Caregiver Burden and Sleep Quality in Dependent People’s Family Caregivers

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Measures
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Characteristics of the Family Caregivers, the Care Recipients and the Care Situation
3.2. Subjective Sleep Quality
3.3. Associated Variables to Sleep Quality in Family Caregivers
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Brodaty, H.; Donkin, M. Family caregivers of people with dementia. Dialogues Clin. Neurosci. 2009, 11, 217–228. [Google Scholar] [PubMed]
- Oliveira, D.; Sousa, L.; Orrell, M. Improving health-promotion self-care in family carers of people with dementia: A review of interventions. Clin. Interv. Aging 2019, 14, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Bastawrous, M. Caregiver burden. A critical discussion. Int. J. Nurs. Stud. 2013, 50, 431–441. [Google Scholar] [CrossRef] [PubMed]
- Carretero, S.; Garcés, J.; Ródenas, F.; Sanjosé, V. The informal caregiver’s burden of dependent people: Theory and empirical review. Arch. Gerontol. Geriatr. 2009, 49, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Mausbach, B.T.; Chattillion, E.A.; Roepke, S.K.; Patterson, T.L.; Grant, I. A comparison of psychosocial outcomes in elderly Alzheimer caregivers and noncaregivers. Am. J. Geriatr. Psychiatry 2013, 21, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Abreu, W.; Rodrigues, T.; Sequeira, C.; Pires, R.; Sanhudo, A. The experience of psychological distress in family caregivers of people with dementia: A cross-sectional study. Perspect. Psychiatr. Care 2018, 54, 317–323. [Google Scholar] [CrossRef]
- Joling, K.J.; van Marwijk, H.W.; Veldhuijzen, A.E.; van der Horst, H.E.; Scheltens, P.; Smit, H.F.; van Hout, H.P. The two-year incidence of depression and anxiety disorders in spousal caregivers of persons with dementia: Who is at the greatest risk? Am. J. Geriatr. Psychiatry 2015, 23, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Li, C.; Shi, Z.; Wang, X.; Zhou, Y.; Liu, S.; Liu, J.; Yu, T.; Ji, Y. Caregiver burden and prevalence of depression, anxiety and sleep disturbances in Alzheimer’s disease caregivers in China. J. Clin. Nurs. 2017, 26, 1291–1300. [Google Scholar] [CrossRef]
- Torres, A.; Blanco, V.; Vázquez, F.L.; Díaz, O.; Otero, P.; Hermida, E. Prevalence of major depressive episodes in non-professional caregivers. Psychiatry Res. 2015, 226, 333–339. [Google Scholar] [CrossRef]
- Roth, D.L.; Perkins, M.; Wadley, V.G.; Temple, E.; Haley, W.E. Family caregiving and emotional strain: Associations with psychological health in a national sample of community-dwelling middle-aged and older adults. Qual. Life Res. 2009, 18, 679–688. [Google Scholar] [CrossRef]
- Schulz, R.; Beach, S.R. Caregiving as a risk factor for mortality: The Caregiver Health Effects Study. JAMA 1999, 282, 2215–2219. [Google Scholar] [CrossRef]
- Von Känel, R.; Mausbach, B.T.; Dimsdale, J.E.; Ziegler, M.G.; Mills, P.J.; Allison, M.A.; Patterson, T.L.; Ancoli-Israel, S.; Grant, I. Refining caregiver vulnerability for clinical practice: Determinants of self-rated health in spousal dementia caregivers. BMC Geriatr. 2019, 19, 18. [Google Scholar] [CrossRef]
- Capistrant, B.D.; Moon, J.R.; Berkman, L.F.; Glymour, M.M. Current and long-term spousal caregiving and onset of cardiovascular disease. J. Epidemiol. Community Health 2012, 66, 951–956. [Google Scholar] [CrossRef]
- Damjanovic, A.K.; Yang, Y.; Glaser, R.; Kiecolt-Glaser, J.K.; Nguyen, H.; Laskowski, B.; Zou, Y.; Beversdorf, D.Q.; Weng, N.P. Accelerated telomere erosion is associated with a declining inmmune function of caregivers of Alzheimer’s disease patients. J. Immunol. 2007, 179, 4249–4254. [Google Scholar] [CrossRef]
- McCurry, S.M.; Logsdon, R.G.; Teri, L.; Vitiello, M.V. Sleep disturbances in caregivers of persons with dementia: Contributing factors and treatment implications. Sleep Med. Rev. 2007, 11, 143–153. [Google Scholar] [CrossRef] [Green Version]
- McKibbin, C.L.; Ancoli-Israel, S.; Dimsdale, J.; Archuleta, C.; von Känel, R.; Mills, P.; Patterson, T.L.; Grant, I. Sleep in spousal caregivers of people with Alzheimer’s disease. Sleep 2005, 28, 1245–1250. [Google Scholar] [CrossRef]
- Lee, D.; Heo, S.; Yoon, S.; Chang, D.; Lee, S.; Rhee, H.; Ku, B.; Park, K. Sleep disturbances and predictive factors in caregivers of patients with mild cognitive impairment and dementia. J. Clin. Neurol. 2014, 10, 304–313. [Google Scholar] [CrossRef]
- Simón, M.A.; Bueno, A.M.; Otero, P.; Blanco, V.; Vázquez, F.L. Insomnia in female family caregivers of totally dependent patients with dementia: An exploratory study. Behav. Psychol. 2019, 27, 107–119. [Google Scholar]
- Cook, S.K.; Snellings, L.; Cohen, S.A. Socioeconomic and demographic factors modify observed relationship between caregiving intensity and three dimensions of quality of life in informal adult children caregivers. Health Qual. Life Outcomes 2018, 16, 169. [Google Scholar] [CrossRef]
- Pinquart, M.; Sorensen, S. Correlates of physical health of informal caregivers: A meta-analysis. J. Gerontol. B Psychol. Sci. Soc. Sci. 2007, 62, 126–137. [Google Scholar] [CrossRef]
- Schulz, R.; Sherwood, P.R. Physical and mental health effects of family caregiving. Am. J. Nurs. 2008, 108, 23–27. [Google Scholar] [CrossRef]
- Beaudreau, S.A.; Spira, A.P.; Gray, H.L.; Depp, C.A.; Long, J.; Rothkopf, M.; Gallagher-Thompson, D. The relationship between objectively measured sleep disturbance and dementia family caregiver distress and burden. J. Geriatr. Psychiatry 2008, 21, 159–165. [Google Scholar] [CrossRef]
- Chiu, Y.; Lee, Y.; Wang, P.; Chang, T.; Li, C.; Hsu, W.; Lee, S. Family caregivers’ sleep disturbance and its associations with multilevel stressors when caring for patients with dementia. Aging Ment. Health 2014, 18, 92–101. [Google Scholar] [CrossRef]
- Happe, S.; Berger, K.; FAQT Study Investigators. The association between caregiver burden and sleep disturbances in partners of patients with Parkinson’s disease. Age Ageing 2002, 31, 349–354. [Google Scholar] [CrossRef]
- Foley, D.J.; Monjan, A.A.; Brown, S.L.; Simonsick, E.M.; Wallace, R.B.; Blazer, D.G. Sleep complaints among elderly persons: An epidemiologic study of three communities. Sleep 1995, 18, 425–432. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Royuela, A.; Macías, J.A. Propiedades clinimétricas de la versión castellana del cuestionario de Pittsburgh. Vigilia-Sueño 1997, 9, 81–94. [Google Scholar]
- Jiménez-Genchi, A.; Monteverde-Maldonado, E.; Nenclares-Portocarrero, A.; Esquivel-Adame, G.; de la Vega-Pacheco, A. Confiabilidad y análisis factorial de la versión en español del índice de calidad de sueño de Pittsburgh en pacientes psiquiátricos. Gac. Med. Mex. 2008, 144, 491–496. [Google Scholar]
- Novak, M.; Guest, C. Application of a multidimensional caregiver burden inventory. Gerontologist 1989, 29, 798–803. [Google Scholar] [CrossRef]
- Vázquez, F.L.; Otero, P.; Simón, M.A.; Bueno, A.M.; Blanco, V. Psychometric properties of the spanish version of the Caregiver Burden Inventory. Int. J. Environ. Res. Public Health 2019, 16, 217. [Google Scholar] [CrossRef]
- Hulley, S.B.; Cummings, S.R.; Newman, T.B. Designing cross-sectional and cohort studies. In Designing Clinical Research, 4th ed.; Hulley, S.B., Cummings, S.R., Browner, W.S., Grady, D.G., Newman, T.B., Eds.; Wolters Kluwer/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013; pp. 85–96. [Google Scholar]
- Creese, J.; Bédard, M.; Brazil, K.; Chambers, L. Sleep disturbances in spousal caregivers of individuals with Alzheimer’s disease. Int. Psychogeriatr. 2008, 20, 149–161. [Google Scholar] [CrossRef]
- Peng, H.L.; Lorenz, R.A.; Chang, Y.P. Factors associated with sleep in family caregivers of individuals with dementia. Perspect. Psychiatr. Care 2019, 55, 95–102. [Google Scholar] [CrossRef]
- Von Känel, R.; Mausbach, B.T.; Ancoli-Israel, S.; Dimsdale, J.E.; Mills, P.J.; Patterson, T.L.; Ziegler, M.G.; Roepke, S.K.; Chattillion, E.A.; Allison, M.; et al. Sleep in spousal Alzheimer caregivers: A longitudinal study with a focus on the effects of major patient transitions on sleep. Sleep 2012, 35, 247–255. [Google Scholar] [CrossRef]
- Stanley, S.; Balakrishnan, S.; Ilangovan, S. Psychological distress, perceived burden and quality of life in caregivers of persons with schizophrenia. J. Ment. Health 2017, 26, 134–141. [Google Scholar] [CrossRef]
- Peng, H.L.; Lorenz, R.A.; Chang, Y.P. Sleep quality in family caregivers of individuals with dementia: A concept analysis. Clin. Nurs. Res. 2016, 25, 448–464. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Group 1 | Group 2 | Control Group | Comparison |
|---|---|---|---|---|
| (CBI ≤ 36) | (CBI > 36) | |||
| n = 293 | n = 86 | n = 115 | n = 92 | |
| Family caregivers/Non-caregiver controls | ||||
| Age (years) | 55.75 (9.64) | 56.45 (10.39) | 57.03 (11.03) | F2,290 = 0.34; p = 0.713 |
| Gender | ||||
| Female | 72 (83.7) | 103 (89.6) | 78 (84.8) | |
| Male | 14 (16.3) | 12 (10.4) | 14 (15.2) | χ2 = 1.70; 2 df; p = 0.426 |
| Marital status | ||||
| With partner | 73 (84.9) | 87 (75.6) | 69 (75) | |
| Without partner | 13 (15.1) | 28 (24.4) | 23 (25) | χ2 = 3.24; 2 df; p = 0.198 |
| Educational level | ||||
| At least primary studies | 73 (84.9) | 101 (87.8) | 79 (85.9) | |
| Without primary studies | 13 (15.1) | 14 (12.2) | 13 (14.1) | χ2 = 0.39; 2 df; p = 0.824 |
| Monthly incomes (Euros) | ||||
| <1000 | 14 (16.3) | 28 (24.3) | 18 (19.6) | |
| 1000–2000 | 37 (43) | 46 (40) | 38 (41.3) | |
| >2000 | 7 (8.1) | 11 (9.6) | 10 (10.9) | |
| Do not know/No answer | 28 (32.6) | 30 (26.1) | 26 (28.2) | χ2 = 4.43; 6 df; p = 0.817 |
| Family relationship with the dependent (only family caregivers) | ||||
| Care recipient is the father/mother | 35 (40.7) | 53 (46.1) | ||
| Care recipient is the son/daughter | 19 (22.1) | 20 (17.4) | ||
| Care recipient is the partner or other | 32 (37.2) | 42 (36.5) | χ2 = 0.89; 2 df; p = 0.639 | |
| family member | ||||
| Care recipient | ||||
| Age (years) | 68.31 (23.27) | 74.01 (19.81) | t = −1.87; 199 df; p = 0.062 | |
| Gender | ||||
| Female | 49 (57) | 63 (54.8) | ||
| Male | 37 (43) | 52 (45.2) | χ2 = 0.10; 1 df; p = 0.756 | |
| Cause of the dependence | ||||
| Physical disability | 63 (73.3) | 54 (47.0) | ||
| Mental disorder | 23 (26.7) | 61 (53.0) | χ2 = 13.99; 1 df; p < 0.001 * | |
| Care situation | ||||
| Years providing care | 14.27 (11.20) | 14.64 (12.08) | t = −0.22; 199 df; p = 0.824 | |
| Daily hours of care | 15.19 (5.85) | 17.04 (4.72) | t = −2.47; 199 df; p < 0.05 * | |
| Measures | Group 1 | Group 2 | Control Group | Tests of Between-Subjects Effects (F and p-Values) |
|---|---|---|---|---|
| (CBI ≤ 36) | (CBI > 36) | |||
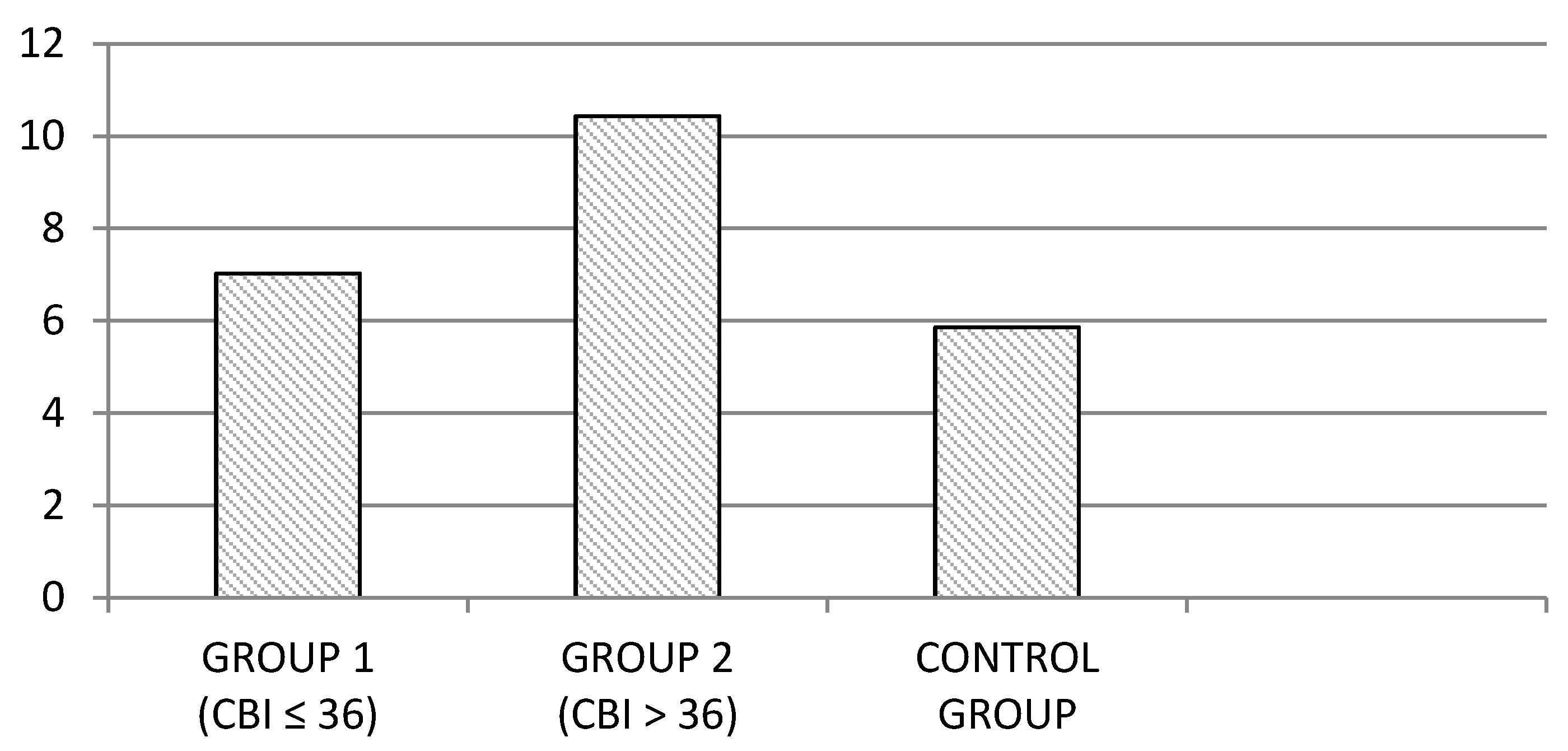
| PSQI total | 7.02 (3.43) | 10.43 (4.27) | 5.86 (3.57) | F2,290 = 40.39; p < 0.001 * |
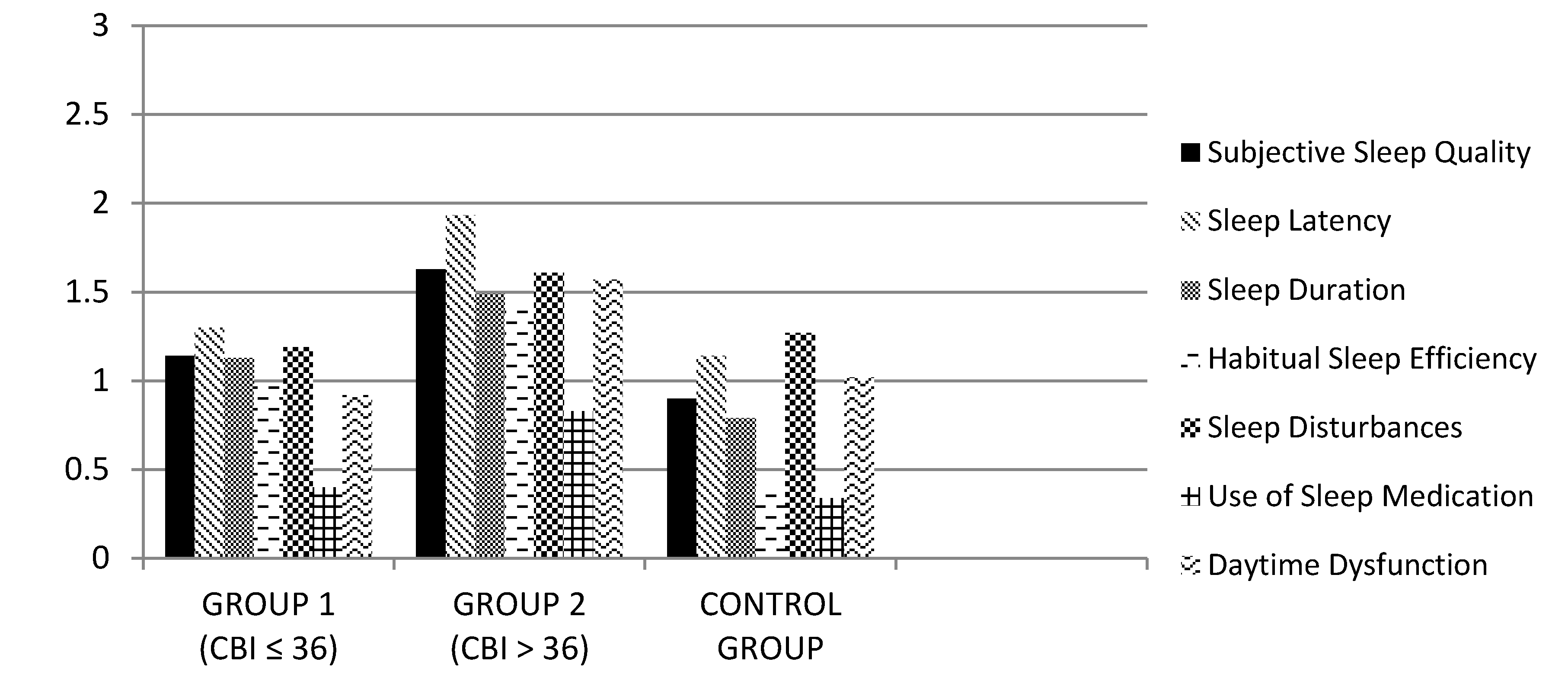
| Subjective sleep quality | 1.14 (0.69) | 1.63 (0.80) | 0.90 (0.73) | F2,290 = 25.55; p < 0.001 * |
| Sleep latency | 1.30 (1.15) | 1.93 (1.07) | 1.14 (0.86) | F2,290 = 16.99; p < 0.001 * |
| Sleep duration | 1.13 (0.97) | 1.49 (0.83) | 0.79 (0.65) | F2,290 = 18.34; p < 0.001 ** |
| Habitual sleep efficiency | 0.97 (1.06) | 1.40 (1.19) | 0.39 (0.77) | F2,290 = 24.24; p < 0.001 ** |
| Sleep disturbances | 1.19 (0.49) | 1.61 (0.64) | 1.27 (0.61) | F2,290 = 14.90; p < 0.001 * |
| Use of sleep medications | 0.40 (0.97) | 0.83 (1.22) | 0.34 (0.90) | F2,290 = 6.94; p < 0.01 * |
| Daytime dysfunction | 0.92 (0.78) | 1.57 (0.81) | 1.02 (0.77) | F2,290 = 20.12; p < 0.001 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simón, M.A.; Bueno, A.M.; Otero, P.; Blanco, V.; Vázquez, F.L. Caregiver Burden and Sleep Quality in Dependent People’s Family Caregivers. J. Clin. Med. 2019, 8, 1072. https://doi.org/10.3390/jcm8071072
Simón MA, Bueno AM, Otero P, Blanco V, Vázquez FL. Caregiver Burden and Sleep Quality in Dependent People’s Family Caregivers. Journal of Clinical Medicine. 2019; 8(7):1072. https://doi.org/10.3390/jcm8071072
Chicago/Turabian StyleSimón, Miguel A., Ana M. Bueno, Patricia Otero, Vanessa Blanco, and Fernando L. Vázquez. 2019. "Caregiver Burden and Sleep Quality in Dependent People’s Family Caregivers" Journal of Clinical Medicine 8, no. 7: 1072. https://doi.org/10.3390/jcm8071072