Preoperative Clinical and Computed Tomography (CT)-Based Nomogram to Predict Oncologic Outcomes in Patients with Pancreatic Head Cancer Resected with Curative Intent: A Retrospective Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Clinical Information
2.2. CT Imaging
2.3. Image Analysis
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Correlation between Preoperative Clinically Detectable Parameters and Long-Term Oncologic Outcomes Following Pancreatectomy
3.3. Subgroup Analysis of the 82 Patients with Resectable Pancreatic Cancer
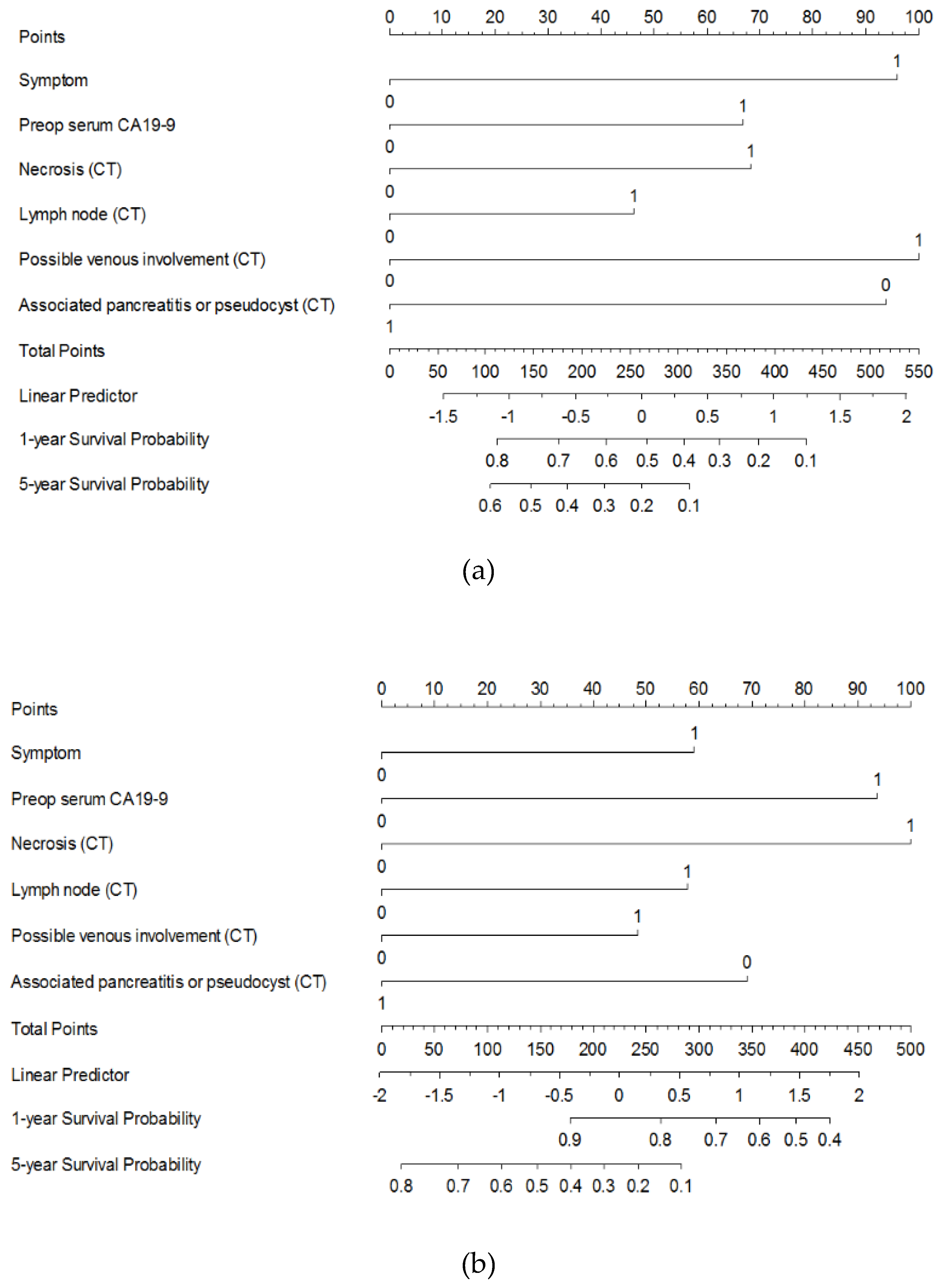
3.4. Developing a Preoperative Clinical and Imaging-Based Nomogram to Predict DFS and OS
3.5. Calibration and Internal Validation
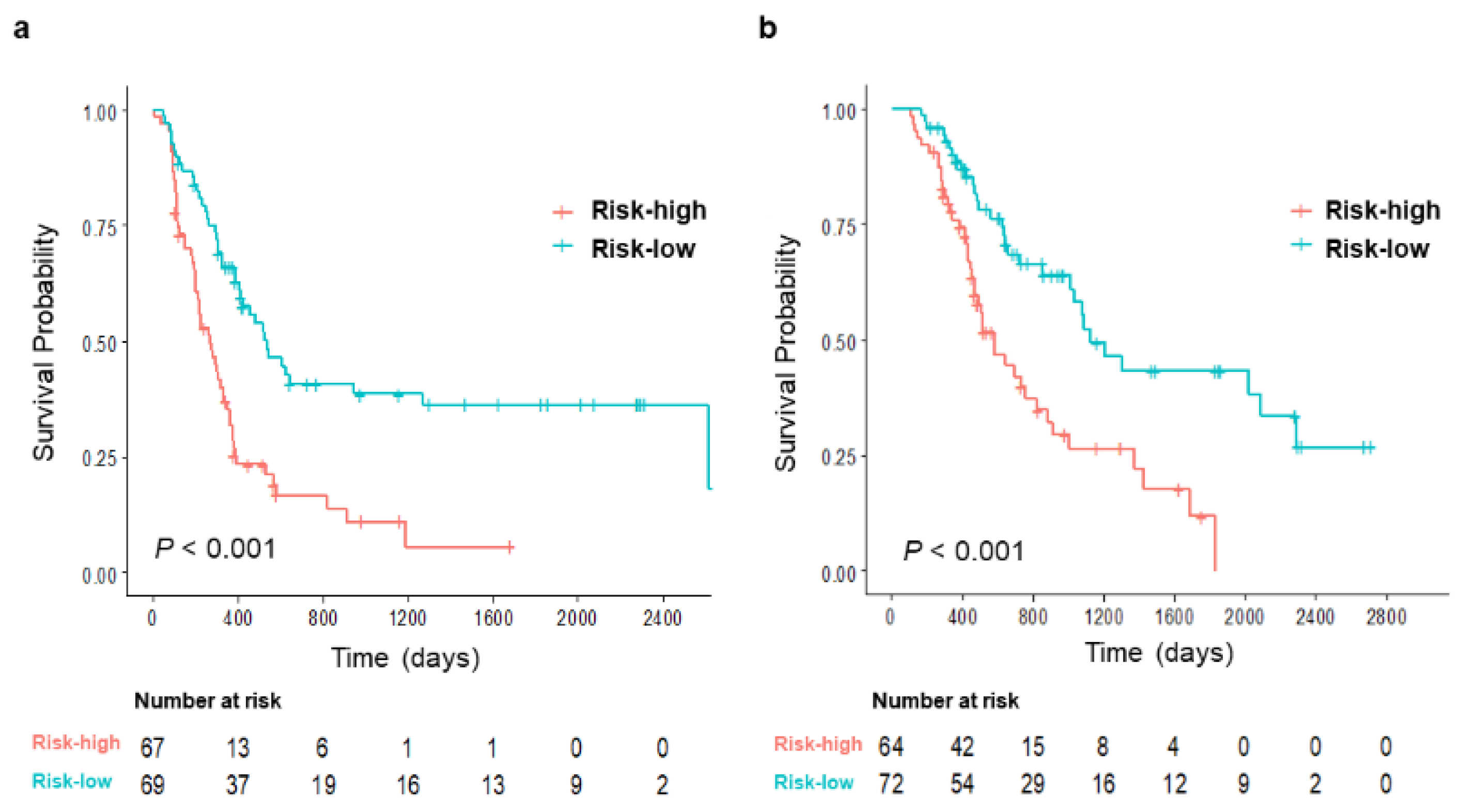
3.6. Risk Stratification According to the Proposed Nomogram to Predict Oncologic Outcomes in Resected Pancreatic Cancer Without Neoadjuvant Treatment
3.7. Developing a Preoperative Clinical and Imaging-Based Nomogram for Patients Resectable Pancreatic Cancer
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Malvezzi, M.; Bertuccio, P.; Levi, F.; La Vecchia, C.; Negri, E. European cancer mortality predictions for the year 2013. Ann. Oncol. 2013, 24, 792–800. [Google Scholar] [CrossRef]
- Tamburrino, D.; Partelli, S.; Crippa, S.; Manzoni, A.; Maurizi, A.; Falconi, M. Selection criteria in resectable pancreatic cancer: A biological and morphological approach. World J. Gastroenterol. 2014, 20, 11210–11215. [Google Scholar] [CrossRef] [PubMed]
- Callery, M.P.; Chang, K.J.; Fishman, E.K.; Talamonti, M.S.; William Traverso, L.; Linehan, D.C. Pretreatment assessment of resectable and borderline resectable pancreatic cancer: Expert consensus statement. Ann. Surg. Oncol. 2009, 16, 1727–1733. [Google Scholar] [CrossRef] [PubMed]
- Varadhachary, G.R.; Tamm, E.P.; Abbruzzese, J.L.; Xiong, H.Q.; Crane, C.H.; Wang, H.; Lee, J.E.; Pisters, P.W.; Evans, D.B.; Wolff, R.A. Borderline resectable pancreatic cancer: Definitions, management, and role of preoperative therapy. Ann. Surg. Oncol. 2006, 13, 1035–1046. [Google Scholar] [CrossRef] [PubMed]
- Hackert, T.; Ulrich, A.; Buchler, M.W. Borderline resectable pancreatic cancer. Cancer Lett. 2016, 375, 231–237. [Google Scholar] [CrossRef]
- Sohn, T.A.; Yeo, C.J.; Cameron, J.L.; Koniaris, L.; Kaushal, S.; Abrams, R.A.; Sauter, P.K.; Coleman, J.; Hruban, R.H.; Lillemoe, K.D. Resected adenocarcinoma of the pancreas-616 patients: Results, outcomes, and prognostic indicators. J. Gastrointest. Surg. 2000, 4, 567–579. [Google Scholar] [CrossRef]
- Oettle, H.; Neuhaus, P.; Hochhaus, A.; Hartmann, J.T.; Gellert, K.; Ridwelski, K.; Niedergethmann, M.; Zulke, C.; Fahlke, J.; Arning, M.B.; et al. Adjuvant chemotherapy with gemcitabine and long-term outcomes among patients with resected pancreatic cancer: The conko-001 randomized trial. JAMA 2013, 310, 1473–1481. [Google Scholar] [CrossRef]
- Okabayashi, T.; Shima, Y.; Sumiyoshi, T.; Sui, K.; Iwata, J.; Morita, S.; Shimada, Y.; Iiyama, T. A novel physiobiological parameter-based grading system for resectable pancreatic cancer. Ann. Surg. Oncol. 2018, 25, 1889–1895. [Google Scholar] [CrossRef]
- Dumont, R.; Puleo, F.; Collignon, J.; Meurisse, N.; Chavez, M.; Seidel, L.; Gast, P.; Polus, M.; Loly, C.; Delvenne, P.; et al. A single center experience in resectable pancreatic ductal adenocarcinoma: The limitations of the surgery-first approach. Critical review of the literature and proposals for practice update. Acta Gastro Enterol. Belg. 2017, 80, 451–461. [Google Scholar]
- Barugola, G.; Partelli, S.; Crippa, S.; Butturini, G.; Salvia, R.; Sartori, N.; Bassi, C.; Falconi, M.; Pederzoli, P. Time trends in the treatment and prognosis of resectable pancreatic cancer in a large tertiary referral centre. Hpb. 2013, 15, 958–964. [Google Scholar] [CrossRef] [Green Version]
- Okada, K.I.; Shimokawa, T.; Hirono, S.; Kawai, M.; Sho, M.; Satoi, S.; Matsumoto, I.; Eguchi, H.; Murakami, Y.; Yamada, S.; et al. Effect of neoadjuvant nab-paclitaxel plus gemcitabine therapy on overall survival in patients with borderline resectable pancreatic cancer: A prospective multicenter phase ii trial (nac-ga trial). Oncology 2017, 93, 343–346. [Google Scholar] [CrossRef]
- Ielpo, B.; Caruso, R.; Duran, H.; Diaz, E.; Fabra, I.; Malave, L.; Ferri, V.; Alvarez, R.; Cubillo, A.; Plaza, C.; et al. A comparative study of neoadjuvant treatment with gemcitabine plus nab-paclitaxel versus surgery first for pancreatic adenocarcinoma. Surg. Oncol. 2017, 26, 402–410. [Google Scholar] [CrossRef] [PubMed]
- Mishra, M.V.; Champ, C.E.; Keith, S.W.; Showalter, T.N.; Anne, P.R.; Lawrence, Y.R.; Bar-Ad, V. Conditional survival probabilities for patients with resected pancreatic adenocarcinoma. Am. J. Clin. Oncol. 2014, 37, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Tas, F.; Sen, F.; Odabas, H.; Kilic, L.; Keskin, S.; Yildiz, I. Performance status of patients is the major prognostic factor at all stages of pancreatic cancer. Int. J. Clin. Oncol. 2013, 18, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Distler, M.; Pilarsky, E.; Kersting, S.; Grutzmann, R. Preoperative cea and ca 19-9 are prognostic markers for survival after curative resection for ductal adenocarcinoma of the pancreas—A retrospective tumor marker prognostic study. Int. J. Surg. 2013, 11, 1067–1072. [Google Scholar] [CrossRef]
- Saka, B.; Balci, S.; Basturk, O.; Bagci, P.; Postlewait, L.M.; Maithel, S.; Knight, J.; El-Rayes, B.; Kooby, D.; Sarmiento, J.; et al. Pancreatic ductal adenocarcinoma is spread to the peripancreatic soft tissue in the majority of resected cases, rendering the ajcc t-stage protocol (7th edition) inapplicable and insignificant: A size-based staging system (pT1: ≤2, pT2: >2–≤4, pT2: >4 cm) is more valid and clinically relevant. Ann. Surg. Oncol. 2016, 23, 2010–2018. [Google Scholar]
- Jamieson, N.B.; Chan, N.I.; Foulis, A.K.; Dickson, E.J.; McKay, C.J.; Carter, C.R. The prognostic influence of resection margin clearance following pancreaticoduodenectomy for pancreatic ductal adenocarcinoma. J. Gastrointest. Surg. 2013, 17, 511–521. [Google Scholar] [CrossRef]
- Brennan, M.F.; Kattan, M.W.; Klimstra, D.; Conlon, K. Prognostic nomogram for patients undergoing resection for adenocarcinoma of the pancreas. Ann. Surg. 2004, 240, 293–298. [Google Scholar] [CrossRef]
- Lee, S.H.; Chung, M.J.; Kim, B.; Lee, H.S.; Lee, H.J.; Heo, J.Y.; Kim, Y.J.; Park, J.Y.; Bang, S.; Park, S.W.; et al. The significance of the prognostic nutritional index for all stages of pancreatic cancer. Nutr. Cancer 2017, 69, 512–519. [Google Scholar] [CrossRef]
- Network®, N.C.C. Nccn Clinical Practice Guidelines in Oncology (nccn guidelines®) Pancreatic Adenocarcinoma, Version 3.2019. Available online: https://www.nccn.org/professionals/physician_gls/default.aspx (accessed on 29 August 2019).
- Kim, Y.H.; Saini, S.; Sahani, D.; Hahn, P.F.; Mueller, P.R.; Auh, Y.H. Imaging diagnosis of cystic pancreatic lesions: Pseudocyst versus nonpseudocyst. Radiographics 2005, 25, 671–685. [Google Scholar] [CrossRef]
- Contal, C.; O’Quigley, J. An application of changepoint methods in studying the effect of age on survival in breast cancer. Comput. Stat. Data Anal. 1999, 30, 253–270. [Google Scholar] [CrossRef]
- Ferrone, C.R.; Kattan, M.W.; Tomlinson, J.S.; Thayer, S.P.; Brennan, M.F.; Warshaw, A.L. Validation of a postresection pancreatic adenocarcinoma nomogram for disease-specific survival. J. Clin. Oncol. 2005, 23, 7529–7535. [Google Scholar] [CrossRef] [PubMed]
- De Castro, S.M.; Biere, S.S.; Lagarde, S.M.; Busch, O.R.; van Gulik, T.M.; Gouma, D.J. Validation of a nomogram for predicting survival after resection for adenocarcinoma of the pancreas. Br. J. Surg. 2009, 96, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Clark, E.J.; Taylor, M.A.; Connor, S.; O’Neill, R.; Brennan, M.F.; Garden, O.J.; Parks, R.W. Validation of a prognostic nomogram in patients undergoing resection for pancreatic ductal adenocarcinoma in a uk tertiary referral centre. HPB 2008, 10, 501–505. [Google Scholar] [CrossRef]
- Shen, Y.N.; Bai, X.L.; Jin, G.; Zhang, Q.; Lu, J.H.; Qin, R.Y.; Yu, R.S.; Pan, Y.; Chen, Y.; Sun, P.W.; et al. A preoperative nomogram predicts prognosis of up front resectable patients with pancreatic head cancer and suspected venous invasion. HPB 2018. [Google Scholar] [CrossRef]
- Tetsuya Nakatsura, T.H.; Tsubono, Y.; Ryu, M.; Kinoshita, T.; Kawano, N.; Konishi, M.; Kosuge, T.; Kanai, Y.; Mukai, K. Histological prognostic parameters for adenocarcinoma of the pancreatic head. Proposal for a scoring system for prediction of outcome. J. Hepato Biliary Pancreat. Surg. 1997, 4, 441–448. [Google Scholar]
- Millikan, K.W.; Deziel, D.J.; Silverstein, J.C.; Kanjo, T.M.; Christein, J.D.; Doolas, A.; Prinz, R.A. Prognostic factors associated with resectable adenocarcinoma of the head of the pancreas. Am. Surg. 1999, 65, 618–623, discussion 623–624. [Google Scholar]
- Roche, C.J.; Hughes, M.L.; Garvey, C.J.; Campbell, F.; White, D.A.; Jones, L.; Neoptolemos, J.P. Ct and pathologic assessment of prospective nodal staging in patients with ductal adenocarcinoma of the head of the pancreas. AJR Am. J. Roentgenol. 2003, 180, 475–480. [Google Scholar] [CrossRef]
- Vyas, S.J.; Puri, Y.S.; John, B.J.; Yu, D.; Watkins, J.; Imber, C.; Fusai, G.; Arjun, S.; Sharma, D.; Davidson, B.R.; et al. Radiological tumor density and lymph node size correlate with survival in resectable adenocarcinoma of the pancreatic head: A retrospective cohort study. J. Cancer Res. Ther. 2016, 12, 417–421. [Google Scholar] [CrossRef]
- Jamieson, N.B.; Glen, P.; McMillan, D.C.; McKay, C.J.; Foulis, A.K.; Carter, R.; Imrie, C.W. Systemic inflammatory response predicts outcome in patients undergoing resection for ductal adenocarcinoma head of pancreas. Br. J. Cancer 2005, 92, 21–23. [Google Scholar] [CrossRef]
- Mujica, V.R.; Barkin, J.S.; Go, V.L. Acute pancreatitis secondary to pancreatic carcinoma. Study group participants. Pancreas 2000, 21, 329–332. [Google Scholar] [CrossRef] [PubMed]
- Hoshimoto, S.; Hishinuma, S.; Shirakawa, H.; Tomikawa, M.; Ozawa, I.; Wakamatsu, S.; Hoshi, S.; Hoshi, N.; Hirabayashi, K.; Ogata, Y. Reassessment of the clinical significance of portal-superior mesenteric vein invasion in borderline resectable pancreatic cancer. Eur. J. Surg. Oncol. 2017, 43, 1068–1075. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total |
|---|---|
| Clinical information | |
| Age (years) | 66 (41–81) |
| Gender | |
| Male | 77 (56.6%) |
| Female | 59 (43.4%) |
| BMI (kg/m2) | 22.7 (15.9–32.3) |
| PNI | 48.2 (30.4–60.1) |
| Symptoms at diagnosis † | 106 (77.9%) |
| Preoperative serum CA19-9 (continuous) (U/mL) | 119.7 (0.1–13,800.0) |
| Serum total bilirubin at diagnosis (mg/dL) | 2.3 (0.1–38.3) |
| Serum albumin at diagnosis (mg/dL) | 4.0 (2.7–5.0) |
| Type of surgery | |
| Whipple’s operation | 10 (7.4 %) |
| PPPD | 126 (92.6%) |
| Combined vascular resection | 36 (26.5%) |
| Adjuvant chemotherapy | 109 (80.1%) |
| CT findings | |
| Size (mm) | 23.6 (11.8–50.2) |
| Radiologists’ conclusion for resectability | |
| Resectable | 82 (60.3%) |
| Borderline resectable | 54 (39.7%) |
| Pathologic findings | |
| Size (mm) | 25.0 (12–70) |
| Differentiation | |
| Well | 15 (11.0%) |
| Moderate | 109 (80.1%) |
| Poorly | 12 (8.8%) |
| Lymphovascular invasion | 65 (47.8%) |
| Perineural invasion | 113 (83.1%) |
| Lymph node metastasis | 87 (64.0%) |
| Resection margin | |
| Negative | 113 (83.1%) |
| Positive | 23 (16.9%) |
| Parameters | Disease-Free Survival | Overall Survival | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | P Value | HR | 95% CI | P Value | |
| Symptoms at diagnosis | 2.01 | 1.12–3.62 | 0.020 | 1.68 | 0.88–3.22 | 0.115 |
| Preoperative serum CA 19-9 ≥ 34 U/mL | 1.63 | 0.97–2.72 | 0.065 | 2.29 | 1.19–4.39 | 0.013 |
| Necrosis on CT | 1.64 | 0.97–2.79 | 0.066 | 2.42 | 1.39–4.21 | 0.002 |
| PV or SMV invasion on CT | 1.4 | 0.89–2.21 | 0.150 | 1.67 | 0.99–2.81 | 0.055 |
| Regional LN suspicious for metastasis on CT | 2.07 | 1.35–3.19 | 0.001 | 1.53 | 0.92–2.54 | 0.099 |
| Associated pancreatitis or pseudocyst on CT | 0.51 | 0.30–0.86 | 0.013 | 0.54 | 0.30–0.98 | 0.041 |
| Harrell’s c-statistics | 0.6496 (0.0325) | 0.6746 (0.0384) | ||||
| Chracteristics | Disease-Free Survival | Overall Survival | ||||
|---|---|---|---|---|---|---|
| Low-Risk (n = 69) | High-Risk (n = 67) | P Value | Low-Risk (n = 72) | High-Risk (n = 64) | P Value | |
| Clinical information | ||||||
| Age, year (Q1–Q3) | 66 (62–71) | 64 (55–71) | 0.237 | 66 (58.5–71) | 65.5 (59–71) | 0.843 |
| Gender | 0.712 | 0.791 | ||||
| Male | 38 (55.1%) | 39 (58.2%) | 40 (55.6%) | 37 (57.8%) | ||
| Female | 31 (44.9%) | 28 (41.8%) | 32 (44.4%) | 27 (42.2%) | ||
| Preoperative serum CA 19-9(continuous), U/mL (Q1–Q3) | 56.0 (26.2–28.6) | 203.9 (49.2–734.8) | 0.003 | 54.0 (19.9–212.6) | 295.0 (97.6–772.0) | <0.001 |
| Adjuvant chemotherapy | 57(82.6%) | 52(77.6%) | 0.4652 | 61 (84.7%) | 48 (75.0%) | 0.156 |
| Gemcitabine-based | 42 (53.8%) | 36 (46.2%) | 0.607 | 44 (56.4%) | 34 (46.6%) | 0.882 |
| Other | 15 (48.4%) | 16 (51.6%) | 17 (54.8%) | 14 (45.2%) | ||
| Pathologic findings | ||||||
| Size, mm (Q1–Q3) | 23 (20–30) | 26 (22–32) | 0.019 | 23.5 (20–30) | 25.5 (22–30) | 0.057 |
| Peripancreatic fat invasion | 68 (98.6%) | 67 (100.0 %) | >0.999 | 71 (98.6%) | 64 (100.0%) | >0.999 |
| Differentiation | 0.741 | 0.844 | ||||
| Well | 7 (10.1%) | 8 (11.9%) | 7 (9.7%) | 8 (12.5%) | ||
| Moderate | 57 (82.6%) | 52 (77.6%) | 59 (82.0%) | 50 (78.1%) | ||
| Poorly | 5 (7.2%) | 7 (10.4%) | 6 (8.3%) | 6 (9.4%) | ||
| Lymphovascular invasion | 31 (45.6%) | 30 (44.8%) | 0.925 | 34 (47.9%) | 29 (45.3%) | 0.765 |
| Perineural invasion | 56 (82.4%) | 57(85.1%) | 0.669 | 60 (84.5%) | 53 (82.8%) | 0.790 |
| Lymph node metastasis | 38 (55.1%) | 49 (73.1%) | 0.028 | 41 (56.9%) | 46 (71.9%) | 0.070 |
| Lymph node ratio (Q1–Q3) | 0.04 (0–0.15) | 0.06 (0–0.18) | 0.143 | 0.06 (0–0.15) | 0.06 (0–0.18) | 0.306 |
| Resection margin positive | 9 (13.0%) | 14 (20.9%) | 0.240 | 12 (16.7%) | 11 (17.2%) | 0.503 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, S.H.; Kim, H.Y.; Lee, E.J.; Hwang, H.K.; Park, M.-S.; Kim, M.-j.; Lee, W.J.; Chung, Y.E.; Kang, C.M. Preoperative Clinical and Computed Tomography (CT)-Based Nomogram to Predict Oncologic Outcomes in Patients with Pancreatic Head Cancer Resected with Curative Intent: A Retrospective Study. J. Clin. Med. 2019, 8, 1749. https://doi.org/10.3390/jcm8101749
Hwang SH, Kim HY, Lee EJ, Hwang HK, Park M-S, Kim M-j, Lee WJ, Chung YE, Kang CM. Preoperative Clinical and Computed Tomography (CT)-Based Nomogram to Predict Oncologic Outcomes in Patients with Pancreatic Head Cancer Resected with Curative Intent: A Retrospective Study. Journal of Clinical Medicine. 2019; 8(10):1749. https://doi.org/10.3390/jcm8101749
Chicago/Turabian StyleHwang, Shin Hye, Ha Yan Kim, Eun Ju Lee, Ho Kyoung Hwang, Mi-Suk Park, Myeong-jin Kim, Woo Jung Lee, Yong Eun Chung, and Chang Moo Kang. 2019. "Preoperative Clinical and Computed Tomography (CT)-Based Nomogram to Predict Oncologic Outcomes in Patients with Pancreatic Head Cancer Resected with Curative Intent: A Retrospective Study" Journal of Clinical Medicine 8, no. 10: 1749. https://doi.org/10.3390/jcm8101749