Cost–Utility of Mindfulness-Based Stress Reduction for Fibromyalgia versus a Multicomponent Intervention and Usual Care: A 12-Month Randomized Controlled Trial (EUDAIMON Study)

 , and
, and 
Abstract
:1. Introduction
2. Methods
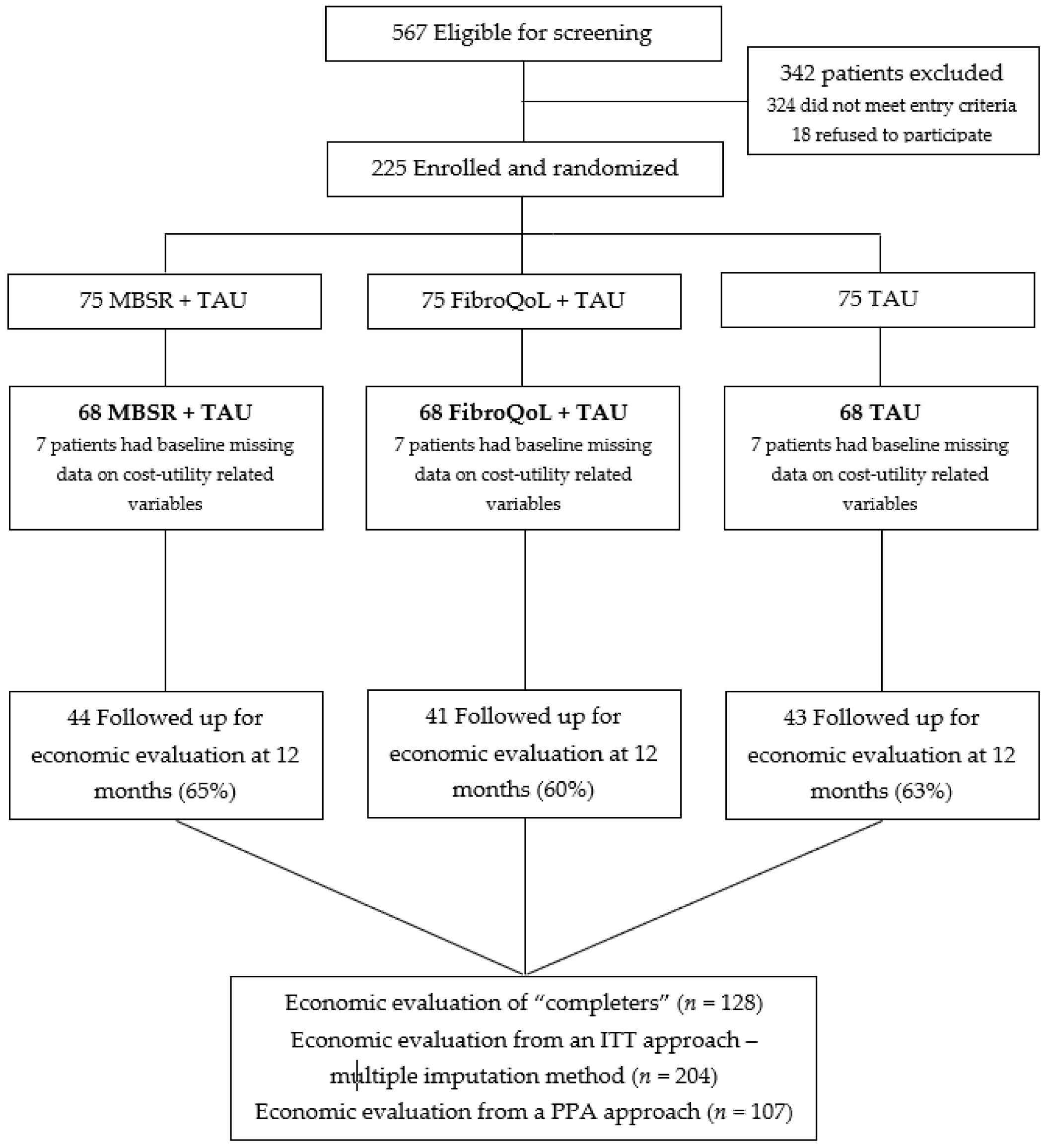
2.1. Participants
2.2. Inclusion and Exclusion Criteria
2.3. Design
2.4. Interventions
2.4.1. MBSR
2.4.2. FibroQoL
2.4.3. TAU
2.5. Outcome Measures
2.5.1. The EuroQol Questionnaire [41]
2.5.2. The Client Service Receipt Inventory (CSRI) Spanish Version
2.6. Statistical Analysis
3. Results
3.1. Baseline Costs
3.2. Follow-Up Costs
3.3. Baseline Quality of Life Outcomes
3.4. Follow-Up Quality of Life Outcomes
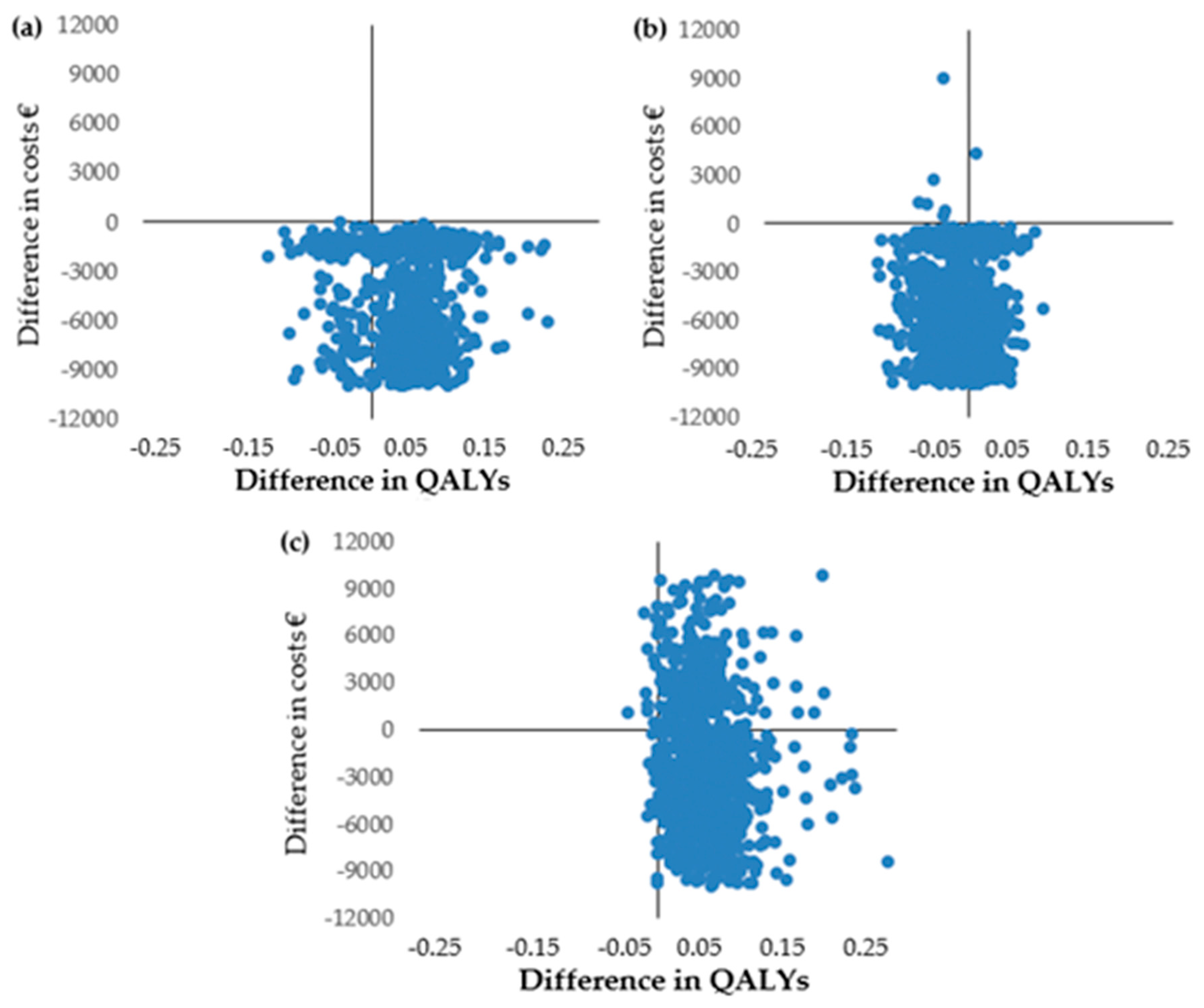
3.5. Cost Utility Analysis from the Government Perspective
3.6. Cost Utility Analysis from the Health Care Perspective
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Häuser, W.; Ablin, J.; Fitzcharles, M.-A.; Littlejohn, G.; Luciano, J.V.; Usui, C.; Walitt, B. Fibromyalgia. Nat. Rev. Dis. Primers 2015, 1, 15022. [Google Scholar] [CrossRef] [PubMed]
- Heidari, F.; Afshari, M.; Moosazadeh, M. Prevalence of fibromyalgia in general population and patients, a systematic review and meta-analysis. Rheumatol. Int. 2017, 37, 1527–1539. [Google Scholar] [CrossRef] [PubMed]
- Cabo-Meseguer, A.; Cerdá-Olmedo, G.; Trillo-Mata, J.L. Fibromyalgia: Prevalence, epidemiologic profiles and economic costs. Med. Clin. 2017, 149, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, D.L.; Dukes, E.M. The health status burden of people with fibromyalgia: A review of studies that assessed health status with the SF-36 or the SF-12. Int. J. Clin. Pract. 2007, 62, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Leadley, R.M.; Armstrong, N.; Lee, Y.C.; Allen, A.; Kleijnen, J. Chronic Diseases in the European Union: The Prevalence and Health Cost Implications of Chronic Pain. J. Pain Palliat. Care Pharmacother. 2012, 26, 310–325. [Google Scholar] [CrossRef] [PubMed]
- Berger, A.; Dukes, E.; Martin, S.; Edelsberg, J.; Oster, G. Characteristics and healthcare costs of patients with fibromyalgia syndrome. Int. J. Clin. Pract. 2007, 61, 1498–1508. [Google Scholar] [CrossRef] [Green Version]
- Gerdle, B.; Björk, J.; Cöster, L.; Henriksson, K.; Henriksson, C.; Bengtsson, A. Prevalence of widespread pain and associations with work status: A population study. BMC Musculoskelet. Disord. 2008, 9, 102. [Google Scholar] [CrossRef]
- Assefi, N.P.; Coy, T.V.; Uslan, D.; Smith, W.R.; Buchwald, D. Financial, occupational, and personal consequences of disability in patients with chronic fatigue syndrome and fibromyalgia compared to other fatiguing conditions. J. Rheumatol. 2003, 30, 804–808. [Google Scholar]
- Henriksson, C.; Liedberg, G.; Gerdle, B. Women with fibromyalgia: Work and rehabilitation. Disabil. Rehabil. 2005, 27, 685–694. [Google Scholar] [CrossRef]
- Wylezinski, L.S.; Gray, J.D.; Polk, J.B.; Harmata, A.J.; Spurlock, C.F. Illuminating an Invisible Epidemic: A Systemic Review of the Clinical and Economic Benefits of Early Diagnosis and Treatment in Inflammatory Disease and Related Syndromes. J. Clin. Med. 2019, 8, 493. [Google Scholar] [CrossRef]
- Nüesch, E.; Häuser, W.; Bernardy, K.; Barth, J.; Jüni, P. Comparative efficacy of pharmacological and non-pharmacological interventions in fibromyalgia syndrome: Network meta-analysis. Ann. Rheum. Dis. 2013, 72, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Aranda, A.; Barceló-Soler, A.; Andrés-Rodríguez, L.; Peñarrubia-María, M.T.; Tuccillo, R.; Borraz-Estruch, G.; García-Campayo, J.; Feliu-Soler, A.; Luciano, J.V. Description and narrative review of well-established and promising psychological treatments for fibromyalgia. Mindfulness Compassion 2017, 2, 112–129. [Google Scholar] [CrossRef]
- Perrot, S.; Russell, I.J. More ubiquitous effects from non-pharmacologic than from pharmacologic treatments for fibromyalgia syndrome: A meta-analysis examining six core symptoms. Eur. J. Pain 2014, 18, 1067–1080. [Google Scholar] [CrossRef] [PubMed]
- Luciano, J.V.; D’Amico, F.; Feliu-Soler, A.; McCracken, L.M.; Aguado, J.; Peñarrubia-María, M.T.; Knapp, M.; Serrano-Blanco, A.; García-Campayo, J. Cost-Utility of Group Acceptance and Commitment Therapy for Fibromyalgia Versus Recommended Drugs: An Economic Analysis Alongside a 6-Month Randomized Controlled Trial Conducted in Spain (EFFIGACT Study). J. Pain 2017, 18, 868–880. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, A.; Boomershine, C.S.; Choy, E.H.; Chandran, A.; Zlateva, G. The cost-effectiveness of pregabalin in the treatment of fibromyalgia: US perspective. J. Med. Econ. 2012, 15, 481–492. [Google Scholar] [CrossRef] [PubMed]
- Zijlstra, T.R.; Braakman-Jansen, L.M.A.; Taal, E.; Rasker, J.J.; van de Laar, M.A.F.J. Cost-effectiveness of Spa treatment for fibromyalgia: General health improvement is not for free. Rheumatology 2007, 46, 1454–1459. [Google Scholar] [CrossRef] [PubMed]
- Gusi, N.; Tomas-Carus, P. Cost-utility of an 8-month aquatic training for women with fibromyalgia: A randomized controlled trial. Arthritis Res. Ther. 2008, 10, R24. [Google Scholar] [CrossRef] [PubMed]
- Choy, E.; Richards, S.; Bowrin, K.; Watson, P.; Lloyd, A.; Sadosky, A.; Zlateva, G. Cost effectiveness of pregabalin in the treatment of fibromyalgia from a UK perspective. Curr. Med. Res. Opin. 2010, 26, 965–975. [Google Scholar] [CrossRef]
- Arreola Ornelas, H.; Rosado Buzzo, A.; García, L.; Dorantes Aguilar, J.; Contreras Hernández, I.; Mould Quevedo, J.F. Cost-effectiveness Analysis of Pharmacologic Treatment of Fibromyalgia in Mexico. Reumatol. Clín. 2012, 8, 120–127. [Google Scholar] [CrossRef]
- Beard, S.M.; Roskell, N.; Le, T.K.; Zhao, Y.; Coleman, A.; Ang, D.; Lawson, K. Cost effectiveness of duloxetine in the treatment of fibromyalgia in the United States. J. Med. Econ. 2016, 14, 463–476. [Google Scholar] [CrossRef]
- Goossens, M.E.; Rutten-van Mölken, M.P.; Leidl, R.M.; Bos, S.G.; Vlaeyen, J.W.; Teeken-Gruben, N.J. Cognitive-educational treatment of fibromyalgia: A randomized clinical trial. II. Economic evaluation. J. Rheumatol. 1996, 23, 1246–1254. [Google Scholar] [PubMed]
- Luciano, J.V.; Sabes-Figuera, R.; Cardeñosa, E.; Peñarrubia-María, M.T.; Fernández-Vergel, R.; García-Campayo, J.; Knapp, M.; Serrano-Blanco, A. Cost-utility of a psychoeducational intervention in fibromyalgia patients compared with usual care: An economic evaluation alongside a 12-month randomized controlled trial. Clin. J. Pain 2013, 29, 702–711. [Google Scholar] [CrossRef] [PubMed]
- Luciano, J.V.; D’Amico, F.; Cerdà-Lafont, M.; Peñarrubia-María, M.T.; Knapp, M.; Cuesta-Vargas, A.I.; Serrano-Blanco, A.; García-Campayo, J. Cost-utility of cognitive behavioral therapy versus U.S. Food and Drug Administration recommended drugs and usual care in the treatment of patients with fibromyalgia: An economic evaluation alongside a 6-month randomized controlled trial. Arthritis Res. Ther. 2014, 16, 451. [Google Scholar] [CrossRef] [PubMed]
- Hedman-Lagerlöf, M.; Hedman-Lagerlöf, E.; Ljótsson, B.; Wicksell, R.K.; Flink, I.; Andersson, E. Cost-Effectiveness and Cost-Utility of Internet-Delivered Exposure Therapy for Fibromyalgia: Results from a Randomized, Controlled Trial. J. Pain 2019, 20, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Schröder, A.; Ørnbøl, E.; Jensen, J.S.; Sharpe, M.; Fink, P. Long-term economic evaluation of cognitive-behavioural group treatment versus enhanced usual care for functional somatic syndromes. J. Psychosom. Res. 2017, 94, 73–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duarte, R.; Lloyd, A.; Kotas, E.; Andronis, L.; White, R. Are acceptance and mindfulness-based interventions ‘value for money’? Evidence from a systematic literature review. Br. J. Clin. Psychol. 2018, 58, 187–210. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.; Grossman, P.; Schwarzer, B.; Jena, S.; Naumann, J.; Walach, H. Treating fibromyalgia with mindfulness-based stress reduction: Results from a 3-armed randomized controlled trial. Pain 2011, 152, 361–369. [Google Scholar] [CrossRef]
- Sephton, S.E.; Salmon, P.; Weissbecker, I.; Ulmer, C.; Floyd, A.; Hoover, K.; Studts, J.L. Mindfulness meditation alleviates depressive symptoms in women with fibromyalgia: Results of a randomized clinical trial. Arthritis Rheum. 2007, 57, 77–85. [Google Scholar] [CrossRef]
- Van Gordon, W.; Shonin, E.; Dunn, T.J.; Garcia-Campayo, J.; Griffiths, M.D. Meditation awareness training for the treatment of fibromyalgia syndrome: A randomized controlled trial. Br. J. Health Psychol. 2017, 22, 186–206. [Google Scholar] [CrossRef]
- Cash, E.; Salmon, P.; Weissbecker, I.; Rebholz, W.N.; Bayley-Veloso, R.; Zimmaro, L.A.; Floyd, A.; Dedert, E.; Sephton, S.E. Mindfulness Meditation Alleviates Fibromyalgia Symptoms in Women: Results of a Randomized Clinical Trial. Ann. Behav. Med. 2015, 49, 319–330. [Google Scholar] [CrossRef]
- Pérez-Aranda, A.; Feliu-Soler, A.; Montero-Marín, J.; García-Campayo, J.; Andrés-Rodríguez, L.; Borràs, X.; Rozadilla-Sacanell, A.; Peñarrubia-María, M.T.; Angarita-Osorio, N.; McCracken, L.M.; et al. A randomized controlled efficacy trial of Mindfulness-Based Stress Reduction compared to an active control group and usual care for fibromyalgia: The eudaimon study. Pain 2019, in press. [Google Scholar]
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P.; et al. The american college of rheumatology 1990 criteria for the classification of fibromyalgia. Arthritis Rheum. 1990, 33, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Lobo, A.; Saz, P.; Marcos, G.; Día, J.L.; de la Cámara, C.; Ventura, T.; Morales Asín, F.; Fernando Pascual, L.; Montañés, J.A.; Aznar, S. Revalidation and standardization of the cognition mini-exam (first Spanish version of the Mini-Mental Status Examination) in the general geriatric population. Med. Clin. 1999, 112, 767–774. [Google Scholar]
- Feliu-Soler, A.; Borràs, X.; Peñarrubia-María, M.T.; Rozadilla-Sacanell, A.; D’Amico, F.; Moss-Morris, R.; Howard, M.A.; Fayed, N.; Soriano-Mas, C.; Puebla-Guedea, M.; et al. Cost-utility and biological underpinnings of Mindfulness-Based Stress Reduction (MBSR) versus a psychoeducational programme (FibroQoL) for fibromyalgia: A 12-month randomised controlled trial (EUDAIMON study). BMC Complement. Altern. Med. 2016, 16, 81. [Google Scholar] [CrossRef] [PubMed]
- Kabat-Zinn, J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: Theoretical considerations and preliminary results. Gen. Hosp. Psychiatry 1982, 4, 33–47. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Mindfulness-based interventions in context: Past, present, and future. Clin. Psychol. Sci. Pract. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Keng, S.L.; Smoski, M.J.; Robins, C.J. Effects of mindfulness on psychological health: A review of empirical studies. Clin. Psychol. Rev. 2011, 31, 1041–1056. [Google Scholar] [CrossRef] [Green Version]
- Martín Asuero, A. Con Rumbo Propio Disfruta de la Vida Sin Estrés; Plataforma: Curia, Portugal, 2010; ISBN 841-5-11-5008. [Google Scholar]
- Luciano, J.V.; Martínez, N.; Peñarrubia-María, M.T.; Fernández-Vergel, R.; García-Campayo, J.; Verduras, C.; Blanco, M.E.; Jiménez, M.; Ruiz, J.M.; Del Hoyo, Y.L.; et al. Effectiveness of a psychoeducational treatment program implemented in general practice for fibromyalgia patients: A randomized controlled trial. Clin. J. Pain 2011, 27, 383–391. [Google Scholar] [CrossRef]
- Belenguer-Prieto, R.; Carbonell-Baeza, A.; García-Campayo, J.; Luciano, J.V.; Martín-Nogueras, A.M.; Martínez-Lavín, M.; Muñoz-Espinalt, E.; Pastor-Mira, M.A.; Peñacoba, C.; Calandre, E.; et al. Beginner’s Guide to Fibromyalgia. Available online: http://www.fibro.info/guideen.pdf (accessed on 1 January 2019).
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Badia, X.; Roset, M.; Montserrat, S.; Herdman, M.; Segura, A. The Spanish version of EuroQol: A description and its applications. European Quality of Life scale. Med. Clin. 1999, 112, 79–85. [Google Scholar]
- Stone, G.; Hutchinson, A.; Corso, P.; Teutsch, S.; Fielding, J.; Carande-Kulis, V.; Briss, P. Understanding and using the economic evidence. In The Guide to Community Preventive Services: What Works to Promote Health? Oxford University Press: Oxford, UK, 2005; pp. 449–463. [Google Scholar]
- Vázquez-Barquero, J.; Gaite, L.; Cuesta, M.; Garcia-Usieto, E.; Knapp, M.; Beecham, J. Spanish version of the CSRI: A mental health cost evaluation interview. Arch. Neuobiol. 1997, 60, 171–184. [Google Scholar]
- Husereau, D.; Drummond, M.; Petrou, S.; Carswell, C.; Moher, D.; Greenberg, D.; Augustovski, F.; Briggs, A.H.; Mauskopf, J.; Loder, E. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. Eur. J. Health Econ. 2013, 14, 367–372. [Google Scholar] [CrossRef] [Green Version]
- Ramsey, S.D.; Willke, R.J.; Glick, H.; Reed, S.D.; Augustovski, F.; Jonsson, B.; Briggs, A.; Sullivan, S.D. Cost-effectiveness analysis alongside clinical trials II—An ISPOR good research practices task force report. Value Health 2015, 18, 161–172. [Google Scholar] [CrossRef]
- Base de Datos de Costes Sanitarios SOIKOS Barcelona: Oblikue Consulting. Base de Datos de Costes Sanitarios eSALUD Barcelona. 2016. Available online: http://www.oblikue.com/en/esalud.html (accessed on 1 April 2019).
- Richardson, G.; Manca, A. Calculation of quality adjusted life years in the published literature: A review of methodology and transparency. Health Econ. 2004, 13, 1203–1210. [Google Scholar] [CrossRef]
- Greene, W. Econometric Analysis; Prentice Hall: Englewood Cliffs, NJ, USA, 2003. [Google Scholar]
- Briggs, A.H.; Wonderling, D.E.; Mooney, C.Z. Pulling cost-effectiveness analysis up by its bootstraps: A non-parametric approach to confidence interval estimation. Health Econ. 1997, 6, 327–340. [Google Scholar] [CrossRef]
- Royston, P.; White, I. Multiple Imputation by Chained Equations (MICE): Implementation in Stata. J. Stat. Softw. 2015, 45, 1–20. [Google Scholar] [CrossRef]
- Becker, A. Health economics of interdisciplinary rehabilitation for chronic pain: Does it support or invalidate the outcomes research of these programs? Curr. Pain Headache Rep. 2012, 16, 127–132. [Google Scholar] [CrossRef]
- Schaefer, C.; Chandran, A.; Hufstader, M.; Baik, R.; McNett, M.; Goldenberg, D.; Gerwin, R.; Zlateva, G. The comparative burden of mild, moderate and severe Fibromyalgia: Results from a cross-sectional survey in the United States. Health Qual. Life Outcomes 2011, 9, 71. [Google Scholar] [CrossRef]
- Pérez-Aranda, A.; Andrés-Rodríguez, L.; Feliu-Soler, A.; Núñez, C.; Stephan-Otto, C.; Pastor-Mira, M.A.; López-Roig, S.; Peñacoba, C.; Calandre, E.P.; Slim, M.; et al. Clustering a large Spanish sample of patients with fibromyalgia using the FIQR. Pain 2019, 160, 908–921. [Google Scholar] [CrossRef]
- Häuser, W.; Jung, E.; Erbslöh-Möller, B.; Gesmann, M.; Kühn-Becker, H.; Petermann, F.; Langhorst, J.; Weiss, T.; Winkelmann, A.; Wolfe, F. Validation of the Fibromyalgia Survey Questionnaire within a Cross-Sectional Survey. PLoS ONE 2012, 7, e37504. [Google Scholar] [CrossRef]
- Sullivan, M.J.L.; Bishop, S.R.; Pivik, J. The Pain Catastrophizing Scale: Development and validation. Psychol. Assess. 1995, 7, 524–532. [Google Scholar] [CrossRef]
- Pradhan, E.K.; Baumgarten, M.; Langenberg, P.; Handwerger, B.; Gilpin, A.K.; Magyari, T.; Hochberg, M.C.; Berman, B.M. Effect of Mindfulness-Based stress reduction in rheumatoid arthritis patients. Arthritis Rheum. 2007, 57, 1134–1142. [Google Scholar] [CrossRef]
- Parsons, C.E.; Crane, C.; Parsons, L.J.; Fjorback, L.O.; Kuyken, W. Home practice in Mindfulness-Based Cognitive Therapy and Mindfulness-Based Stress Reduction: A systematic review and meta-analysis of participants’ mindfulness practice and its association with outcomes. Behav. Res. Ther. 2017, 95, 29–41. [Google Scholar] [CrossRef]
- Mathew, K.L.; Whitford, H.S.; Kenny, M.A.; Denson, L.A. The Long-Term Effects of Mindfulness-Based Cognitive Therapy as a Relapse Prevention Treatment for Major Depressive Disorder. Behav. Cogn. Psychother. 2010, 38, 561–576. [Google Scholar] [CrossRef]
- Carmody, J.; Baer, R.A. Relationships between mindfulness practice and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program. J. Behav. Med. 2008, 31, 23–33. [Google Scholar] [CrossRef]
- Hayes, S.M.; Myhal, G.C.; Thornton, J.F.; Camerlain, M.; Jamison, C.; Cytryn, K.N.; Murray, S. Fibromyalgia and the Therapeutic Relationship: Where Uncertainty Meets Attitude. Pain Res. Manag. 2010, 15, 385–391. [Google Scholar] [CrossRef] [Green Version]
- Album, D.; Westin, S. Do diseases have a prestige hierarchy? A survey among physicians and medical students. Soc. Sci. Med. 2008, 66, 182–188. [Google Scholar] [CrossRef]
- Hernandez Alava, M.; Wailoo, A.; Grimm, S.; Pudney, S.; Gomes, M.; Sadique, Z.; Meads, D.; O’Dwyer, J.; Barton, G.; Irvine, L. EQ-5D-5L versus EQ-5D-3L: The Impact on Cost Effectiveness in the United Kingdom. Value Health 2018, 21, 49–56. [Google Scholar] [CrossRef]
- Bhandari, A.; Wagner, T. Self-Reported Utilization of Health Care Services: Improving Measurement and Accuracy. Med. Care Res. Rev. 2006, 63, 217–235. [Google Scholar] [CrossRef]
- Bellón, J.Á.; Lardelli, P.; de Dios Luna, J.; Delgado, A. Validity of self reported utilisation of primary health care services in an urban population in Spain. J. Epidemiol. Community Health 2000, 54, 544–551. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Schmid, C.H.; Rones, R.; Kalish, R.; Yinh, J.; Goldenberg, D.L.; Lee, Y.; McAlindon, T. A Randomized Trial of Tai Chi for Fibromyalgia. N. Engl. J. Med. 2010, 363, 743–754. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Service (Unit) | Costs (€) |
|---|---|
| Health care General practitioner (per appointment) | |
| 36.97 | |
| Nurse/psychiatric nurse (per appointment) | 34.13 |
| Social worker (per appointment) | 35.78 |
| Clinical Psychologist (per appointment) | 45.06 |
| Psychiatrist (per appointment) | 45.06 |
| Other medical specialists (per appointment) | 43.82 |
| Accident & Emergency in hospital (per attendance) | 99.34 |
| Hospital stay (per night) | 112 |
| Diagnostic tests (range) | 6.13–455.53 |
| Pharmacological treatment (per daily dose) * | Various |
| MBSR & FibroQoL (per participant per group session) | 45.06 |
| Productivity loss Absenteeism from work (minimum daily wage) | |
| 21.8 |
| MBSR (n = 68) | FibroQoL (n = 68) | TAU (n = 68) | p | |
|---|---|---|---|---|
| Gender (women, %) | 66 (97.1%) | 67 (98.5%) | 67 (98.5%) | 0.78 |
| Age, mean (SD) | 52.63 (8.03) | 54.44 (7.69) | 53.16 (8.39) | 0.4 |
| Marital status, n (%) | 0.59 | |||
| Single | 2 (2.9%) | 3 (4.4%) | 1 (1.5%) | |
| Married/living with a partner | 53 (77.9%) | 50 (73.5%) | 55 (80.9%) | |
| Separated/divorced | 11 (16.2%) | 9 (13.2%) | 10 (14.7%) | |
| Widowed | 2 (2.9%) | 6 (8.8%) | 2 (2.9%) | |
| Education level, n (%) | 0.21 | |||
| Illiterate | 0 (0%) | 1 (1.5%) | 1 (1.5%) | |
| Did not graduate from primary school | 4 (5.9%) | 1 (1.5%) | 4 (5.9%) | |
| Primary school | 31 (45.6%) | 37 (54.4%) | 32 (47.1%) | |
| Secondary school | 31 (45.6%) | 24 (35.3%) | 28 (41.2%) | |
| University | 0 (0%) | 5 (7.4%) | 3 (4.4%) | |
| Others | 2 (2.9%) | 0 (0%) | 0 (0%) | |
| Employment status, n (%) | 0.47 | |||
| Homemaker | 10 (14.7%) | 10 (14.7%) | 4 (5.9%) | |
| Paid employment | 19 (27.9%) | 21 (30.9%) | 19 (27.9%) | |
| Paid employment but in sick leave | 6 (8.8%) | 4 (5.9%) | 4 (5.9%) | |
| Unemployed with subsidy | 8 (11.8%) | 9 (13.2%) | 11 (16.2%) | |
| Unemployed without subsidy | 8 (11.8%) | 15 (22.1%) | 9 (13.2%) | |
| Retired/pensioner | 9 (13.2%) | 4 (5.9%) | 10 (14.7%) | |
| Temporal disability | 1 (1.5%) | 2 (2.9%) | 1 (1.5%) | |
| Others | 7 (10.3%) | 3 (4.4%) | 10 (14.7%) | |
| Clinical variables | ||||
| Years of diagnosis, mean (SD) | 14.46 (9.17) | 11.28 (7.17) | 13.68 (10.02) | 0.14 |
| Current episode of depression, n (%) | 24 (35.3%) | 39 (57.4%) | 38 (55.9%) | 0.02 |
| Previous episode(s) of depression, n (%) | 25 (36.8%) | 20 (29.4%) | 34 (50%) | 0.04 |
| Dysthymia, n (%) | 14 (20.6%) | 9 (13.2%) | 8 (11.8%) | 0.31 |
| Daily FM-related medication | ||||
| Analgesics, n (%) | 21 (30.9%) | 21 (30.9%) | 15 (22.1%) | 0.42 |
| Anti-inflammatory, n (%) | 17 (25%) | 17 (25%) | 24 (35.3%) | 0.31 |
| Opioids, n (%) | 25 (36.8%) | 21 (30.9%) | 17 (25%) | 0.33 |
| Antiepileptic, n (%) | 13 (19.1%) | 11 (16.2%) | 14 (20.6%) | 0.8 |
| Muscle relaxant, n (%) | 2 (2.9%) | 5 (7.4%) | 3 (4.4%) | 0.48 |
| Antidepressants, n (%) | 35 (51.5%) | 30 (44.1%) | 26 (38.2%) | 0.3 |
| Anxiolytics, n (%) | 30 (44.1%) | 33 (48.5%) | 31 (45.6%) | 0.87 |
| MBSR | FibroQoL | TAU | OMNIBUS Significance Test | ||
|---|---|---|---|---|---|
| Baseline (N = 204) | n = 68 | n = 68 | n = 68 | p | Adjusted p |
| Primary health care services | 349.6 (325.8) | 322.4 (282.8) | 316.4 (269.6) | 0.78 | 0.81 |
| Specialized health care services | 537.6 (438.1) | 398.5 (411.9) | 661.9 (674.8) | 0.01 | 0.02 |
| Medical tests | 455.8 (462.8) | 474.2 (634.7) | 424.3 (480.4) | 0.86 | 0.94 |
| FM-related medications | 307.6 (488.6) | 204.3 (262.6) | 171.6 (282.5) | 0.15 | 0.19 |
| Direct costs | 1650.7 (1069.9) | 1399.4 (1006.5) | 1574.3 (1220.6) | 0.35 | 0.39 |
| Indirect costs | 667.8 (1951.1) | 669.7 (1569.6) | 1144.8 (2953.1) | 0.45 | 0.24 |
| Total costs | 2318.4 (2417.6) | 2069.1 (2075.5) | 2719.1 (3783.9) | 0.45 | 0.18 |
| Outcomes | |||||
| EQ-5D utility score (0 to 1) | 0.50 (0.21) | 0.48 (0.23) | 0.53 (0.23) | 0.44 | 0.28 |
| EQ VAS (0 to 100) * | 46.61 (21.82) | 47.31 (19.91) | 47.32 (18.51) | 0.97 | 0.75 |
| 12-months Follow-up (N = 128) | n = 44 | n = 41 | n = 43 | ||
| Primary health care services | 197.3 (233.4) | 319.4 (312.3) | 357.9 (301.8) | 0.01 | 0.02 |
| Specialized health care services | 498 (485.3) | 534.1 (552) | 664.8 (754.3) | 0.45 | 0.5 |
| Medical tests | 225.4 (360.3) | 257.3 (280.4) | 328.2 (417.6) | 0.44 | 0.42 |
| FM-related medications | 235.9 (349.2) | 189.8 (205.1) | 255.4 (434.3) | 0.56 | 0.58 |
| Intervention (MBSR/FibroQoL) | 702.5 (298.9) | 578.1 (181.3) | 0 (0) | 0 | 0 |
| Direct costs | 1156.6 (938.3) | 1300.6 (872.4) | 1598.7 (1265.1) | 0.17 | 0.13 |
| Indirect costs | 400.9 (1325.2) | 714.6 (1905.8) | 929.9 (2229.8) | 0.36 | 0.1 |
| Total costs | 1557.5 (1626.9) | 2015.2 (2122.1) | 2528.7 (3017) | 0.14 | 0.04 |
| Outcomes | |||||
| EQ-5D utility score (0 to 1) | 0.57 (0.25) | 0.53 (0.27) | 0.45 (0.26) | 0.11 | 0.05 |
| EQ VAS (0 to 100 points) | 52.41 (23.06) | 42.44 (21.16) | 44.98 (19.85) | 0.09 | 0.21 |
| QALY (0 to 1, on the basis of EQ-5D utility score) | 0.54 (0.18) | 0.50 (0.20) | 0.48 (0.22) | 0.34 | 0.05 |
| Incremental Cost | Incremental Effect | ICER | |
|---|---|---|---|
| Mean | Mean | ||
| (95% Bootstrap CI) | (95% Bootstrap CI) | ||
| MBSR vs TAU | |||
| Completers (n = 128) | |||
| QALY (EQ-5D) | −1023.5 (−2024.7 to −270.5) | 0.053 (−0.040 to 0.129) | MBSR dominant |
| EQ VAS (0-100) * | −1072 (−2048.5 to −273.6) | 7.89 (−1.72 to 18.69) | MBSR dominant |
| ITT (n = 204) | |||
| QALY (EQ-5D) | −828.1 (−1699.4 to 43.2) | 0.053 (0.004 to 0.101) | MBSR dominant |
| EQ VAS (0-100) * | −855.2 (−1727.6 to 17.3) | 7.13 (−0.52 to 14.79) | MBSR dominant |
| PPA (n = 107) | |||
| QALY (EQ-5D) | −1036.6 (−1894.3 to −178.9) | 0.080 (-0.060 to 0.220) | MBSR dominant |
| EQ VAS (0–100) * | −1108.6 (−1968.8 to −248.4) | 12.23 (−2.33 to 26.78) | MBSR dominant |
| MBSR vs FibroQoL | |||
| Completers (n = 128) | |||
| QALY (EQ-5D) | −770.8 (−1401.4 to −172.4) | -0.002 (-0.066 to 0.059) | €385,400/QALY |
| EQ VAS (0-100) * | −822.5 (−1529.1 to −195) | 9.46 (-0.84 to 20.35) | MBSR dominant |
| ITT (n = 204) | |||
| QALY (EQ-5D) | −539.9 (−1214.6 to 134.8) | 0.012 (−0.032 to 0.056) | MBSR dominant |
| EQ VAS (0-100) * | −575 (−1246.1 to 96.1) | 6.68 (−1.01 to 14.37) | MBSR dominant |
| PPA (n = 107) | |||
| QALY (EQ-5D) | −582.8 (−1269.1 to 103.4) | 0.011 (−0.083 to 0.104) | MBSR dominant |
| EQ VAS (0-100) * | −651.6 (−1328 to 24.8) | 12.08 (−3.62 to 27.78) | MBSR dominant |
| FibroQoL vs TAU | |||
| Completers (n = 128) | |||
| QALY (EQ-5D) | −252.7 (−1176.6 to 536) | 0.056 (0.006 to 0.172) | FibroQoL dominant |
| EQ VAS (0-100) * | −249.6 (−1164.5 to 654) | −1.57 (−6.71 to 10.44) | €159/EQ VAS |
| ITT (n = 204) | |||
| QALY (EQ-5D) | −288.2 (−1307.9 to 731.6) | 0.041 (−0.003 to 0.084) | FibroQoL dominant |
| EQ VAS (0-100) * | −280.1 (−1297 to 736.6) | 0.45 (−7.31 to 8.22) | FibroQoL dominant |
| PPA (n = 107) | |||
| QALY (EQ-5D) | −453.8 (−1290.3 to 382.8) | 0.069 (-0.010 to 0.149) | FibroQoL dominant |
| EQ VAS (0-100) * | −456.9 (−1301 to 387.1) | 0.15 (−9.47 to 9.76) | FibroQoL dominant |
| Incremental Cost | Incremental Effect | ICER | |
|---|---|---|---|
| Mean | Mean | ||
| (95% Bootstrap CI) | (95% Bootstrap CI) | ||
| MBSR vs. TAU | |||
| Completers (n = 128) | |||
| QALY (EQ-5D) | −420.7 (−883.8 to −34.9) | 0.053 (−0.041 to 0.131) | MBSR dominant |
| EQ VAS (0–100) * | −464.8 (−884.2 to −63.3) | 7.89 (−1.65 to 18.65) | MBSR dominant |
| ITT (n = 204) | |||
| QALY (EQ-5D) | −455.2 (−904.6 to −4.9) | 0.053 (0.004 to 0.102) | MBSR dominant |
| EQ VAS (0–100) * | −483 (−929.5 to −36.5) | 7.14 (−0.49 to 14.77) | MBSR dominant |
| PPA (n = 107) | |||
| QALY (EQ-5D) | −431.5 (−866.7 to 3.7) | 0.080 (−0.060 to 0.220) | MBSR dominant |
| EQ VAS (0–100) * | −493.6 (−914.9 to −72.2) | 12.22 (−2.57 to 27.02) | MBSR dominant |
| MBSR vs FibroQoL | |||
| Completers (n = 128) | |||
| QALY (EQ-5D) | −232.6 (−572 to 129.6) | −0.002 (−0.067 to 0.059) | 116,300 €/QALY |
| EQ VAS (0–100) * | −275.2 (−629.2 to 96.7) | 9.47 (−1.03 to 20.24) | MBSR dominant |
| ITT (n = 204) | |||
| QALY (EQ-5D) | −236.2 (−551.8 to 79.5) | 0.012 (−0.033 to 0.058) | MBSR dominant |
| EQ VAS (0–100) * | −265.2 (−573.9 to 43.6) | 6.69 (−0.87 to 14.25) | MBSR dominant |
| PPA (n = 107) | |||
| QALY (EQ-5D) | −117.6 (−505.4 to 270.1) | 0.011 (−0.083 to 0.104) | MBSR dominant |
| EQ VAS (0–100) * | −174.2 (−551.3 to 202.8) | 12.07 (−3.76 to 27.90) | MBSR dominant |
| FibroQoL vs TAU | |||
| Completers (n = 128) | |||
| QALY (EQ-5D) | −188 (−696.2 to 227.8) | 0.056 (0.007 to 0.173) | FibroQoL dominant 121 €/EQ VAS |
| EQ VAS (0–100) * | −189.6 (−625.8 to 259.4) | −1.57 (−10.49 to 6.68) | |
| ITT (n = 204) | |||
| QALY (EQ-5D) | −219.1 (−656.3 to 218.1) | 0.041 (−0.002 to 0.084) | FibroQoL dominant |
| EQ VAS (0–100) * | −217.8 (−655.9 to 220.3) | 0.45 (−7.22 to 8.12) | FibroQoL dominant |
| PPA (n = 107) | |||
| QALY (EQ-5D) | −313.9 (−747.9 to 120.2) | 0.069 (−0.010 to 0.149) | FibroQoL dominant |
| EQ VAS (0–100) * | −319.4 (−748.8 to 110.1) | 0.15 (−9.42 to 9.73) | FibroQoL dominant |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Aranda, A.; D’Amico, F.; Feliu-Soler, A.; McCracken, L.M.; Peñarrubia-María, M.T.; Andrés-Rodríguez, L.; Angarita-Osorio, N.; Knapp, M.; García-Campayo, J.; Luciano, J.V. Cost–Utility of Mindfulness-Based Stress Reduction for Fibromyalgia versus a Multicomponent Intervention and Usual Care: A 12-Month Randomized Controlled Trial (EUDAIMON Study). J. Clin. Med. 2019, 8, 1068. https://doi.org/10.3390/jcm8071068
Pérez-Aranda A, D’Amico F, Feliu-Soler A, McCracken LM, Peñarrubia-María MT, Andrés-Rodríguez L, Angarita-Osorio N, Knapp M, García-Campayo J, Luciano JV. Cost–Utility of Mindfulness-Based Stress Reduction for Fibromyalgia versus a Multicomponent Intervention and Usual Care: A 12-Month Randomized Controlled Trial (EUDAIMON Study). Journal of Clinical Medicine. 2019; 8(7):1068. https://doi.org/10.3390/jcm8071068
Chicago/Turabian StylePérez-Aranda, Adrián, Francesco D’Amico, Albert Feliu-Soler, Lance M. McCracken, María T. Peñarrubia-María, Laura Andrés-Rodríguez, Natalia Angarita-Osorio, Martin Knapp, Javier García-Campayo, and Juan V. Luciano. 2019. "Cost–Utility of Mindfulness-Based Stress Reduction for Fibromyalgia versus a Multicomponent Intervention and Usual Care: A 12-Month Randomized Controlled Trial (EUDAIMON Study)" Journal of Clinical Medicine 8, no. 7: 1068. https://doi.org/10.3390/jcm8071068