Is Two Better Than One? The Impact of Doubling Training Volume in Severe COPD: A Randomized Controlled Study

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Experimental Section
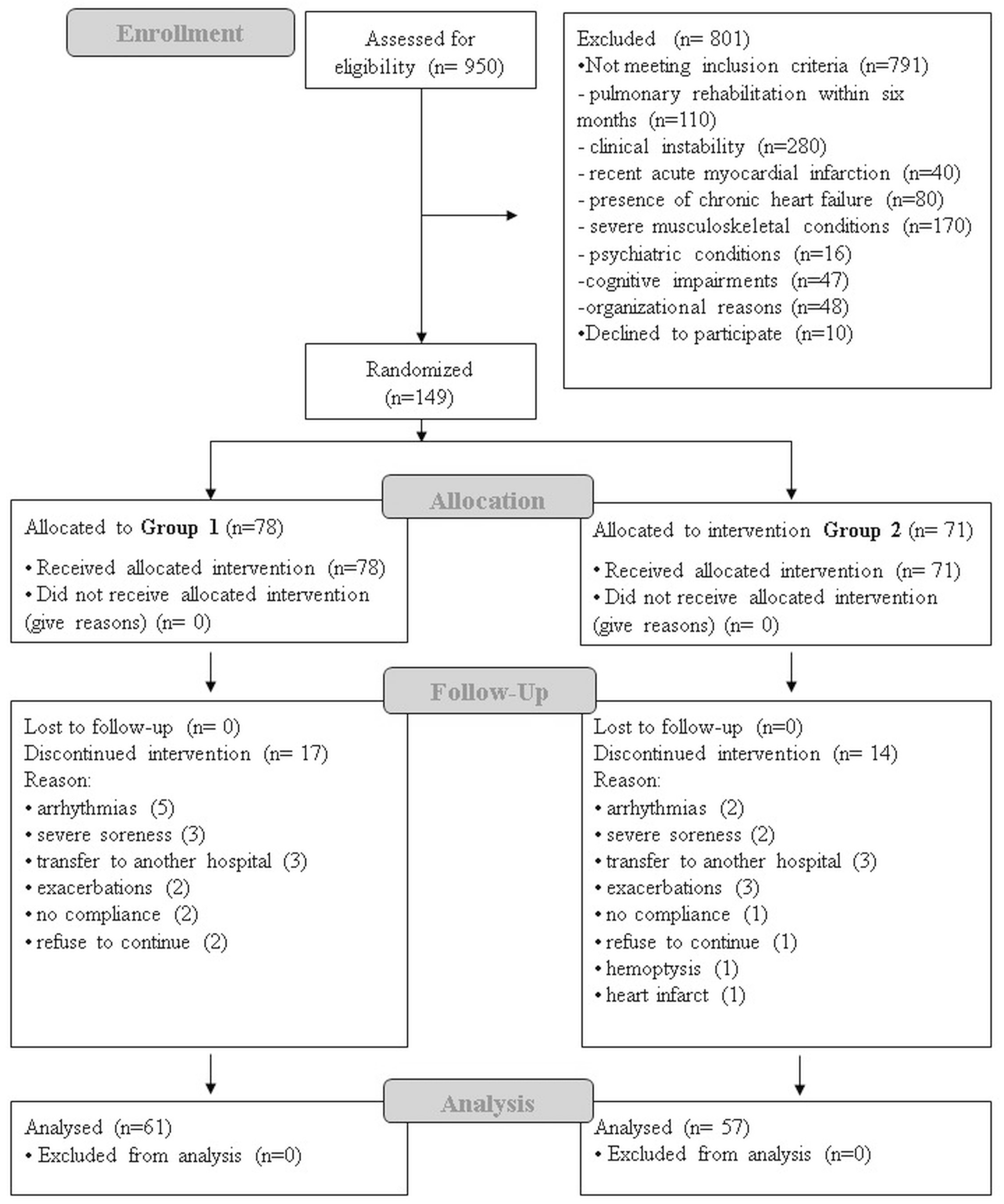
2.1. Study Population
2.2. Study Design
2.3. Assessments
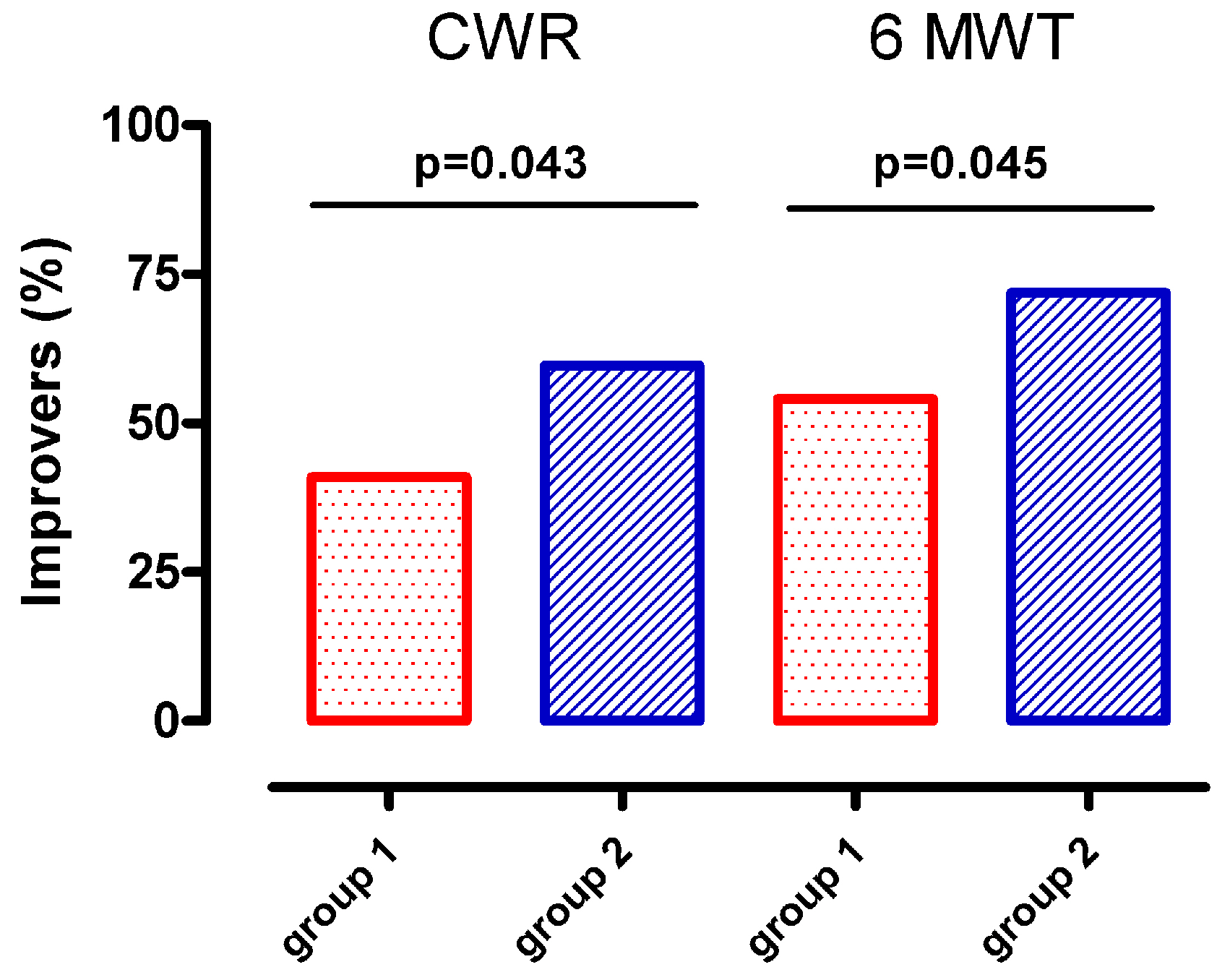
- The Six-Minute Walking Test (6MWT), performed according to ATS/ERS [20]. Supplemental oxygen, when needed (SpO2 < 90%), was delivered at the flow prescribed by the physician and was kept at the same level during both assessment time points. Predictive values were calculated according to Chetta et al. [21]. We evaluated meters walked and percentage of patients that improved above the minimal clinical important difference (MCID) of 30 m [20].
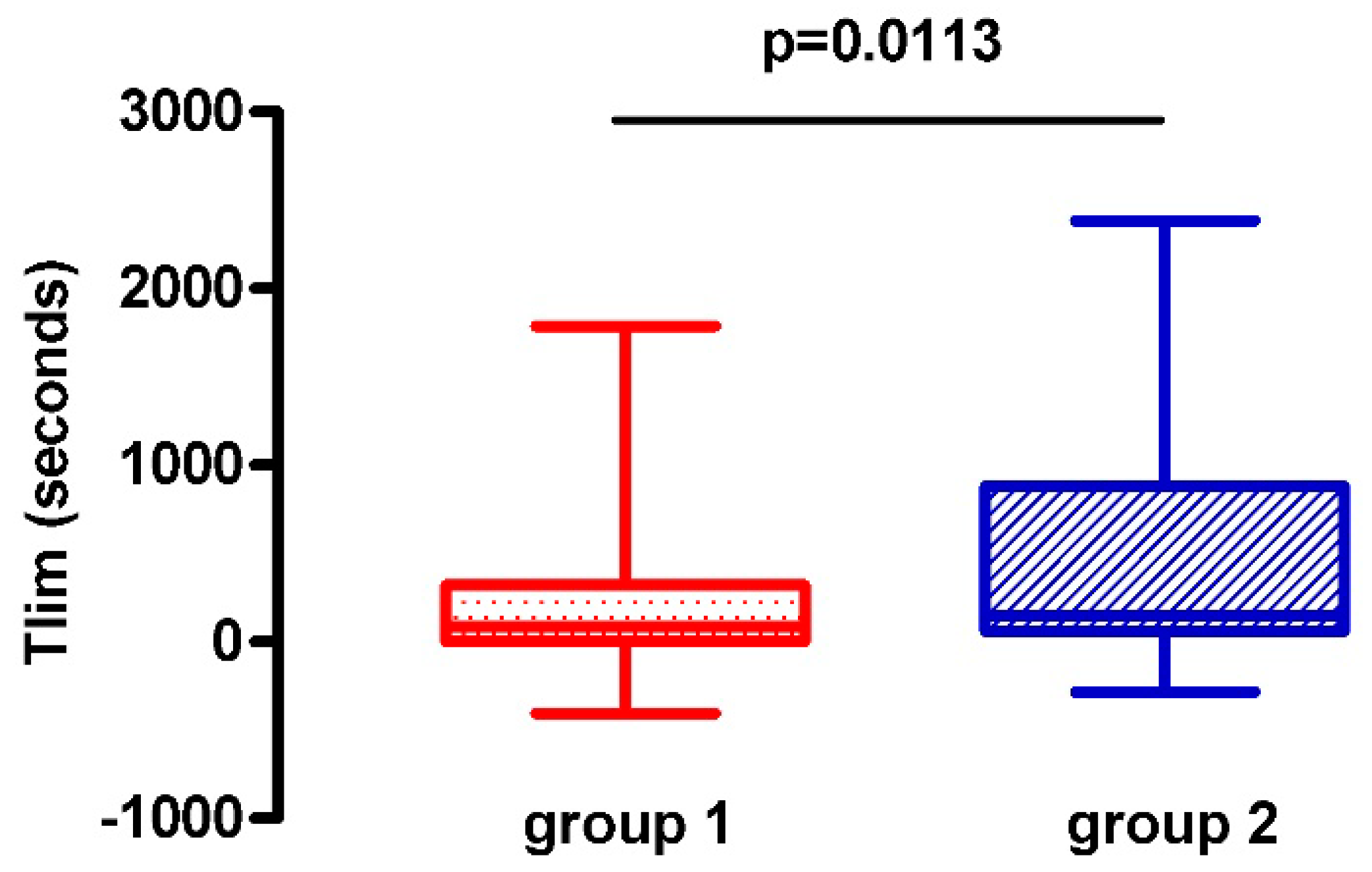
- The Constant Work Rate Exercise Test (CWR) (primary outcome) [22], cycling with a load set at 70% of the individual maximum predicted load, calculated according to the equation of Luxton et al. [23]. Patients pedaled at 50–60 revolutions per minute at constant load until their limit of tolerance (reaching Borg dyspnea or fatigue ≥8, or a ≥90% maximum theoretical heart rate). Endurance time to the limit of tolerance (in seconds) was measured, and pre-to-post variation (before and after the training program) was calculated. We also defined the percentage of patients with an improvement above the minimal clinical important difference (MCID) of 105 s [22].
- Maximal voluntary contraction (MVC) of the quadriceps muscles was carried out using a hand-held dynamometer (Chatillon DMG-200, Ametek, Largo, FL, USA). Body positions for the tests were standardized, and predictive values were calculated using the method proposed by Andrews et al. [26].
- Medical Research Council (MRC) dyspnea, on a 0–5 scale, with 0 corresponding to no dyspnea and 5 to the worse level of dyspnea [27].
2.4. Interventions
2.4.1. Endurance Training
- Group 1 (G1) underwent a single daily 40-min session carried out in the morning or in the afternoon according to individual preferences for 20 consecutive days (20 sessions in total).
- Group 2 (G2) underwent two daily 40-min sessions for 20 consecutive days (40 sessions in total) comprising one session in the morning and one session in the afternoon; sessions were separated by at least three hours of rest in between.
2.4.2. Active Mobilization Exercises
2.5. Statistics
3. Results
3.1. Study Population
3.2. Intervention Results
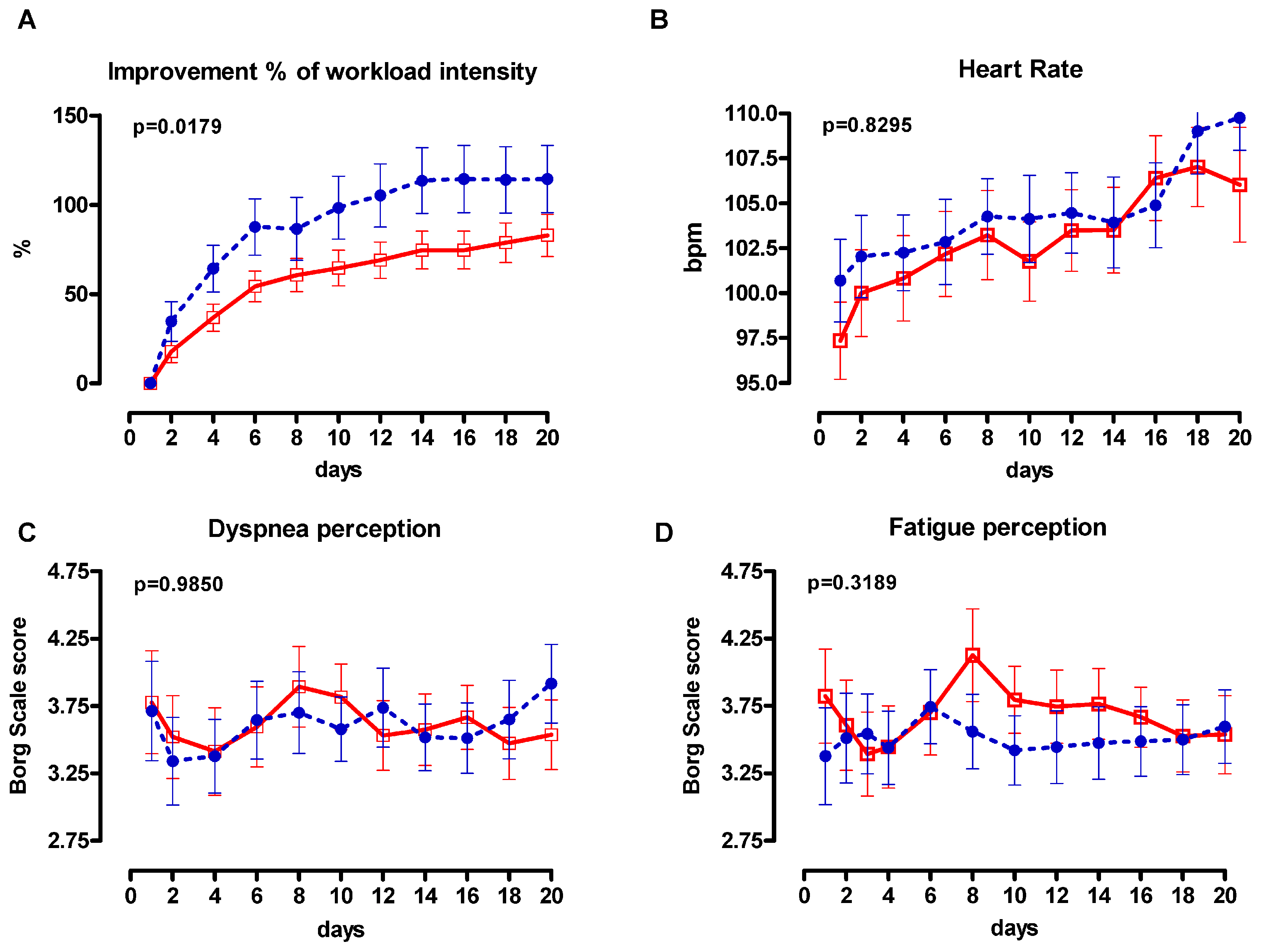
3.3. Training Program Progression
4. Discussion
4.1. Clinical Implications
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- McCarthy, B.; Casey, D.; Devane, D.; Murphy, K.; Murphy, E.; Lacasse, Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2015, Cd003793. [Google Scholar] [CrossRef] [PubMed]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.; et al. An official American Thoracic Society/European Respiratory Society statement: Key concepts and advances in pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, 13–64. [Google Scholar] [CrossRef] [PubMed]
- Clini, E.; Foglio, K.; Bianchi, L.; Porta, R.; Vitacca, M.; Ambrosino, N. In-hospital short-term training program for patients with chronic airway obstruction. Chest 2001, 120, 1500–1505. [Google Scholar] [CrossRef] [PubMed]
- Gormley, S.E.; Swain, D.P.; High, R.; Spina, R.J.; Dowling, E.A.; Kotipalli, U.S.; Gandrakota, R. Effect of intensity of aerobic training on VO2max. Med. Sci. Sports Exerc. 2008, 40, 1336–1343. [Google Scholar] [CrossRef] [PubMed]
- Gass, G.; Gass, E.; Wicks, J.; Browning, J.; Bennett, G.; Morris, N. Rate and amplitude of adaptation to two intensities of exercise in men aged 65–75 yr. Med. Sci. Sports Exerc. 2004, 36, 1811–1818. [Google Scholar] [CrossRef] [PubMed]
- Belman, M.J.; Gaesser, G.A. Exercise training below and above the lactate threshold in the elderly. Med. Sci. Sports Exerc. 1991, 23, 562–568. [Google Scholar] [CrossRef]
- Casaburi, R.; Patessio, A.; Ioli, F.; Zanaboni, S.; Donner, C.F.; Wasserman, K. Reductions in exercise lactic acidosis and ventilation as a result of exercise training in patients with obstructive lung disease. Am. Rev. Respir. Dis. 1991, 143, 9–18. [Google Scholar] [CrossRef]
- Maltais, F.; Bourbeau, J.; Shapiro, S.; Lacasse, Y.; Perrault, H.; Baltzan, M.; Hernandez, P.; Rouleau, M.; Julien, M.; Parenteau, S.; et al. Effects of home-based pulmonary rehabilitation in patients with chronic obstructive pulmonary disease: A randomized trial. Ann. Intern. Med. 2008, 149, 869–878. [Google Scholar] [CrossRef]
- Santos, C.; Rodrigues, F.; Santos, J.; Morais, L.; Barbara, C. Pulmonary Rehabilitation in COPD: Effect of 2 Aerobic Exercise Intensities on Subject-Centered Outcomes—A Randomized Controlled Trial. Respir. Care 2015, 60, 1603–1609. [Google Scholar] [CrossRef]
- Puhan, M.A.; Busching, G.; Schunemann, H.J.; VanOort, E.; Zaugg, C.; Frey, M. Interval versus continuous high-intensity exercise in chronic obstructive pulmonary disease: A randomized trial. Ann. Intern. Med. 2006, 145, 816–825. [Google Scholar] [CrossRef]
- Vogiatzis, I.; Terzis, G.; Nanas, S.; Stratakos, G.; Simoes, D.C.; Georgiadou, O.; Zakynthinos, S.; Roussos, C. Skeletal muscle adaptations to interval training in patients with advanced COPD. Chest 2005, 128, 3838–3845. [Google Scholar] [CrossRef] [PubMed]
- Vogiatzis, I.; Nanas, S.; Roussos, C. Interval training as an alternative modality to continuous exercise in patients with COPD. Eur. Respir. J. 2002, 20, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Morris, N.R.; Walsh, J.; Adams, L.; Alision, J. Exercise training in COPD: What is it about intensity? Respirology 2016, 21, 1185–1192. [Google Scholar] [CrossRef] [PubMed]
- Borde, R.; Hortobagyi, T.; Granacher, U. Dose-Response Relationships of Resistance Training in Healthy Old Adults: A Systematic Review and Meta-Analysis. Sports Med. 2015, 45, 1693–1720. [Google Scholar] [CrossRef] [PubMed]
- Killian, K.J.; Leblanc, P.; Martin, D.H.; Summers, E.; Jones, N.L.; Campbell, E.J. Exercise capacity and ventilatory, circulatory, and symptom limitation in patients with chronic airflow limitation. Am. Rev. Respir. Dis. 1992, 146, 935–940. [Google Scholar] [CrossRef] [PubMed]
- Maltais, F.; LeBlanc, P.; Jobin, J.; Berube, C.; Bruneau, J.; Carrier, L.; Breton, M.J.; Falardeau, G.; Belleau, R. Intensity of training and physiologic adaptation in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 1997, 155, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Decramer, M.; Fabbri, L.M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report. GOLD Executive Summary. Am. J. Respir. Crit. Care Med. 2017, 195, 557–582. [Google Scholar] [CrossRef]
- Magni, E.; Binetti, G.; Bianchetti, A.; Rozzini, R.; Trabucchi, M. Mini-Mental State Examination: A normative study in Italian elderly population. Eur. J. Neurol. 1996, 3, 198–202. [Google Scholar] [CrossRef]
- Salvi, F.; Miller, M.D.; Grilli, A.; Giorgi, R.; Towers, A.L.; Morichi, V.; Spazzafumo, L.; Mancinelli, L.; Espinosa, E.; Rappelli, A.; et al. A manual of guidelines to score the modified cumulative illness rating scale and its validation in acute hospitalized elderly patients. J. Am. Geriatr. Soc. 2008, 56, 1926–1931. [Google Scholar] [CrossRef]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef]
- Chetta, A.; Zanini, A.; Pisi, G.; Aiello, M.; Tzani, P.; Neri, M.; Olivieri, D. Reference values for the 6-min walk test in healthy subjects 20–50 years old. Respir. Med. 2006, 100, 1573–1578. [Google Scholar] [CrossRef] [PubMed]
- Puente-Maestu, L.; Palange, P.; Casaburi, R.; Laveneziana, P.; Maltais, F.; Neder, J.A.; O’Donnell, D.E.; Onorati, P.; Porszasz, J.; Rabinovich, R.; et al. Use of exercise testing in the evaluation of interventional efficacy: An official ERS statement. Eur. Respir. J. 2016, 47, 429–460. [Google Scholar] [CrossRef] [PubMed]
- Luxton, N.; Alison, J.A.; Wu, J.; Mackey, M.G. Relationship between field walking tests and incremental cycloergometry in COPD. Respirology 2008, 13, 856–862. [Google Scholar] [CrossRef] [PubMed]
- ATS/ERS. Statement on respiratory muscle testing. Am. J. Respir. Crit. Care Med. 2002, 166, 518–624. [Google Scholar]
- Black, L.F.; Hyatt, R.E. Maximal respiratory pressures: Normal values and relationship to age and sex. Am. Rev. Respir. Dis. 1969, 99, 696–702. [Google Scholar] [PubMed]
- Andrews, A.W.; Thomas, M.W.; Bohannon, R.W. Normative values for isometric muscle force measurements obtained with hand-held dynamometers. Phys. Ther. 1996, 76, 248–259. [Google Scholar] [CrossRef]
- Parshall, M.B.; Schwartzstein, R.M.; Adams, L.; Banzett, R.B.; Manning, H.L.; Bourbeau, J.; Calverley, P.M.; Gift, A.G.; Harver, A.; Lareau, S.C.; et al. An official American Thoracic Society statement: Update on the mechanisms, assessment, and management of dyspnea. Am. J. Respir. Crit. Care Med. 2012, 185, 435–452. [Google Scholar] [CrossRef]
- Agustí, A.; Soler, J.J.; Molina, J.; Muñoz, M.J.; García-Losa, M.; Roset, M.; Jones, P.W.; Badia, X. Is the CAT questionnaire sensitive to changes in health status in patients with severe COPD exacerbations? COPD J. Chronic Obstr. Pulm. Dis. 2012, 9, 492–498. [Google Scholar] [CrossRef]
- Vidotto, G.; Carone, M.; Jones, P.W.; Salini, S.; Bertolotti, G. Maugeri Respiratory Failure questionnaire reduced form: A method for improving the questionnaire using the Rasch model. Disabil. Rehabil. 2007, 29, 991–998. [Google Scholar] [CrossRef]
- Norman, G. Likert scales, levels of measurement and the laws of statistics. Adv. Health Sci. Educ. Theory Pract. 2010, 15, 625–632. [Google Scholar] [CrossRef]
- Borg, G. Perceived exertion as an indicator of somatic stress. Scand. J. Rehabil. Med. 1970, 2, 92–98. [Google Scholar]
- Gloeckl, R.; Marinov, B.; Pitta, F. Practical recommendations for exercise training in patients with COPD. Eur. Respir. Rev. 2013, 22, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.L.; Holland, A.E. Time to adapt exercise training regimens in pulmonary rehabilitation—A review of the literature. Int. J. Chron. Obstruct. Pulmon. Dis. 2014, 9, 1275–1288. [Google Scholar] [CrossRef] [PubMed]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K.; Saltin, B. Evidence for prescribing exercise as therapy in chronic disease. Scand. J. Med. Sci. Sports 2006, 16, 3–63. [Google Scholar] [CrossRef] [PubMed]
- Zainuldin, R.; Mackey, M.G.; Alison, J.A. Optimal intensity and type of leg exercise training for people with chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2011. [Google Scholar] [CrossRef]
- Almeida, P.; Rodrigues, F. Exercise training modalities and strategies to improve exercise performance in patients with respiratory disease. Rev. Port. Pneumol. 2014, 20, 36–41. [Google Scholar] [CrossRef]
- Sanseverino, M.A.; Pecchiari, M.; Bona, R.L.; Berton, D.C.; de Queiroz, F.B.; Gruet, M.; Peyre-Tartaruga, L.A. Limiting Factors in Walking Performance of Subjects with COPD. Respir. Care 2018, 63, 301–310. [Google Scholar] [CrossRef]
- Ilgin, D.; Ozalevli, S.; Kilinc, O.; Sevinc, C.; Cimrin, A.H.; Ucan, E.S. Gait speed as a functional capacity indicator in patients with chronic obstructive pulmonary disease. Ann. Thorac. Med. 2011, 6, 141–146. [Google Scholar]
- Sillen, M.J.; Vercoulen, J.H.; Hul, A.J.V.T.; Klijn, P.H.; Wouters, E.F.; van Ranst, D.; Peters, J.B.; van Keimpema, A.R.; Franssen, F.M.; Otten, H.J.; et al. Inaccuracy of estimating peak work rate from six-minute walk distance in patients with COPD. COPD 2012, 9, 281–288. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MEASURES | Group 1 (n = 78) | Group 2 (n = 71) | P |
|---|---|---|---|
| Sex, male/female | 60/18 | 53/18 | 0.8200 |
| Age, years | 69 (9) | 69 (8) | 0.9818 |
| BMI, Kg/m2 | 25.53 (5.46) | 25.61 (4.09) | 0.9118 |
| FEV1, %predicted | 39.54 (11.93) | 39.56 (11.36) | 0.9303 |
| FVC, % | 75.03 (19.73) | 75.32 (17.26) | 0.9428 |
| FEV1/FVC | 43.94 (11.41) | 42.75 (10.20) | 0.4930 |
| RV, % | 180 (56) | 180 (53) | 0.7619 |
| MIP, cmH2O | 66.59 (22.28) | 69.43 (25.22) | 0.2517 |
| MEP, cmH2O | 90.33 (35.77) | 85.73 (32.88) | 0.4822 |
| LTOT, % | 60 | 59 | 0.7940 |
| CIRS, 1st item, score | 2.27 (2.92) | 2.09 (3.16) | 0.6939 |
| CIRS, 2nd item, score | 2.51 (1.42) | 2.49 (1.61) | 0.8131 |
| PaO2/FiO2 | 310 (53) | 308 (45) | 0.5410 |
| PaCO2, mmHg | 40.47 (6.31) | 40.54 (5.63) | 0.7083 |
| pH | 7.42 (0.03) | 7.43 (0.03) | 0.0951 |
| 6MWT, meters | 376 (92) | 358 (88) | 0.4202 |
| CWR, s | 288 (226) | 246 (186) | 0.2592 |
| MRC, score | 3.31 (4.13) | 2.57 (1.07) | 0.1630 |
| MVC, quadriceps, Kg | 24 (7) | 24 (9) | 0.9415 |
| MRF26, score | 11.53 (6.811) | 9.98 (5.97) | 0.2058 |
| CAT, score | 21 (7.25) | 20.33 (6.76) | 0.7762 |
| Group 1 (n = 61) | Group 2 (n = 57) | |||||||
|---|---|---|---|---|---|---|---|---|
| Baseline | At the end | P Pre-to-post | Baseline | At the end | P Pre-to-post | Differences between Groups (G2-G1) Mean (IC 95%) | P between Groups | |
| 6MWT, meters | 373 (89) | 416 (89) | 0.001 | 360 (93) | 410 (99) | 0.001 | 7.953 (−14.44, 30.35) | 0.4832 |
| MIP, cmH2O | 67 (23) | 74 (23) | 0.0471 | 72 (26) | 76 (20) | 0.2538 | −3.05 (−11.8, 5.7) | 0.4900 |
| MEP, cmH2O | 92 (39) | 104 (47) | 0.040 | 86 (33) | 99 (34) | 0.0002 | 0.939 (−12.36, 14.23) | 0.8887 |
| Quadriceps, Kg | 24.4 (7.2) | 25.1 (7.5) | 0.5164 | 25 (9.2) | 27 (10.9) | 0.2690 | 1.29(−2.90, 5.48) | 0.5400 |
| MRC, score | 3.6 (4.9) | 1.7 (1.2) | 0.007 | 2.7 (1.1) | 1.5 (1) | 0.0001 | 0.763(−0.07, 2.20) | 0.2960 |
| CAT, score | 21.5 (7.6) | 14.4 (7.8) | 0.001 | 21.1 (7.1) | 11.9 (7) | 0.0001 | −2.03(−5.08,1.02) | 0.1900 |
| MRF, score | 11.53 (6.8) | 8.22 (6.7) | 0.001 | 9.98 (5.97) | 7.28 (5.81) | 0.0001 | 0.6122 (−1.20, 2.43) | 0.5049 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paneroni, M.; Vogiatzis, I.; Belli, S.; Savio, G.; Visca, D.; Zampogna, E.; Aliani, M.; De Carolis, V.; Maniscalco, M.; Simonelli, C.; et al. Is Two Better Than One? The Impact of Doubling Training Volume in Severe COPD: A Randomized Controlled Study. J. Clin. Med. 2019, 8, 1052. https://doi.org/10.3390/jcm8071052
Paneroni M, Vogiatzis I, Belli S, Savio G, Visca D, Zampogna E, Aliani M, De Carolis V, Maniscalco M, Simonelli C, et al. Is Two Better Than One? The Impact of Doubling Training Volume in Severe COPD: A Randomized Controlled Study. Journal of Clinical Medicine. 2019; 8(7):1052. https://doi.org/10.3390/jcm8071052
Chicago/Turabian StylePaneroni, Mara, Ioannis Vogiatzis, Stefano Belli, Gloria Savio, Dina Visca, Elisabetta Zampogna, Maria Aliani, Vito De Carolis, Mauro Maniscalco, Carla Simonelli, and et al. 2019. "Is Two Better Than One? The Impact of Doubling Training Volume in Severe COPD: A Randomized Controlled Study" Journal of Clinical Medicine 8, no. 7: 1052. https://doi.org/10.3390/jcm8071052