Righting the Misperceptions of Men Having Sex with Men: A Pre-Requisite for Protecting and Understanding Gender Incongruence in Vietnam

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
1.1. Global Health Burdens of Men Who Have Sex with Men (MSM) and Transgenders
1.2. Research on MSM and Transgenders in Vietnam
1.3. Research Rationale
2. Materials and Methods
2.1. Study Design and Settings
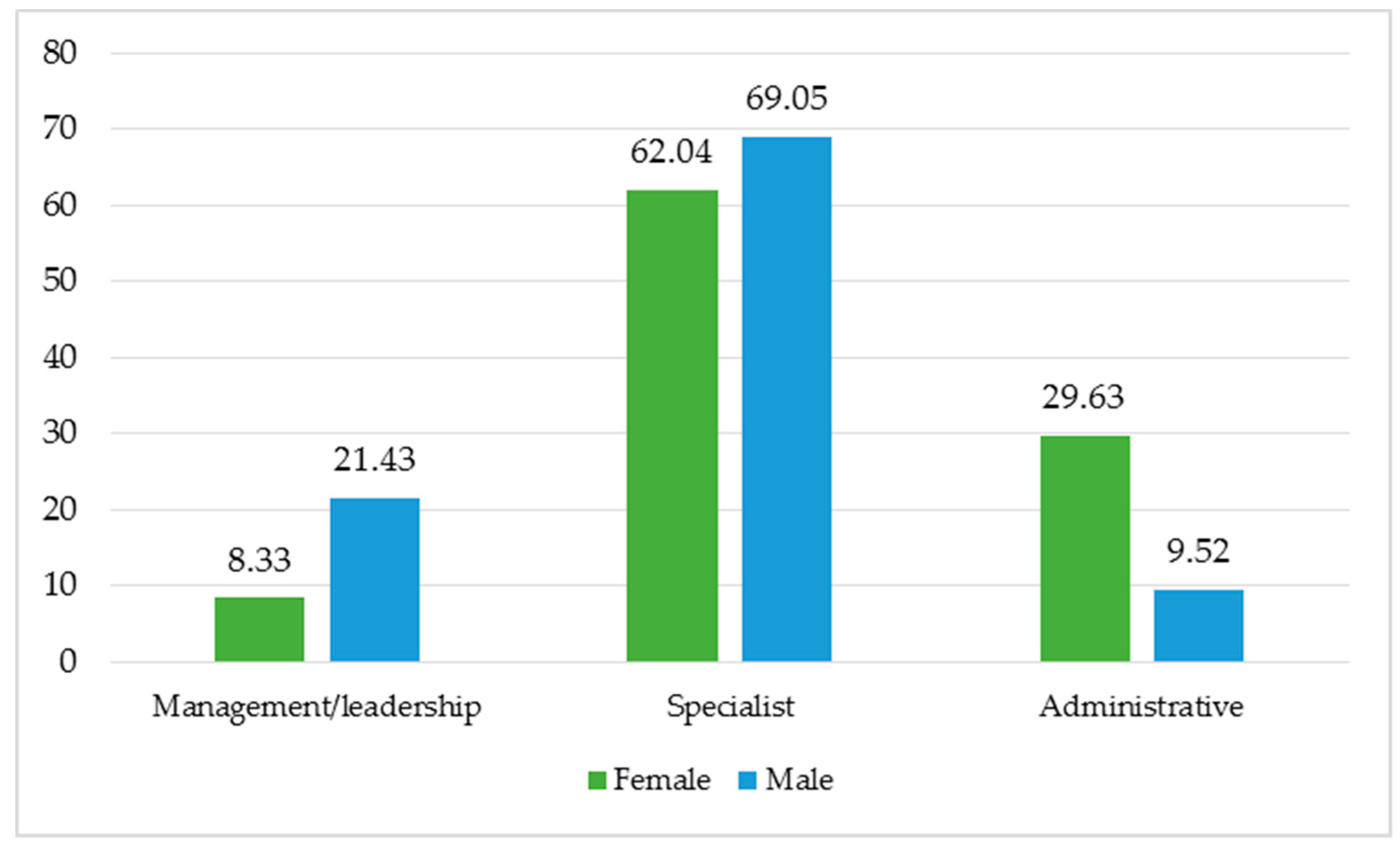
2.2. Participants
3. Results and interpretations
3.1. General Knowledge about MSM and Transgenders
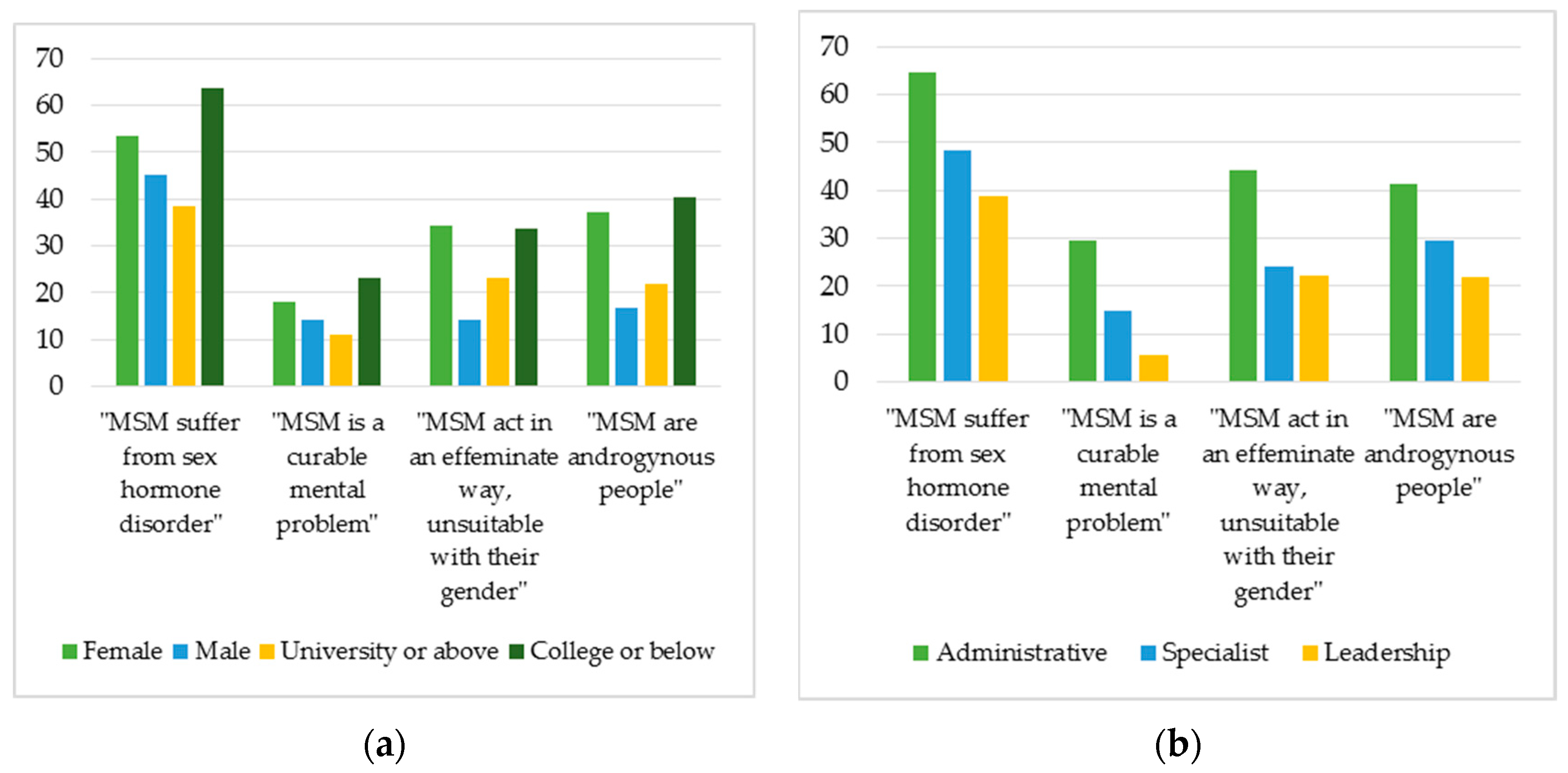
3.1.1. Concerning MSM
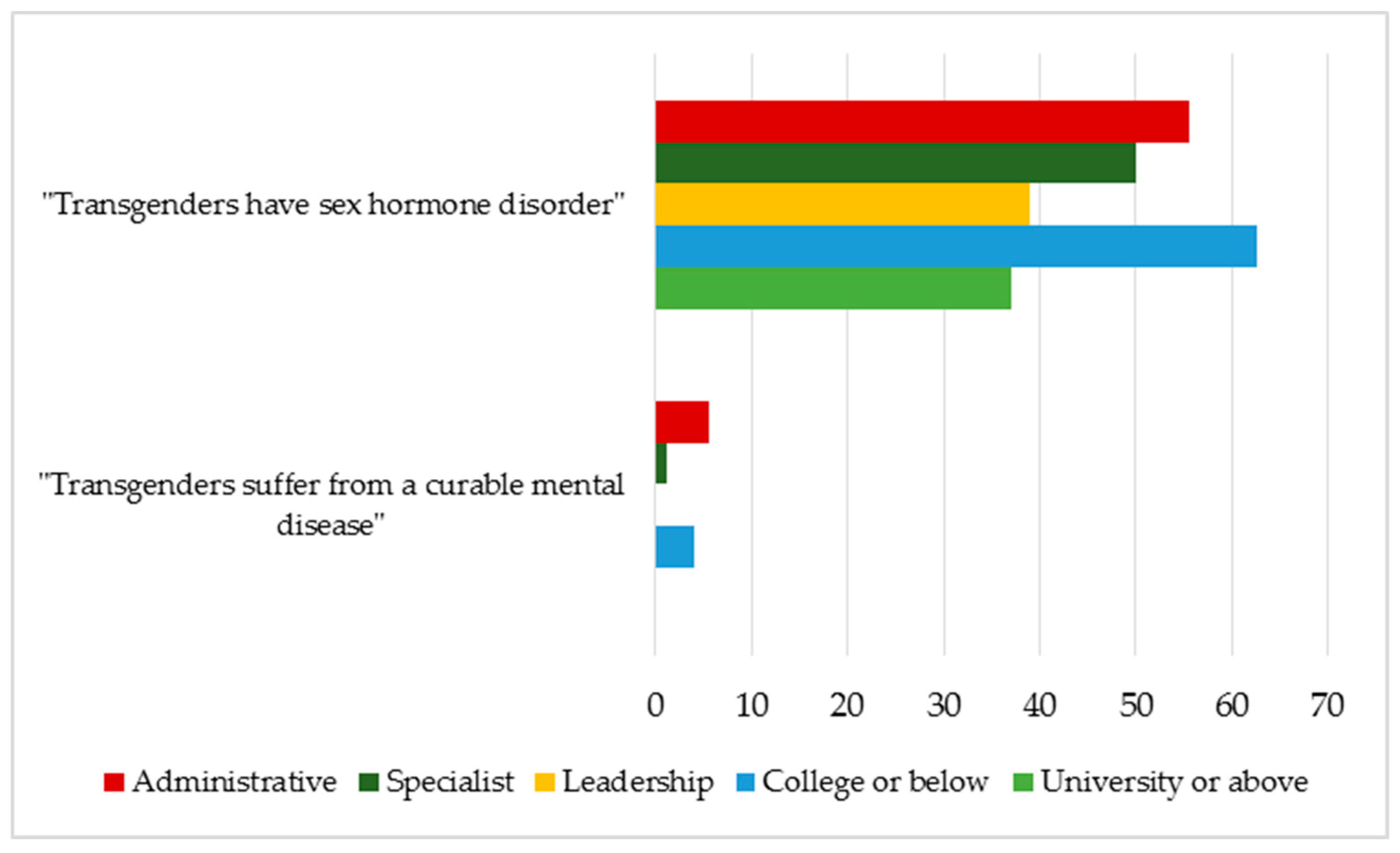
3.1.2. Concerning Transgenders
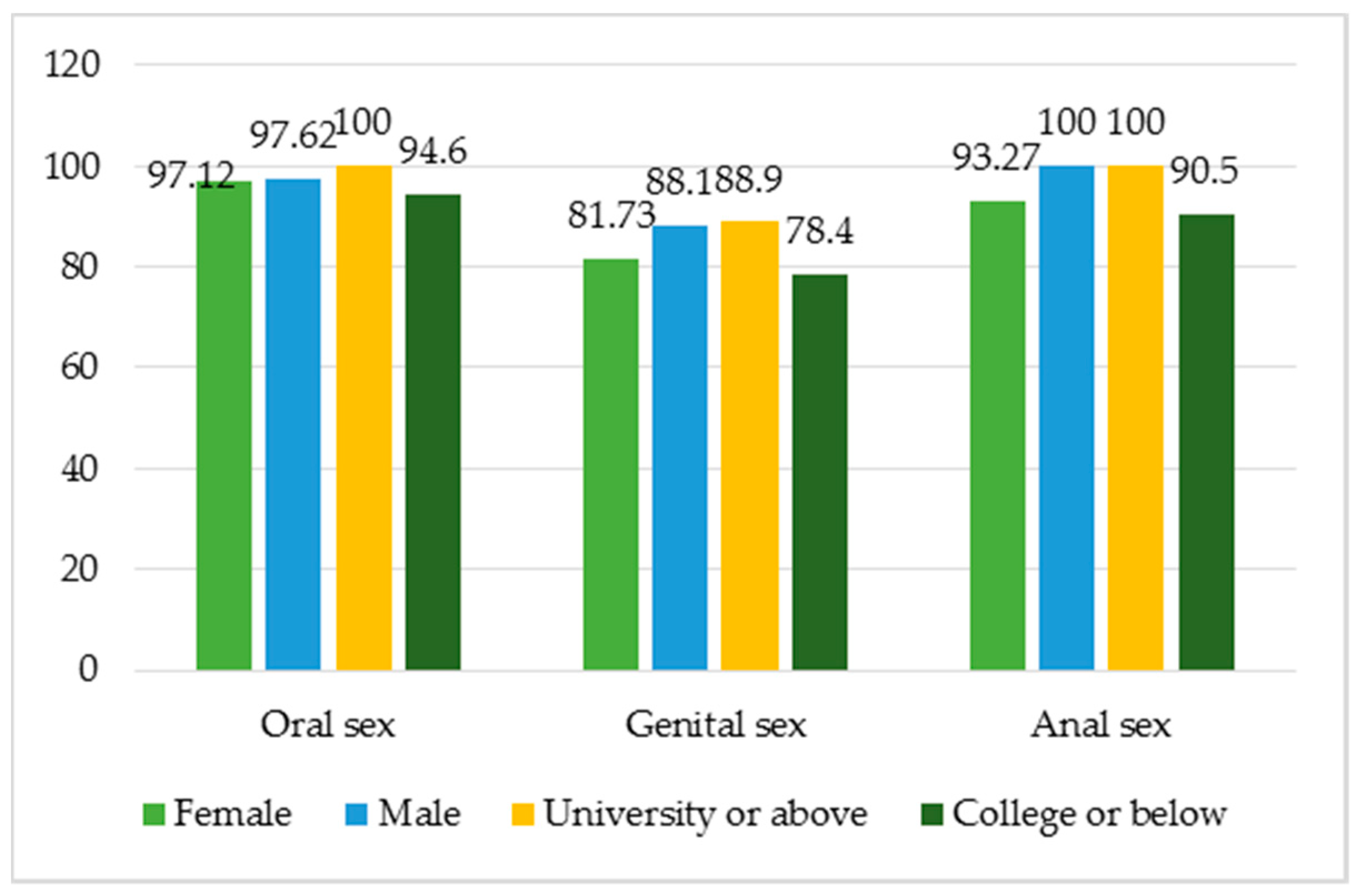
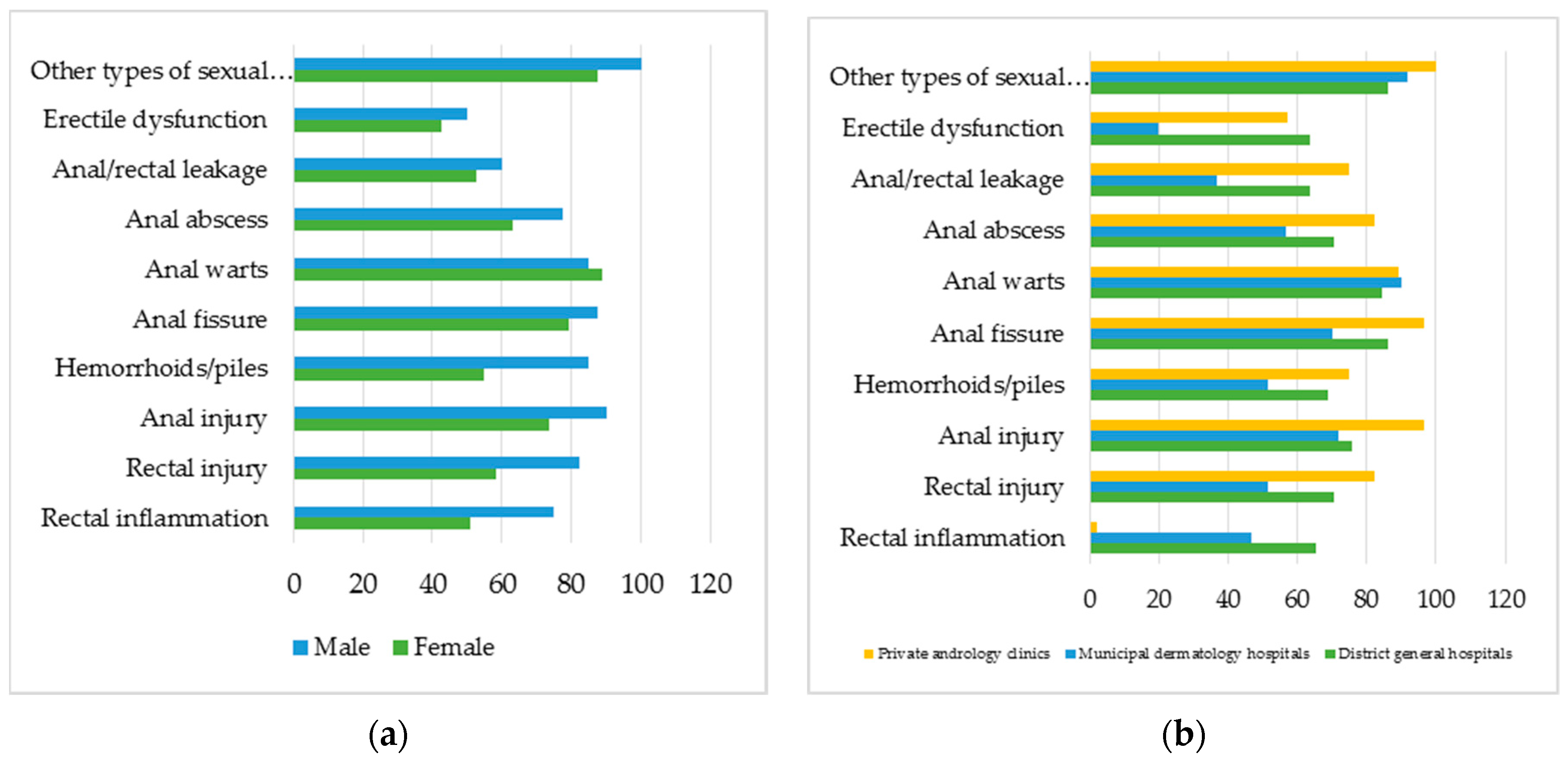
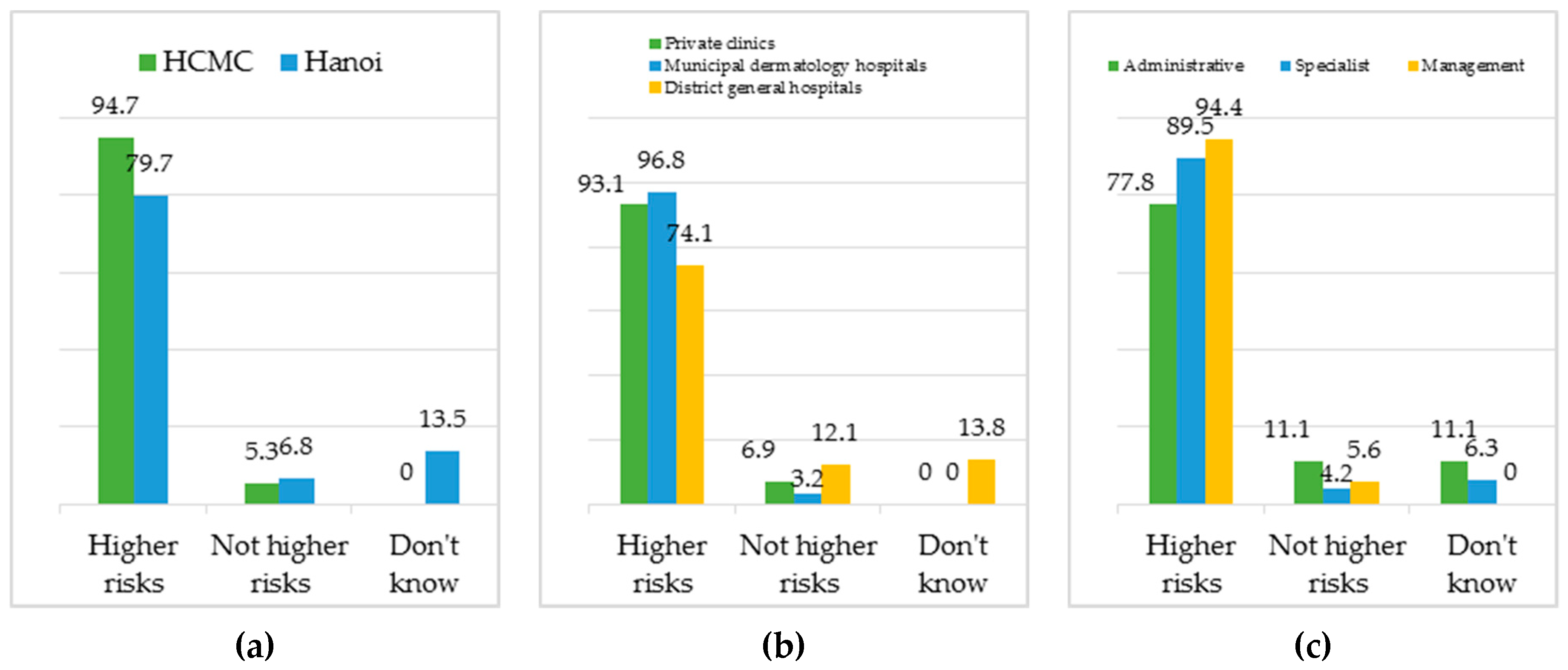
3.2. General Knowledge about Sexual Reproductive Health and HIV/AIDS Risks of MSM and Transgenders
3.2.1. Concerning MSM
3.2.2. Concerning Transgenders
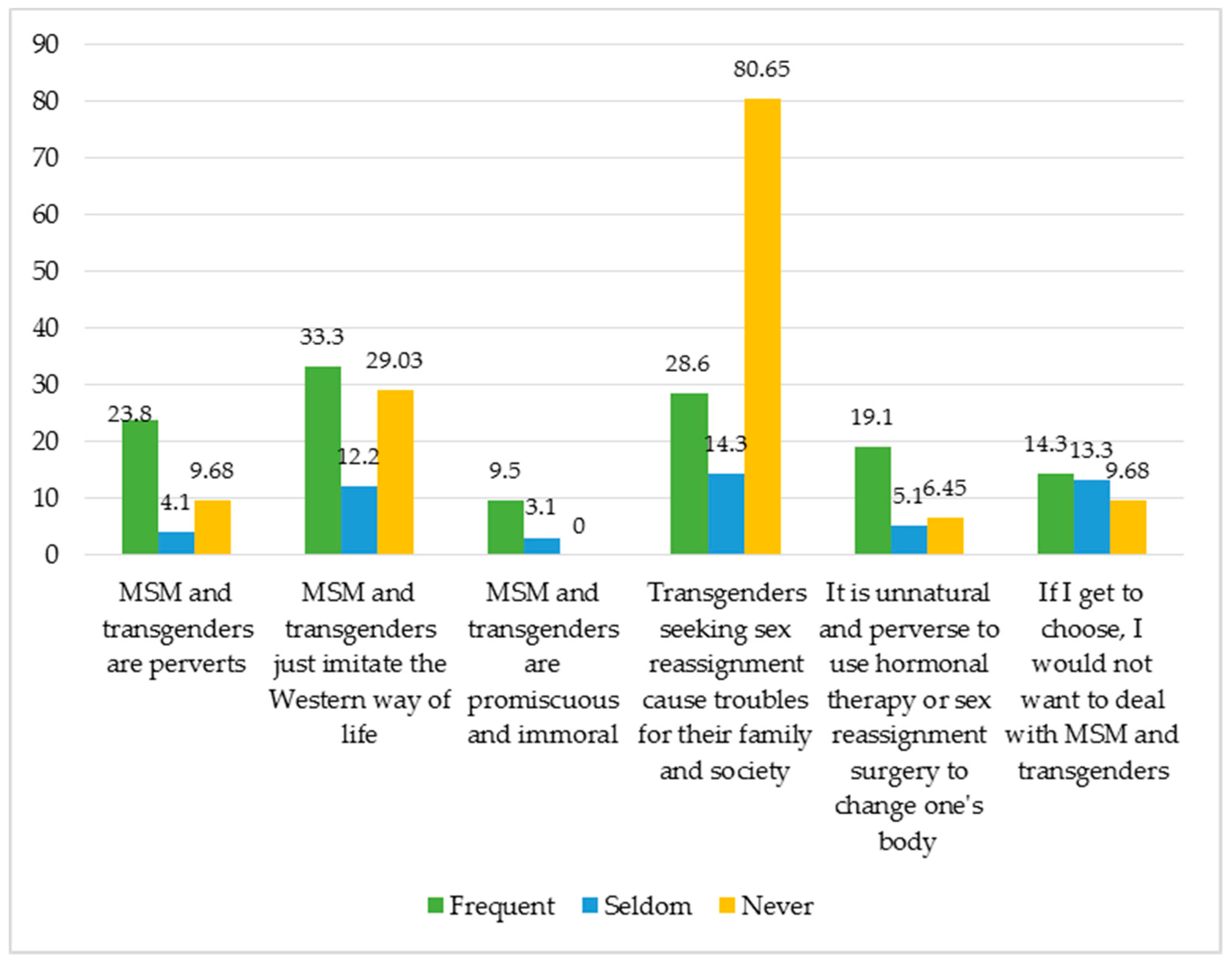
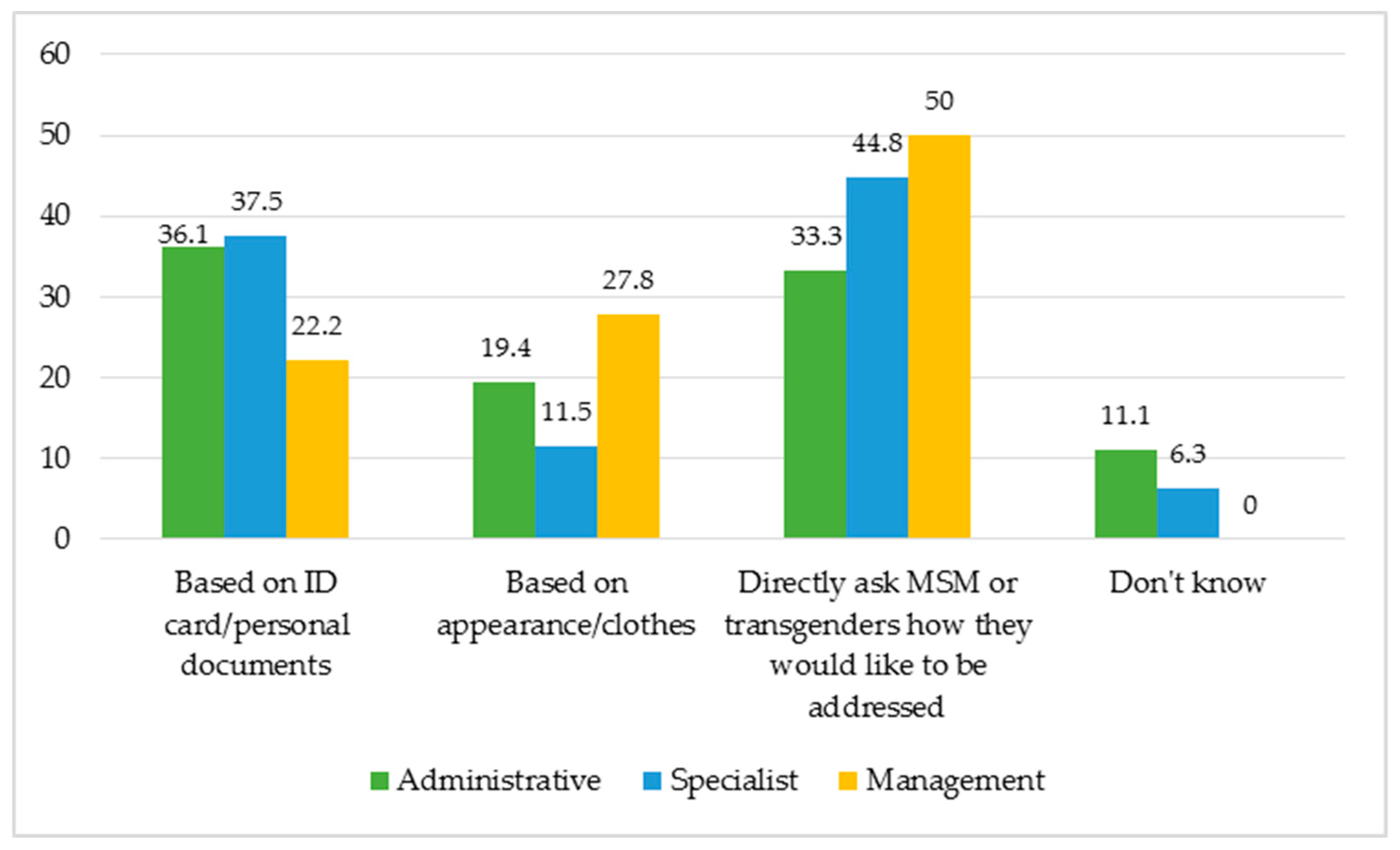
3.3. The Attitudes and Behaviors of Health Professionals towards MSM and Transgenders
4. Discussion
4.1. Limitations
4.2. Implications
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Reisner, S.L.; Poteat, T.; Keatley, J.; Cabral, M.; Mothopeng, T.; Dunham, E.; Holland, C.E.; Max, R.; Baral, S.D. Global health burden and needs of transgender populations: A review. Lancet 2016, 388, 412–436. [Google Scholar]
- Wong, W.; Zhang, J.; Wu, S.; Kong, T.; Ling, D. The HIV related risks among men having sex with men in rural Yunnan, China: A qualitative study. Sex. Trans. Inf. 2006, 82, 127–130. [Google Scholar]
- Clatts, M.C. Disembodied acts: On the perverse use of sexual categories in the study of high-risk behaviour. In Culture Sexual Risk: Anthropological Perspectives on AIDS; Brummelhuis, H.T., Herdt, G.H., Eds.; Gordon and Breach Publishers: Amsterdam, The Netherlands, 1995; pp. 241–256. [Google Scholar]
- Guadamuz, T.E.; Wimonsate, W.; Varangrat, A.; Phanuphak, P.; Jommaroeng, R.; McNicholl, J.M.; Mock, P.A.; Tappero, J.W.; van Griensven, F. HIV prevalence, risk behavior, hormone use and surgical history among transgender persons in Thailand. AIDS Behav. 2011, 15, 650–658. [Google Scholar] [CrossRef]
- USAID. Vietnam Recognizes Transgender Identity Rights. Available online: https://www.usaid.gov/results-data/success-stories/vietnam-recognizes-transgender-identity-rights (accessed on 22 October 2018).
- Global Commission on HIV the Law. HIV and the Law: Risks, Rights & Health. Available online: https://hivlawcommission.org/wp-content/uploads/2017/06/FinalReport-RisksRightsHealth-EN.pdf (accessed on 22 October 2018).
- Reports, S. Same-Sex Marriage Now Legal in Vietnam, but without Government Recognition. Available online: https://www.lgbtqnation.com/2015/01/same-sex-marriage-now-legal-in-vietnam-but-without-government-recognition/ (accessed on 22 October 2018).
- Blanc, M.E. Social construction of male homosexualities in Vietnam. Some keys to understanding discrimination and implications for HIV prevention strategy. Int. Soc. Sci. J. 2005, 57, 661–673. [Google Scholar] [CrossRef]
- Mosbergen, D. Vietnam has been praised as a leader in LGBT rights. Activists beg to differ. Available online: https://www.huffingtonpost.com/entry/lgbt-vietnam_us_56163a78e4b0e66ad4c68090 (accessed on 22 October 2018).
- USAID; UNDP. Being LGBT in Asia: Vietnam Country Report. Available online: https://www.usaid.gov/sites/default/files/documents/1861/Being_LGBT_in_Asia_Viet_Nam_report_ENG.pdf (accessed on 22 October 2018).
- Doan, P.L. Queers in the American city: Transgendered perceptions of urban space. Gend. Place Cult. 2007, 14, 57–74. [Google Scholar]
- Mohale, R. An Exploration on the Challenges Faced by Youth in Lesbians, Gays, Business, Transgender and Intersex Relationships at Mkhuhlu Location, Mpumalanga Province, South Africa. Ph.D. Thesis, University of Venda, Thohoyandou, South Africa, 2018. [Google Scholar]
- Mizock, L.; Hopwood, R. Conflation and interdependence in the intersection of gender and sexuality among transgender individuals. Psychol. Sex. Orientat. Gend. Divers. 2016, 3, 93. [Google Scholar]
- Koh, K.C.; Yong, L.S. HIV risk perception, sexual behavior, and HIV prevalence among men-who-have-sex-with-men at a community-based voluntary counseling and testing center in Kuala Lumpur, Malaysia. Interdiscip. Perspect. Infect. Dis. 2014, 2014, 236240. [Google Scholar] [CrossRef]
- Fein, L.A.; Wong, A.; Honorio, D.; Salgado, C.J.; Medina, C.A. Transgender men’s experiences with and perceptions of gynecologic care [10D]. Obstet. Gynecol. 2017, 129, 44S. [Google Scholar] [CrossRef]
- Logie, C.H.; Lacombe-Duncan, A.; Brien, N.; Jones, N.; Lee-Foon, N.; Levermore, K.; Marshall, A.; Nyblade, L.; Newman, P.A. Barriers and facilitators to HIV testing among young men who have sex with men and transgender women in Kingston, Jamaica: A qualitative study. J. Int. AIDS Soc. 2017, 20, 21385. [Google Scholar]
- Reisner, S.L.; Perez-Brumer, A.G.; McLean, S.A.; Lama, J.R.; Silva-Santisteban, A.; Huerta, L.; Sanchez, J.; Clark, J.L.; Mimiaga, M.J.; Mayer, K.H. Perceived barriers and facilitators to integrating HIV prevention and treatment with cross-sex hormone therapy for transgender women in Lima, Peru. AIDS Behav. 2017, 21, 3299–3311. [Google Scholar]
- White Hughto, J.M.; Clark, K.A.; Altice, F.L.; Reisner, S.L.; Kershaw, T.S.; Pachankis, J.E. Creating, reinforcing, and resisting the gender binary: A qualitative study of transgender women’s healthcare experiences in sex-segregated jails and prisons. Int. J. Prison. Health 2018, 14, 69–88. [Google Scholar]
- Pisani, E.; Girault, P.; Gultom, M.; Sukartini, N.; Kumalawati, J.; Jazan, S.; Donegan, E. HIV, syphilis infection, and sexual practices among transgenders, male sex workers, and other men who have sex with men in Jakarta, Indonesia. Sex. Trans. Inf. 2004, 80, 536–540. [Google Scholar]
- Tun, W.; De Mello, M.; Pinho, A.; Chinaglia, M.; Diaz, J. Sexual risk behaviours and HIV seroprevalence among male sex workers who have sex with men and non-sex workers in Campinas, Brazil. Sex. Trans. Inf. 2008, 84, 455–457. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). HIV prevalence, unrecognized infection, and HIV testing among men who have sex with men—Five US cities, June 2004–April 2005. MMWR Morb. Mortal. Wkly. Rep. 2005, 54, 597. [Google Scholar]
- Sullivan, P.S.; Hamouda, O.; Delpech, V.; Geduld, J.E.; Prejean, J.; Semaille, C.; Kaldor, J.; Folch, C.; de Coul, E.O.; Marcus, U. Reemergence of the HIV epidemic among men who have sex with men in North America, Western Europe, and Australia, 1996–2005. Ann. Epidemiol. 2009, 19, 423–431. [Google Scholar]
- Beyrer, C.; Baral, S.D.; Van Griensven, F.; Goodreau, S.M.; Chariyalertsak, S.; Wirtz, A.L.; Brookmeyer, R. Global epidemiology of HIV infection in men who have sex with men. Lancet 2012, 380, 367–377. [Google Scholar] [Green Version]
- Pathela, P.; Braunstein, S.L.; Schillinger, J.A.; Shepard, C.; Sweeney, M.; Blank, S. Men who have sex with men have a 140-fold higher risk for newly diagnosed HIV and syphilis compared with heterosexual men in New York City. JAIDS J. Acquir. Immune Defic. Syndr. 2011, 58, 408–416. [Google Scholar]
- Safren, S.A.; Martin, C.; Menon, S.; Greer, J.; Solomon, S.; Mimiaga, M.J.; Mayer, K.H. A survey of MSM HIV prevention outreach workers in Chennai, India. AIDS Educ. Prev. 2006, 18, 323–332. [Google Scholar] [CrossRef]
- Bockting, W.O.; Robinson, B.; Rosser, B. Transgender HIV prevention: A qualitative needs assessment. AIDS Care 1998, 10, 505–525. [Google Scholar]
- Baral, S.D.; Poteat, T.; Strömdahl, S.; Wirtz, A.L.; Guadamuz, T.E.; Beyrer, C. Worldwide burden of HIV in transgender women: A systematic review and meta-analysis. Lancet Infect. Dis. 2013, 13, 214–222. [Google Scholar] [CrossRef]
- Sevelius, J. “There’s no pamphlet for the kind of sex I have”: HIV-related risk factors and protective behaviors among transgender men who have sex with nontransgender men. J. Assoc. Nurses AIDS Care 2009, 20, 398–410. [Google Scholar] [CrossRef]
- Goldsamt, L.; Clatts, M.; Giang, L.; Le, B.; Colby, D. Sexual health promotion intervention for male sex workers in Vietnam increases knowledge of STI/HIV transmission risk. J. AIDS Clin. Res. STDs 2017, 4, 009. [Google Scholar]
- Le, M.G.; Vu, D.V.; Bui, T.M.H. Sexual health and men who have sex with men in Vietnam: An integrated approach to preventive health care. Adv. Prev. Med. 2012, 2012, 796192. [Google Scholar] [CrossRef]
- Goldsamt, L.A.; Clatts, M.C.; Giang, L.M.; Le, B.Q.; Colby, D.J.; Yu, G. HIV and other STIs in male sex workers: Findings from a sexual health promotion intervention in Vietnam. Int. J. STD AIDS 2018, 29, 540–546. [Google Scholar] [CrossRef]
- Colby, D.; Cao, N.H.; Doussantousse, S. Men who have sex with men and HIV in Vietnam: A review. AIDS Educ. Prev. 2004, 16, 45–54. [Google Scholar]
- Nguyen, M.X.; Krishnan, A.; Le, G.M.; Nguyen, Q.T.; Bhadra, N.M.; Nguyen, S.M.; Miller, W.C.; Go, V.F. The use of technology to find sexual health information online among men who have sex with men in Hanoi, Vietnam, 2016. Int. J. STD AIDS 2018, 29, 505–510. [Google Scholar]
- Khuat, T.H.; Nguyen, T.V.A.; Ogden, J. Understanding HIV and AIDS-Related Stigma and Discrimination in Vietnam; International Center for Research on Women (ICRW): Washington, DC, USA, 2004. [Google Scholar]
- Pham, H.N.; Protsiv, M.; Larsson, M.; Ho, H.T.; De Vries, D.H.; Thorson, A. Stigma, an important source of dissatisfaction of health workers in HIV response in Vietnam: A qualitative study. BMC Health Serv. Res. 2012, 12, 474. [Google Scholar] [CrossRef]
- Colby, D.; Nguyen, N.A.; Le, B.; Toan, T.; Thien, D.D.; Huyen, H.T.; Mai, T.D.A.; Friedman, M.R.; Stall, R. HIV and syphilis prevalence among transgender women in Ho Chi Minh City, Vietnam. AIDS Behav. 2016, 20, 379–385. [Google Scholar] [CrossRef]
- Do, T.T.; Nguyen, T.V.A.; Vu, X.T.; Nguyen, T.P.T. Seeking healthcare as a transgender woman in contemporary Vietnam: Access barriers and the situation of hormone use. Reg. J. Southeast Asian Stud. 2018, 3, 30–58. [Google Scholar]
- Vu, N.T.T.; Holt, M.; Phan, H.T.T.; La, L.T.; Tran, G.M.; Doan, T.T.; Nguyen, T.N.N.; de Wit, J. The relationship between methamphetamine use, sexual sensation seeking and condomless anal intercourse among men who have sex with men in Vietnam: Results of a community-based, cross-sectional study. AIDS Behav. 2017, 21, 1105–1116. [Google Scholar]
- Ha, H.; Risser, J.M.; Ross, M.W.; Huynh, N.T.; Nguyen, H.T. Homosexuality-related stigma and sexual risk behaviors among men who have sex with men in Hanoi, Vietnam. Arch. Sex. Behav. 2015, 44, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Clatts, M.C.; Goldsamt, L.A.; Yu, G. Sexual practices, partner concurrency and high rates of sexually transmissible infections among male sex workers in three cities in Vietnam. Sex. Health 2015, 12, 39–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biello, K.B.; Colby, D.; Closson, E.; Mimiaga, M. The syndemic condition of psychosocial problems and HIV risk among male sex workers in Ho Chi Minh City, Vietnam. AIDS Behav. 2014, 18, 1264–1271. [Google Scholar] [CrossRef] [PubMed]
- Yu, G.; Clatts, M.C.; Goldsamt, L.A.; Giang, L.M. Substance use among male sex workers in Vietnam: Prevalence, onset, and interactions with sexual risk. Int. J. Drug Policy 2015, 26, 516–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vietnam Authority of HIV/AIDS Control. An Annual Update on HIV Epidemic in Vietnam; Vietnam Authority of HIV/AIDS Control: Hanoi, Vietnam, 2014. [Google Scholar]
- Goldsamt, L.A.; Clatts, M.C.; Giang, L.M.; Yu, G. Prevalence and behavioral correlates of depression and anxiety among male sex workers in Vietnam. Int. J. Sex. Health 2015, 27, 145–155. [Google Scholar] [PubMed]
- Lim, F.A.; Brown, D.V., Jr.; Kim, S.M.J. CE: Addressing health care disparities in the lesbian, gay, bisexual, and transgender population: A review of best practices. AJN Am. J. Nurs. 2014, 114, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Pham, N.H. Human Resources and the Response to HIV in Vietnam: Policies and Health Workers’ Perspectives; Karolinska Institutet: Stockholm, Sweden, 2013. [Google Scholar]
- Quach, L.; Mayer, K.; McGarvey, S.T.; Lurie, M.N.; Do, P. Knowledge, attitudes, and practices among physicians on HIV/AIDS in Quang Ninh, Vietnam. AIDS Patient Care STDs 2005, 19, 335–346. [Google Scholar] [CrossRef]
- Platten, M.; Pham, H.N.; Nguyen, H.V. Knowledge of HIV and factors associated with attitudes towards HIV among final-year medical students at Hanoi medical university in Vietnam. BMC Public Health 2014, 14, 265. [Google Scholar] [CrossRef]
- Thi, M.D.A.; Brickley, D.B.; Vinh, D.T.N.; Colby, D.J.; Sohn, A.H.; Trung, N.Q.; Mandel, J.S. A qualitative study of stigma and discrimination against people living with HIV in Ho Chi Minh City, Vietnam. AIDS Behav. 2008, 12, 63–70. [Google Scholar] [CrossRef]
- Khuat, T.H.; Do, T.T.; Nguyen, V.A.; Vu, X.T.; Nguyen, P.T.; Tran, K.; Ho, M.T.; T Nguyen, H.K.; Vuong, T.; La, V.P. The dark side of female HIV patient care: Sexual and reproductive health risks in pre-and post-clinical treatments. J. Clin. Med. 2018, 7, 402. [Google Scholar] [CrossRef]
- Cahill, S.; Makadon, H. Sexual orientation and gender identity data collection in clinical settings and in electronic health records: A key to ending LGBT health disparities. LGBT Health 2014, 1, 34–41. [Google Scholar]
- Vuong, Q.-H. The (ir)rational consideration of the cost of science in transition economies. Nat. Hum. Behav. 2018, 2, 5. [Google Scholar] [CrossRef]
- Cheong, K.-C.; Duoc, L.S. Right Time, Right Place: The Role of Context in the Making of a Successful Project in Vietnam. Inst. Econ. 2017, 9, 1–20. [Google Scholar]
- Aidsfonds. PITCH LGBT Vietnam, SCDI. Available online: https://aidsfonds.org/work/pitch-lgbt-vietnam-scdi (accessed on 8 November 2018).
- Vuong, Q.-H.; Ho, T.-M.; Nguyen, H.-K.; Vuong, T.-T. Healthcare consumers’ sensitivity to costs: A reflection on behavioural economics from an emerging market. Palgrave Commun. 2018, 4, 70. [Google Scholar]
- Lee, H.-C.; Yoon, S.; Yang, S.-M.; Kim, W.; Ryu, H.-G.; Jung, C.-W.; Suh, K.-S.; Lee, K. Prediction of Acute Kidney Injury after Liver Transplantation: Machine Learning Approaches vs. Logistic Regression Model. J. Clin. Med. 2018, 7, 428. [Google Scholar]
- Vuong, Q.; Vu, Q.H. Learning healthcare needs when the body speaks: Insights from a 2016 Vietnamese survey on general physical examinations. Indian J. Community Health 2017, 29, 101–107. [Google Scholar]
- Le, T.M.; Yu, N. Ideological and Philosophical Underpinnings of Attitudes Toward Sexual Minorities in Vietnamese Society. Sex. Cult. 2018, 1–14. [Google Scholar] [CrossRef]
- Vuong, Q.; La, V.; Vuong, T.; Nguyen, V.; Ho, M.; Nguyen, T.; Bui, Q.; Ho, M. Cultural additivity: Behavioural insights from the interaction of Confucianism, Buddhism, and Taoism in folktales. Palgrave Commun. 2018, 4. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Percentage (%) | |
|---|---|
| Sex | |
| Male | 28.0 |
| Female | 72.0 |
| Age | |
| <30 | 38.3 |
| 30–45 | 47.0 |
| >45 | 14.8 |
| Education | |
| University and above | 50.7 |
| College/vocational college or lower | 49.3 |
| Medical facilities | |
| Public hospitals | 38.7 |
| Dermatology hospitals | 41.3 |
| Andrology clinics and private clinics | 20.0 |
| Work positions | |
| Management/leadership | 12.0 |
| Specialist | 64.0 |
| Administrative | 24.0 |
| Years of experience | |
| <5 years | 39.6 |
| 5–10 years | 26.2 |
| >10 years | 34.2 |
| Total | 100 |
| Number | |
|---|---|
| Sex | |
| Male | 6 |
| Female | 6 |
| Medical facilities | |
| General hospitals | 4 |
| Dermatology hospitals | 4 |
| Andrology clinics and private clinics | 4 |
| Work positions | |
| Management/leadership | 4 |
| Specialist | 8 |
| Years of experience | |
| <5 years | 1 |
| 5–10 years | 3 |
| >10 years | 8 |
| Total | 12 |
| Statements | Percentage (%) | |
|---|---|---|
| 1 | MSM are males who only have sex with males | 45.6 |
| 2 | MSM can have sex with both males and females | 74.8 |
| 3 | MSM are those with sex hormone disorder | 51.0 |
| 4 | MSM are those with curable mental problem | 17.0 |
| 5 | MSM are those with effeminate behaviors that are not suitable for their sex | 28.6 |
| 6 | MSM are androgynous | 31.3 |
| 7 | MSM have typical male genitalia | 81.6 |
| 8 | MSM may have typical female genitalia | 19.1 |
| 9 | MSM may not have any genitalia characteristics of either sex | 29.9 |
| Incorrect Statements | General Hospitals | Dermatology Hospitals | Andrology Clinics and Private Clinics | |||
|---|---|---|---|---|---|---|
| Hanoi | HCMC | Hanoi | HCMC | Hanoi | HCMC | |
| MSM are those with sex hormone disorders | 60.0 | 60.0 | 65.6 | 30.0 | 69.2 | 56.3 |
| MSM are those with a curable mental problem | 10.0 | 10.0 | 18.8 | 6.7 | 30.8 | 6.3 |
| MSM are those with effeminate behaviors that are not suitable for their sex | 30.0 | 30.0 | 43.8 | 6.7 | 53.9 | 12.5 |
| MSM are androgynous | 33.3 | 33.3 | 53.1 | 3.3 | 61.5 | 31.3 |
| Statements | Percentage (%) | |
|---|---|---|
| 1 | Female transgenders are those who were born as males but feel and express themselves as females | 85.8 |
| 2 | Male transgenders are those who were born as females but feel and express themselves as males | 81.1 |
| 3 | Female transgenders are those who were born as male but use medical intervention to have a female body | 82.4 |
| 4 | Male transgenders are those who were born as male but use medical intervention to have a male body | 74.3 |
| 5 | Transgenders have a curable mental problem | 2.0 |
| 6 | Transgender are those with sex hormone disorder | 50.0 |
| 7 | Transgenders may have typical male genitalia | 68.9 |
| 8 | Transgenders may have typical female genitalia | 72.3 |
| 9 | Transgenders may have genitalia atypical of both sexes | 34.5 |
| 10 | Transgenders may not want to alter their body but want to be acknowledged as members of the sex different from their innate sex | 62.8 |
| 11 | A male transgender may have sex with both males and females | 74.3 |
| 12 | A female transgender may have sex with both males and females | 75.7 |
| Incorrect Statements | General Hospitals | Dermatology Hospitals | Andrology Clinics and Private Clinics | |||
|---|---|---|---|---|---|---|
| Hanoi | HCMC | Hanoi | HCMC | Hanoi | HCMC | |
| Transgenders are those with a curable mental problem | 3.3 | 0.0 | 0.0 | 0.0 | 15.4 | 0.0 |
| Transgenders are those with sex hormone disorders | 63.3 | 38.5 | 46.9 | 40.0 | 69.2 | 52.9 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, V.A.T.; Nguyen, N.Q.H.; Khuat, T.H.; Nguyen, P.T.T.; Do, T.T.; Vu, X.T.; Tran, K.; Ho, M.T.; Nguyen, H.K.T.; Vuong, T.T.; et al. Righting the Misperceptions of Men Having Sex with Men: A Pre-Requisite for Protecting and Understanding Gender Incongruence in Vietnam. J. Clin. Med. 2019, 8, 105. https://doi.org/10.3390/jcm8010105
Nguyen VAT, Nguyen NQH, Khuat TH, Nguyen PTT, Do TT, Vu XT, Tran K, Ho MT, Nguyen HKT, Vuong TT, et al. Righting the Misperceptions of Men Having Sex with Men: A Pre-Requisite for Protecting and Understanding Gender Incongruence in Vietnam. Journal of Clinical Medicine. 2019; 8(1):105. https://doi.org/10.3390/jcm8010105
Chicago/Turabian StyleNguyen, Van Anh T., Ngoc Quynh H. Nguyen, Thu Hong Khuat, Phuong Thao T. Nguyen, Thu Trang Do, Xuan Thai Vu, Kien Tran, Manh Tung Ho, Hong Kong T. Nguyen, Thu Trang Vuong, and et al. 2019. "Righting the Misperceptions of Men Having Sex with Men: A Pre-Requisite for Protecting and Understanding Gender Incongruence in Vietnam" Journal of Clinical Medicine 8, no. 1: 105. https://doi.org/10.3390/jcm8010105