The Importance of Time to Prostate-Specific Antigen (PSA) Nadir after Primary Androgen Deprivation Therapy in Hormone-Naïve Prostate Cancer Patients


Abstract
:1. Introduction
2. Prostate-Specific Antigen (PSA)
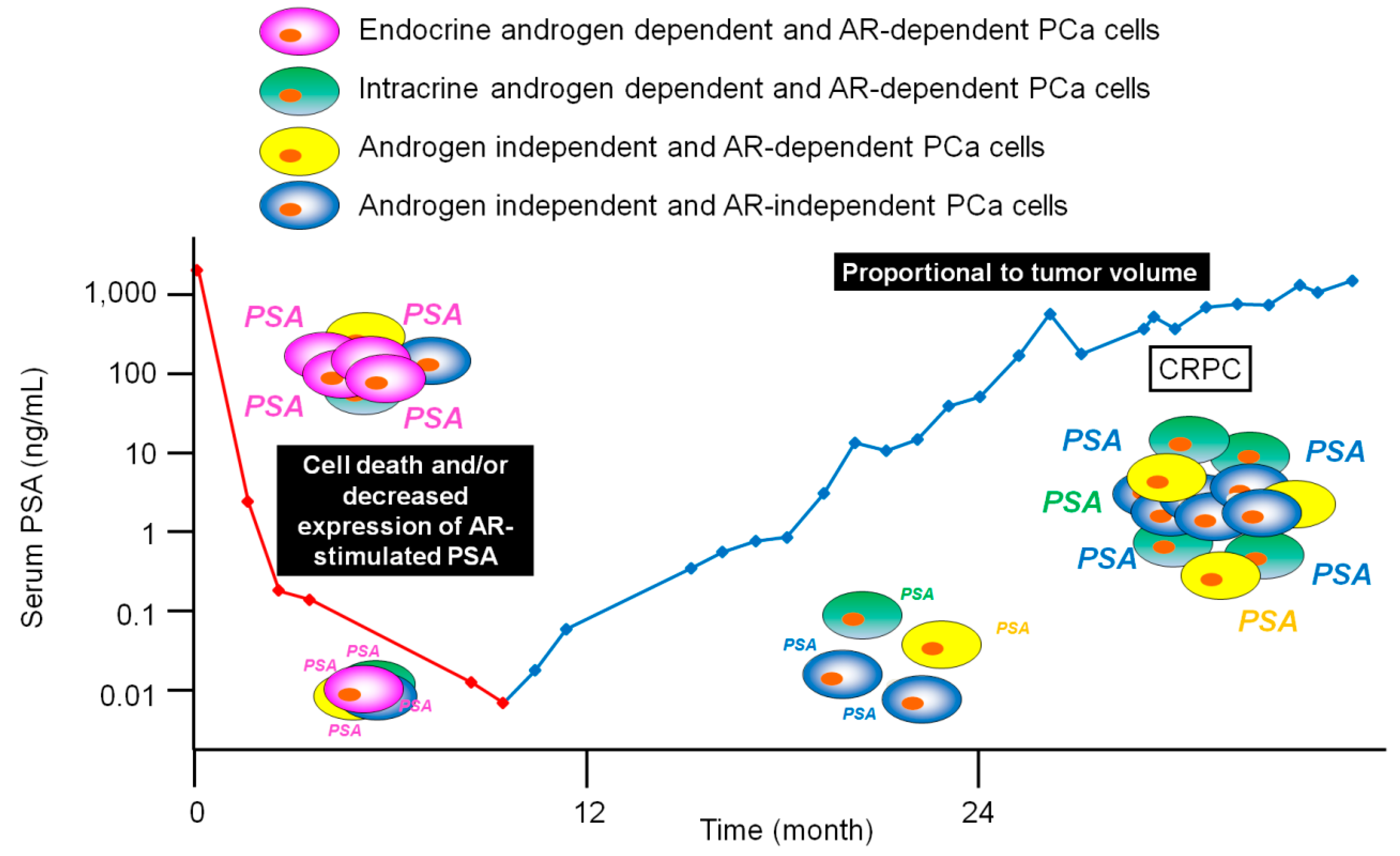
3. PSA Expression after Androgen Deprivation Therapy (ADT)
4. Time to PSA Nadir (TTN) after Primary ADT
5. Biological Mechanism of TTN after ADT
6. Concluding Remarks
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- De Voogt, H.J.; Suciu, S.; Sylvester, R.; Pavone-Macaluso, M.; Smith, P.H.; de Pauw, M. Multivariate analysis of prognostic factors in patients with advanced prostatic cancer: Results from 2 european organization for research on treatment of cancer trials. J. Urol. 1989, 141, 883–888. [Google Scholar] [CrossRef]
- Ishikawa, S.; Soloway, M.S.; Van der Zwaag, R.; Todd, B. Prognostic factors in survival free of progression after androgen deprivation therapy for treatment of prostate cancer. J. Urol. 1989, 141, 1139–1142. [Google Scholar] [CrossRef]
- Cooperberg, M.R.; Hinotsu, S.; Namiki, M.; Ito, K.; Broering, J.; Carroll, P.R.; Akaza, H. Risk assessment among prostate cancer patients receiving primary androgen deprivation therapy. J. Clin. Oncol. 2009, 27, 4306–4313. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, J.; Thompson, I.M. Prostate-specific antigen: A review of the validation of the most commonly used cancer biomarker. Cancer 2004, 101, 894–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki, T.; Onishi, T.; Hoshina, A. Nadir PSA level and time to PSA nadir following primary androgen deprivation therapy are the early survival predictors for prostate cancer patients with bone metastasis. Prostate Cancer Prostatic Dis. 2011, 14, 248–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki, T.; Onishi, T.; Hoshina, A. Cutoff value of time to prostate-specific antigen nadir is inversely correlated with disease progression in advanced prostate cancer. Endocr. Relat. Cancer 2012, 19, 725–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki, T.; Ishii, K.; Iwamoto, Y.; Kato, M.; Miki, M.; Kanda, H.; Arima, K.; Shiraishi, T.; Sugimura, Y. Fibroblasts prolong serum prostate-specific antigen decline after androgen deprivation therapy in prostate cancer. Lab. Invest. 2016, 96, 338–349. [Google Scholar] [CrossRef] [PubMed]
- Yousef, G.M.; Diamandis, E.P. The new human tissue kallikrein gene family: Structure, function, and association to disease. Endocr. Rev. 2001, 22, 184–204. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, T.; Franco, O.E.; Hayward, S.W. Male reproductive tract: Prostate overview. In Encyclopedia of Reproduction, 2nd ed.; Skinner, M., Ed.; Elsevier: Cambridge, MA, USA, 2018; Volume 1, pp. 309–314. ISBN 9780128012383. [Google Scholar]
- Balk, S.P.; Ko, Y.J.; Bubley, G.J. Biology of prostate-specific antigen. J. Clin. Oncol. 2003, 21, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Young, C.Y.; Montgomery, B.T.; Andrews, P.E.; Qui, S.D.; Bilhartz, D.L.; Tindall, D.J. Hormonal regulation of prostate-specific antigen messenger RNA in human prostatic adenocarcinoma cell line lncap. Cancer Res. 1991, 51, 3748–3752. [Google Scholar] [PubMed]
- Riegman, P.H.; Vlietstra, R.J.; van der Korput, J.A.; Brinkmann, A.O.; Trapman, J. The promoter of the prostate-specific antigen gene contains a functional androgen responsive element. Mol. Endocrinol. 1991, 5, 1921–1930. [Google Scholar] [CrossRef] [PubMed]
- Schuur, E.R.; Henderson, G.A.; Kmetec, L.A.; Miller, J.D.; Lamparski, H.G.; Henderson, D.R. Prostate-specific antigen expression is regulated by an upstream enhancer. J. Biol. Chem. 1996, 271, 7043–7051. [Google Scholar] [CrossRef] [PubMed]
- Cleutjens, K.B.; van der Korput, H.A.; van Eekelen, C.C.; van Rooij, H.C.; Faber, P.W.; Trapman, J. An androgen response element in a far upstream enhancer region is essential for high, androgen-regulated activity of the prostate-specific antigen promoter. Mol. Endocrinol. 1997, 11, 148–161. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Murtha, P.E.; Young, C.Y. Defining a functional androgen responsive element in the 5’ far upstream flanking region of the prostate-specific antigen gene. Biochem. Biophys. Res. Commun. 1997, 231, 784–788. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Shostak, Y.; Tarr, P.; Sawyers, C.; Carey, M. Cooperative assembly of androgen receptor into a nucleoprotein complex that regulates the prostate-specific antigen enhancer. J. Biol. Chem. 1999, 274, 25756–25768. [Google Scholar] [CrossRef] [PubMed]
- Culig, Z.; Klocker, H.; Bartsch, G.; Hobisch, A. Androgen receptors in prostate cancer. Endocr. Relat. Cancer 2002, 9, 155–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nazareth, L.V.; Weigel, N.L. Activation of the human androgen receptor through a protein kinase a signaling pathway. J. Biol. Chem. 1996, 271, 19900–19907. [Google Scholar] [CrossRef] [PubMed]
- Sadar, M.D. Androgen-independent induction of prostate-specific antigen gene expression via cross-talk between the androgen receptor and protein kinase a signal transduction pathways. J. Biol. Chem. 1999, 274, 7777–7783. [Google Scholar] [CrossRef] [PubMed]
- Ikonen, T.; Palvimo, J.J.; Kallio, P.J.; Reinikainen, P.; Janne, O.A. Stimulation of androgen-regulated transactivation by modulators of protein phosphorylation. Endocrinology 1994, 135, 1359–1366. [Google Scholar] [CrossRef] [PubMed]
- Franco, O.E.; Onishi, T.; Yamakawa, K.; Arima, K.; Yanagawa, M.; Sugimura, Y.; Kawamura, J. Mitogen-activated protein kinase pathway is involved in androgen-independent PSA gene expression in lncap cells. Prostate 2003, 56, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Coetzee, G.A. Prostate specific antigen gene regulation by androgen receptor. J. Cell. Biochem. 2004, 93, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Mizokami, A.; Namiki, M. Reconsideration of progression to CRPC during androgen deprivation therapy. J. Steroid Biochem. Mol. Biol. 2015, 145, 164–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crawford, E.D.; Bennett, C.L.; Andriole, G.L.; Garnick, M.B.; Petrylak, D.P. The utility of prostate-specific antigen in the management of advanced prostate cancer. BJU Int. 2013, 112, 548–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwak, C.; Jeong, S.J.; Park, M.S.; Lee, E.; Lee, S.E. Prognostic significance of the nadir prostate specific antigen level after hormone therapy for prostate cancer. J. Urol. 2002, 168, 995–1000. [Google Scholar] [CrossRef]
- Arai, Y.; Yoshiki, T.; Yoshida, O. Prognostic significance of prostate specific antigen in endocrine treatment for prostatic cancer. J. Urol. 1990, 144, 1415–1419. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Xie, W.; D’Amico, A.V.; Ross, R.W.; Hu, J.C.; Pomerantz, M.; Regan, M.M.; Taplin, M.E.; Kantoff, P.W.; Sartor, O.; et al. Time to prostate-specific antigen nadir independently predicts overall survival in patients who have metastatic hormone-sensitive prostate cancer treated with androgen-deprivation therapy. Cancer 2009, 115, 981–987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitagawa, Y.; Ueno, S.; Izumi, K.; Mizokami, A.; Hinotsu, S.; Akaza, H.; Namiki, M. Nadir prostate-specific antigen (PSA) level and time to PSA nadir following primary androgen deprivation therapy as independent prognostic factors in a Japanese large-scale prospective cohort study (J-CaP). J. Cancer Res. Clin. Oncol. 2014, 140, 673–679. [Google Scholar] [CrossRef] [PubMed]
- Akbay, E.; Bozlu, M.; Cayan, S.; Kara, P.O.; Tek, M.; Aytekin, C. Prostate-specific antigen decline pattern in advanced prostate cancer receiving androgen deprivation therapy and relationship with prostate-specific antigen progression. Aging Male 2017, 20, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Morote, J.; Trilla, E.; Esquena, S.; Abascal, J.M.; Reventos, J. Nadir prostate-specific antigen best predicts the progression to androgen-independent prostate cancer. Int. J. Cancer 2004, 108, 877–881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hori, S.; Jabbar, T.; Kachroo, N.; Vasconcelos, J.C.; Robson, C.N.; Gnanapragasam, V.J. Outcomes and predictive factors for biochemical relapse following primary androgen deprivation therapy in men with bone scan negative prostate cancer. J. Cancer Res. Clin. Oncol. 2011, 137, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.P.; Bao, B.Y.; Wu, M.T.; Choueiri, T.K.; Goggins, W.B.; Huang, C.Y.; Pu, Y.S.; Yu, C.C.; Huang, C.H. Impact of prostate-specific antigen (PSA) nadir and time to PSA nadir on disease progression in prostate cancer treated with androgen-deprivation therapy. Prostate 2011, 71, 1189–1197. [Google Scholar] [CrossRef] [PubMed]
- Hussain, M.; Tangen, C.M.; Higano, C.; Schelhammer, P.F.; Faulkner, J.; Crawford, E.D.; Wilding, G.; Akdas, A.; Small, E.J.; Donnelly, B.; et al. Absolute prostate-specific antigen value after androgen deprivation is a strong independent predictor of survival in new metastatic prostate cancer: Data from southwest oncology group trial 9346 (INT-0162). J. Clin. Oncol. 2006, 24, 3984–3990. [Google Scholar] [CrossRef] [PubMed]
- Morote, J.; Esquena, S.; Abascal, J.M.; Trilla, E.; Cecchini, L.; Raventos, C.X.; Orsola, A.; Planas, J.; Catalan, R.; Reventos, J. Usefulness of prostate-specific antigen nadir as predictor of androgen-independent progression of metastatic prostate cancer. Int. J. Biol. Markers 2005, 20, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.P.; Bao, B.Y.; Wu, M.T.; Choueiri, T.K.; Goggins, W.B.; Liu, C.C.; Huang, C.Y.; Pu, Y.S.; Yu, C.C.; Wu, T.T.; et al. Significant associations of prostate-specific antigen nadir and time to prostate-specific antigen nadir with survival in prostate cancer patients treated with androgen-deprivation therapy. Aging Male 2012, 15, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.Y.; Cho, D.S.; Kim, S.I.; Ahn, H.S.; Kim, S.J. Prostate-specific antigen nadir and time to prostate-specific antigen nadir following maximal androgen blockade independently predict prognosis in patients with metastatic prostate cancer. Korean J. Urol. 2012, 53, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.M.; Jiang, H.W.; Tong, S.J.; Zhu, H.Q.; Liu, J.; Ding, Q. Prostate-specific antigen kinetics under androgen deprivation therapy and prostate cancer prognosis. Urol. Int. 2013, 91, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Tomioka, A.; Tanaka, N.; Yoshikawa, M.; Miyake, M.; Anai, S.; Chihara, Y.; Okajima, E.; Hirayama, A.; Hirao, Y.; Fujimoto, K. Nadir PSA level and time to nadir PSA are prognostic factors in patients with metastatic prostate cancer. BMC Urol. 2014, 14, 33. [Google Scholar] [CrossRef] [PubMed]
- Teoh, J.Y.; Tsu, J.H.; Yuen, S.K.; Chiu, P.K.; Chan, S.Y.; Wong, K.W.; Ho, K.L.; Hou, S.S.; Ng, C.F.; Yiu, M.K. Association of time to prostate-specific antigen nadir and logarithm of prostate-specific antigen velocity after progression in metastatic prostate cancer with prior primary androgen deprivation therapy. Asian J. Androl. 2017, 19, 98–102. [Google Scholar] [PubMed]
- Nelson, P.S. Molecular states underlying androgen receptor activation: A framework for therapeutics targeting androgen signaling in prostate cancer. J. Clin. Oncol. 2012, 30, 644–646. [Google Scholar] [CrossRef] [PubMed]
- So, A.; Gleave, M.; Hurtado-Col, A.; Nelson, C. Mechanisms of the development of androgen independence in prostate cancer. World J. Urol. 2005, 23, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Jennbacken, K.; Tesan, T.; Wang, W.; Gustavsson, H.; Damber, J.E.; Welen, K. N-cadherin increases after androgen deprivation and is associated with metastasis in prostate cancer. Endocr. Relat. Cancer 2010, 17, 469–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, M.L.; Kyprianou, N. Androgen receptor and growth factor signaling cross-talk in prostate cancer cells. Endocr. Relat. Cancer 2008, 15, 841–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki, T.; Franco, O.E.; Hayward, S.W. Interaction of prostate carcinoma-associated fibroblasts with human epithelial cell lines in vivo. Differentiation 2017, 96, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Kato, M.; Ishii, K.; Iwamoto, Y.; Sasaki, T.; Kanda, H.; Yamada, Y.; Arima, K.; Shiraishi, T.; Sugimura, Y. Activation of fgf2-fgfr signaling in the castrated mouse prostate stimulates the proliferation of basal epithelial cells. Biol. Reprod. 2013, 89, 81. [Google Scholar] [CrossRef] [PubMed]
- Gravina, G.L.; Mancini, A.; Ranieri, G.; Di Pasquale, B.; Marampon, F.; Di Clemente, L.; Ricevuto, E.; Festuccia, C. Phenotypic characterization of human prostatic stromal cells in primary cultures derived from human tissue samples. Int. J. Oncol. 2013, 42, 2116–2122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanner, M.J.; Welliver, R.C., Jr.; Chen, M.; Shtutman, M.; Godoy, A.; Smith, G.; Mian, B.M.; Buttyan, R. Effects of androgen receptor and androgen on gene expression in prostate stromal fibroblasts and paracrine signaling to prostate cancer cells. PLoS ONE 2011, 6, e16027. [Google Scholar] [CrossRef] [PubMed]
- Ishii, K.; Mizokami, A.; Tsunoda, T.; Iguchi, K.; Kato, M.; Hori, Y.; Arima, K.; Namiki, M.; Sugimura, Y. Heterogenous induction of carcinoma-associated fibroblast-like differentiation in normal human prostatic fibroblasts by co-culturing with prostate cancer cells. J. Cell. Biochem. 2011, 112, 3604–3611. [Google Scholar] [CrossRef] [PubMed]
- Ishii, K.; Imamura, T.; Iguchi, K.; Arase, S.; Yoshio, Y.; Arima, K.; Hirano, K.; Sugimura, Y. Evidence that androgen-independent stromal growth factor signals promote androgen-insensitive prostate cancer cell growth in vivo. Endocr. Relat. Cancer 2009, 16, 415–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halin, S.; Hammarsten, P.; Wikstrom, P.; Bergh, A. Androgen-insensitive prostate cancer cells transiently respond to castration treatment when growing in an androgen-dependent prostate environment. Prostate 2007, 67, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Olumi, A.F.; Grossfeld, G.D.; Hayward, S.W.; Carroll, P.R.; Tlsty, T.D.; Cunha, G.R. Carcinoma-associated fibroblasts direct tumor progression of initiated human prostatic epithelium. Cancer Res. 1999, 59, 5002–5011. [Google Scholar] [PubMed]
- Hayashi, N.; Cunha, G.R. Mesenchyme-induced changes in the neoplastic characteristics of the dunning prostatic adenocarcinoma. Cancer Res. 1991, 51, 4924–4930. [Google Scholar] [PubMed]
- Flaberg, E.; Markasz, L.; Petranyi, G.; Stuber, G.; Dicso, F.; Alchihabi, N.; Olah, E.; Csizy, I.; Jozsa, T.; Andren, O.; et al. High-throughput live-cell imaging reveals differential inhibition of tumor cell proliferation by human fibroblasts. Int. J. Cancer 2011, 128, 2793–2802. [Google Scholar] [CrossRef] [PubMed]
- Alkasalias, T.; Flaberg, E.; Kashuba, V.; Alexeyenko, A.; Pavlova, T.; Savchenko, A.; Szekely, L.; Klein, G.; Guven, H. Inhibition of tumor cell proliferation and motility by fibroblasts is both contact and soluble factor dependent. Proc. Natl. Acad. Sci. USA 2014, 111, 17188–17193. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Study | Patients (N) | Treatment | TTN Cutoff Threshold (Months) | Outcome |
|---|---|---|---|---|
| Morote et al. 2004 [30] | 283 (98 locally advanced, 185 metastatic) | Orchidectomy or maximal androgen blockade | 12 | Progression-free survival |
| Morote et al. 2005 [34] | 185 (metastatic) | Orchidectomy or LHRH agonist with antiandrogen | 9 | Progression-free survival |
| Choueiri et al. 2009 [27] | 179 (metastatic, 47.5% had prior RP or RT) | LHRH agonist or orchidectomy with or without antiandrogen | 6 | Overall survival |
| Hori et al. 2011 [31] | 155 (46 with bone metastasis, 109 without bone metastasis) | LHRH agonist or orchidectomy with or without antiandrogen | 24 (without bone metastasis) | Progression-free survival |
| Huang et al. 2011 [32] | 650 (advanced or metastatic, 35% had RP or RT) | LHRH agonist or orchidectomy with or without antiandrogen | 10 | Progression-free survival |
| Huang et al. 2011 [35] | 650 (advanced or metastatic, 35% had RP or RT) | LHRH agonist or orchidectomy with or without antiandrogen | 10 | Overall survival |
| Sasaki et al. 2011 [5] | 87 (with bone metastasis) | LHRH agonist or orchidectomy with antiandrogen | 9 | Overall survival |
| Sasaki et al. 2012 [6] | 184 (advanced, 101 with bone metastasis, 83 without bone metastasis) | LHRH agonist or orchidectomy with antiandrogen | 8 with bone metastasis, 11 without bone metastasis | Progression-free survival |
| Hong et al. 2012 [36] | 131 (metastatic) | LHRH agonist or orchidectomy with antiandrogen | 8 | Progression-free survival |
| Zhang et al. 2013 [37] | 332 (advanced or metastatic) | LHRH antagonist or orchidectomy with flutamide | 10 | Overall survival Progression-free survival |
| Kitagawa et al. 2014 [28] | 10,958 (all stage) | LHRH agonist or orchidectomy with or without antiandrogen | 9 | Overall survival Progression-free survival |
| Tomioka et al. 2014 [38] | 286 (metastatic) | LHRH agonist or orchidectomy with or without antiandrogen | <6, 6–12, ≥12 | Overall survival Progression-free survival |
| Teoh et al. 2017 [39] | 419 (metastatic) | LHRH agonist or orchidectomy | <3, 3–17, >17 | Overall survival Progression-free survival |
| Akbay et al. 2017 [29] | 97 (advanced) | LHRH agonist or orchidectomy with or without antiandrogen | 12 | Progression-free survival |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sasaki, T.; Sugimura, Y. The Importance of Time to Prostate-Specific Antigen (PSA) Nadir after Primary Androgen Deprivation Therapy in Hormone-Naïve Prostate Cancer Patients. J. Clin. Med. 2018, 7, 565. https://doi.org/10.3390/jcm7120565
Sasaki T, Sugimura Y. The Importance of Time to Prostate-Specific Antigen (PSA) Nadir after Primary Androgen Deprivation Therapy in Hormone-Naïve Prostate Cancer Patients. Journal of Clinical Medicine. 2018; 7(12):565. https://doi.org/10.3390/jcm7120565
Chicago/Turabian StyleSasaki, Takeshi, and Yoshiki Sugimura. 2018. "The Importance of Time to Prostate-Specific Antigen (PSA) Nadir after Primary Androgen Deprivation Therapy in Hormone-Naïve Prostate Cancer Patients" Journal of Clinical Medicine 7, no. 12: 565. https://doi.org/10.3390/jcm7120565