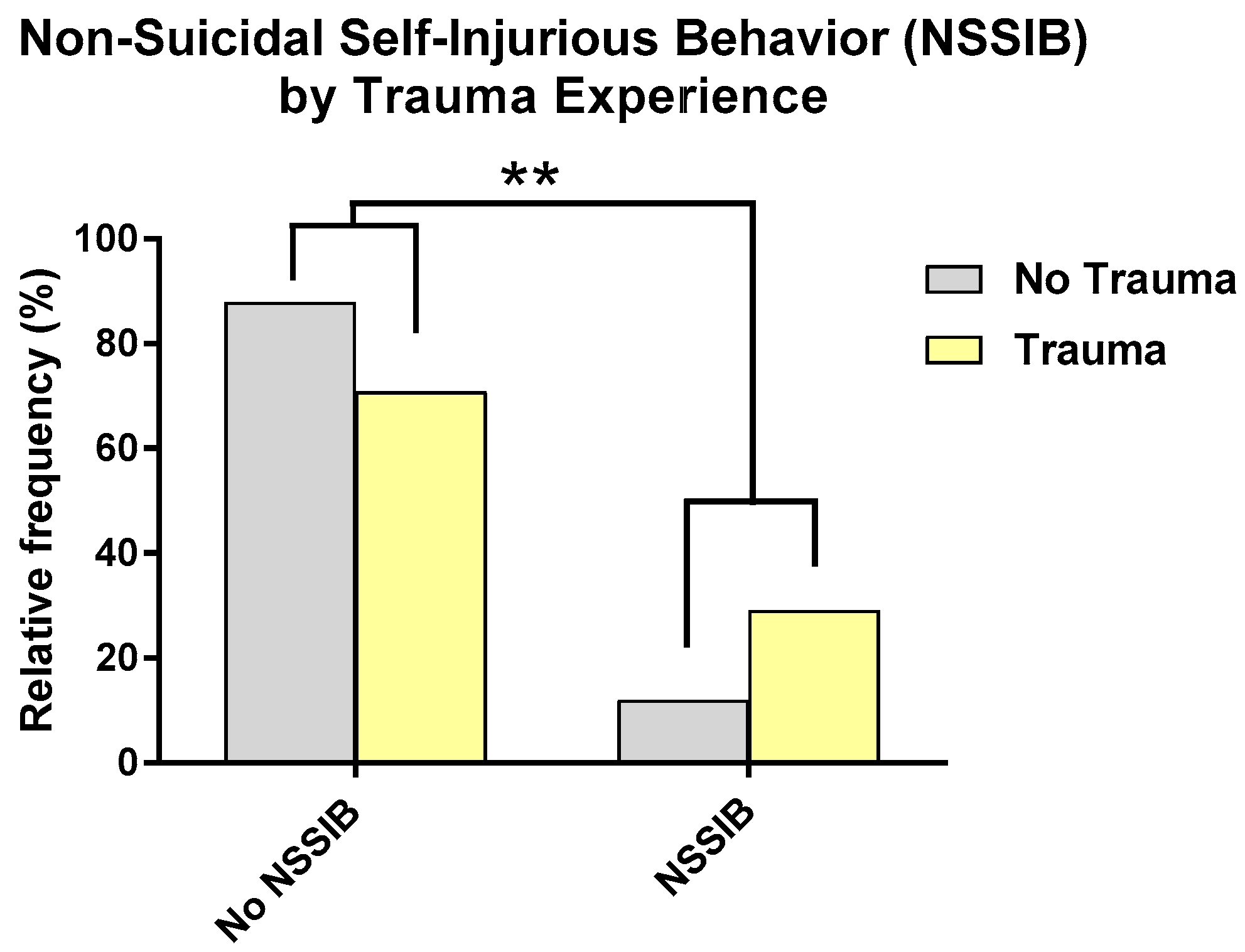
3.2.4. NSSIB
3.2.5. Social and Role Functioning
4. Discussion
4.1. Trauma and Symptoms
4.2. Trauma and Suicide Ideation and Behavior
4.3. Trauma and Aggression
4.4. Trauma and NSSIB
4.5. Trauma and Functioning
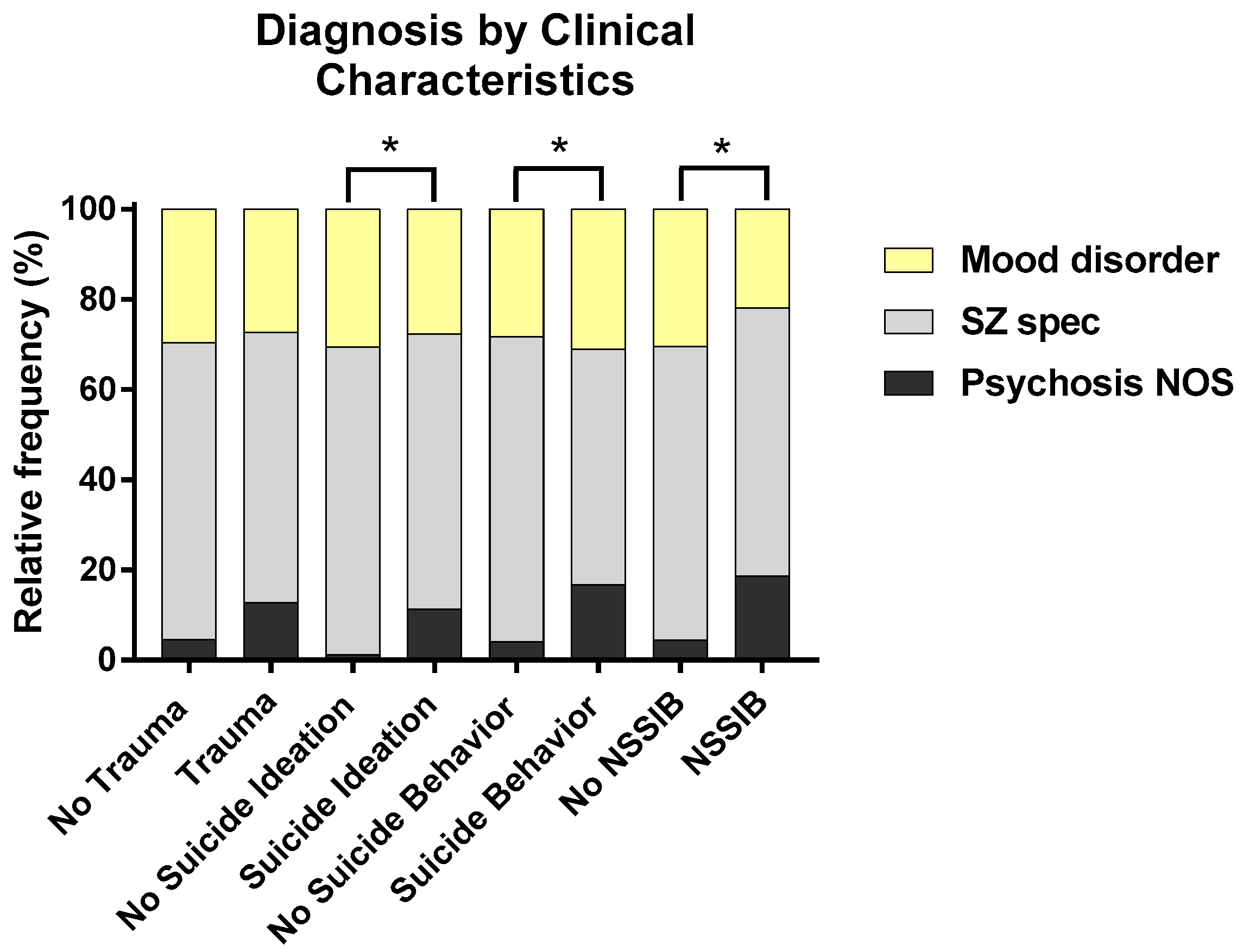
4.6. Trauma and Diagnosis
4.7. Implications for Theoretical Models of Psychosis
4.8. Implications for Treatment
4.9. Limitations and Strengths
4.10. Implications for Future Research
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Varese, F.; Smeets, F.; Drukker, M.; Lieverse, R.; Lataster, T.; Viechtbauer, W.; Read, J.; van Os, J.; Bentall, R.P. Childhood adversities increase the risk of psychosis: A meta-analysis of patient-control, prospective- and cross-sectional cohort studies. Schizophr. Bull. 2012, 38, 661–671. [Google Scholar] [CrossRef] [PubMed]
- Gibson, L.E.; Alloy, L.B.; Ellman, L.M. Trauma and the psychosis spectrum: A review of symptom specificity and explanatory mechanisms. Clin. Psychol. Rev. 2016, 49, 92–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, L.C.; Petruzzi, L.J.; Greene, M.C.; Mueser, K.T.; Borba, C.P.; Henderson, D.C. Posttraumatic stress disorder symptoms and social and occupational functioning of people with schizophrenia. J. Nerv. Ment. Dis. 2016, 204, 590–598. [Google Scholar] [CrossRef] [PubMed]
- Lecomte, T.; Spidel, A.; Leclerc, C.; MacEwan, G.W.; Greaves, C.; Bentall, R.P. Predictors and profiles of treatment non-adherence and engagement in services problems in early psychosis. Schizophr. Res. 2008, 102, 295–302. [Google Scholar] [CrossRef] [PubMed]
- De Kloet, L.; Starling, J.; Hainsworth, C.; Berntsen, E.; Chapman, L.; Hancock, K. Risk factors for self-harm in children and adolescents admitted to a mental health inpatient unit. Aust. N. Z. J. Psychiatry 2011, 45, 749–755. [Google Scholar] [CrossRef]
- Gladstone, G.; Parker, G.; Mitchell, P.; Malhi, G.; Wilhelm, K.; Austin, M. Implications of childhood trauma for depressed women: An analysis of pathways from childhood sexual abuse to deliberate self-harm and revictimization. Am. J. Psychiatry 2004, 161, 1417–1425. [Google Scholar] [CrossRef] [PubMed]
- Ford, J.; Chapman, J.; Connor, D.; Cruise, K. Complex trauma and aggression in secure juvenile justice settings. Crim. Justice Behav. 2012, 39, 694–724. [Google Scholar] [CrossRef]
- Ford, J.; Fournier, D. Psychological trauma and post-traumatic stress disorder among women in community mental health aftercare following psychiatric intensive care. J. Psychiatr. Intensive Care 2007, 3, 27–34. [Google Scholar] [CrossRef]
- Van Dorn, R.A.; Mustillo, S.; Elbogen, E.B.; Dorsey, S.; Swanson, J.W.; Swartz, M.S. The effects of early sexual abuse on adult risky sexual behaviors among persons with severe mental illness. Child Abus. Negl. 2005, 29, 1265–1279. [Google Scholar] [CrossRef]
- Carballo, J.J.; Harkavy-Friedman, J.; Burke, A.K.; Sher, L.; Baca-Garcia, E.; Sullivan, G.M.; Grunebaum, M.F.; Parsey, R.V.; Mann, J.J.; Oquendo, M.A. Family history of suicidal behavior and early traumatic experiences: Additive effect on suicidality and course of bipolar illness? J. Affect. Disord. 2008, 109, 57–63. [Google Scholar] [CrossRef] [Green Version]
- Mazza, J.; Reynolds, W. Exposure to violence in young inner-city adolescents: Relationships with suicidal ideation, depression and PTSD symptomatology. J. Abnorm. Child Psychol. 1999, 27, 203–213. [Google Scholar] [CrossRef] [PubMed]
- Grubaugh, A.L.; Zinzow, H.M.; Paul, L.; Egede, L.E.; Frueh, B.C. Trauma exposure and posttraumatic stress disorder in adults with severe mental illness: A critical review. Clin. Psychol. Rev. 2011, 31, 883–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopes Cardozo, B.; Talley, L.; Burton, A.; Crawford, C. Karenni refugees living in Thai-Burmese border camps: Traumatic experiences, mental health outcomes, and social functioning. Soc. Sci. Med. 2004, 58, 2637–2644. [Google Scholar] [CrossRef] [PubMed]
- Pagano, M.E.; Skodol, A.E.; Stout, R.L.; Shea, M.T.; Yen, S.; Grilo, C.M.; Sanislow, C.A.; Bender, D.S.; McGlashan, T.H.; Zanarini, M.C.; et al. Stressful life events as predictors of functioning: Findings from the collaborative longitudinal personality disorders study. Acta Psychiatr. Scand. 2004, 110, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Bolton, D.; Hill, J.; O’Ryan, D.; Udwin, O.; Boyle, S.; Yule, W. Long-term effects of psychological trauma on psychosocial functioning. J. Child Psychol. Psychiatry 2004, 45, 1007–1014. [Google Scholar] [CrossRef] [PubMed]
- Laffaye, C.; Cavella, S.; Drescher, K.; Rosen, C. Relationships among PTSD symptoms, social support, and support source in veterans with chronic PTSD. J. Trauma. Stress 2008, 21, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Mohammadzadeh, A.; Azadi, S.; King, S.; Khosravani, V.; Sharifi Bastan, F. Childhood trauma and the likelihood of increased suicidal risk in schizophrenia. Psychiatry Res. 2019, 275, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Grivel, M.M.; Leong, W.; Masucci, M.D.; Altschuler, R.A.; Arndt, L.Y.; Redman, S.L.; Yang, L.H.; Brucato, G.; Girgis, R.R. Impact of lifetime traumatic experiences on suicidality and likelihood of conversion in a cohort of individuals at clinical high-risk for psychosis. Schizophr. Res. 2018, 195, 549–553. [Google Scholar] [CrossRef]
- Ucok, A.; Bikmaz, S. The effects of childhood trauma in patients with first-episode schizophrenia. Acta Psychiatr. Scand. 2007, 116, 371–377. [Google Scholar] [CrossRef]
- Robinson, J.; Cotton, S.; Conus, P.; Schimmelmann, B.G.; McGorry, P.; Lambert, M. Prevalence and predictors of suicide attempt in an incidence cohort of 661 young people with first-episode psychosis. Aust. N. Z. J. Psychiatry 2009, 43, 149–157. [Google Scholar] [CrossRef]
- Sautter, F.; Brailey, K.; Uddo, M.; Hamilton, M.; Beard, M.; Borges, A. PTSD and comorbid psychotic disorder: Comparison with veterans diagnosed with PTSD or psychotic disorder. J. Trauma. Stress 1999, 12, 73–88. [Google Scholar] [CrossRef] [PubMed]
- Bosqui, T.J.; Shannon, C.; Tiernan, B.; Beattie, N.; Ferguson, J.; Mulholland, C. Childhood trauma and the risk of violence in adulthood in a population with a psychotic illness. J. Psychiatr. Res. 2014, 54, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Spidel, A.; Lecomte, T.; Greaves, C.; Sahlstrom, K.; Yuille, J.C. Early psychosis and aggression: Predictors and prevalence of violent behaviour amongst individuals with early onset psychosis. Int. J. Law Psychiatry 2010, 33, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Foley, S.; Kelly, B.; O’Callaghan, E.; Clarke, M.; Larkin, C. 0373 Duration of Untreated Psychosis and Violence at Presentation in Patients with First Episode Psychosis. Schizophr. Res. 2006, 86, S122–S123. [Google Scholar] [CrossRef]
- Merk, W.; Orobio de Castro, B.; Koops, W.; Matthys, W. The distinction between reactive and proactive aggression: Utility for theory, diagnosis and treatment? Eur. J. Dev. Psychol. 2005, 2, 197–220. [Google Scholar] [CrossRef]
- Bilgi, M.M.; Taspinar, S.; Aksoy, B.; Oguz, K.; Coburn, K.; Gonul, A.S. The relationship between childhood trauma, emotion recognition, and irritability in schizophrenia patients. Psychiatry Res. 2017, 251, 90–96. [Google Scholar] [CrossRef]
- Duhig, M.; Patterson, S.; Connell, M.; Foley, S.; Capra, C.; Dark, F.; Gordon, A.; Singh, S.; Hides, L.; McGrath, J.J.; et al. The prevalence and correlates of childhood trauma in patients with early psychosis. Aust. N. Z. J. Psychiatry 2015, 49, 651–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabínio, T.; Ricci, T.; Kahn, J.P.; Malaspina, D.; Moreira, H.; Veras, A.B. Early trauma, attachment experiences and comorbidities in schizophrenia. Trends Psychiatry Psychother. 2018, 40, 179–184. [Google Scholar] [CrossRef] [Green Version]
- Bentall, R.P.; de Sousa, P.; Varese, F.; Wickham, S.; Sitko, K.; Haarmans, M.; Read, J. From adversity to psychosis: Pathways and mechanisms from specific adversities to specific symptoms. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 1011–1022. [Google Scholar] [CrossRef]
- Kraan, T.; Velthorst, E.; Smit, F.; de Haan, L.; van der Gaag, M. Trauma and recent life events in individuals at ultra high risk for psychosis: Review and meta-analysis. Schizophr. Res. 2015, 161, 143–149. [Google Scholar] [CrossRef]
- Hodgins, S.; Lincoln, T.; Mak, T. Experiences of victimisation and depression are associated with community functioning among men with schizophrenia. Soc. Psychiatry Psychiatr. Epidemiol. 2009, 44, 448–457. [Google Scholar] [CrossRef] [PubMed]
- Lysaker, P.; Meyer, P.; Evans, J.; Clements, C.; Marks, K. Childhood sexual trauma and psychosocial functioning in adults with schizophrenia. Psychiatr. Serv. 2001, 52, 1485–1488. [Google Scholar] [CrossRef] [PubMed]
- Conus, P.; Cotton, S.; Schimmelmann, B.G.; McGorry, P.D.; Lambert, M. Pretreatment and outcome correlates of sexual and physical trauma in an epidemiological cohort of first-episode psychosis patients. Schizophr. Bull. 2010, 36, 1105–1114. [Google Scholar] [CrossRef] [PubMed]
- Stain, H.J.; Brønnick, K.; Hegelstad, W.T.V.; Joa, I.; Johannessen, J.O.; Langeveld, J.; Mawn, L.; Larsen, T.K. Impact of interpersonal trauma on the social functioning of adults with first-episode psychosis. Schizophr. Bull. 2013, 40, 1491–1498. [Google Scholar] [CrossRef] [PubMed]
- Cotter, J.; Kaess, M.; Yung, A.R. Childhood trauma and functional disability in psychosis, bipolar disorder and borderline personality disorder: A review of the literature. Ir. J. Psychol. Med. 2015, 32, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Mayo, D.; Corey, S.; Kelly, L.H.; Yohannes, S.; Youngquist, A.L.; Stuart, B.K.; Niendam, T.A.; Loewy, R.L. The role of trauma and stressful life events among individuals at clinical high risk for psychosis: A review. Front. Psychiatry 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- Neacsiu, A.D.; Fang, C.M.; Rodriguez, M.; Rosenthal, M.Z. Suicidal behavior and problems with emotion regulation. Suicide Life Threat. Behav. 2018, 48, 52–74. [Google Scholar] [CrossRef]
- Mikolajczak, M.; Petrides, K.V.; Hurry, J. Adolescents choosing self-harm as an emotion regulation strategy: The protective role of trait emotional intelligence. Br. J. Clin. Psychol. 2009, 48, 181–193. [Google Scholar] [CrossRef]
- Roberton, T.; Daffern, M.; Bucks, R.S. Emotion regulation and aggression. Aggress. Violent Behav. 2012, 17, 72–82. [Google Scholar] [CrossRef]
- Lysaker, P.; Outcalt, S.; Ringer, J. Clinical and psychosocial significance of trauma history in schizophrenia spectrum disorders. Expert Rev. Neurother. 2010, 10, 1143–1151. [Google Scholar] [CrossRef]
- Mondelli, V.; Ciufolini, S.; Belvederi Murri, M.; Bonaccorso, S.; Di Forti, M.; Giordano, A.; Marques, T.R.; Zunszain, P.A.; Morgan, C.; Murray, R.M.; et al. Cortisol and inflammatory biomarkers predict poor treatment response in first episode psychosis. Schizophr. Bull. 2015, 41, 1162–1170. [Google Scholar] [CrossRef] [PubMed]
- First, M.B.; Spitzer, R.L.; Gibbon, M.; Williams, J.B. Structured Clinical Interview for DSM-IV-TR Axis I Disorders, Research Version, Patient Edition; (SCID-I/P); New York State Psychiatric Institute: New York, NY, USA, 2002. [Google Scholar]
- Kaufman, J.; Birmaher, B.; Brent, D.; Rao, U.; Flynn, C.; Moreci, P.; Williamson, D.; Ryan, N. Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): Initial reliability and validity data. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 980–988. [Google Scholar] [CrossRef] [PubMed]
- Stano, J.F. Wechsler abbreviated scale of intelligence. Rehabil. Couns. Bull. 2004, 48, 56–57. [Google Scholar] [CrossRef]
- Lopez-Garcia, P.; Ashby, S.; Patel, P.; Pierce, K.; Meyer, M.; Rosenthal, A.; Titone, M.; Carter, C.; Niendam, T. Clinical and neurodevelopmental correlates of aggression in early psychosis. Schizophr. Res. 2019. Submitted. [Google Scholar]
- Miller, T.J.; McGlashan, T.H.; Rosen, J.L.; Cadenhead, K.; Ventura, J.; McFarlane, W.; Perkins, D.O.; Pearlson, G.D.; Woods, S.W. Prodromal assessment with the structured interview for prodromal syndromes and the scale of prodromal symptoms: Predictive validity, interrater reliability, and training to reliability. Schizophr. Bull. 2003, 29, 703–715. [Google Scholar] [CrossRef] [PubMed]
- Steel, C.; Doukani, A.; Hardy, A. The PCL as a brief screen for posttraumatic stress disorder within schizophrenia. Int. J. Psychiatry Clin. Pract. 2017, 21, 148–150. [Google Scholar] [CrossRef] [PubMed]
- Posner, K.; Brown, G.K.; Stanley, B.; Brent, D.A.; Yershova, K.V.; Oquendo, M.A.; Currier, G.W.; Melvin, G.A.; Greenhill, L.; Shen, S. The Columbia–Suicide Severity Rating Scale: Initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am. J. Psychiatry 2011, 168, 1266–1277. [Google Scholar] [CrossRef] [PubMed]
- Lukoff, D.; Nuechterlein, K.; Ventura, J. Manual for the expanded brief psychiatric rating scale. Schizophr. Bull. 1986, 12, 594–602. [Google Scholar]
- Cornblatt, B.A.; Auther, A.M.; Niendam, T.; Smith, C.W.; Zinberg, J.; Bearden, C.E.; Cannon, T.D. Preliminary findings for two new measures of social and role functioning in the prodromal phase of schizophrenia. Schizophr. Bull. 2007, 33, 688–702. [Google Scholar] [CrossRef] [PubMed]
- Shafer, A.; Dazzi, F.; Ventura, J. Factor structure of the Brief Psychiatric Rating Scale - Expanded (BPRS-E) in a large hospitalized sample. J. Psychiatr. Res. 2017, 93, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Keane, S.; Szigeti, A.; Fanning, F.; Clarke, M. Are patterns of violence and aggression at presentation in patients with first-episode psychosis temporally stable? A comparison of 2 cohorts. Early Interv. Psychiatry 2018, 10.1111/eip.12694. [Google Scholar] [CrossRef] [PubMed]
- Sorgi, P.; Ratey, J.J.; Knoedler, D.W.; Markert, R.J.; Reichman, M. Rating aggression in the clinical setting: A retrospective adaptation of the Overt Aggression Scale: Preliminary results. J. Neuropsychiatry Clin. Neurosci. 1991, 3, S52–S56. [Google Scholar] [PubMed]
- IBM Corp. IBM SPSS Statistics for Windows; Version 25; IBM Corp.: Armonk, NY, USA, 2017. [Google Scholar]
- Spauwen, J.; Krabbendam, L.; Lieb, R.; Wittchen, H.; Van Os, J. Impact of psychological trauma on the development of psychotic symptoms: Relationship with psychosis proneness. Br. J. Psychiatry 2006, 188, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.L.; Kelly, M.; Kimhy, D.; Harkavy-Friedman, J.M.; Khan, S.; Messinger, J.W.; Schobel, S.; Goetz, R.; Malaspina, D.; Corcoran, C. Childhood trauma and prodromal symptoms among individuals at clinical high risk for psychosis. Schizophr. Res. 2009, 108, 176–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, M.O.; Crawford, E.; Del Castillo, D. Childhood emotional maltreatment and later psychological distress among college students: The mediating role of maladaptive schemas. Child Abus. Negl. 2009, 33, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Bahk, Y.C.; Jang, S.K.; Choi, K.H.; Lee, S.H. The Relationship between childhood trauma and suicidal ideation: Role of maltreatment and potential mediators. Psychiatry Investig. 2017, 14, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Grattan, R.; Tully, L.; Lesh, T.; Carter, C.; Niendam, T. F64. Exploring the Role of Emotion Dysregulation and Impulsivity on Suicidal Ideation and Behavior within an Early Psychosis Population. Schizophr. Bull. 2019, 45, S279. [Google Scholar] [CrossRef]
- Lansford, J.E.; Miller-Johnson, S.; Berlin, L.J.; Dodge, K.A.; Bates, J.E.; Pettit, G.S. Early physical abuse and later violent delinquency: A prospective longitudinal study. Child Maltreat 2007, 12, 233–245. [Google Scholar] [CrossRef]
- Witt, K.; Van Dorn, R.; Fazel, S. Risk factors for violence in psychosis: Systematic review and meta-regression analysis of 110 studies. PLoS ONE 2013, 8, e55942. [Google Scholar] [CrossRef]
- Brady, K.T.; Back, S.E.; Coffey, S.F. Substance Abuse and Posttraumatic Stress Disorder. Curr. Dir. Psychol. Sci. 2004, 13, 206–209. [Google Scholar] [CrossRef]
- Fliege, H.; Lee, J.R.; Grimm, A.; Klapp, B.F. Risk factors and correlates of deliberate self-harm behavior: A systematic review. J. Psychosom. Res. 2009, 66, 477–493. [Google Scholar] [CrossRef] [PubMed]
- Roy, A. Childhood trauma and impulsivity. Possible relevance to suicidal behavior. Arch. Suicide Res. 2005, 9, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Zetterqvist, M.; Lundh, L.-G.; Dahlström, Ö.; Svedin, C.G. Prevalence and function of non-suicidal self-injury (NSSI) in a community sample of adolescents, using suggested DSM-5 criteria for a potential NSSI disorder. J. Abnorm. Child Psychol. 2013, 41, 759–773. [Google Scholar] [CrossRef] [PubMed]
- Loewy, R.L.; Corey, S.; Amirfathi, F.; Dabit, S.; Fulford, D.; Pearson, R.; Hua, J.P.Y.; Schlosser, D.; Stuart, B.K.; Mathalon, D.H.; et al. Childhood trauma and clinical high risk for psychosis. Schizophr. Res. 2019, 205, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Trauelsen, A.M.; Bendall, S.; Jansen, J.E.; Nielsen, H.-G.L.; Pedersen, M.B.; Trier, C.H.; Haahr, U.H.; Simonsen, E. Childhood adversities: Social support, premorbid functioning and social outcome in first-episode psychosis and a matched case-control group. Aust. N. Z. J. Psychiatry 2016, 50, 770–782. [Google Scholar] [CrossRef] [PubMed]
- Alameda, L.; Ferrari, C.; Baumann, P.; Gholam-Rezaee, M.; Do, K.; Conus, P. Childhood sexual and physical abuse: Age at exposure modulates impact on functional outcome in early psychosis patients. Psychol. Med. 2015, 45, 2727–2736. [Google Scholar] [CrossRef]
- Palmier-Claus, J.; Berry, K.; Darrell-Berry, H.; Emsley, R.; Parker, S.; Drake, R.; Bucci, S. Childhood adversity and social functioning in psychosis: Exploring clinical and cognitive mediators. Psychiatry Res. 2016, 238, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Dunn, E.C.; Nishimi, K.; Powers, A.; Bradley, B. Is developmental timing of trauma exposure associated with depressive and post-traumatic stress disorder symptoms in adulthood? J. Psychiatr. Res. 2017, 84, 119–127. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Van den Berg, D.P.; van der Vleugel, B.; de Bont, P.; Staring, A.; Kraan, T.; Ising, H.; de Roos, C.; de Jongh, A.; van Minnen, A.; van der Gaag, M. Predicting trauma-focused treatment outcome in psychosis. Schizophr. Res. 2016, 176, 239–244. [Google Scholar] [CrossRef]
- Van den Berg, D.P.; van der Gaag, M. Treating trauma in psychosis with EMDR: A pilot study. J. Behav. Ther. Exp. Psychiatry 2012, 43, 664–671. [Google Scholar] [CrossRef]
- Alameda, L.; Golay, P.; Baumann, P.S.; Progin, P.; Mebdouhi, N.; Elowe, J.; Ferrari, C.; Do, K.Q.; Conus, P. Mild Depressive Symptoms Mediate the Impact of Childhood Trauma on Long-Term Functional Outcome in Early Psychosis Patients. Schizophr. Bull. 2017, 43, 1027–1035. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, A.; Johnston, M.; Bureau, Y. Stigma of mental illness-2: Non-compliance and intervention. Mens Sana Monogr. 2012, 10, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Swartz, M.S.; Swanson, J.W.; Hiday, V.A.; Borum, R.; Wagner, H.R.; Burns, B.J. Violence and severe mental illness: The effects of substance abuse and nonadherence to medication. Am. J. Psychiatry 1998, 155, 226–231. [Google Scholar] [PubMed]
- Caqueo-Urízar, A.; Rus-Calafell, M.; Urzúa, A.; Escudero, J.; Gutiérrez-Maldonado, J. The role of family therapy in the management of schizophrenia: Challenges and solutions. Neuropsychiatr. Dis. Treat. 2015, 11, 145–151. [Google Scholar] [PubMed]
- Onwumere, J.; Grice, S.; Garety, P.; Bebbington, P.; Dunn, G.; Freeman, D.; Fowler, D.; Kuipers, E. Caregiver reports of patient-initiated violence in psychosis. Can. J. Psychiatry 2014, 59, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Have, M.T.; de Graaf, R.; Van Dorsselaer, S.; Verdurmen, J.; van’t Land, H.; Vollebergh, W.; Beekman, A. Incidence and course of suicidal ideation and suicide attempts in the general population. Can. J. Psychiatry 2009, 54, 824–833. [Google Scholar] [CrossRef] [PubMed]
- Weems, C.F.; Carrion, V.G. The association between PTSD symptoms and salivary cortisol in youth: The role of time since the trauma. J. Trauma. Stress 2007, 20, 903–907. [Google Scholar] [CrossRef]
- Shevlin, M.; Houston, J.E.; Dorahy, M.J.; Adamson, G. Cumulative traumas and psychosis: An analysis of the national comorbidity survey and the British Psychiatric Morbidity Survey. Schizophr. Bull. 2007, 34, 193–199. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No Trauma (n = 132) | History of Trauma (n = 55) | ||
|---|---|---|---|
| N (%) | |||
| Sex | Male | 98 (74.2%) | 37 (67.3%) |
| Female | 34 (25.8%) | 18 (32.7%) | |
| Race | Caucasian | 87 (65.9%) | 31 (56.4%) |
| African American | 13 (9.8%) | 13 (23.6%) | |
| Asian | 15 (11.4%) | 5 (9.1%) | |
| Pacific Islander | 4 (3.0%) | 0 (0.0%) | |
| American Indian | 1 (0.8%) | 0 (0.0%) | |
| Other | 1 (0.8%) | 0 (0.0%) | |
| More than one race | 11 (8.3%) | 6 (10.9%) | |
| Ethnicity | Hispanic | 27 (20.5%) | 10 (18.2%) |
| DSM-IV Diagnosis | Schizophrenia Spectrum | 87 (65.9%) | 33 (60.0%) |
| Mood with Psychotic Features | 39 (29.5%) | 15 (27.3%) | |
| Psychotic Disorder NOS * | 6 (4.5%) | 7 (12.7%) | |
| Mean (SD) | |||
| Age | Years | 19.41 (4.11) | 18.91 (3.94) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grattan, R.E.; Lara, N.; Botello, R.M.; Tryon, V.L.; Maguire, A.M.; Carter, C.S.; Niendam, T.A. A History of Trauma is Associated with Aggression, Depression, Non-Suicidal Self-Injury Behavior, and Suicide Ideation in First-Episode Psychosis. J. Clin. Med. 2019, 8, 1082. https://doi.org/10.3390/jcm8071082
Grattan RE, Lara N, Botello RM, Tryon VL, Maguire AM, Carter CS, Niendam TA. A History of Trauma is Associated with Aggression, Depression, Non-Suicidal Self-Injury Behavior, and Suicide Ideation in First-Episode Psychosis. Journal of Clinical Medicine. 2019; 8(7):1082. https://doi.org/10.3390/jcm8071082
Chicago/Turabian StyleGrattan, Rebecca E., Natalia Lara, Renata M. Botello, Valerie L. Tryon, Adrienne M. Maguire, Cameron S. Carter, and Tara A. Niendam. 2019. "A History of Trauma is Associated with Aggression, Depression, Non-Suicidal Self-Injury Behavior, and Suicide Ideation in First-Episode Psychosis" Journal of Clinical Medicine 8, no. 7: 1082. https://doi.org/10.3390/jcm8071082