Dose-Response Relationship between Exercise Duration and Executive Function in Older Adults

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Task Switching Paradigm
2.3. Cardiorespiratory Fitness Assessment
2.4. Exercise Intensity Manipulation Check
2.5. Procedure
2.6. Statistical Analysis
3. Results
3.1. Exercise Intensity Manipulation Check
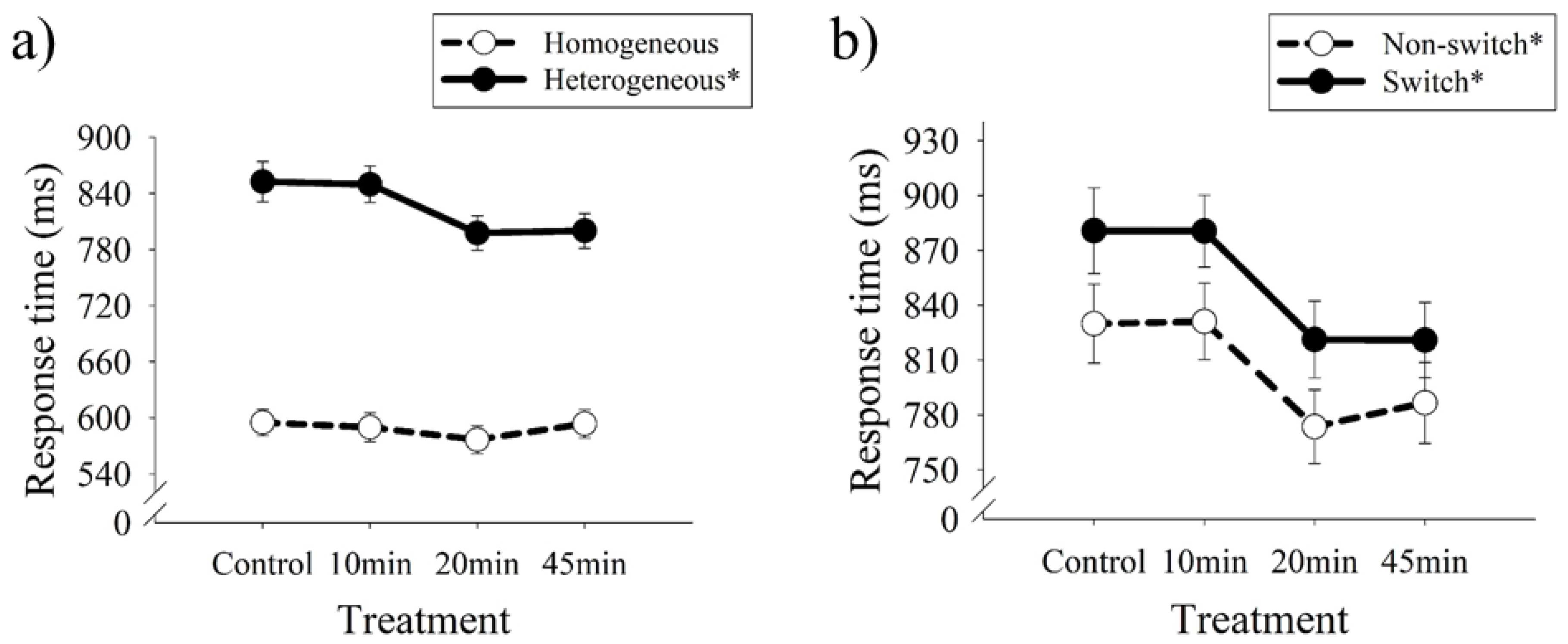
3.2. Task Switching
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Paradise, M.; McCade, D.; Hickie, I.B.; Diamond, K.; Lewis, S.J.G.; Naismith, S.L. Caregiver burden in mild cognitive impairment. Aging Ment. Health 2015, 19, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Wolff, H.G. Societies can both grow old and lower dementia burden. J. Sport Exerc. Psychol. 2015, 14, 967–1064. [Google Scholar]
- Etnier, J.L.; Chang, Y.K. The effect of physical activity on executive function: A brief commentary on definitions, measurement issues, and the current state of the literature. J. Sport Exerc. Psychol. 2009, 31, 469–483. [Google Scholar] [CrossRef] [PubMed]
- Marshall, G.A.; Rentz, D.M.; Frey, M.T.; Locascio, J.J.; Johnson, K.A.; Sperling, R.A.; ADNI. Executive function and instrumental activities of daily living in mild cognitive impairment and alzheimer’s disease. Alzheimers Dement. 2011, 7, 300–308. [Google Scholar] [CrossRef] [PubMed]
- McGuinness, B.; Barrett, S.L.; Craig, D.; Lawson, J.; Passmore, A.P. Executive functioning in alzheimer’s disease and vascular dementia. Int. J. Geriatr. Psychiatry 2010, 25, 562–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, P.; Raz, N. Prefrontal cortex and executive functions in healthy adults: A meta-analysis of structural neuroimaging studies. Neurosci. Biobehav. Rev. 2014, 42, 180–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raz, N.; Ghisletta, P.; Rodrigue, K.M.; Kennedy, K.M.; Lindenberger, U. Trajectories of brain aging in middle-aged and older adults: Regional and individual differences. Neuroimage 2010, 51, 501–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reuter-Lorenz, P.A.; Park, D.C. Human neuroscience and the aging mind: A new look at old problems. J. Gerontol. Ser. B 2010, 65B, 405–415. [Google Scholar] [CrossRef] [PubMed]
- Prakash, R.S.; Voss, M.W.; Erickson, K.I.; Kramer, A.F. Physical activity and cognitive vitality. Annu. Rev. Psychol. 2015, 769–797. [Google Scholar] [CrossRef] [PubMed]
- Scherder, E.; Scherder, R.; Verburgh, L.; Konigs, M.; Blom, M.; Kramer, A.F.; Eggermont, L. Executive functions of sedentary elderly may benefit from walking: A systematic review and meta-analysis. Am. J. Geriatr. Psychiatry 2014, 22, 782–791. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Iwamoto, K.; Kawano, N.; Noda, Y.; Ozaki, N.; Noda, A. Differential effects of physical activity and sleep duration on cognitive function in young adults. J. Sport Health Sci. 2017, 7, 227–236. [Google Scholar] [CrossRef]
- Chang, C.H.; Chu, C.H.; Karageorghis, C.I.; Wang, C.C.; Tsai, H.C.; Wang, Y.S.; Chang, Y.K. Relationship between mode of sport training and general cognitive performance. J. Sport Health Sci. 2017, 6, 89–95. [Google Scholar] [CrossRef]
- Lambourne, K.; Tomporowski, P.D. The effect of exercise-induced arousal on cognitive task performance: A meta-regression analysis. Brain Res. 2010, 1341, 12–24. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.K.; Ku, P.W.; Tomporowski, P.D.; Chen, F.T.; Huang, C.C. Effects of acute resistance exercise on late-middle-aged adults’ goal planning. Med. Sci. Sports Exerc. 2012, 44, 1773–1779. [Google Scholar] [CrossRef] [PubMed]
- Razon, S.; Lebeau, J.; Basevitch, I.; Foster, B.; Akpan, A.; Mason, J.; Boiangin, N.; Tenenbaum, G. Effects of acute exercise on executive functioning: Testing the moderators. Int. J. Sport Exerc. Psychol. 2017, 1–18. [Google Scholar] [CrossRef]
- Hsieh, S.S.; Chang, Y.K.; Fang, C.L.; Hung, T.M. Acute resistance exercise facilitates attention control in adult males without an age-moderating effect. Int. J. Sport Exerc. Psychol. 2016, 38, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Pesce, C.; Audiffren, M. Does acute exercise switch off switch costs? A study with younger and older athletes. Int. J. Sport Exerc. Psychol. 2011, 33, 609–626. [Google Scholar] [CrossRef]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: A latent variable analysis. Cogn. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.K.; Chu, C.H.; Wang, C.C.; Song, T.F.; Wei, G.X. Effect of acute exercise and cardiovascular fitness on cognitive function: An event-related cortical desynchronization study. Psychophysiology 2015, 52, 342–351. [Google Scholar] [CrossRef] [PubMed]
- Kamijo, K.; Hayashi, Y.; Sakai, T.; Yahiro, T.; Tanaka, K.; Nishihira, Y. Acute effects of aerobic exercise on cognitive function in older adults. J. Gerontol. Ser. B 2009, 64, 356–363. [Google Scholar] [CrossRef] [PubMed]
- McMorris, T.; Sproule, J.; Turner, A.; Hale, B.J. Acute, intermediate intensity exercise, and speed and accuracy in working memory tasks: A meta-analytical comparison of effects. Physiol. Behav. 2011, 102, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Weng, T.B.; Pierce, G.L.; Darling, W.G.; Voss, M.W. Differential effects of acute exercise on distinct aspects of executive function. Med. Sci. Sports Exerc. 2015, 47, 1460–1469. [Google Scholar] [CrossRef] [PubMed]
- Lawo, V.; Koch, I. Examining age-related differences in auditory attention control using a task-switching procedure. J. Gerontol. Ser. B 2014, 69, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Hakun, J.G.; Johnson, N.F.; Gold, B.T. Age-related increases in right frontal activation during task switching are mediated by reaction time and white matter microstructure. Neuroscience 2014, 278, 51–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monsell, S. Task switching. Trends Cogn. Sci. 2003, 7, 134–140. [Google Scholar] [CrossRef]
- Zheng, D.; Sun, H.; Dong, X.; Liu, B.; Xu, Y.; Chen, S.; Song, L.; Zhang, H.; Wang, X. Executive dysfunction and gray matter atrophy in amnestic mild cognitive impairment. Neurobiol. Aging 2014, 35, 548–555. [Google Scholar] [CrossRef] [PubMed]
- Yanagisawa, H.; Dan, I.; Tsuzuki, D.; Kato, M.; Okamoto, M.; Kyutoku, Y.; Soya, H. Acute moderate exercise elicits increased dorsolateral prefrontal activation and improves cognitive performance with stroop test. Neuroimage 2010, 50, 1702–1710. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, P.D.; Kane, C.J. Exercise and cognitive function: A randomized controlled trial examining acute exercise and free-living physical activity and sedentary effects. Mayo Clin. Proc. 2015, 90, 450–460. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 9th ed.; Lippincott Williams and Wilkins: New York, NY, USA, 2014. [Google Scholar]
- McMorris, T.; Hale, B.J. Differential effects of differing intensities of acute exercise on speed and accuracy of cognition: A meta-analytical investigation. Brain Cogn. 2012, 80, 338–351. [Google Scholar] [CrossRef] [PubMed]
- Yerkes, R.M.; Dodson, J.D. The relation of strength of stimulus to rapidity of habit formation. J. Comp. Neurol. 1908, 18, 459–482. [Google Scholar] [CrossRef]
- Chang, Y.K.; Chu, C.H.; Wang, C.C.; Wang, Y.C.; Song, T.F.; Tsai, C.L.; Etnier, J.L. Dose-response relation between exercise duration and cognition. Med. Sci. Sports Exerc. 2015, 47, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Liou, Y.M.; Jwo, C.J.C.; Yao, K.G.; Chiang, L.C.; Huang, L.H. Selection of appropriate chinese terms to represent intensity and types of physical activity terms for use in the taiwan version of ipaq. J. Nurs. Res. 2008, 16, 252–263. [Google Scholar] [CrossRef] [PubMed]
- Dai, C.T.; Chang, Y.K.; Huang, C.J.; Hung, T.M. Exercise mode and executive function in older adults: An erp study of task-switching. Brain Cogn. 2013, 83, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Franks, B.D. YMCA Fitness Testing and Assessment Manual; Human Kinetics: Champaign, IL, USA, 1989. [Google Scholar]
- Song, T.F.; Chen, F.T.; Chu, C.H.; Chi, L.; Liu, S.; Chang, Y.K. Obesity and cardiovascular fitness associated with inhibition of executive function: An erp study. Phys. Educ. J. 2017, 50, 43–56. [Google Scholar]
- Fletcher, G.F.; Balady, G.J.; Amsterdam, E.A.; Chaitman, B.; Eckel, R.; Fleg, J.; Froelicher, V.F.; Leon, A.S.; Piña, I.L.; Rodney, R. Exercise standards for testing and training a statement for healthcare professionals from the american heart association. Circulation 2001, 104, 1694–1740. [Google Scholar] [CrossRef] [PubMed]
- Borg, G.A. Borg’s Perceived Exertion and Pain Scales; Human Kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- Tomporowski, P.D. Effects of acute bouts of exercise on cognition. Acta Psychol. 2003, 112, 297–324. [Google Scholar] [CrossRef]
- Derrfuss, J.; Brass, M.; Neumann, J.; von Cramon, D.Y. Involvement of the inferior frontal junction in cognitive control: Meta-analyses of switching and stroop studies. Hum. Brain Map. 2005, 25, 22–34. [Google Scholar] [CrossRef] [PubMed]
- McNab, F.; Klingberg, T. Prefrontal cortex and basal ganglia control access to working memory. Nat. Neurosci. 2008, 11, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.K.; Tsai, C.L.; Huang, C.C.; Wang, C.C.; Chu, I.H. Effects of acute resistance exercise on cognition in late middle-aged adults: General or specific cognitive improvement? J. Sci. Med. Sport 2014, 17, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Kamijo, K.; Nishihira, Y.; Higashiura, T.; Kuroiwa, K. The interactive effect of exercise intensity and task difficulty on human cognitive processing. Int. Organ. Psychophysiol. 2007, 65, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Hillman, C.H.; Snook, E.M.; Jerome, G.J. Acute cardiovascular exercise and executive control function. Int. J. Psychophysiol. 2003, 48, 307–314. [Google Scholar] [CrossRef]
- Polich, J. Updating p300: An integrative theory of p3a and p3b. Clin. Neurophysiol. 2007, 118, 2128–2148. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Men, W.W.; Chang, Y.K.; Fan, M.X.; Li, L.; Wei, G.X. Acute aerobic exercise increases cortical activity during working memory: A functional mri study in female college students. PLoS ONE 2014, 9, e99222. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Total |
|---|---|
| n | 45 |
| Female/Male (% Male) | 26/19 (42%) |
| Age (Year) | 57.67 ± 5.06 |
| Height (cm) | 163.04 ± 8.38 |
| Weight (kg) | 64.38 ± 13.09 |
| Body mass index (kg m−2) | 23.86 ± 3.74 |
| Education (year) | 14.11 ± 2.50 |
| MMSE (Total score) | 28.47 ± 1.79 |
| Digit span (score) Forward Backward | 15.29 ± 2.51 5.07 ± 2.09 |
| Resting heart rate (bpm) | 71.26 ± 8.84 |
| IPAQ (METs wk−1) | 1104.67 ± 1443.75 |
| VO2peak (mL kg−1 min−1) | 37.52 ± 9.92 |
| Variable | Session | |||
|---|---|---|---|---|
| Control | 10 min | 20 min | 45 min | |
| Response time | ||||
| Global switching (ms) | ||||
| Heterogeneous | 852.55 ± 144.21 | 849.72 ± 130.55 | 797.66 ± 124.16 | 800.10 ± 125.26 |
| Homogeneous | 594.96 ± 95.68 | 589.78 ± 103.47 | 576.46 ± 100.25 | 593.57 ± 100.86 |
| Local switching (ms) | ||||
| Switch | 880.74 ± 157.02 | 880.53 ± 132.17 | 821.28 ± 141.21 | 820.93 ± 138.35 |
| Non-switch | 829. 95± 144.83 | 831.14 ± 140.22 | 773.61 ± 134.42 | 786.61 ± 148.03 |
| Accuracy | ||||
| Global switching (%) | ||||
| Heterogeneous | 94.01 ± 7.43 | 94.55 ± 7.47 | 93.55 ± 8.07 | 94.27 ± 9.42 |
| Homogeneous | 96.67 ± 5.60 | 96.49 ± 7.67 | 96.22 ± 5.63 | 95.76 ± 8.34 |
| Local switching (%) | ||||
| Switch | 94.23 ± 7.41 | 94.88 ± 8.50 | 93.83 ± 8.52 | 94.04 ± 9.68 |
| Non-switch | 94.69 ± 7.00 | 94.96 ± 8.46 | 94.32 ± 8.24 | 94.73 ± 9.59 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, F.-T.; Etnier, J.L.; Wu, C.-H.; Cho, Y.-M.; Hung, T.-M.; Chang, Y.-K. Dose-Response Relationship between Exercise Duration and Executive Function in Older Adults. J. Clin. Med. 2018, 7, 279. https://doi.org/10.3390/jcm7090279
Chen F-T, Etnier JL, Wu C-H, Cho Y-M, Hung T-M, Chang Y-K. Dose-Response Relationship between Exercise Duration and Executive Function in Older Adults. Journal of Clinical Medicine. 2018; 7(9):279. https://doi.org/10.3390/jcm7090279
Chicago/Turabian StyleChen, Feng-Tzu, Jennifer L. Etnier, Chih-Han Wu, Yu-Min Cho, Tsung-Min Hung, and Yu-Kai Chang. 2018. "Dose-Response Relationship between Exercise Duration and Executive Function in Older Adults" Journal of Clinical Medicine 7, no. 9: 279. https://doi.org/10.3390/jcm7090279