Expression of PD-1 and CTLA-4 Are Negative Prognostic Markers in Renal Cell Carcinoma

 ,
,  and
and
Abstract
:1. Introduction
2. Experimental Section
3. Results
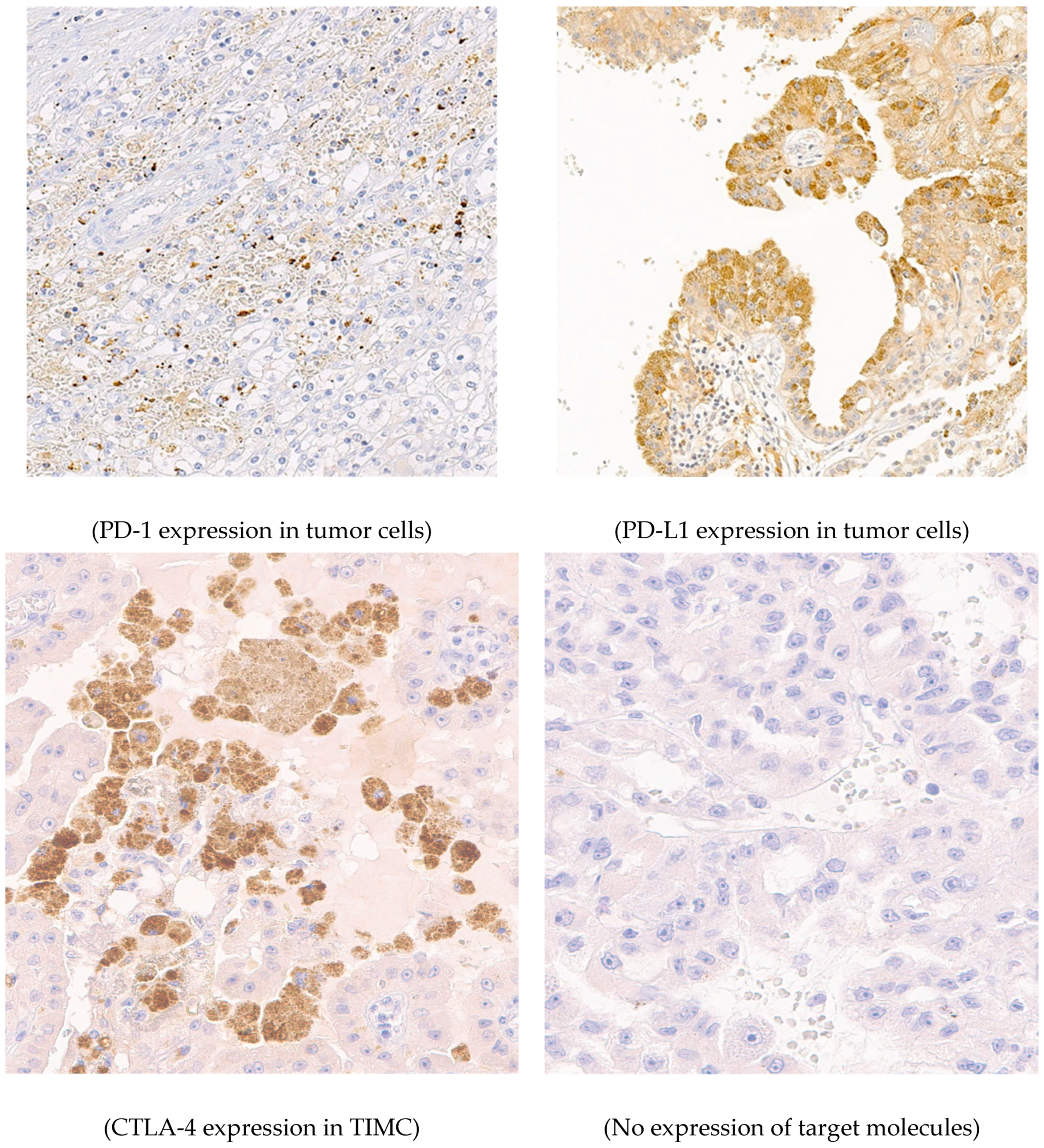
3.1. Patients’ Characteristics and Expression of Target Molecules of CI Therapies
3.2. Survival Analysis
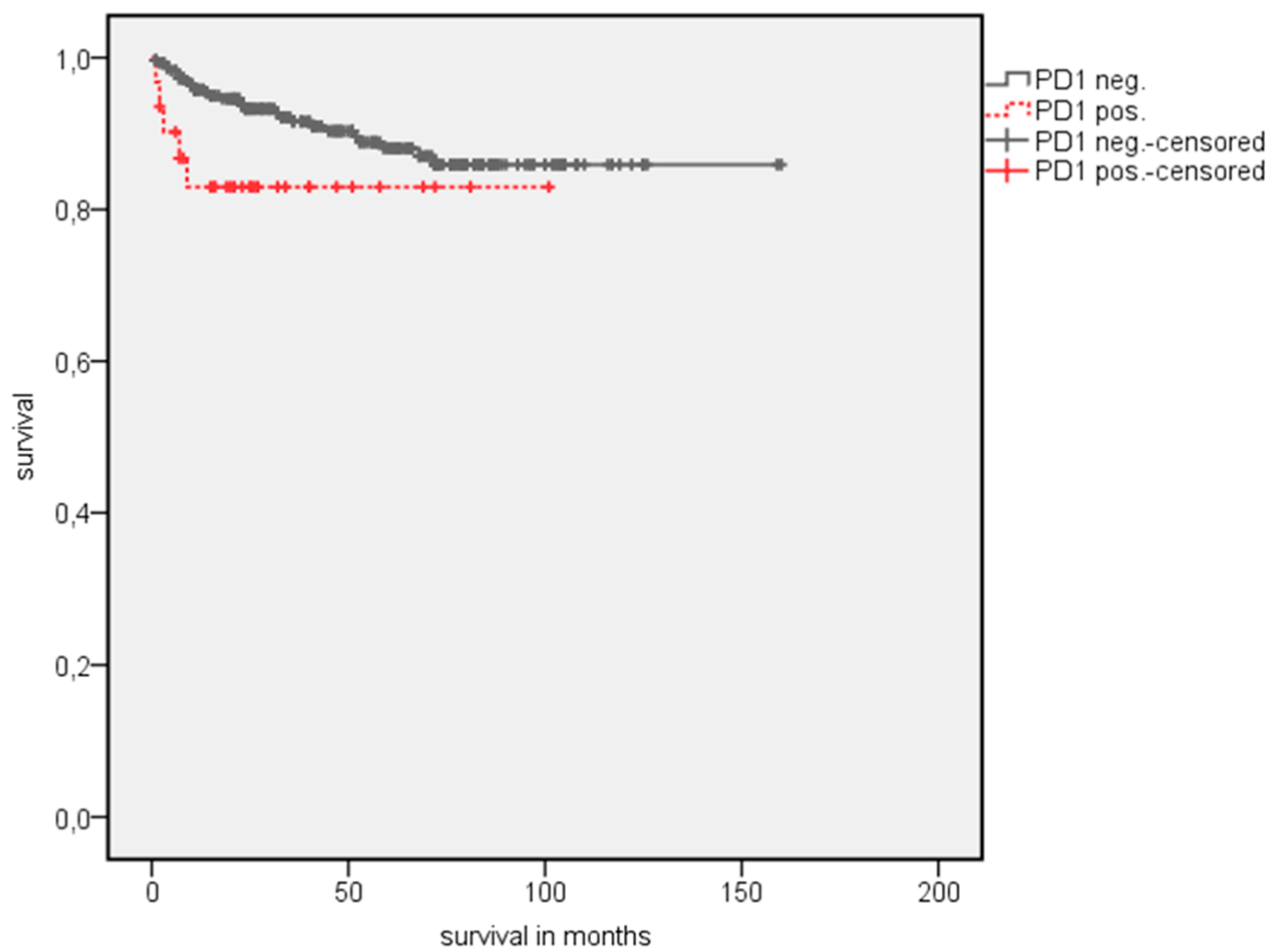
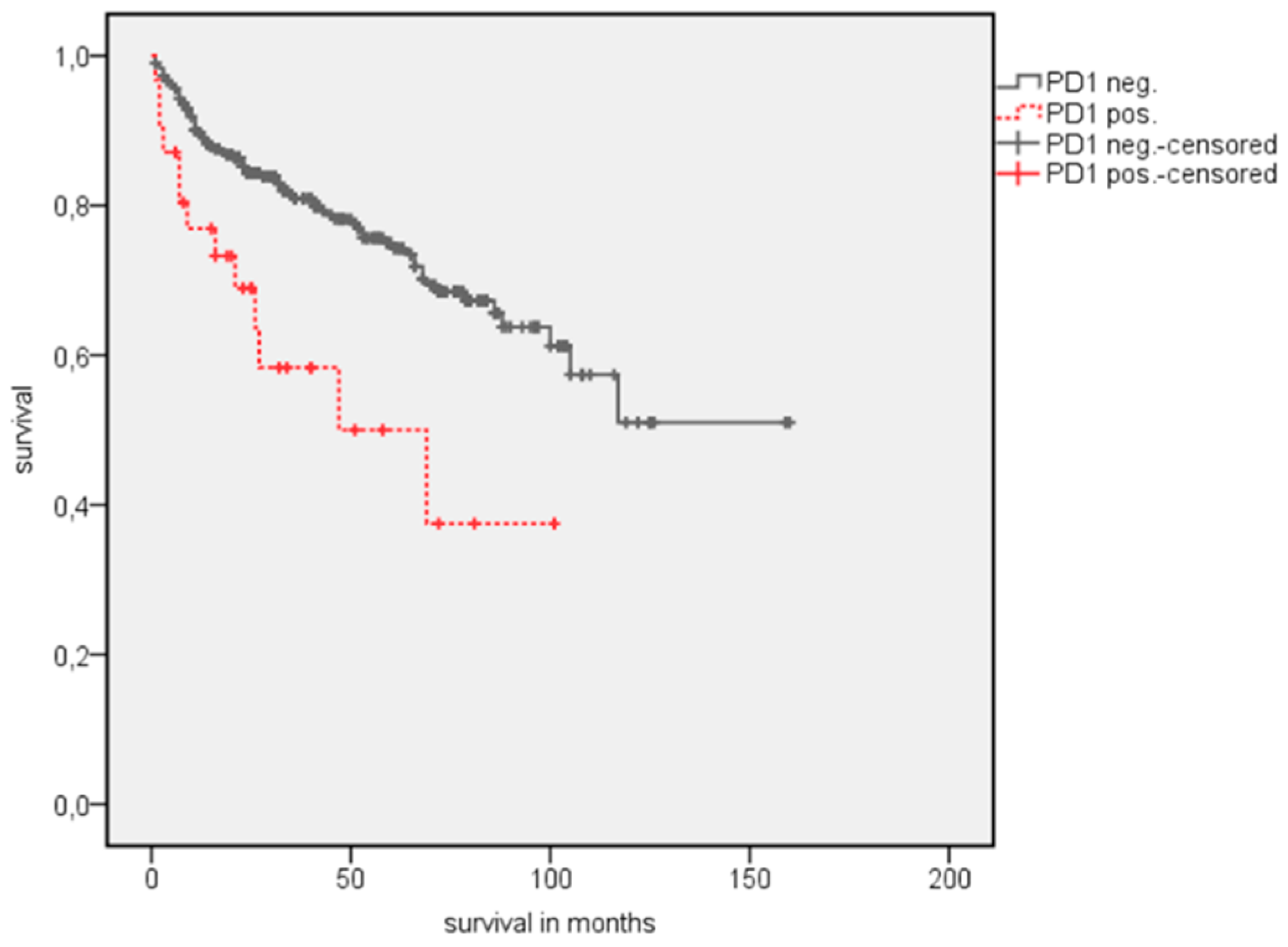
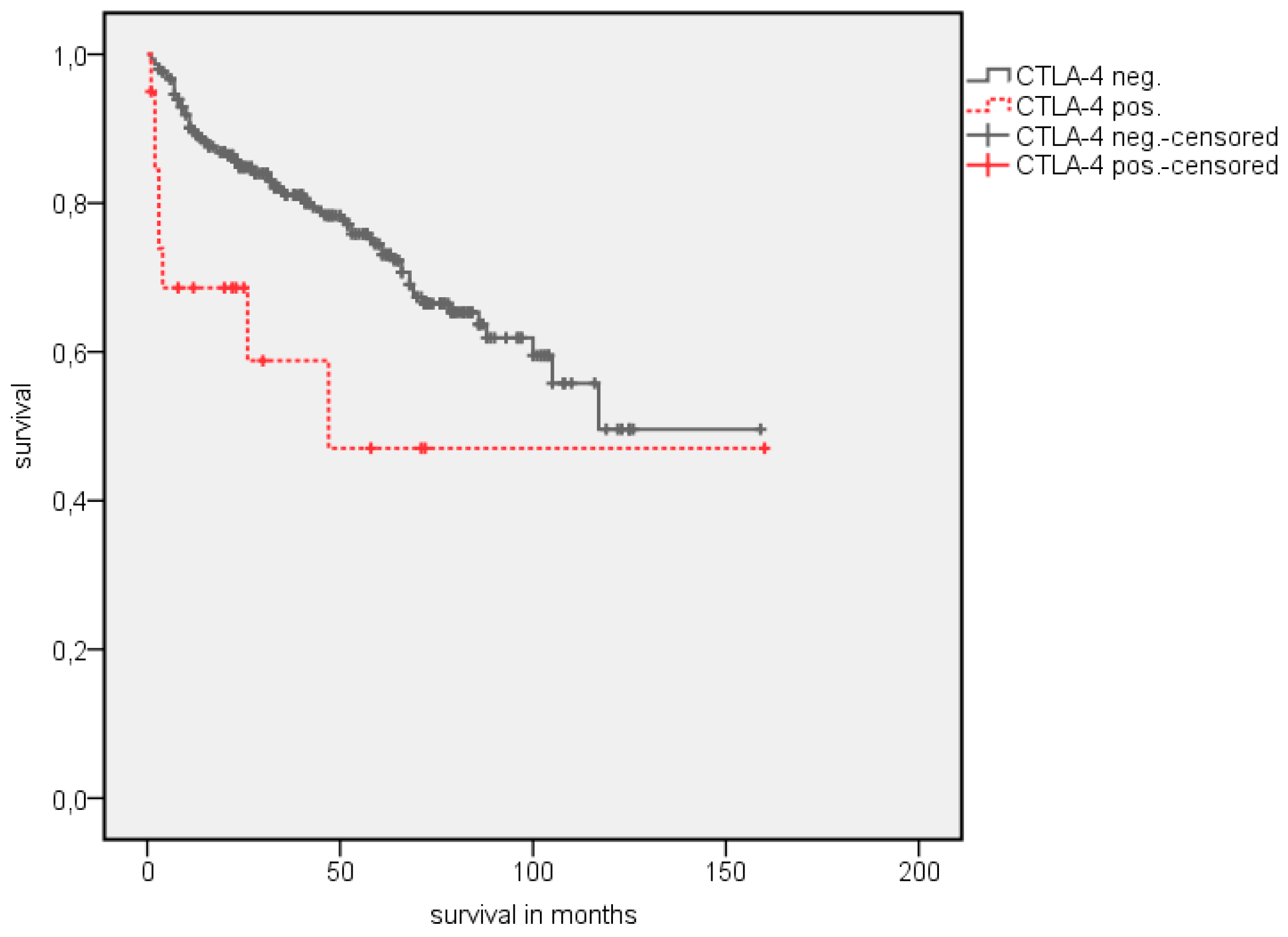
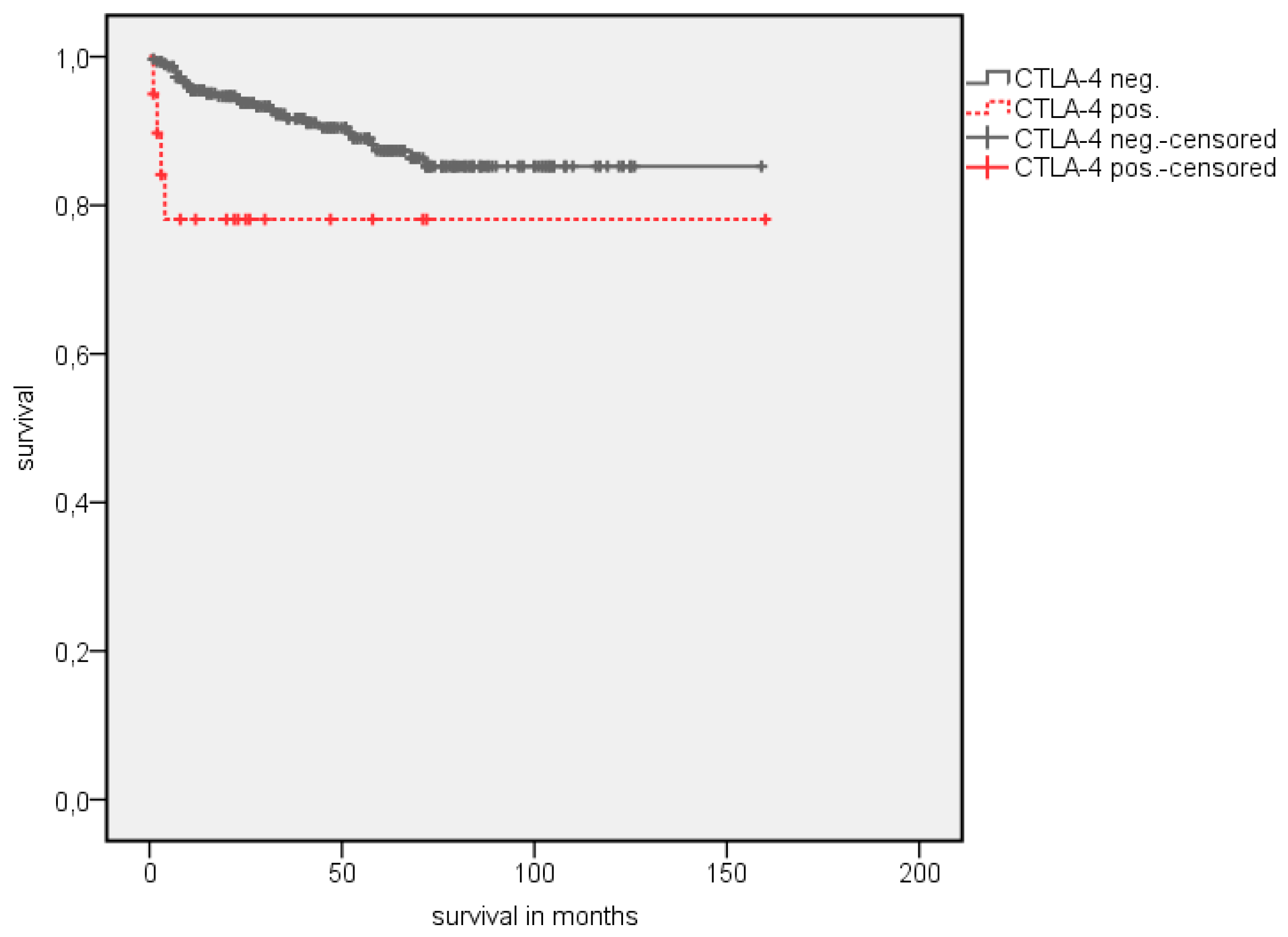
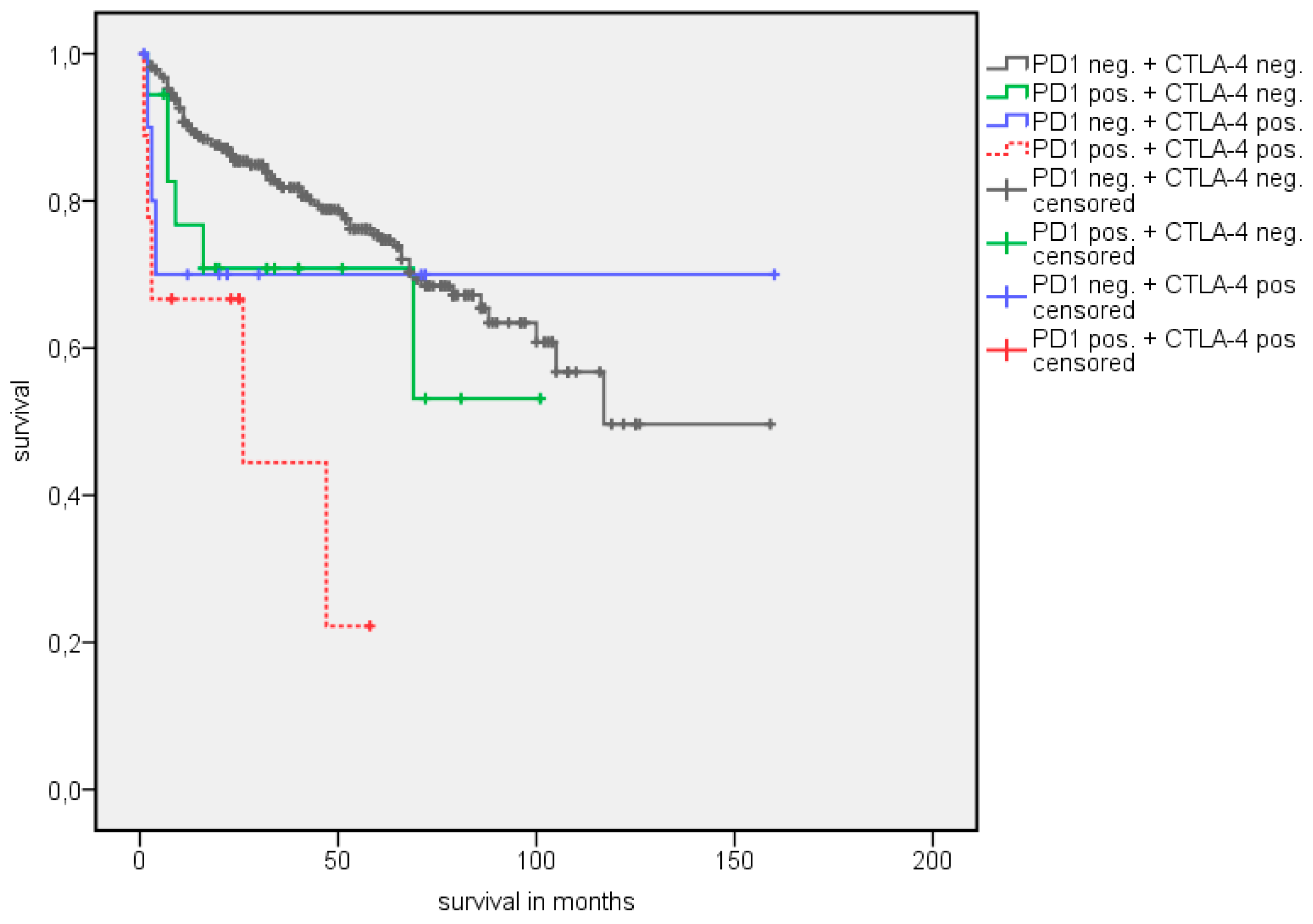
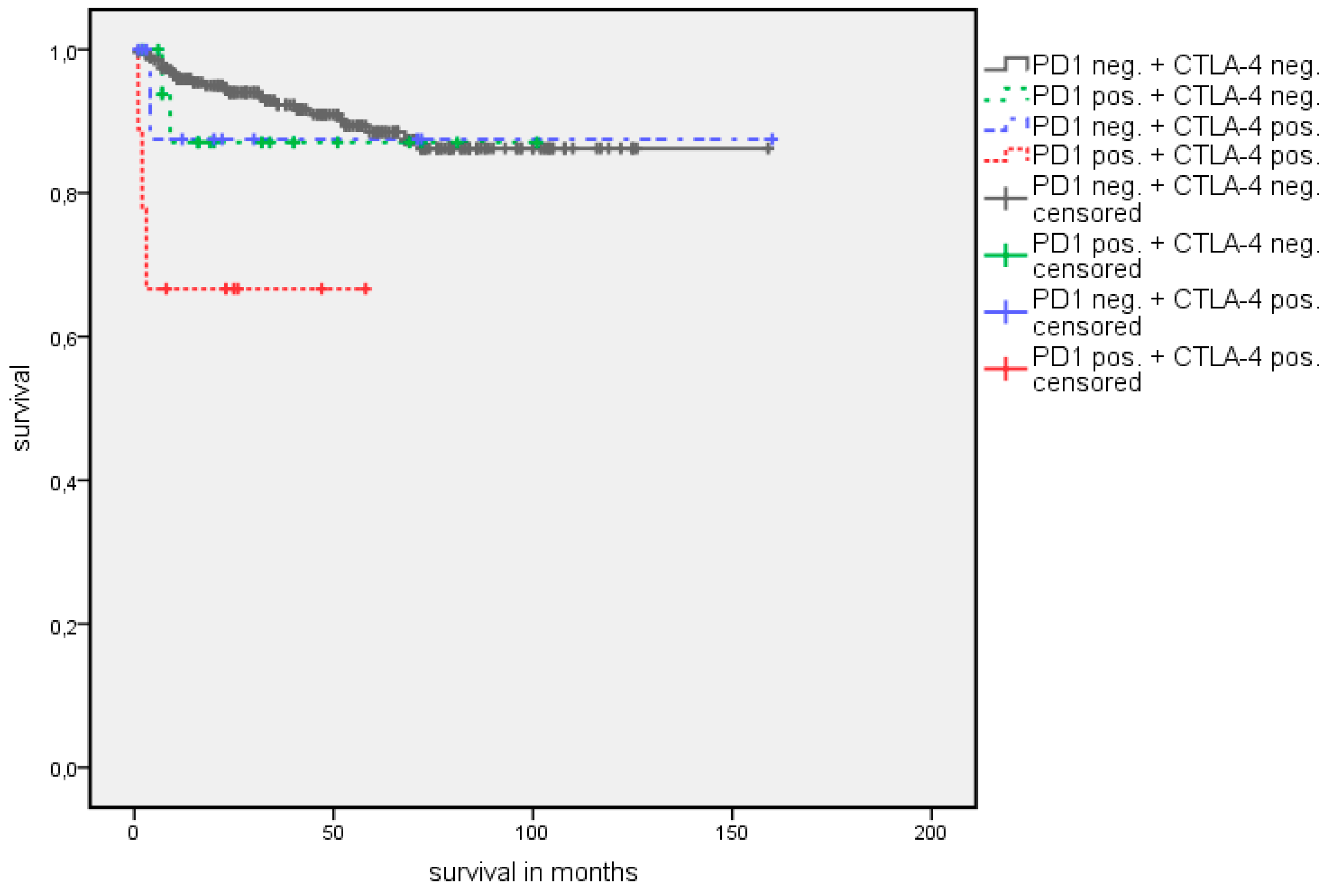
3.2.1. Log Rank Test
3.2.2. Univariate Cox Regression Analysis
3.2.3. Multivariate Cox Regression Analysis
4. Discussion
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics, 2012. CA Cancer J. Clin. 2012, 62, 10–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2015. CA Cancer J. Clin. 2015, 65, 5–29. [Google Scholar] [CrossRef] [PubMed]
- Ljungberg, B.; Bensalah, K.; Canfield, S.; Dabestani, S.; Hofmann, F.; Hora, M.; Kuczyk, M.A.; Lam, T.; Marconi, L.; Merseburger, A.S.; et al. EAU guidelines on renal cell carcinoma: 2014 update. Eur. Urol. 2015, 67, 913–924. [Google Scholar] [CrossRef] [PubMed]
- Lipworth, L.; Tarone, R.E.; Lund, L.; McLaughlin, J.K. Epidemiologic characteristics and risk factors for renal cell cancer. Clin. Epidemiol. 2009, 1, 33–43. [Google Scholar] [PubMed] [Green Version]
- Rini, B.I.; Campbell, S.C.; Escudier, B. Renal cell carcinoma. Lancet 2009, 373, 1119–1132. [Google Scholar] [CrossRef]
- Heng, D.Y.; Xie, W.; Regan, M.M.; Warren, M.A.; Golshayan, A.R.; Sahi, C.; Eigl, B.J.; Ruether, J.D.; Cheng, T.; North, S.; et al. Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor-targeted agents: Results from a large, multicenter study. J. Clin. Oncol. 2009, 27, 5794–5799. [Google Scholar] [CrossRef] [PubMed]
- Shah, B.K.; Ghimire, K.B. Survival trends among patients with advanced renal cell carcinoma in the United States. Urol. Int. 2015, 94, 133–136. [Google Scholar] [CrossRef]
- Marschner, N.; Staehler, M.; Muller, L.; Nusch, A.; Harde, J.; Koska, M.; Janicke, M.; Goebell, P.J. Survival of Patients with Advanced or Metastatic Renal Cell Carcinoma in Routine Practice Differs from That in Clinical Trials-Analyses From the German Clinical RCC Registry. Clin. Genitourin. Cancer 2017, 15, e209–e215. [Google Scholar] [CrossRef]
- Mazza, C.; Escudier, B.; Albiges, L. Nivolumab in renal cell carcinoma: Latest evidence and clinical potential. Ther. Adv. Med. Oncol. 2017, 9, 171–181. [Google Scholar] [CrossRef]
- Thorsson, V.; Gibbs, D.L.; Brown, S.D.; Wolf, D.; Bortone, D.S.; Ou Yang, T.H.; Porta-Pardo, E.; Gao, G.F.; Plaisier, C.L.; Eddy, J.A.; et al. The Immune Landscape of Cancer. Immunity 2018, 48, 812–830. [Google Scholar] [CrossRef] [PubMed]
- Holzman, S.A.; de la Calle, C.M.; Kissick, H.T.; Osunkoya, A.O.; Pollack, B.P.; Patil, D.; Ogan, K.; Master, V.A. High Expression of Major Histocompatibility Complex Class I in Clear Cell Renal Cell Carcinoma Is Associated with Improved Prognosis. Urol. Int. 2015, 95, 72–78. [Google Scholar] [CrossRef]
- Bedke, J.; Stuhler, V.; Stenzl, A.; Brehmer, B. Immunotherapy for kidney cancer: Status quo and the future. Curr. Opin. Urol. 2018, 28, 8–14. [Google Scholar] [CrossRef]
- Sittig, S.P.; Kollgaard, T.; Gronbaek, K.; Idorn, M.; Hennenlotter, J.; Stenzl, A.; Gouttefangeas, C.; Thor Straten, P. Clonal expansion of renal cell carcinoma-infiltrating T lymphocytes. Oncoimmunology 2013, 2, e26014. [Google Scholar] [CrossRef] [Green Version]
- Hegde, N.; Melanson, E.; Sazonov, E. Development of a real time activity monitoring Android application utilizing SmartStep. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 1886–1889. [Google Scholar] [CrossRef]
- Kim, K.S.; Sekar, R.R.; Patil, D.; Dimarco, M.A.; Kissick, H.T.; Bilen, M.A.; Osunkoya, A.O.; Master, V.A. Evaluation of programmed cell death protein 1 (PD-1) expression as a prognostic biomarker in patients with clear cell renal cell carcinoma. Oncoimmunology 2018, 7, e1413519. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.J.; Kim, K.M.; Bae, J.S.; Park, H.S.; Lee, H.; Chung, M.J.; Moon, W.S.; Lee, D.G.; Jang, K.Y. Tumor-infiltrating PD1-Positive Lymphocytes and FoxP3-Positive Regulatory T Cells Predict Distant Metastatic Relapse and Survival of Clear Cell Renal Cell Carcinoma. Transl. Oncol. 2013, 6, 282–289. [Google Scholar] [CrossRef] [Green Version]
- Thompson, R.H.; Gillett, M.D.; Cheville, J.C.; Lohse, C.M.; Dong, H.; Webster, W.S.; Krejci, K.G.; Lobo, J.R.; Sengupta, S.; Chen, L.; et al. Costimulatory B7-H1 in renal cell carcinoma patients: Indicator of tumor aggressiveness and potential therapeutic target. Proc. Natl. Acad. Sci. USA 2004, 101, 17174–17179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, R.H.; Kuntz, S.M.; Leibovich, B.C.; Dong, H.; Lohse, C.M.; Webster, W.S.; Sengupta, S.; Frank, I.; Parker, A.S.; Zincke, H.; et al. Tumor B7-H1 is associated with poor prognosis in renal cell carcinoma patients with long-term follow-up. Cancer Res. 2006, 66, 3381–3385. [Google Scholar] [CrossRef] [PubMed]
- Choueiri, T.K.; Fay, A.P.; Gray, K.P.; Callea, M.; Ho, T.H.; Albiges, L.; Bellmunt, J.; Song, J.; Carvo, I.; Lampron, M.; et al. PD-L1 expression in nonclear-cell renal cell carcinoma. Ann. Oncol. 2014, 25, 2178–2184. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Figueroa, D.J.; Fay, A.P.; Signoretti, S.; Liu, Y.; Gagnon, R.; Deen, K.; Carpenter, C.; Benson, P.; Ho, T.H.; et al. Correlation of PD-L1 tumor expression and treatment outcomes in patients with renal cell carcinoma receiving sunitinib or pazopanib: Results from COMPARZ, a randomized controlled trial. Clin. Cancer Res. 2015, 21, 1071–1077. [Google Scholar] [CrossRef]
- Xu, F.; Xu, L.; Wang, Q.; An, G.; Feng, G.; Liu, F. Clinicopathological and prognostic value of programmed death ligand-1 (PD-L1) in renal cell carcinoma: A meta-analysis. Int. J. Clin. Exp. Med. 2015, 8, 14595–14603. [Google Scholar]
- Fukuda, T.; Kamai, T.; Masuda, A.; Nukui, A.; Abe, H.; Arai, K.; Yoshida, K. Higher preoperative serum levels of PD-L1 and B7-H4 are associated with invasive and metastatic potential and predictable for poor response to VEGF-targeted therapy and unfavorable prognosis of renal cell carcinoma. Cancer Med. 2016, 5, 1810–1820. [Google Scholar] [CrossRef]
- Iacovelli, R.; Nole, F.; Verri, E.; Renne, G.; Paglino, C.; Santoni, M.; Cossu Rocca, M.; Giglione, P.; Aurilio, G.; Cullura, D.; et al. Prognostic Role of PD-L1 Expression in Renal Cell Carcinoma. A Systematic Review and Meta-Analysis. Targeted Oncol. 2016, 11, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Krummel, M.F.; Allison, J.P. CD28 and CTLA-4 have opposing effects on the response of T cells to stimulation. J. Exp. Med. 1995, 182, 459–465. [Google Scholar] [CrossRef]
- Fife, B.T.; Bluestone, J.A. Control of peripheral T-cell tolerance and autoimmunity via the CTLA-4 and PD-1 pathways. Immunol. Rev. 2008, 224, 166–182. [Google Scholar] [CrossRef] [PubMed]
- Buchbinder, E.I.; Desai, A. CTLA-4 and PD-1 Pathways: Similarities, Differences, and Implications of Their Inhibition. Am. J. Clin. Oncol. 2016, 39, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Brunet, J.F.; Denizot, F.; Luciani, M.F.; Roux-Dosseto, M.; Suzan, M.; Mattei, M.G.; Golstein, P. A new member of the immunoglobulin superfamily—CTLA-4. Nature 1987, 328, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Walunas, T.L.; Bakker, C.Y.; Bluestone, J.A. CTLA-4 ligation blocks CD28-dependent T cell activation. J. Exp. Med. 1996, 183, 2541–2550. [Google Scholar] [CrossRef] [PubMed]
- Zou, W.; Chen, L. Inhibitory B7-family molecules in the tumour microenvironment. Nat. Rev. Immunol. 2008, 8, 467–477. [Google Scholar] [CrossRef]
- Geissler, K.; Fornara, P.; Lautenschlager, C.; Holzhausen, H.J.; Seliger, B.; Riemann, D. Immune signature of tumor infiltrating immune cells in renal cancer. Oncoimmunology 2015, 4, e985082. [Google Scholar] [CrossRef]
- Tupikowski, K.; Partyka, A.; Kolodziej, A.; Dembowski, J.; Debinski, P.; Halon, A.; Zdrojowy, R.; Frydecka, I.; Karabon, L. CTLA-4 and CD28 genes’ polymorphisms and renal cell carcinoma susceptibility in the Polish population—A prospective study. Tissue Antigens 2015, 86, 353–361. [Google Scholar] [CrossRef]
- Liu, X.; Swen, J.J.; Diekstra, M.H.M.; Boven, E.; Castellano, D.; Gelderblom, H.; Mathijssen, R.H.J.; Vermeulen, S.H.; Oosterwijk, E.; Junker, K.; et al. A Genetic Polymorphism in CTLA-4 Is Associated with Overall Survival in Sunitinib-Treated Patients with Clear Cell Metastatic Renal Cell Carcinoma. Clin. Cancer Res. 2018. [Google Scholar] [CrossRef]
- Zhu, J.; Armstrong, A.J.; Friedlander, T.W.; Kim, W.; Pal, S.K.; George, D.J.; Zhang, T. Biomarkers of immunotherapy in urothelial and renal cell carcinoma: PD-L1, tumor mutational burden, and beyond. J. Immunother. Cancer 2018, 6, 4. [Google Scholar] [CrossRef] [Green Version]
- Jasinski-Bergner, S.; Stoehr, C.; Bukur, J.; Massa, C.; Braun, J.; Huttelmaier, S.; Spath, V.; Wartenberg, R.; Legal, W.; Taubert, H.; et al. Clinical relevance of miR-mediated HLA-G regulation and the associated immune cell infiltration in renal cell carcinoma. Oncoimmunology 2015, 4, e1008805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, L. Labor und Diagnose; Th-Books Gmbh: Frankfurt am Main, Germany, 2005. [Google Scholar]
- Motzer, R.J.; Tannir, N.M.; McDermott, D.F.; Aren Frontera, O.; Melichar, B.; Choueiri, T.K.; Plimack, E.R.; Barthelemy, P.; Porta, C.; George, S.; et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2018, 378, 1277–1290. [Google Scholar] [CrossRef]
- Erlmeier, F.; Weichert, W.; Schrader, A.J.; Autenrieth, M.; Hartmann, A.; Steffens, S.; Ivanyi, P. Prognostic impact of PD-1 and its ligands in renal cell carcinoma. Med. Oncol. 2017, 34, 99. [Google Scholar] [CrossRef]
- George, D.J.; Martini, J.F.; Staehler, M.; Motzer, R.J.; Magheli, A.; Escudier, B.; Gerletti, P.; Li, S.; Casey, M.; Laguerre, B.; et al. Immune Biomarkers Predictive for Disease-Free Survival with Adjuvant Sunitinib in High-Risk Locoregional Renal Cell Carcinoma: From Randomized Phase III S-TRAC Study. Clin. Cancer Res. 2018. [Google Scholar] [CrossRef]
- Leach, D.R.; Krummel, M.F.; Allison, J.P. Enhancement of antitumor immunity by CTLA-4 blockade. Science 1996, 271, 1734–1736. [Google Scholar] [CrossRef]
- Lipson, E.J.; Drake, C.G. Ipilimumab: An anti-CTLA-4 antibody for metastatic melanoma. Clin. Cancer Res. 2011, 17, 6958–6962. [Google Scholar] [CrossRef] [PubMed]
- Ribas, A.; Tumeh, P.C. The future of cancer therapy: Selecting patients likely to respond to PD1/L1 blockade. Clin. Cancer Res. 2014, 20, 4982–4984. [Google Scholar] [CrossRef]
- Rodriguez-Vida, A.; Strijbos, M.; Hutson, T. Predictive and prognostic biomarkers of targeted agents and modern immunotherapy in renal cell carcinoma. ESMO Open 2016, 1, e000013. [Google Scholar] [CrossRef] [Green Version]
- Motzer, R.J.; Escudier, B.; McDermott, D.F.; George, S.; Hammers, H.J.; Srinivas, S.; Tykodi, S.S.; Sosman, J.A.; Procopio, G.; Plimack, E.R.; et al. Nivolumab versus Everolimus in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2015, 373, 1803–1813. [Google Scholar] [CrossRef] [PubMed]
- Gandini, S.; Massi, D.; Mandala, M. PD-L1 expression in cancer patients receiving anti PD-1/PD-L1 antibodies: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2016, 100, 88–98. [Google Scholar] [CrossRef]
- Thompson, R.H.; Dong, H.; Kwon, E.D. Implications of B7-H1 expression in clear cell carcinoma of the kidney for prognostication and therapy. Clin. Cancer Res. 2007, 13, 709s–715s. [Google Scholar] [CrossRef] [PubMed]
- Jilaveanu, L.B.; Shuch, B.; Zito, C.R.; Parisi, F.; Barr, M.; Kluger, Y.; Chen, L.; Kluger, H.M. PD-L1 Expression in Clear Cell Renal Cell Carcinoma: An Analysis of Nephrectomy and Sites of Metastases. J. Cancer 2014, 5, 166–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Callea, M.; Albiges, L.; Gupta, M.; Cheng, S.C.; Genega, E.M.; Fay, A.P.; Song, J.; Carvo, I.; Bhatt, R.S.; Atkins, M.B.; et al. Differential Expression of PD-L1 between Primary and Metastatic Sites in Clear-Cell Renal Cell Carcinoma. Cancer Immunol. Res. 2015, 3, 1158–1164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDermott, D.F.; Huseni, M.A.; Atkins, M.B.; Motzer, R.J.; Rini, B.I.; Escudier, B.; Fong, L.; Joseph, R.W.; Pal, S.K.; Reeves, J.A.; et al. Clinical activity and molecular correlates of response to atezolizumab alone or in combination with bevacizumab versus sunitinib in renal cell carcinoma. Nat. Med. 2018, 24, 749–757. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Rini, B.; Garcia, J.A.; Baz, R.C.; Abou-Jawde, R.M.; Thakkar, S.G.; Elson, P.; Mekhail, T.M.; Zhou, M.; Bukowski, R.M. Prognostic factors associated with long-term survival in previously untreated metastatic renal cell carcinoma. Ann. Oncol. 2007, 18, 249–255. [Google Scholar] [CrossRef]
- Noessner, E.; Brech, D.; Mendler, A.N.; Masouris, I.; Schlenker, R.; Prinz, P.U. Intratumoral alterations of dendritic-cell differentiation and CD8(+) T-cell anergy are immune escape mechanisms of clear cell renal cell carcinoma. Oncoimmunology 2012, 1, 1451–1453. [Google Scholar] [CrossRef]
- Perez-Gracia, J.L.; Labiano, S.; Rodriguez-Ruiz, M.E.; Sanmamed, M.F.; Melero, I. Orchestrating immune check-point blockade for cancer immunotherapy in combinations. Curr. Opin. Immunol. 2014, 27, 89–97. [Google Scholar] [CrossRef]
- Erlmeier, F.; Hartmann, A.; Autenrieth, M.; Wiedemann, M.; Ivanyi, P.; Steffens, S.; Weichert, W. PD-1/PD-L1 expression in chromophobe renal cell carcinoma: An immunological exception? Med. Oncol. 2016, 33, 120. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All RCC | PD-1 Positive in TIMC | PD-L1 Positive in Tumor Cells | PD-L1 Positive in TIMC | CTLA-4 ≥ 2% in TIMC | PD-1 in TIMC Positive and CTLA-4 in TIMC ≥ 2% | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n = 342 | n = 31 (9.4%) | p-Value | n = 41 (12.3%) | p-Value | n = 16 (4.8%) | p-Value | n = 20 (6.3%) | p-Value | n = 9 (2.9%) | p-Value | |
| Age median | 66.0 | 69 | 67.0 | 67.5 | 69.5 | 73 | |||||
| (range) | (23–92) | (40–84) | 0.576 | (28–83) | 0.842 | (46–80) | 0.887 | (46–79) | 0.191 | (57–79) | 0.339 |
| Gender | |||||||||||
| female | 121 (35.4%) | 7 (5.9%) | 11 (9.2%) | 8 (6.7%) | 4 (3.6%) | 4 (3.6%) | |||||
| male | 221 (64.6%) | 24 (11.3%) | 0.108 | 30 (14%) | 0.210 | 8 (3.7%) | 0.224 | 16 (7.7%) | 0.147 | 5 (2.5%) | 0.064 |
| Histology | |||||||||||
| clear cell | 270 (78.9%) | 25 (9.6%) | 24 (9.1%) | 10 (3.8%) | 15 (6.0%) | 7 (2.8%) | |||||
| papillary | 41 (12.0%) | 5 (12.8%) | 0.536 | 13 (32.5%) | <0.001 ** | 3 (7.7%) | 0.265 | 3 (7.9%) | 0.650 | 2 (5.4%) | 0.037 |
| chromophobe | 24 (7.0%) | 0 (0%) | 0.112 | 1 (4.2%) | 0.411 | 1 (4.2%) | 0.929 | 0 (0%) | 0.220 | 0 (0%) | 0.095 |
| other | 7 (2%) | 1 (14.3%) | 0.682 | 3 (42.9%) | 0.003 * | 2 (28.6%) | 0.002 * | 2 (28.6%) | 0.017 * | 0 (0%) | 0.088 |
| Grade | |||||||||||
| G1 | 43 (12.6%) | 2 (5.0%) | 3 (7.5%) | 1 (2.5%) | 2 (5.1%) | 2 (5.1%) | |||||
| G2 | 219 (64.2%) | 13 (6.1%) | 0.782 | 23 (10.6%) | 0.547 | 9 (4.2%) | 0.616 | 12 (5.9%) | 0.859 | 4 (2.0%) | 0.862 |
| G3 | 79 (23.2%) | 16 (20.8%) | <0.001 ** | 15 (19.5%) | 0.029* | 6 (7.8%) | 0.166 | 6 (8.0%) | 0.481 | 3 (4.1%) | 0.005 * |
| Stage | |||||||||||
| pT1 and pT2 | 247 (74.6%) | 18 (7.6%) | 29 (12.1%) | 12 (5.0%) | 12 (5.2%) | 4 (1.8%) | |||||
| pT3 and pT4 | 84 (25.4%) | 12 (14.3%) | 0.071 | 10 (11.9%) | 0.956 | 4 (4.8%) | 0.942 | 8 (10.0%) | 0.135 | 5 (6.3%) | 0.037 * |
| Metastases | |||||||||||
| non-metastatic | 262 (76.6%) | 18 (7.2%) | 37 (14.4%) | 15 (5.8%) | 12 (4.9%) | 5 (2.1%) | |||||
| primary metastatic | 37 (10.8%) | 8 (21.6%) | 0.007* | 3 (8.1%) | 0.482 | 0 (0%) | 0.161 | 6 (16.7%) | 0.006 ** | 3 (8.3%) | <0.001 ** |
| secondary metastatic | 43 (12.6%) | 5 (11.6%) | 0.320 | 1 (2.4%) | 0.030 * | 1 (2.4%) | 0.372 | 2 (4.9%) | 0.987 | 1 (2.4%) | 0.620 |
| ECOG | |||||||||||
| 0 | 209 (73.6%) | 17 (8.3%) | 28 (13.7%) | 11 (5.4%) | 11 (5.7%) | 3 (1.6%) | |||||
| >0 | 75 (26.4%) | 10 (13.9%) | 0.174 | 9 (12.2%) | 0.736 | 4 (5.4%) | 0.997 | 6 (8.3%) | 0.432 | 4 (5.7%) | 0.186 |
| Survival | |||||||||||
| OS | 250 (73.1%) | 18 (58.1%) | 0.044 * | 29 (70.7%) | 0.686 | 12 (75%) | 0.895 | 12 (60%) | 0.173 | 4 (44%) | 0.050 * |
| CSS | 307 (89.8%) | 26 (83.9%) | 0.233 | 37 (90.2%) | 0.924 | 16 (100%) | 0.175 | 16 (80%) | 0.142 | 6 (66%) | 0.055 |
| PD-1 Positive in TIMC | PD-L1 Positive in Tumor Cells | PD-L1 Positive in TIMC | CTLA-4 ≥2 % in TIMC | PD-1 in TIMC Positive and CTLA-4 in TIMC ≥ 2% | ||
|---|---|---|---|---|---|---|
| Pearson Correlation | PD-1 positive in TIMC | 1 | 0.171 ** | 0.030 | 0.339 ** | 0.845 ** |
| Significance (p-value) | 0.002 ** | 0.588 | <0.001 ** | <0.001 ** | ||
| Pearson Correlation | PD-L1 positive in tumor cells | 0.171 ** | 1 | 0.044 | 0.281 ** | 0.273 ** |
| Significance (p-value) | 0.002 ** | 0.423 | <0.001 ** | <0.001 ** | ||
| Pearson Correlation | PD-L1 positive in TIMC | 0.030 | 0.044 | 1 | 0.131 * | 0.106 |
| Significance (p-value) | 0.588 | 0.423 | 0.020 * | 0.063 | ||
| Pearson Correlation | CTLA-4 ≥ 2% in TIMC | 0.339 ** | 0.281 ** | 0.131 * | 1 | 0.789 ** |
| Significance (p-value) | <0.001 ** | <0.001 ** | 0.020 * | <0.001 ** | ||
| Pearson Correlation | PD-1 in TIMC positive and CTLA-4 in TIMC ≥ 2% | 0.845 ** | 0.273 ** | 0.106 | 0.789 ** | 1 |
| Significance (p-value) | <0.001 ** | <0.001 ** | 0.063 | <0.001 ** | ||
| All RCC | Estimated Mean OS (months) | Estimated Mean CSS (months) | ||||
|---|---|---|---|---|---|---|
| neg. | pos. | p-Value | neg. | pos. | p-Value | |
| PD-1 TIMC | 109.707 | 55.753 | 0.002 ** | 142.071 | 84.576 | 0.072 |
| PD-L1 TU | 108.923 | 86.661 | 0.694 | 140.353 | 105.148 | 0.964 |
| PD-L1 TIMC | 106.277 | 119.932 | 0.649 | No cancer specific death | ||
| CTLA-4 | 107.758 | 84.142 | 0.013 * | 140.590 | 125.534 | 0.019 * |
| PD-1 + CTLA-4 | 108.779 | 29.778 | 0.001 ** | 142.388 | 39.333 | 0.001 ** |
| CD3 | 103.920 | 112.413 | 0.628 | 142.116 | 138.045 | 0.390 |
| ccRCC | Estimated Mean OS (months) | Estimated Mean CSS (months) | ||||
|---|---|---|---|---|---|---|
| neg. | pos. | p-Value | neg. | pos. | p-Value | |
| PD-1 TIMC | 108.796 | 56.304 | 0.009 ** | 139.561 | 84.690 | 0.180 |
| PD-L1 TU | 108.894 | 86.841 | 0.691 | 138.745 | 102.306 | 0.883 |
| PD-L1 TIMC | 105.603 | 121.350 | 0.484 | No cancer specific death | ||
| CTLA-4 | 107.005 | 86.924 | 0.020 * | 138.789 | 113.542 | 0.004 ** |
| PD-1 + CTLA-4 | 107.778 | 24.857 | <0.001 ** | 139.737 | 34.000 | <0.001 ** |
| CD3 | 102.642 | 111.860 | 0.602 | 138.746 | 137.061 | 0.712 |
| No Primary Metastases | Estimated Mean OS (months) | Estimated Mean CSS (months) | ||||
|---|---|---|---|---|---|---|
| neg. | pos. | p-Value | neg. | pos. | p-Value | |
| PD-1 TIMC | 116.190 | 65.937 | 0.058 | 147.971 | 92.391 | 0.329 |
| PD-L1 TU | 115.848 | 92.812 | 0.737 | 146.010 | 110.674 | 0.738 |
| PD-L1 TIMC | 113.784 | 119.932 | 1.000 | No cancer specific death | ||
| CTLA-4 | 114.781 | 94.893 | 0.041 * | 146.821 | 125.273 | 0.001 ** |
| PD-1 + CTLA-4 | 116.216 | 32.000 | <0.001 ** | 148.705 | 32.000 | <0.001 ** |
| CD3 | 108.641 | 124.215 | 0.165 | 146.946 | 146.186 | 0.979 |
| All RCC | OS | CSS | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio | Range | p-Value | Hazard Ratio | Range | p-Value | |
| CTLA-4 | 2.838 | 1.248–6.451 | 0.013 * | 3.726 | 1.011–13.727 | 0.048 * |
| Age > 65 years | 2.501 | 1.436–4.356 | 0.001 ** | 1.818 | 0.736–4.487 | 0.195 |
| Gender male | 1.336 | 0.764–2.335 | 0.309 | 0.797 | 0.333–1.912 | 0.612 |
| Stage > pT2 | 3.450 | 2.119–5.617 | <0.001 ** | 2.520 | 1.096–5.791 | 0.030 * |
| Grade = G3 | 2.828 | 1.724–4.641 | <0.001 ** | 9.587 | 3.689–24.931 | <0.001 ** |
| ECOG > 0 | 1.576 | 0.952–2.608 | 0.077 | 0.477 | 2.701–1.135 | 0.775 |
| ccRCC | OS | CSS | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio | Range | p-Value | Hazard Ratio | Range | p-Value | |
| CTLA-4 | 4.059 | 1.506–10.940 | 0.006 ** | 8.161 | 2.003–33.26 | 0.003 * |
| Age > 65 years | 2.132 | 1.182–3.846 | 0.012 * | 2.162 | 0.843–5.546 | 0.109 |
| Gender male | 1.220 | 0.662–2.249 | 0.524 | 0.753 | 0.313–1.81 | 0.526 |
| Stage > pT2 | 3.026 | 1.786–5.301 | <0.001 ** | 1.568 | 0.623–3.944 | 0.339 |
| Grade = G3 | 3.132 | 1.796–5.462 | <0.001 ** | 11.341 | 4.108–30.676 | <0.001 ** |
| ECOG > 0 | 1.630 | 0.928–2.864 | 0.089 * | 1.545 | 0.612–3.899 | 0.357 |
| No Primary Metastases | OS | CSS | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio | Range | p-Value | Hazard Ratio | Range | p-Value | |
| CTLA-4 | 3.370 | 1.144–9.924 | 0.028 * | 7.351 | 1.337–40.42 | 0.022 * |
| Age > 65 years | 2.643 | 1.395–5.008 | 0.003 ** | 1.600 | 0.437–5.861 | 0.478 |
| Gender male | 1.794 | 0.906–3.554 | 0.094 | 0.983 | 0.236–4.104 | 0.981 |
| Stage > pT2 | 4.115 | 2.247–7.537 | <0.001 ** | 2.457 | 0.681–8.868 | 0.170 |
| Grade = G3 | 1.605 | 0.854–3.015 | 0.142 | 6.272 | 1.71–23.01 | 0.006 ** |
| ECOG > 0 | 2.071 | 1.135–3.784 | 0.018 * | 1.261 | 0.34–4.673 | 0.729 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kahlmeyer, A.; Stöhr, C.G.; Hartmann, A.; Goebell, P.J.; Wullich, B.; Wach, S.; Taubert, H.; Erlmeier, F. Expression of PD-1 and CTLA-4 Are Negative Prognostic Markers in Renal Cell Carcinoma. J. Clin. Med. 2019, 8, 743. https://doi.org/10.3390/jcm8050743
Kahlmeyer A, Stöhr CG, Hartmann A, Goebell PJ, Wullich B, Wach S, Taubert H, Erlmeier F. Expression of PD-1 and CTLA-4 Are Negative Prognostic Markers in Renal Cell Carcinoma. Journal of Clinical Medicine. 2019; 8(5):743. https://doi.org/10.3390/jcm8050743
Chicago/Turabian StyleKahlmeyer, Andreas, Christine G. Stöhr, Arndt Hartmann, Peter J. Goebell, Bernd Wullich, Sven Wach, Helge Taubert, and Franziska Erlmeier. 2019. "Expression of PD-1 and CTLA-4 Are Negative Prognostic Markers in Renal Cell Carcinoma" Journal of Clinical Medicine 8, no. 5: 743. https://doi.org/10.3390/jcm8050743