Identifying Knowledge Gaps among LVAD Candidates

Abstract
:1. Introduction
2. Methods
2.1. Knowledge Scale Development
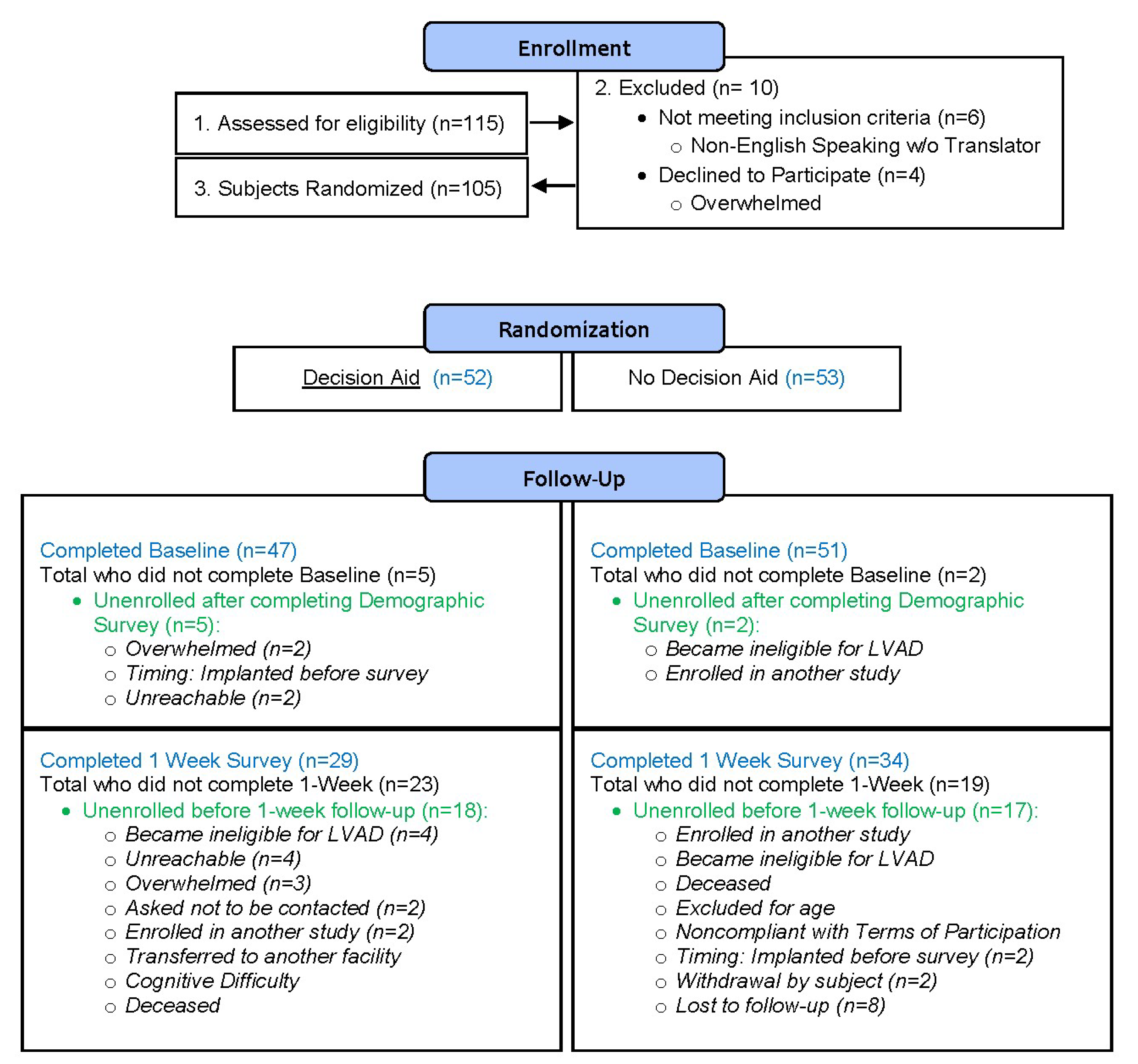
2.2. KS Administration
2.3. Analysis
3. Results
3.1. Candidate Knowledge
3.2. Changes in Knowledge
3.2.1. Candidates Educated with Decision Aid
3.2.2. Candidates Educated with Standard Education
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dew, M.A.; DiMartini, A.F.; Dobbels, F.; Grady, K.L.; Jowsey-Gregoire, S.G.; Kaan, A.; Kendall, K.; Young, Q.-R.; Abbey, S.E.; Butt, Z. The 2018 ISHLT/APM/AST/ICCAC/STSW recommendations for the psychosocial evaluation of adult cardiothoracic transplant candidates and candidates for long-term mechanical circulatory support. J. Heart Lung Transplant. 2018, 37, 803–823. [Google Scholar] [CrossRef]
- Barry, M.J.; Edgman-Levitan, S. Shared decision making—The pinnacle of patient-centered care. N. Engl. J. Med. 2012, 366, 780–781. [Google Scholar] [CrossRef] [PubMed]
- Stacey, D.; Légaré, F.; Lewis, K.; Barry, M.J.; Bennett, C.L.; Eden, K.B.; Holmes-Rovner, M.; Llewellyn-Thomas, H.; Lyddiatt, A.; Thomson, R. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst. Rev. 2017, 4, CD001431. [Google Scholar] [CrossRef]
- Knops, A.M.; Legemate, D.A.; Goossens, A.; Bossuyt, P.M.; Ubbink, D.T. Decision aids for patients facing a surgical treatment decision: A systematic review and meta-analysis. Ann. Surg. 2013, 257, 860–866. [Google Scholar] [CrossRef] [PubMed]
- Fedson, S.E.; MacKenzie, K.K.; Delgado, E.D.; Abraham, M.N.; Estep, J.D.; Blumenthal-Barby, J.S.; Bruce, C.R. Mapping the informed consent process for left ventricular assist devices. ASAIO J. 2018, 64, 630–635. [Google Scholar] [CrossRef]
- Iacovetto, M.C.; Matlock, D.D.; McIlvennan, C.K.; Thompson, J.S.; Bradley, W.; LaRue, S.J.; Allen, L.A. Educational resources for patients considering a left ventricular assist device: A cross-sectional review of internet, print, and multimedia materials. Circ. Cardiovasc. Qual. Outcomes 2014, 7, 905–911. [Google Scholar] [CrossRef] [PubMed]
- Widmar, S.B.; Dietrich, M.S.; Minnick, A.F. How self-care education in ventricular assist device programs is organized and provided: A national study. Heart Lung J. Acute Crit. Care 2014, 43, 25–31. [Google Scholar] [CrossRef]
- Kostick, K.M.; Minard, C.G.; Wilhelms, L.A.; Delgado, E.; Abraham, M.; Bruce, C.R.; Estep, J.D.; Loebe, M.; Volk, R.J.; Blumenthal-Barby, J.S. Development and validation of a patient-centered knowledge scale for left ventricular assist device placement. J. Heart Lung Transplant. 2016, 35, 768–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edlund, J.E.; Edlund, A.E.; Carey, M.G. Patient understanding of potential risk and benefit with informed consent in a left ventricular assist device population: A pilot study. J. Cardiovasc. Nurs. 2015, 30, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.S.; Matlock, D.D.; McIlvennan, C.K.; Jenkins, A.R.; Allen, L.A. Development of a decision aid for patients with advanced heart failure considering a destination therapy left ventricular assist device. JACC Heart Fail. 2015, 3, 965–976. [Google Scholar] [CrossRef]
- Kirkpatrick, J.; Hull, S.; Kellom, K.; Henderson, R.; Barg, F. Pumped up, but Not Prepared: Examining LVAD-DT Patients’ Comprehension of Advance Directive Specifications. J. Card. Fail. 2012, 18, S37. [Google Scholar] [CrossRef]
- Stiles, S. Doctor-Patient Device Communication Falls Short. Available online: http://www.medscape.com/viewarticle/771171 (accessed on 12 March 2019).
- Kostick, K.M.; Bruce, C.R.; Minard, C.G.; Volk, R.J.; Civitello, A.; Krim, S.R.; Horstmanshof, D.; Thohan, V.; Loebe, M.; Hanna, M. A Multisite Randomized Controlled Trial of a Patient-Centered Ventricular Assist Device Decision Aid (VADDA Trial). J. Card. Fail. 2018, 24, 661–671. [Google Scholar] [CrossRef] [PubMed]
- Allen, L.A.; McIlvennan, C.K.; Thompson, J.S.; Dunlay, S.M.; LaRue, S.J.; Lewis, E.F.; Patel, C.B.; Blue, L.; Fairclough, D.L.; Leister, E.C. Effectiveness of an intervention supporting shared decision making for destination therapy left ventricular assist device: The DECIDE-LVAD randomized clinical trial. JAMA Intern. Med. 2018, 178, 520–529. [Google Scholar] [CrossRef]
- McIlvennan, C.K.; Matlock, D.D.; Narayan, M.P.; Nowels, C.; Thompson, J.S.; Cannon, A.; Bradley, W.J.; Allen, L.A. Perspectives from mechanical circulatory support coordinators on the pre-implantation decision process for destination therapy left ventricular assist devices. Heart Lung 2015, 44, 219–224. [Google Scholar] [CrossRef]
- Lloyd, A.; Hayes, P.; Bell, P.R.; Naylor, A.R. The role of risk and benefit perception in informed consent for surgery. Med. Decis. Mak. 2001, 21, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Mulsow, J.J.; Feeley, T.M.; Tierney, S. Beyond consent—improving understanding in surgical patients. Am. J. Surg. 2012, 203, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Mishra, P.K.; Ozalp, F.; Gardner, R.S.; Arangannal, A.; Murday, A. Informed consent in cardiac surgery: Is it truly informed? J. Cardiovasc. Med. 2006, 7, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.; Williams, C. Informed consent: Patients listen and read, but what information do they retain? N. Z. Med. J. Online 2002, 115. [Google Scholar]
- Falagas, M.E.; Korbila, I.P.; Giannopoulou, K.P.; Kondilis, B.K.; Peppas, G. Informed consent: How much and what do patients understand? Am. J. Surg. 2009, 198, 420–435. [Google Scholar] [CrossRef]
- Holmboe, E.S.; Fiellin, D.A.; Cusanelli, E.; Remetz, M.; Krumholz, H.M. Perceptions of benefit and risk of patients undergoing first-time elective percutaneous coronary revascularization. J. Gen. Intern. Med. 2000, 15, 632–637. [Google Scholar] [CrossRef]
- Liberman, A.; Chaiken, S. Defensive processing of personally relevant health messages. Pers. Soc. Psychol. Bull. 1992, 18, 669–679. [Google Scholar] [CrossRef]
- Brown, S.; Locker, E. Defensive responses to an emotive anti-alcohol message. Psychol. Health 2009, 24, 517–528. [Google Scholar] [CrossRef]
- Kessels, L.T.; Ruiter, R.A.; Jansma, B.M. Increased attention but more efficient disengagement: Neuroscientific evidence for defensive processing of threatening health information. Health Psychol. 2010, 29, 346. [Google Scholar] [CrossRef]
- Blumenthal-Barby, J.S.; Kostick, K.M.; Delgado, E.D.; Volk, R.J.; Kaplan, H.M.; Wilhelms, L.A.; McCurdy, S.A.; Estep, J.D.; Loebe, M.; Bruce, C.R. Assessment of patients’ and caregivers’ informational and decisional needs for left ventricular assist device placement: Implications for informed consent and shared decision-making. J. Heart Lung Transplant. 2015, 34, 1182–1189. [Google Scholar] [CrossRef] [Green Version]
- Tversky, A.; Kahneman, D. Availability: A heuristic for judging frequency and probability. Cognit. Psychol. 1973, 5, 207–232. [Google Scholar] [CrossRef]
- Sepucha, K.R.; Borkhoff, C.M.; Lally, J.; Levin, C.A.; Matlock, D.D.; Ng, C.J.; Ropka, M.E.; Stacey, D.; Joseph-Williams, N.; Wills, C.E. Establishing the effectiveness of patient decision aids: Key constructs and measurement instruments. BMC Med. Inform. Decis. Mak. 2013, 13, S12. [Google Scholar] [CrossRef]
- Agard, A.; Hermerén, G.; Herlitz, J. When is a patient with heart failure adequately informed? A study of patients’ knowledge of and attitudes toward medical information. Heart Lung J. Acute Crit. Care 2004, 33, 219–226. [Google Scholar] [CrossRef]
- Adams, E.E.; Wrightson, M.L. Quality of life with an LVAD: A misunderstood concept. Heart Lung 2018, 47, 177–183. [Google Scholar] [CrossRef]
- Emin, A.; Rogers, C.A.; Banner, N.R.; Steering Group, U.C.T.A.; Hedger, M.; Hards, R.; Lincoln, P.; Wrightson, N.; Clarkson, J.; Robinson, N. Quality of life of advanced chronic heart failure: Medical care, mechanical circulatory support and transplantation. Eur. J. Cardiothorac. Surg. 2016, 50, 269–273. [Google Scholar] [CrossRef]
- Kitko, L.A.; Hupcey, J.E.; Birriel, B.; Alonso, W. Patients’ decision making process and expectations of a left ventricular assist device pre and post implantation. Heart Lung 2016, 45, 95–99. [Google Scholar] [CrossRef]
- Modica, M.; Ferratini, M.; Torri, A.; Oliva, F.; Martinelli, L.; De Maria, R.; Frigerio, M. Quality of Life and Emotional Distress Early After Left Ventricular Assist Device Implant: A Mixed-Method Study. Artif. Organs. 2015, 39, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Elwyn, G.; O’Connor, A.; Stacey, D.; Volk, R.; Edwards, A.; Coulter, A.; Thomson, R.; Barratt, A.; Barry, M.; Bernstein, S. Developing a quality criteria framework for patient decision aids: Online international Delphi consensus process. BMJ 2006, 333, 417. [Google Scholar] [CrossRef] [PubMed]
- Adams, R.J. Improving health outcomes with better patient understanding and education. Risk Manag. Healthc. Policy 2010, 3, 61. [Google Scholar] [CrossRef]
- Coulter, A.; Ellins, J. Effectiveness of strategies for informing, educating, and involving patients. BMJ 2007, 335, 24–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Question | % Correct at Baseline: Standard Education Group (n = 51) | % Correct at Baseline: Decision Aid Group (n = 47) | % Correct at 1-Week: Standard Education Group (n = 34) | % Correct at 1-Week: Decision Aid Group (n = 29) |
|---|---|---|---|---|
| 1. The LVAD is a device that… | 80% | 79% | 88% | 90% |
| 3. Which of the following is NOT a potential LVAD complication? | 61% | 64% | 74% | 93% |
| 4. When should you call the LVAD team for support? | 84% | 81% | 97% | 100% |
| 10. When you leave your house for a day trip, you should always have with you… | 39% | 40% | 56% | 93% |
| 15. In the first weeks after going home from surgery, LVAD patients need daily help from a caregiver. (T/F) | 88% | 83% | 100% | 100% |
| 18. Why do you have to take blood thinners (such as Coumadin) after you get an LVAD? | 78% | 74% | 97% | 97% |
| Question | % Correct at Baseline: Standard Education Group (n = 51) | % Correct at Baseline: Decision Aid Group (n = 47) | % Correct at 1-Week: Standard Education Group (n = 34) | % Correct at 1-Week: Decision Aid Group (n = 29) |
|---|---|---|---|---|
| 5. Which statement below most accurately reflects how likely it is that a patient will have to go back into the hospital within one year after getting an LVAD? | 20% | 17% | 32% | 55% |
| 8. What percentage of patients are still alive 2 years after receiving an LVAD? | 22% | 17% | 29% | 41% |
| 9. For most people, who covers expenses for additional LVAD maintenance supplies? | 25% | 30% | 41% | 48% |
| 14. After getting an LVAD, most people experience improvements in which of the following? | 33% | 45% | 56% | 48% |
| 17. How does an LVAD affect your future eligibility for a heart transplant, if at all? | 25% | 36% | 35% | 45% |
| 19. What will happen to you if the LVAD stops? | 18% | 19% | 24% | 34% |
| Increase in Correct Responses (Standard Education) | LVAD Knowledge Questionnaire | Increase in Correct Responses (Decision Aid Education) |
|---|---|---|
| 8% | 1. The LVAD is a device that… | 11% |
| 13% | 2. Factors that affect how fast you recover after LVAD surgery include… | 10% |
| 13% | 3. Which of the following is NOT a potential LVAD complication? | 30% * |
| 13% | 4. When should you call the LVAD team for support? | 19% * |
| 13% | 5. Which statement below most accurately reflects how likely it is that a patient will have to go back into the hospital within one year after getting an LVAD? | 38% ** |
| 10% | 6. How long should the average patient expect to stay in intensive care (ICU) after the operation? | 40% ** |
| 10% | 7. For the average patient, about how long is the total expected hospital stay (including intensive care and rehabilitation) after surgery? | 9% |
| 8% | 8. What percentage of patients are still alive 2 years after receiving an LVAD? | 24% * |
| 16% | 9. For most people, expenses for additional LVAD maintenance supplies (such as extra gauze, gloves and cleaning supplies, etc.) are covered by: | 18% |
| 17% | 10. When you leave your house for a day trip, you should always have with you… | 53% ** |
| 33% * | 11. Which one of the following activities will be true after you receive an LVAD? | 19% |
| 26% * | 12. When my LVAD battery power is getting low, the controller will alert me by: | 37% * |
| 3% † | 13. How likely is it that a patient with end-stage heart failure will be alive in one year, if he or she does not receive an LVAD? | −9% † |
| 23% * | 14. After getting an LVAD, most people experience improvements in which of the following? | 4% |
| 12% | 15. In the first weeks after going home from surgery, LVAD patients need daily help from a caregiver. (T/F) | 17% * |
| 38% ** | 16. How often will you need to clean your driveline? | 42% ** |
| 10% | 17. How does an LVAD affect your future eligibility for a heart transplant, if at all? | 9% |
| 19% * | 18. Why do you have to take blood thinners (such as Coumadin) after you get an LVAD? | 22% * |
| 6% | 19. What will happen to you if the LVAD stops? | 15% |
| 21% | 20. Which one of the following does NOT provide an advantage for how well patients do with an LVAD? | 36% ** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buchberg Trejo, M.; Kostick, K.M.; Estep, J.D.; Blumenthal-Barby, J.S. Identifying Knowledge Gaps among LVAD Candidates. J. Clin. Med. 2019, 8, 549. https://doi.org/10.3390/jcm8040549
Buchberg Trejo M, Kostick KM, Estep JD, Blumenthal-Barby JS. Identifying Knowledge Gaps among LVAD Candidates. Journal of Clinical Medicine. 2019; 8(4):549. https://doi.org/10.3390/jcm8040549
Chicago/Turabian StyleBuchberg Trejo, Meredith, Kristin M. Kostick, Jerry D. Estep, and J.S. Blumenthal-Barby. 2019. "Identifying Knowledge Gaps among LVAD Candidates" Journal of Clinical Medicine 8, no. 4: 549. https://doi.org/10.3390/jcm8040549