Antibiotic Use and Long-Term Outcome in Patients with Tick-Borne Encephalitis and Co-Infection with Borrelia Burgdorferi Sensu Lato in Central Europe. A Retrospective Cohort Study

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
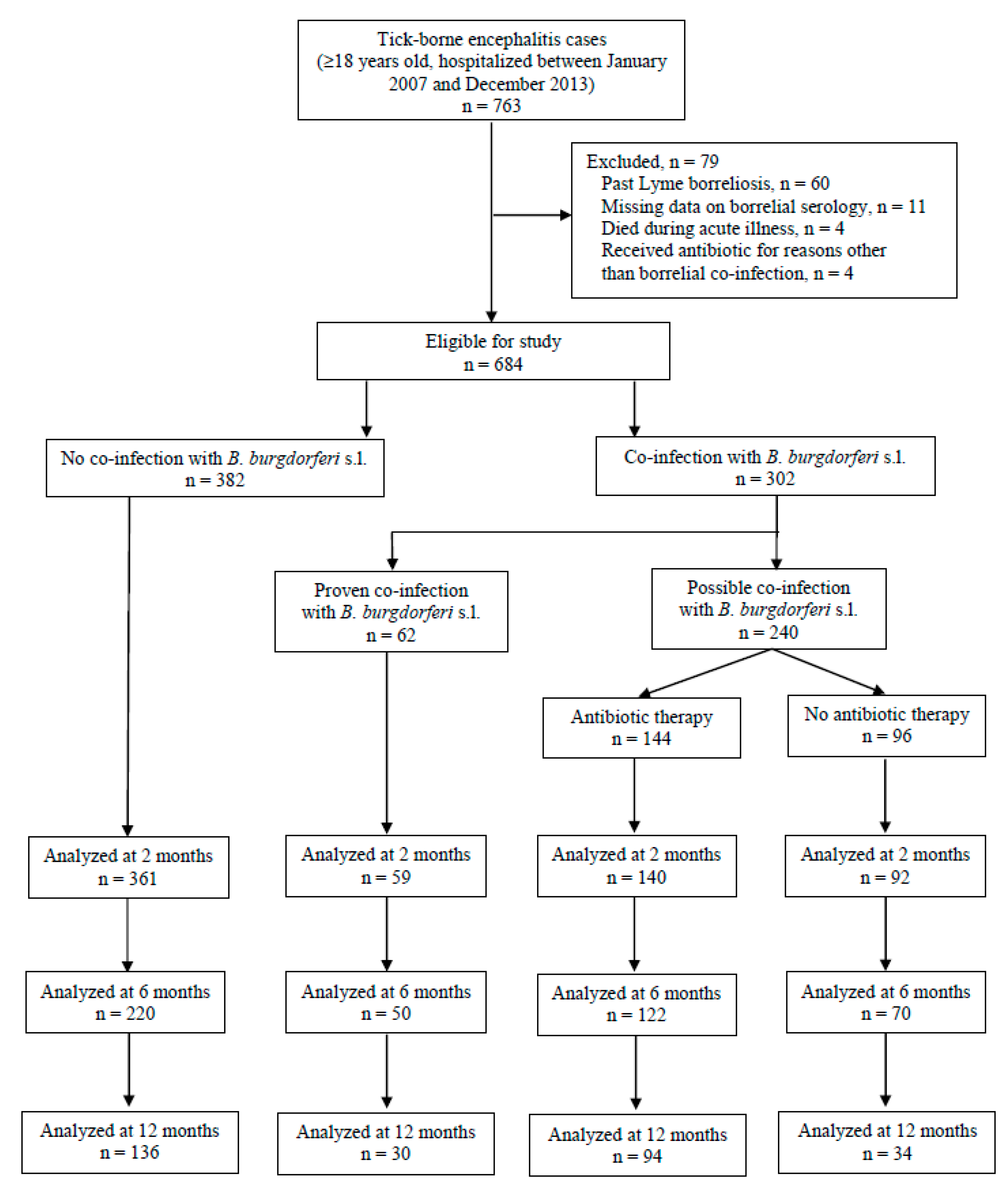
2.1. Setting and Patients
2.2. Evaluation of Patients
2.3. Laboratory Evaluation
2.4. Statistical Analysis
3. Results
3.1. Patients’ Characteristics on Admission
3.2. Patients with Tick-Borne Encephalitis (TBE) and Proven Borrelial Co-Infection (TBE-Lyme Borreliosis (LB) Group)
3.3. Outcome in Patients with TBE and Possible Borrelial Co-Infection (TBE-Bb Group) According to Anti-Borrelial Antibiotic Therapy
3.4. Outcome in Patients with TBE in Relation to Borrelial Co-Infection
3.5. Intercurrent Antibiotics, Intercurrent Lyme Borreliosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Lindquist, L.; Vapalahti, O. Tick-borne encephalitis. Lancet 2008, 371, 1861–1871. [Google Scholar] [CrossRef]
- Stanek, G.; Strle, F. Lyme borreliosis—from tick bite to diagnosis and treatment. FEMS Microbiol. Rev. 2018, 42, 233–258. [Google Scholar] [CrossRef] [PubMed]
- Institute of Public Health of the Republic of Slovenia. Epidemiologic Surveillance of Communicable Diseases in Slovenia in 2016. Ljubljana 2017. Available online: http://www.nijz.si/sites/www.nijz.si/files/publikacije-datoteke/epidemiolosko_spremljanje_nb_slo_2016.pdf (accessed on 28 April 2019).
- Cimperman, J.; Maraspin, V.; Lotrič-Furlan, S.; Ružić-Sabljić, E.; Avšič Županc, T.; Picken, R.N.; Strle, F. Concomitant infection with tick-borne encephalitis virus and Borrelia burgdorferi sensu lato in patients with acute meningitis or meningoencephalitis. Infection 1998, 26, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Tomažič, J.; Pikelj, F.; Schwartz, B.; Kunze, M.; Kraigher, A.; Matjašič, M.; Lešničar, G.; Gorišek, J.; Kunz, C.; Marth, E. The clinical features of tick-borne encephalitis in Slovenia: A study of 492 cases in 1994. Antibiot. Monit. 1996, 12, 115–120. [Google Scholar]
- Lotrič-Furlan, S.; Petrovec, M.; Avsic-Zupanc, T.; Nicholson, W.L.; Sumner, J.W.; Childs, J.E.; Strle, F. Prospective assessment of the etiology of acute febrile illness after a tick bite in Slovenia. Clin. Infect. Dis. 2001, 33, 503–510. [Google Scholar] [CrossRef]
- Vorobyeva, N.N.; Korenberg, E.I.; Grigoryan, Y.V. Diagnostics of tick-borne diseases in the endemic region of Russia. Wien. Klin. Wochenschr. 2002, 114, 610–612. [Google Scholar]
- Cerar, T.; Ogrinc, K.; Strle, F.; Ružić-Sabljić, E. Humoral Immune Responses in Patients with Lyme Neuroborreliosis. Clin. Vaccine Immunol. 2010, 17, 645–650. [Google Scholar] [CrossRef] [Green Version]
- Czupryna, P.; Moniuszko, A.; Pancewicz, S.A.; Grygorczuk, S.; Kondrusik, M.; Zajkowska, J. Tick-borne encephalitis in Poland in years 1993–2008—epidemiology and clinical presentation. A retrospective study of 687 patients. Eur. J. Neurol. 2011, 18, 673–679. [Google Scholar] [CrossRef]
- Lotric-Furlan, S.; Strle, F. Peripheral facial palsy in patients with tick-borne encephalitis. Clin. Microbiol. Infect. 2012, 18, 1027–1032. [Google Scholar] [CrossRef] [Green Version]
- Moniuszko, A.; Dunaj, J.; Święcicka, I.; Zambrowski, G.; Chmielewska-Badora, G.; Żukiewicz-Sobczak, W.; Zajkowska, J.; Czupryna, P.; Kondrusik, M.; Grygorczuk, S.; et al. Co-infections with Borrelia species, Anaplasma phagocytophilum and Babesia spp. in patients with tick-borne encephalitis. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 1835–1841. [Google Scholar] [CrossRef]
- Bogovič, P.; Lotrič-Furlan, S.; Avšič-Županc, T.; Lusa, L.; Strle, F. Factors associated with severity of tick-borne encephalitis: A prospective observational study. Travel Med. Infect. Dis. 2018, 26, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, R. Tick-borne encephalitis. Infect. Dis. Clin. N. Am. 2008, 22, 561–575. [Google Scholar] [CrossRef] [PubMed]
- Mansfield, K.L.; Johnson, N.; Phipps, L.P.; Stephenson, J.R.; Fooks, A.R.; Solomon, T. Tick-borne encephalitis virus—A review of an emerging zoonosis. J. Gen. Virol. 2009, 90, 1781–1794. [Google Scholar] [CrossRef] [PubMed]
- Wormser, G.P.; Dattwyler, R.J.; Shapiro, E.D.; Halperin, J.J.; Steere, A.C.; Klempner, M.S.; Krause, P.J.; Bakken, J.S.; Strle, F.; Stanek, G.; et al. The clinical assessment, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis: Clinical practice guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 2006, 43, 1089–1134. [Google Scholar] [CrossRef]
- Stanek, G.; Fingerle, V.; Hunfeld, K.P.; Jaulhac, B.; Kaiser, R.; Krause, A.; Kristoferitsch, W.; O’Connell, S.; Ornstein, K.; Strle, F.; et al. Lyme borreliosis: Clinical case definitions for diagnosis and management in Europe. Clin. Microbiol. Infect. 2011, 17, 69–79. [Google Scholar] [CrossRef] [Green Version]
- Taba, P.; Schmutzhard, E.; Forsberg, P.; Lutsar, I.; Ljøstad, U.; Mygland, A.; Levchenko, I.; Strle, F.; Steiner, I. EAN consensus review on prevention, diagnosis and management of tick-borne encephalitis. Eur. J. Neurol. 2017, 10, 1214. [Google Scholar] [CrossRef]
- Bogovic, P.; Logar, M.; Avsic-Zupanc, T.; Strle, F.; Lotric-Furlan, S. Quantitative evaluation of the severity of acute illness in adult patients with tick-borne encephalitis. Biomed. Res. Int. 2014, 2014, 841027. [Google Scholar] [CrossRef]
- Ružić-Sabljić, E.; Maraspin, V.; Cimperman, J.; Lotrič-Furlan, S.; Strle, F. Evaluation of immunofluorescence test (IFT) and immuno (western) blot (WB) test in patients with erythema migrans. Wien. Klin. Wochenschr. 2002, 114, 586–590. [Google Scholar]
- Cerar, T.; Ružić-Sabljić, E.; Cimperman, J.; Strle, F. Comparison of immunofluorescence assay (IFA) and Liaison® in patients with different clinical manifestations of Lyme borreliosis. Wien. Klin. Wochenschr. 2006, 118, 686–690. [Google Scholar] [CrossRef] [PubMed]
- Reiber, H.; Peter, J.B. Cerebrospinal fluid analysis: Disease related data patterns and evaluation progams. J. Neurol. Sci. 2001, 184, 101–122. [Google Scholar] [CrossRef]
- Ružić-Sabljić, E.; Zore, A.; Strle, F. Characterization of Borrelia burgdorferi sensu lato isolates by pulsed-field gel electrophoresis after MluI restriction of genomic DNA. Res. Microbiol. 2008, 159, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Postic, D.; Assous, M.V.; Grimont, P.A.; Baranton, G. Diversityof Borrelia burgdorferi sensu lato evidenced by restriction fragment length polymorphism of rrf (5S)–rrl (23S) intergenic spacer amplicons. Int. J. Syst. Bacteriol. 1994, 44, 743–752. [Google Scholar] [CrossRef] [PubMed]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2016; Available online: http://www.R-project.org (accessed on 12 June 2019).
- Mickiene, A.; Laiskonis, A.; Günther, G.; Vene, S.; Lundkvist, A.; Lindquist, L. Tickborne encephalitis in an area of high endemicity in Lithuania: Disease severity and long-term prognosis. Clin. Infect. Dis. 2002, 35, 650–658. [Google Scholar] [CrossRef]
- Hofhuis, A.; van de Kassteele, J.; Sprong, H.; van den Wijngaard, C.C.; Harms, M.G.; Fonville, M.; Docters van Leeuwen, A.; Simões, M.; van Pelt, W. Predicting the risk of Lyme borreliosis after a tick bite, using a structural equation model. PLoS ONE 2017, 7, e0181807. [Google Scholar] [CrossRef] [PubMed]
- Nahimana, I.; Gern, L.; Blanc, D.S.; Praz, G.; Francioli, P.; Peter, O. Risk of Borrelia burgdorferi infection in western Switzerland following a tick bite. Eur. J. Clin. Microbiol. Infect. Dis. 2004, 23, 603–608. [Google Scholar] [CrossRef]
- Huegli, D.; Moret, J.; Rais, O.; Moosmann, Y.; Erard, P.; Malinverni, R.; Gern, L. Prospective study on the incidence of infection by Borrelia burgdorferi sensu lato after a tick bite in a highly endemic area of Switzerland. Ticks Tick Borne Dis. 2011, 2, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Fryland, L.; Wilhelmsson, P.; Lindgren, P.E.; Nyman, D.; Ekerfelt, C.; Forsberg, P. Low risk of developing Borrelia burgdorferi infection in the south-east of Sweden after being bitten by a Borrelia burgdorferi-infected tick. Int. J. Infect. Dis. 2011, 15, 174–181. [Google Scholar] [CrossRef]
- Stanek, G.; Lusa, L.; Ogrinc, K.; Markowicz, M.; Strle, F. Intrathecally produced IgG and IgM antibodies to recombinant VlsE, VlsE peptide, recombinant OspC and whole cell extracts in the diagnosis of Lyme neuroborreliosis. Med. Microbiol. Immunol. 2014, 203, 125–132. [Google Scholar] [CrossRef]
- Strle, F.; Ružić-Sabljić, E.; Cimperman, J.; Lotrič-Furlan, S.; Maraspin, V. Comparison of findings for patients with Borrelia garinii and Borrelia afzelii isolated from cerebrospinal fluid. Clin. Infect. Dis. 2006, 43, 704–710. [Google Scholar] [CrossRef]
- Korenberg, E.I.; Gorban, L.Y.; Kovalevskii, Y.V.; Frizen, V.I.; Karavanov, A.S. Risk for human tick-borne encephalitis, borrelioses, and double infection in the pre-Ural region of Russia. Emerg. Inf. Dis. 2001, 7, 459–462. [Google Scholar] [CrossRef]
- Dessau, R.B. Diagnostic accuracy and comparison of two assays for Borrelia-specific IgG and IgM antibodies: Proposals for statistical evaluation methods, cut-off values and standardization. J. Med. Microbiol. 2013, 62, 1835–1844. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.; Nelson, C.; Molins, C.; Mead, P.; Schriefer, M. Current guidelines, common clinical pitfalls, and future directions for laboratory diagnosis of Lyme disease, United States. Emerg. Inf. Dis. 2017, 22, 1169–1177. [Google Scholar]
- Johansson, M.; Manfredsson, L.; Wistedt, A.; Serrander, L.; Tjernberg, I. Significant variations in the seroprevalence of C6 ELISA antibodies in a highly endemic area for Lyme borreliosis: Evaluation of age, sex and seasonal differences. APMIS 2017, 125, 476–481. [Google Scholar] [CrossRef] [PubMed]
- Boršič, K.; Blagus, R.; Cerar, T.; Strle, F.; Stupica, D. Clinical course, serologic response, and long-term outcome in elderly patients with early Lyme borreliosis. J. Clin. Med. 2018, 7, 506. [Google Scholar] [CrossRef] [PubMed]
- Logina, I.; Krumina, A.; Karelis, G.; Elsone, L.; Viksna, L.; Rozentale, B.; Donaghy, M. Clinical features of double infection with tick-borne encephalitis and Lyme borreliosis transmitted by tick bite. J. Neurol. Neurosurg. Psychiatry 2006, 77, 1350–1353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vos, R.C.; Kasteleyn, M.J.; Heijmans, M.J.; de Leeuw, E.; Schellevis, F.G.; Rijken, M.; Rutten, G.E.; on behalf of the Diacourse study group. Disentangling the effect of illness perceptions on health status in people with type 2 diabetes after an acute coronary event. BMC Fam. Pract. 2018, 19, 35. [Google Scholar] [CrossRef]


{kind=link}
| Study Period Country | Number of Patients and Patients’ Characteristics | Proven Borrelial Co-Infection | Proven Borrelial CNS Co-Infection b | Possible Borrelial Co-Infection c | Proven and Possible Borrelial Co-Infection |
|---|---|---|---|---|---|
| 1992–1993 Slovenia [4] | 89 patients with TBE | 12 (13.5) | 6 (6.7) | / | / |
| 1994 Slovenia [5] | 492 patients with TBE | 82 (16.7) | 61/489 (12.5) | 60/484 (12.4) d | / |
| 1995–1996 Slovenia [6] | 36 patients with TBE out of 130 patients with acute febrile illness after a tick bite | 6 (16.7) | / | 3 (8.3) d | 9 (25) |
| 1999–2001 Russia [7] | 445 patients with TBE out of 1952 patients with acute febrile illness after a tick bite | / | / | 33 (7.4) e | / |
| 1995–2004 Slovenia [8] | 32 patients with TBE | / | 6 (18.8) f | 15 (46.9) g | / |
| 1993–2008 Poland [9] | 687 patients with TBE | / | 13 (1.9) | 116 (16.9) h | / |
| 2003–2009 Slovenia [10] | 11 patients with peripheral facial palsy out of 1218 patients with TBE | / | 1 (9.1) | 2 (18.2) d | 3 (27.3) |
| 2009–2012 Poland [11] | 110 patients with TBE | / | / | 30 (27) i | / |
| 2007–2012 Slovenia [12] | 717 patients with TBE | / | 22/661 (3.3) | 66/655 (10.1) g | / |
| Characteristic | TBE n = 382 | TBE-LB n = 62 | TBE-Bb n = 240 | p Value a |
|---|---|---|---|---|
| Age | 49 (35–61) | 53 (43–68) | 59 (46–69) | <0.001 |
| Male sex | 208 (54.5) | 39 (62.9) | 148 (61.7) | 0.143 |
| Charlson comorbidity index | 1 (0–2) | 1 (0–2) | 2 (0–3) | <0.001 |
| Vaccinated against TBE | 14 (3.7) | 2 (3.2) | 12 (5.0) | 0.670 |
| Clinical presentation | 0.615 | |||
| Meningitis | 91 (23.8) | 16 (25.8) | 50 (20.8) | |
| Meningoencephalitis | 259 (67.8) | 38 (61.3) | 169 (70.4) | |
| Meningoencephalomyelitis | 32 (8.4) | 8 (12.9) | 21 (8.8) | |
| Severity of acute illness | 0.649 | |||
| Mild | 99 (25.9) | 16 (25.8) | 54 (22.5) | |
| Moderate | 232 (60.7) | 38 (61.3) | 145 (60.4) | |
| Severe | 51 (13.4) | 8 (12.9) | 41 (17.1) | |
| Severity score of acute illness | 12 (8–17) | 12 (6.8–17.8) | 12.5 (9–19) | 0.324 |
| CSF leukocyte count (× 106/L) | 104 (54.8–192) | 101 (65.3–154) | 68.5 (35–134.3) | <0.001 |
| OR (95% CI) a | p Value b | |
|---|---|---|
| Intercept | 0.05 (0.00–0.51) | 0.011 |
| Antibiotic therapy (yes vs. no) | 1.23 (0.53–2.81) | 0.630 |
| Time | ||
| 6 vs. 2 months | 0.24 (0.13–0.44) | <0.001 |
| 12 vs. 6 months | 0.50 (0.25–0.98) | 0.043 |
| Sex (male vs. female) | 0.47 (0.20–1.08) | 0.075 |
| Age, years | 1.05 (1.00–1.10) | 0.058 |
| Charlson comorbidity index | 0.53 (0.32–0.87) | 0.012 |
| Severity score of acute illness | 1.07 (1.02–1.13) | 0.007 |
| All n = 684 | TBE n = 382 | TBE-LB n = 62 | TBE-Bb n = 240 | p Value a | |
|---|---|---|---|---|---|
| 2 months post-hospitalization | 363/652 (55.7) | 202/361 (56.0) | 32/59 (54.2) | 129/232 (55.6) | 0.9698 |
| 6 months post-hospitalization | 170/462 (36.8) | 82/220 (37.3) | 16/50 (32.0) | 72/192 (37.5) | 0.757 |
| 12 months post-hospitalization | 95/294 (32.3) | 44/136 (32.4) | 10/30 (33.3) | 41/128 (32.0) | 0.991 |
| At final evaluable visit | 219/653 (33.5) | 129/361 (35.7) | 15/59 (25.4) | 75/233 (32.2%) | 0.257 |
| OR (95% CI) a | p Value b | |
|---|---|---|
| Intercept | 0.05 (0.01–0.22) | <0.001 |
| TBE-LB vs. TBE | 0.82 (0.34–2.00) | 0.670 |
| TBE-Bb vs. TBE | 1.05 (0.61–1.83) | 0.853 |
| Time | ||
| 6 vs. 2 months | 0.21 (0.14–0.31) | <0.001 |
| 12 vs. 6 months | 0.48 (0.30–0.76) | 0.002 |
| Sex (male vs. female) | 0.51 (0.31–0.86) | 0.011 |
| Age, years | 1.04 (1.01–1.07) | 0.012 |
| Charlson comorbidity index | 0.57 (0.41–0.80) | <0.001 |
| Severity score of acute illness | 1.09 (1.06–1.13) | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Velušček, M.; Blagus, R.; Cerar Kišek, T.; Ružić-Sabljić, E.; Avšič-Županc, T.; F Bajrović, F.; Stupica, D. Antibiotic Use and Long-Term Outcome in Patients with Tick-Borne Encephalitis and Co-Infection with Borrelia Burgdorferi Sensu Lato in Central Europe. A Retrospective Cohort Study. J. Clin. Med. 2019, 8, 1740. https://doi.org/10.3390/jcm8101740
Velušček M, Blagus R, Cerar Kišek T, Ružić-Sabljić E, Avšič-Županc T, F Bajrović F, Stupica D. Antibiotic Use and Long-Term Outcome in Patients with Tick-Borne Encephalitis and Co-Infection with Borrelia Burgdorferi Sensu Lato in Central Europe. A Retrospective Cohort Study. Journal of Clinical Medicine. 2019; 8(10):1740. https://doi.org/10.3390/jcm8101740
Chicago/Turabian StyleVelušček, Maša, Rok Blagus, Tjaša Cerar Kišek, Eva Ružić-Sabljić, Tatjana Avšič-Županc, Fajko F Bajrović, and Daša Stupica. 2019. "Antibiotic Use and Long-Term Outcome in Patients with Tick-Borne Encephalitis and Co-Infection with Borrelia Burgdorferi Sensu Lato in Central Europe. A Retrospective Cohort Study" Journal of Clinical Medicine 8, no. 10: 1740. https://doi.org/10.3390/jcm8101740