Short-Term Effects of Anodal Transcranial Direct Current Stimulation on Endurance and Maximal Force Production: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria and Study Selection
2.3. Coding
2.4. Assessment of Methodological Quality
2.5. Statistical Analysis
3. Results
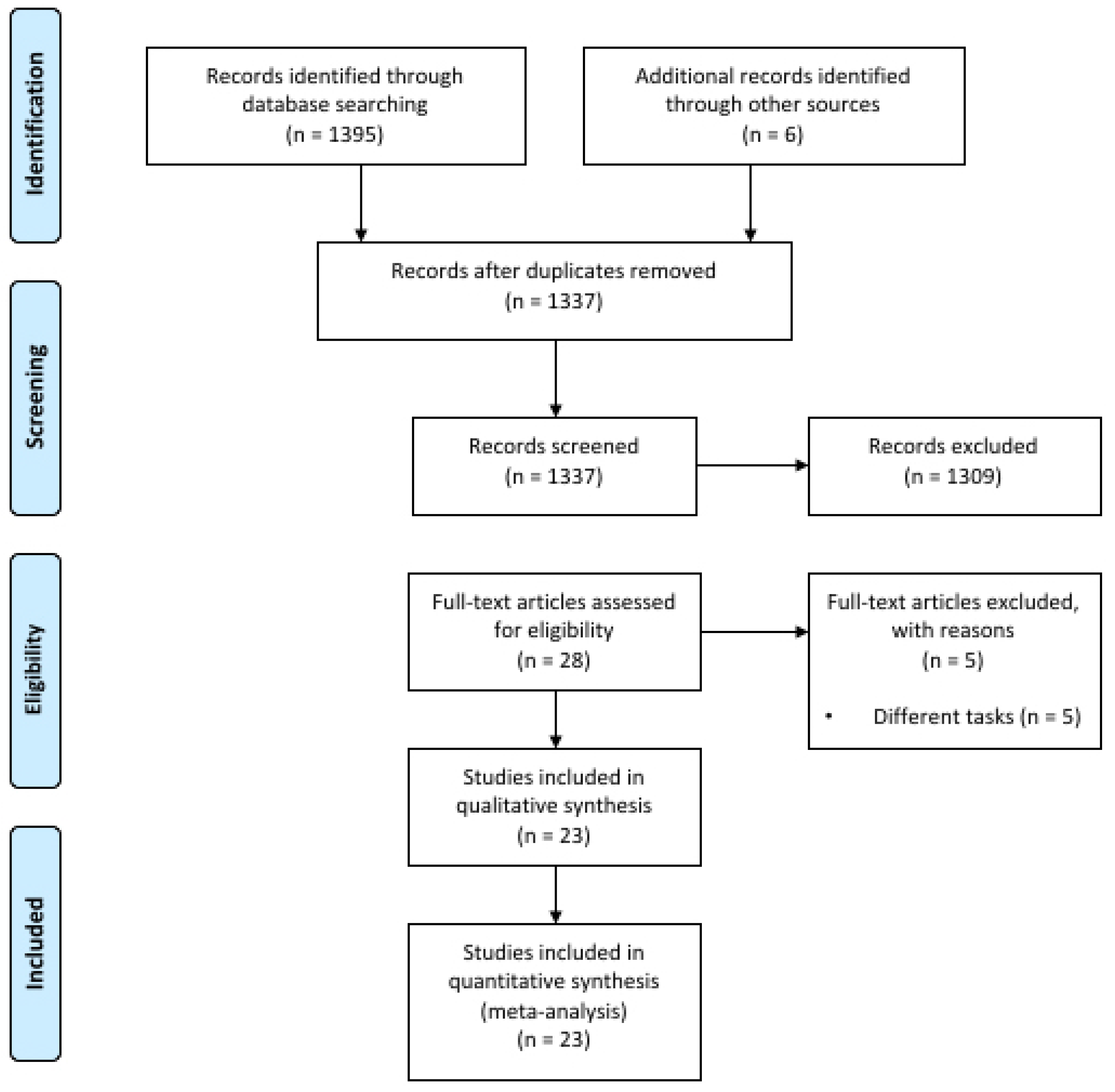
3.1. Study Selection and Characteristics
3.2. Study Quality Assessment and Publication Bias Evaluation
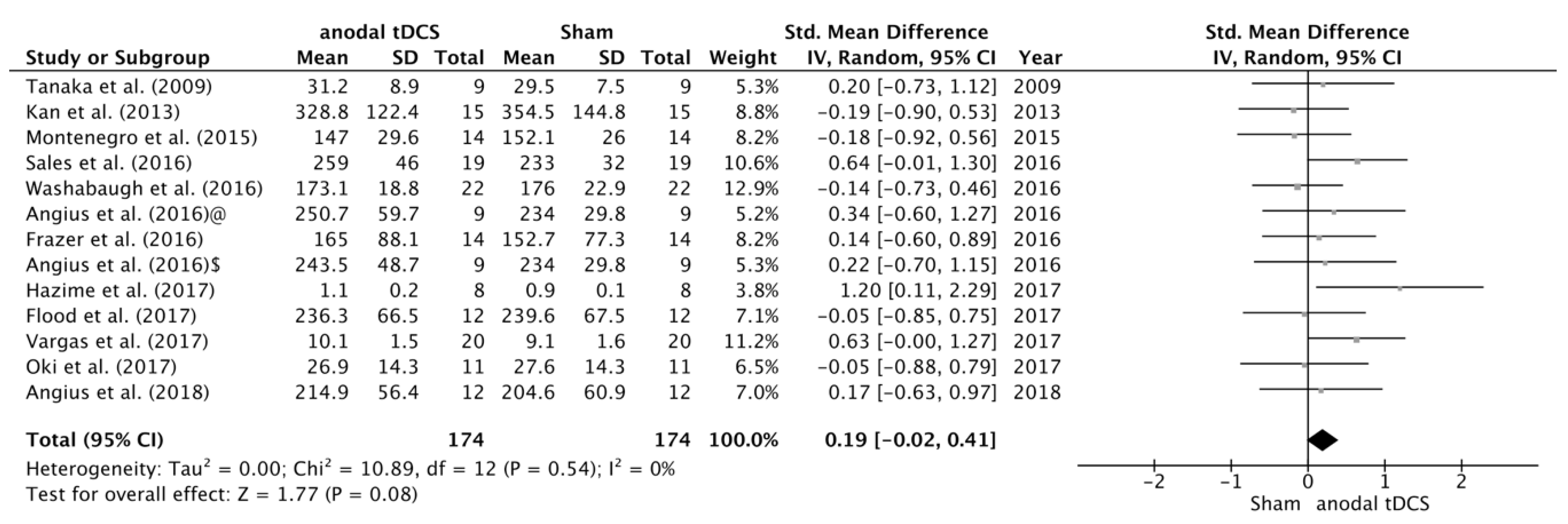
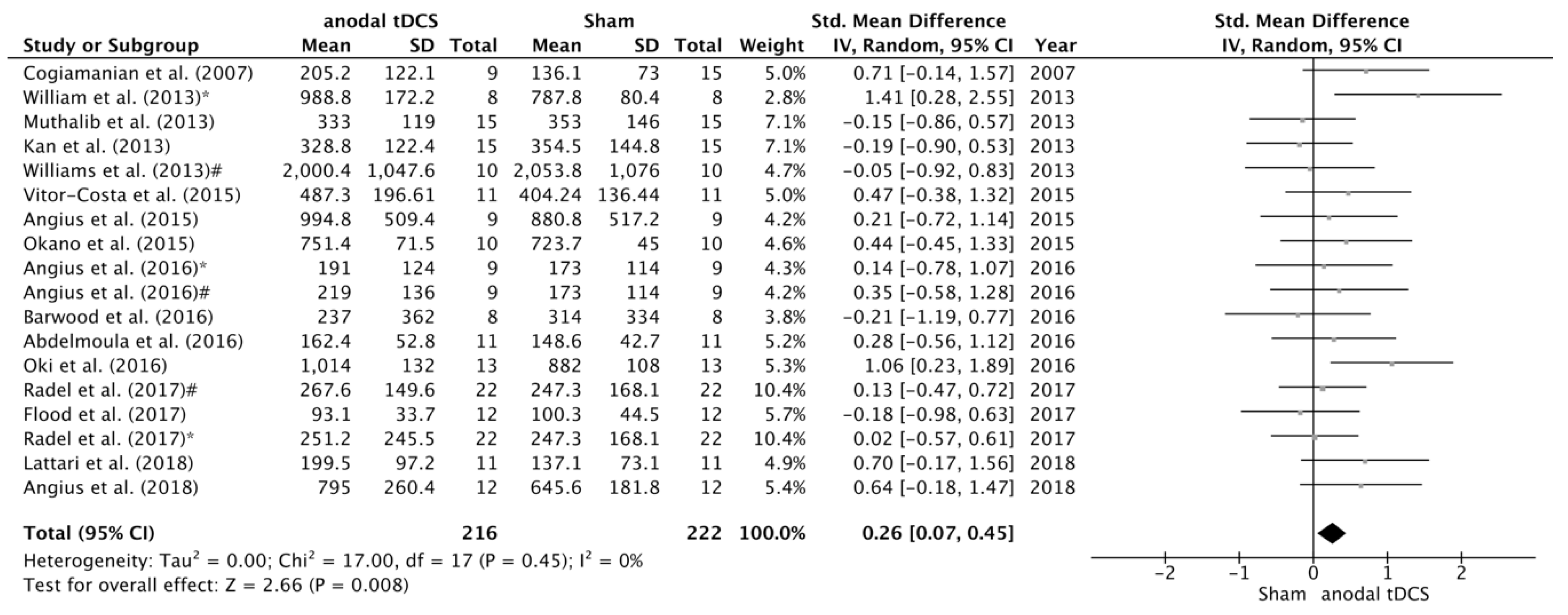
3.3. Effects of tDCS on TTF and MVC
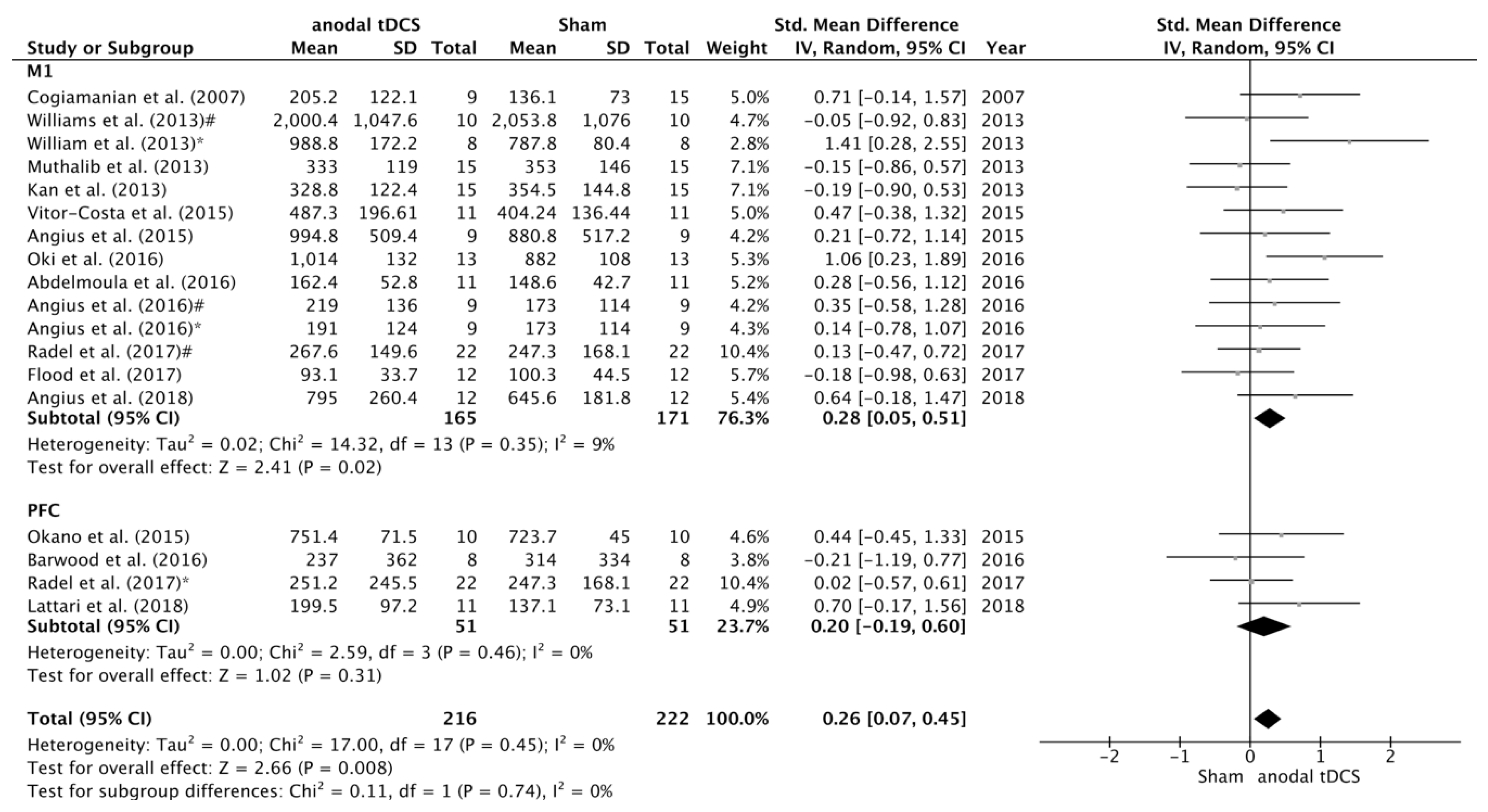
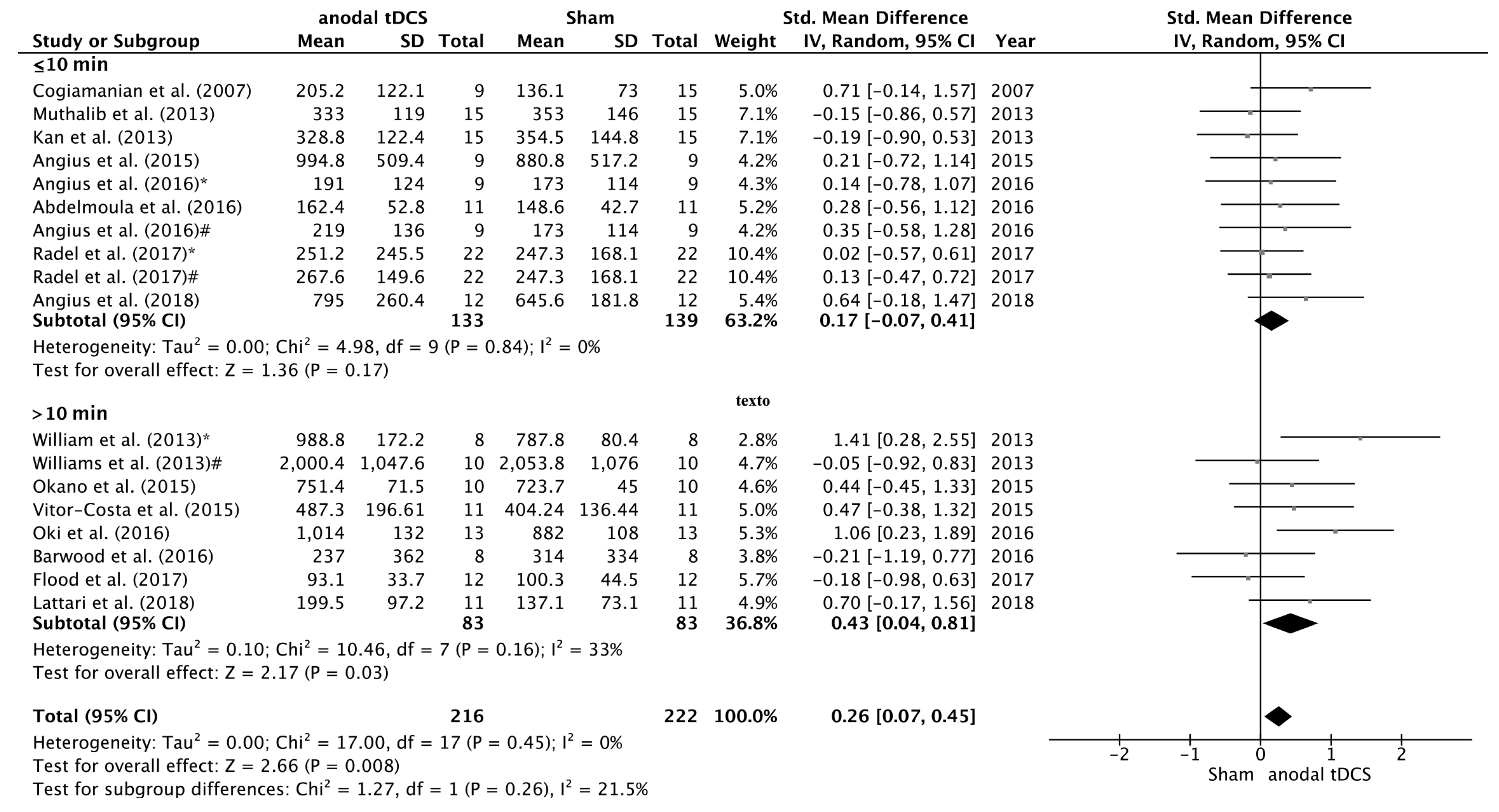
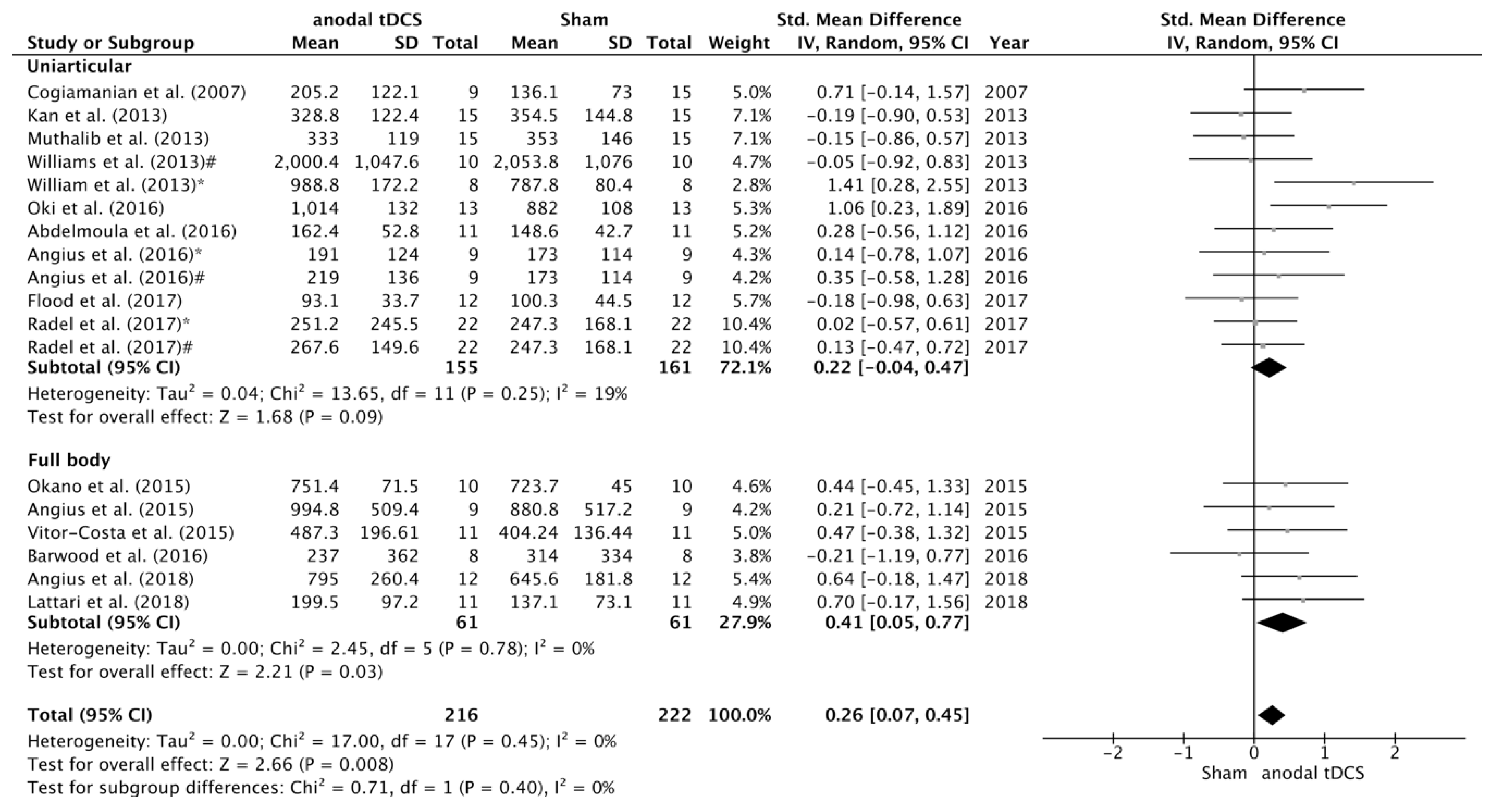
3.4. Subgroup Analyses of the Effects of tDCS
4. Discussion
4.1. tDCS Effects on Maximal Voluntary Contraction
4.2. The Effect of Anodal tDCS on Time to Task Failure
4.3. Stimulation Region
4.4. Duration of Stimulation
4.5. Whole-Body Exercise Versus Uniarticular-Based Exercise
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Stagg, C.J.; Nitsche, M.A. Physiological basis of transcranial direct current stimulation. Neuroscientist 2011, 17, 37–53. [Google Scholar] [CrossRef] [PubMed]
- Poreisz, C.; Boros, K.; Antal, A.; Paulus, W. Safety aspects of transcranial direct current stimulation concerning healthy subjects and patients. Brain Res. Bull. 2007, 72, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, M.A.; Paulus, W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J. Physiol. 2000, 527, 633–639. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Paulus, W. Sustained excitability elevations induced by transcranial DC motor cortex stimulation in humans. Neurology 2001, 57, 1899–1901. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, M.A.; Fricke, K.; Henschke, U.; Schlitterlau, A.; Liebetanz, D.; Lang, N.; Henning, S.; Tergau, F.; Paulus, W. Pharmacological modulation of cortical excitability shifts induced by transcranial direct current stimulation in humans. J. Physiol. 2003, 553, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Hartwigsen, G. Adaptive Plasticity in the Healthy Language Network: Implications for Language Recovery after Stroke. Neural Plast. 2016, 2016, 9674790. [Google Scholar]
- Schlaug, G.; Renga, V.; Nair, D. Transcranial direct current stimulation in stroke recovery. Arch. Neurol. 2008, 65, 1571–1576. [Google Scholar] [CrossRef] [PubMed]
- Brunelin, J.; Mondino, M.; Gassab, L.; Haesebaert, F.; Gaha, L.; Suaud-Chagny, M.F.; Saoud, M.; Mechri, A.; Poulet, E. Examining transcranial direct-current stimulation (tDCS) as a treatment for hallucinations in schizophrenia. Am. J. Psychiatry 2012, 169, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Fregni, F.; Boggio, P.S.; Nitsche, M.A.; Marcolin, M.A.; Rigonatti, S.P.; Pascual-Leone, A. Treatment of major depression with transcranial direct current stimulation. Bipolar Disord. 2006, 8, 203–204. [Google Scholar] [CrossRef] [PubMed]
- Coffman, B.A.; Clark, V.P.; Parasuraman, R. Battery powered thought: Enhancement of attention, learning, and memory in healthy adults using transcranial direct current stimulation. Neuroimage 2014, 85, 895–908. [Google Scholar] [CrossRef]
- Fregni, F.; Boggio, P.S.; Nitsche, M.; Bermpohl, F.; Antal, A.; Feredoes, E.; Marcolin, M.A.; Rigonatti, S.P.; Silva, M.T.A.; Paulus, W.; et al. Anodal transcranial direct current stimulation of prefrontal cortex enhances working memory. Exp. Brain Res. 2005, 166, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Hazime, F.A.; da Cunha, R.A.; Soliaman, R.R.; Romancini, A.C.B.; Pochini, A.D.C.; Ejnisman, B.; Baptista, A.F. Anodal transcranial direct current stimulation (tDCS) increases isometric strength of shoulder rotators muscles in handball players. Int. J. Sports Phys. Ther. 2017, 12, 402–407. [Google Scholar] [PubMed]
- Kan, B.; Dundas, J.E.; Nosaka, K. Effect of transcranial direct current stimulation on elbow flexor maximal voluntary isometric strength and endurance. Appl. Physiol. Nutr. Metab. 2013, 38, 734–739. [Google Scholar] [CrossRef]
- Tanaka, S.; Hanakawa, T.; Honda, M.; Watanabe, K. Enhancement of pinch force in the lower leg by anodal transcranial direct current stimulation. Exp. Brain Res. 2009, 196, 459–465. [Google Scholar] [CrossRef]
- Cogiamanian, F.; Marceglia, S.; Ardolino, G.; Barbieri, S.; Priori, A. Improved isometric force endurance after transcranial direct current stimulation over the human motor cortical areas. Eur. J. Neurosci. 2007, 26, 242–249. [Google Scholar] [CrossRef]
- Radel, R.; Tempest, G.; Denis, G.; Besson, P.; Zory, R. Extending the limits of force endurance: Stimulation of the motor or the frontal cortex? Cortex 2017, 97, 96–108. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.S.; Hoffman, R.L.; Clark, B.C. Preliminary evidence that anodal transcranial direct current stimulation enhances time to task failure of a sustained submaximal contraction. PLoS ONE 2013, 8, e81418. [Google Scholar] [CrossRef] [PubMed]
- Angius, L.; Hopker, J.; Mauger, A.R. The ergogenic effects of transcranial direct current stimulation on exercise performance. Front. Pysiol. 2017, 8, 90. [Google Scholar] [CrossRef] [PubMed]
- Okano, A.H.; Fontes, E.B.; Montenegro, R.A.; De Tarso Veras Farinatti, P.; Cyrino, E.S.; Li, L.M.; Bikson, M.; Noakes, T.D. Brain stimulation modulates the autonomic nervous system, rating of perceived exertion and performance during maximal exercise. Br. J. Sports Med. 2015, 49, 1213–1218. [Google Scholar] [CrossRef]
- Angius, L.; Mauger, A.R.R.; Hopker, J.; Pascual-Leone, A.; Santarnecchi, E.; Marcora, S.M.M. Bilateral extracephalic transcranial direct current stimulation improves endurance performance in healthy individuals. Brain Stimul. 2018, 11, 108–117. [Google Scholar] [CrossRef]
- Frazer, A.; Williams, J.; Spittles, M.; Rantalainen, T.; Kidgell, D. Anodal transcranial direct current stimulation of the motor cortex increases cortical voluntary activation and neural plasticity. Muscle Nerve 2016, 54, 903–913. [Google Scholar] [CrossRef]
- Vargas, V.Z.; Baptista, A.F.; Pereira, G.O.C.; Pochini, A.C.; Ejnisman, B.; Santos, M.B.; João, S.M.A.; Hazime, F.A. Modulation of Isometric Quadriceps Strength in Soccer Players With Transcranial Direct Current Stimulation: A Crossover Study. J. Strength Cond. Res. 2018, 32, 1336–1341. [Google Scholar] [CrossRef]
- Lattari, E.; Campos, C.; Lamego, M.K.; Passos de Souza, S.L.; Neto, G.M.; Rocha, N.B.; José de Oliveira, A.; Carpenter, S.; Machado, S. Can transcranial direct current stimulation improve muscle power in individuals with advanced resistance training experience? J. Strength Cond. Res. 2017, in press. [Google Scholar] [CrossRef] [PubMed]
- Flood, A.; Waddington, G.; Keegan, R.J.; Thompson, K.G.; Cathcart, S. The effects of elevated pain inhibition on endurance exercise performance. PeerJ 2017, 5, e3028. [Google Scholar] [CrossRef] [PubMed]
- Montenegro, R.; Okano, A.; Gurgel, J.; Porto, F.; Cunha, F.; Massaferri, R.; Farinatti, P. Motor cortex tDCS does not improve strength performance in healthy subjects. Mot. Rev. Educ. Física 2015, 21, 185–193. [Google Scholar] [CrossRef]
- Abdelmoula, A.; Baudry, S.; Duchateau, J. Anodal transcranial direct current stimulation enhances time to task failure of a submaximal contraction of elbow flexors without changing corticospinal excitability. Neuroscience 2016, 322, 94–103. [Google Scholar] [CrossRef] [PubMed]
- Angius, L.; Pageaux, B.; Hopker, J.; Marcora, S.M.; Mauger, A.R. Transcranial direct current stimulation improves isometric time to exhaustion of the knee extensors. Neuroscience 2016, 339, 363–375. [Google Scholar] [CrossRef] [PubMed]
- Lattari, E.; de Oliveira, B.S.; Oliveira, B.R.R.; de Mello Pedreiro, R.C.; Machado, S.; Neto, G.A.M. Effects of transcranial direct current stimulation on time limit and ratings of perceived exertion in physically active women. Neurosci. Lett. 2018, 662, 12–16. [Google Scholar] [CrossRef]
- Oki, K.; Mahato, N.K.; Nakazawa, M.; Amano, S.; France, C.R.; Russ, D.W.; Clark, B.C. Preliminary Evidence That Excitatory Transcranial Direct Current Stimulation Extends Time to Task Failure of a Sustained, Submaximal Muscular Contraction in Older Adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 71, 1109–1112. [Google Scholar] [CrossRef]
- Vitor-Costa, M.; Okuno, N.M.; Bortolotti, H.; Bertollo, M.; Boggio, P.S.; Fregni, F.; Altimari, L.R. Improving Cycling Performance: Transcranial Direct Current Stimulation Increases Time to Exhaustion in Cycling. PLoS ONE 2015, 10, e0144916. [Google Scholar] [CrossRef]
- Angius, L.; Hopker, J.G.; Marcora, S.M.; Mauger, A.R. The effect of transcranial direct current stimulation of the motor cortex on exercise-induced pain. Eur. J. Appl. Physiol. 2015, 115, 2311–2319. [Google Scholar] [CrossRef] [PubMed]
- Barwood, M.J.; Butterworth, J.; Goodall, S.; House, J.R.; Laws, R.; Nowicky, A.; Corbett, J. The Effects of Direct Current Stimulation on Exercise Performance, Pacing and Perception in Temperate and Hot Environments. Brain Stimul. 2016, 9, 842–849. [Google Scholar] [CrossRef] [PubMed]
- Muthalib, M.; Kan, B.; Nosaka, K.; Perrey, S. Effects of transcranial direct current stimulation of the motor cortex on prefrontal cortex activation during a neuromuscular fatigue task: An fNIRS study. Adv. Exp. Med. Biol. 2013, 78, 73–79. [Google Scholar]
- Gandevia, S.C. Spinal and supraspinal factors in human muscle fatigue. Physiol. Rev. 2001, 81, 1725–1789. [Google Scholar] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Altman, D.G.; Booth, A.; et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioural Science, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988; pp. 1–567. [Google Scholar]
- Washabaugh, E.P.; Santos, L.; Claflin, E.S.; Krishnan, C. Low-level intermittent quadriceps activity during transcranial direct current stimulation facilitates knee extensor force-generating capacity. Neuroscience 2016, 329, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Oki, K.; Clark, L.A.; Amano, S.; Clark, B.C. Effect of Anodal Transcranial Direct Current Stimulation of the Motor Cortex on Elbow Flexor Muscle Strength in the Very Old. J. Geriatr. Phys. Ther. 2017, in press. [Google Scholar] [CrossRef] [PubMed]
- Sales, M.M.; De Sousa, C.V.; Browne, R.A.V.; Fontes, E.B.; Olher, R.R.V.; Ernesto, C.; Simões, H.G. Transcranial direct current stimulation improves muscle isokinetic performance of young trained individuals. Med. Dello Sport 2016, 69, 163–172. [Google Scholar]
- Farina, D.; Negro, F. Common synaptic input to motor neurons, motor unit synchronization, and force control. Exerc. Sport Sci. Rev. 2015, 43, 23–33. [Google Scholar] [CrossRef]
- Dutta, A.; Krishnan, C.; Kantak, S.S.; Ranganathan, R.; Nitsche, M.A. Recurrence quantification analysis of surface electromyogram supports alterations in motor unit recruitment strategies by anodal transcranial direct current stimulation. Restor. Neurol. Neurosci. 2015, 33, 663–669. [Google Scholar] [CrossRef]
- Krishnan, C.; Ranganathan, R.; Kantak, S.S.; Dhaher, Y.Y.; Rymer, W.Z. Anodal transcranial direct current stimulation alters elbow flexor muscle recruitment strategies. Brain Stimul. 2014, 7, 443–450. [Google Scholar] [CrossRef]
- Taylor, J.L.; Amann, M.; Duchateau, J.; Meeusen, R.; Rice, C.L. Neural contributions to muscle fatigue: From the brain to the muscle and back again. Med. Sci. Sports Exerc. 2016, 48, 2294–2306. [Google Scholar] [CrossRef] [PubMed]
- Robertson, C.V.; Marino, F.E. A role for the prefrontal cortex in exercise tolerance and termination. J. Appl. Physiol. 2016, 120, 464–466. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.Z.; Shan, Z.Y.; Zhang, L.D.; Sahgal, V.; Brown, R.W.; Yue, G.H. Human Brain Activation During Sustained and Intermittent Submaximal Fatigue Muscle Contractions: An fMRI Study. J. Neurophysiol. 2003, 90, 300–312. [Google Scholar] [CrossRef] [PubMed]
- Rushworth, M.F.S. Anatomical and functional subdivision within the primate lateral prefrontal cortex. Psychobiology 2000, 28, 187–196. [Google Scholar]
- Bigland-Ritchie, B.; Rice, C.L.; Garland, S.J.; Walsh, M.L. Task-dependent factors in fatigue of human voluntary contractions. Adv. Exp. Med. Biol. 1995, 384, 361–380. [Google Scholar] [PubMed]
- Enoka, R.M.; Baudry, S.; Rudroff, T.; Farina, D.; Klass, M.; Duchateau, J. Unraveling the neurophysiology of muscle fatigue. J. Electromyogr. Kinesiol. 2011, 21, 208–219. [Google Scholar] [CrossRef] [PubMed]
- Iguchi, M.; Shields, R.K. Quadriceps low-frequency fatigue and muscle pain are contraction-type-dependent. Muscle Nerve 2010, 42, 230–238. [Google Scholar] [CrossRef]
- Amann, M.; Blain, G.M.; Proctor, L.T.; Sebranek, J.J.; Pegelow, D.F.; Dempsey, J.A. Group III and IV muscle afferents contribute to ventilatory and cardiovascular response to rhythmic exercise in humans. J. Appl. Physiol. 2010, 109, 966–976. [Google Scholar] [CrossRef] [PubMed]
- Amann, M.; Venturelli, M.; Ives, S.J.; McDaniel, J.; Layec, G.; Rossman, M.J.; Richardson, R.S. Peripheral fatigue limits endurance exercise via a sensory feedback-mediated reduction in spinal motoneuronal output. J. Appl. Physiol. 2013, 115, 355–364. [Google Scholar] [CrossRef]
- Rossman, M.J.; Garten, R.S.; Venturelli, M.; Amann, M.; Richardson, R.S. The role of active muscle mass in determining the magnitude of peripheral fatigue during dynamic exercise. AJP Regul. Integr. Comp. Physiol. 2014, 306, R934–R940. [Google Scholar] [CrossRef] [PubMed]
- López-Alonso, V.; Cheeran, B.; Río-Rodríguez, D.; Fernández-Del-Olmo, M. Inter-individual variability in response to non-invasive brain stimulation paradigms. Brain Stimul. 2014, 7, 372–380. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Sample | tDCS Intensity | Polarity | Stimulation Electrode | Reference Electrode | Duration (Minutes) | Task | Main Outcome (MVC in N, N·m, N/kg) |
|---|---|---|---|---|---|---|---|---|
| Tanaka et al. [14] | 10 (8 M, 2 F); 27.5 ± 7.5 years | tDCS 2 mA | A/S | M1 | Orbital | 10 | MVC of lower leg pinch force | A: 31.2 ± 8.9 S: 29.5 ± 7.5 |
| Kan et al. [13] | 15 (15 M) 27.7 ± 8.4 years | tDCS 2 mA | A/S | M1 | Shoulder | 10 | MVC of elbow flexors | S: 62.2 ± 11.1 A: 62.0 ± 11.2 |
| Montenegro et al. [25] | 14 (14 M) 26 ± 4 years | tDCS 2 mA | A/S | M1 | Supraorbital | 20 | MVC of knee extensors | A: 147 ± 29.6 S: 152.1 ± 26 |
| Sales et al. [39] | 19 (19 M) 25.2 ± 4 years | tDCS 2 mA | A/S | Temporal lobe | Supraorbital | 20 | MVC of knee extensors | A: 259 ± 46 S: 233 ± 32 |
| Washabaugh et al. [37] | 22 (15 M, 7 F) 22.8 ± 5.7 years | tDCS 2 mA | A/S | M1 | Supraorbital | 12 | MVC of knee extensors | A: 173.1 ± 18.8 S: 176.0 ± 22.9 |
| Angius et al. [27] | 9 (9 M) 23 ± 2 years | tDCS 2 mA | A-C/A-E/S | M1 | A-E: Shoulder A-C: Right DLPFC | 10 | MVC of knee extensors | A-E: 250.7 ± 59.7 A-C: 243.5 ± 48.7 S: 234.0 ± 29.8 |
| Frazer et al. [21] | 14 (6 M, 8 F) 18–35 years | tDCS 2mA | A/S | M1 | Supraorbital | 20 | MVC of wrist extensors | A: 165 ± 88.1 S: 152.7 ± 77.3 |
| Hazime et al. [12] | 8 (8 F) 19.7 ± 2.6 years | tDCS 2 mA | A/S | M1 | Supraorbital | 20 | MVC of external shoulder rotators | A: 1.1 ± 0.2 S: 0.9 ± 0.1 |
| Flood et al. [24] | 12 (12 M) 24.4 ± 3.9 years | tDCS 2 mA | A/S | M1 | 4 cathodes around the anode | 20 | MVC of knee extensors | A: 236.3 ± 66.5 S: 239.6 ± 67.5 |
| Vargas et al. [22] | 20 (20 F) 16.1 ± 0.9 years | tDCS 2 mA | A/S | M1 | Supraorbital | 20 | MVC of knee extensors | A: 10.1 ± 1.5 S: 9.1 ± 1.6 |
| Oki et al. [38] | 11 (4 M, 7 W) 85.8 ± 4.3 years | tDCS 1.5 mA | A/S | M1 | Supraorbital | 20 | MVC of elbow flexors | A: 26.9 ± 14.3 S: 27.6 ± 14.3 |
| Angius et al. [20] | 12 (8 M, 4 F) 24 ± 5 years | tDCS 2 mA | A/S | M1 | Shoulders | 10 | MVC of knee extensors | A: 214.9 ± 56.4 S: 204.6 ± 60.9 |
| Study | Sample | NIBS | Polarity | Stimulation Electrode | Reference Electrode | Duration (Minutes) | Task | Main Outcome (Seconds) |
|---|---|---|---|---|---|---|---|---|
| Cogiamanian et al. [15] | 24 (10 M, 14 F) 24.3 years | tDCS 1.5 mA | A/S | M1 | Shoulder | 10 | TTF at 35% of MVC of elbow flexors | A: 205.2 ± 24.9 S: 136.1 ± 14.9 |
| Williams et al. [17] | 18 (9 M, 9 F) 25 ± 6 years | tDCS 1.5 mA | A/S | M1 | Orbitofrontal cortex | 20 | TTF at 20% MVC of elbow flexors | Full-time stimulation group: A: 988.8 ± 172.2 S: 787.8 ± 80.4 Part-time stimulation group: A: 2000.4 ± 1047.6 S: 2053.8 ± 1076.0 |
| Muthalib et al. [33] | 15 (15 M) 27.7 ± 8.4 years | tDCS 2 mA | A/S | M1 | Shoulder | 10 | TTF at 30% of MVC of elbows flexors | A: 333 ± 119 S: 353 ± 146 |
| Kan et al. [13] | 15 (15 M) 27.7 ± 8.4 years | tDCS 2 mA | A/S | M1 | Shoulder | 10 | TTF at 30% of MVC of elbow flexors | S: 354.5 ± 144.8 A1: 328.8 ± 122.4 |
| Vitor-Costa et al. [30] | 11 (11 M) 26 ± 4 years | tDCS 2 mA | A/S | M1 | Occipital protuberance (inion) | 13 | TTE cycling at 80% of Pmax | A: 487.3 ± 196.6 S: 404.2 ± 136.4 |
| Angius et al. [31] | 9 (9 M) 23 ± 4 years | tDCS 2 mA | A/S/C | M1 | DLPFC | 10 | TTE cycling at 70% of Pmax | A: 994.8 ± 509,4 S: 880.8 ± 517.2 |
| Okano et al. [19] | 10 (10 M) 33 ± 9 years | tDCS 2 mA | A/S | Left Temporal Cortex | Supraorbital | 20 | Maximal incremental cycling test | A: 751.4 ± 71.5 S: 723.7 ± 45.0 |
| Angius et al. [27] | 9 (9 M) 23 ± 2 years | tDCS 2 mA | A-C/A-E/S | M1 | A-E: Shoulder A-C: right DLPFC | 10 | TTF at 20% of MVC of knee extensors | A-E: 219 ± 136 A-C: 191 ± 124 S: 173 ± 114 |
| Barwood et al. [32] | 8 (8 M) 21 ± 1 years | tDCS 2 mA | A/S | PFC | Supraorbital | 20 | TTE cycling at 70% of Pmax | A: 237 ± 362 S: 314 ± 334 |
| Abdelmoula et al. [26] | 11 (8 M, 3 F) 25 ± 1.8 years | tDCS 1.5 mA | A/S | M1 | Shoulder | 10 | TTF at 35% of MVC of elbow flexors | A: 162.4 ± 52.8 S: 148.6 ± 42.7 |
| Oki et al. [29] | 13 (5 M, 8 F) 68.3 ± 2 years | tDCS 1.5 mA | A/S | M1 | Orbitofrontal cortex | 20 | TTF at 30% of MVC of elbow flexors | A: 1014 ± 132 S: 882 ± 108 |
| Radel et al. [16] | 22 (13 M, 9 F) 21.36 ± 0.43 years | tDCS 2 mA | A/S | PFC and M1 | 4 cathodes around anode | 10 | TTF at 35% of MVC of elbow flexors | A-PFC: 251.2 ± 245.5 A-M1: 267.6 ± 149.6 S: 247.3 ± 168.1 |
| Flood et al. [24] | 12 (12 M) 24.42 ± 3.85 years | tDCS 2 mA | A/S | M1 | 4 cathodes around anode | 20 | TTF at 30% of MVC of non dominant knee extensors | A: 93.1 ± 33.7 S: 100.3 ± 44.3 |
| Lattari et al. [28] | 11 (11 F) 24.0 ± 2.2 years | tDCS 2 mA | A/S | DLPFC | Orbitofrontal cortex | 20 | TTE cycling at 100% of Pmax | A: 199.5 ± 97.2 S: 137.1 ± 73.1 |
| Angius et al. [20] | 12 (8 M, 4 F) 24 ± 5 years | tDCS 2 mA | A/S | M1 | Shoulders | 10 | TTE cycling at 70% of Pmax | A: 795 ± 260.4 S: 645.6 ± 181.8 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alix-Fages, C.; Romero-Arenas, S.; Castro-Alonso, M.; Colomer-Poveda, D.; Río-Rodriguez, D.; Jerez-Martínez, A.; Fernandez-del-Olmo, M.; Márquez, G. Short-Term Effects of Anodal Transcranial Direct Current Stimulation on Endurance and Maximal Force Production: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 536. https://doi.org/10.3390/jcm8040536
Alix-Fages C, Romero-Arenas S, Castro-Alonso M, Colomer-Poveda D, Río-Rodriguez D, Jerez-Martínez A, Fernandez-del-Olmo M, Márquez G. Short-Term Effects of Anodal Transcranial Direct Current Stimulation on Endurance and Maximal Force Production: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2019; 8(4):536. https://doi.org/10.3390/jcm8040536
Chicago/Turabian StyleAlix-Fages, Carlos, Salvador Romero-Arenas, Marcos Castro-Alonso, David Colomer-Poveda, Dan Río-Rodriguez, Agustín Jerez-Martínez, Miguel Fernandez-del-Olmo, and Gonzalo Márquez. 2019. "Short-Term Effects of Anodal Transcranial Direct Current Stimulation on Endurance and Maximal Force Production: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 8, no. 4: 536. https://doi.org/10.3390/jcm8040536