Elevated Serum Interleukin-8 Level Correlates with Cancer-Related Cachexia and Sarcopenia: An Indicator for Pancreatic Cancer Outcomes

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Clinical Parameters
2.2. Serum Sample Collection and Cytokine Detection Assays
2.3. Computed Tomography (CT) Image Analysis
2.4. Immunofluorescence Staining and Measurement
2.5. Statistical Analysis
3. Results
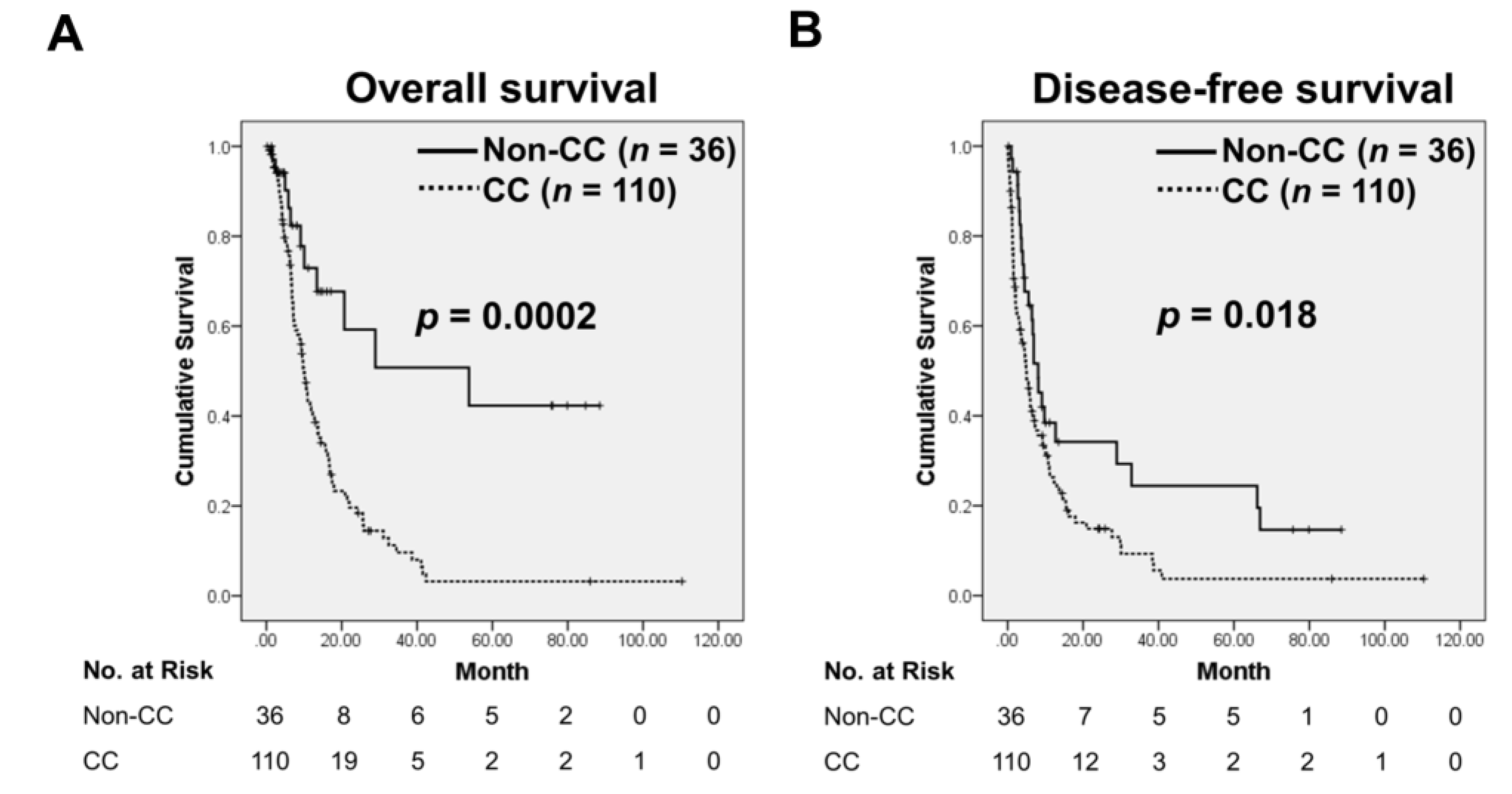
3.1. Cancer Cachexia (CC) Status Is Associated with Poor Clinical Outcome in Pancreatic Cancer (PC) Patients
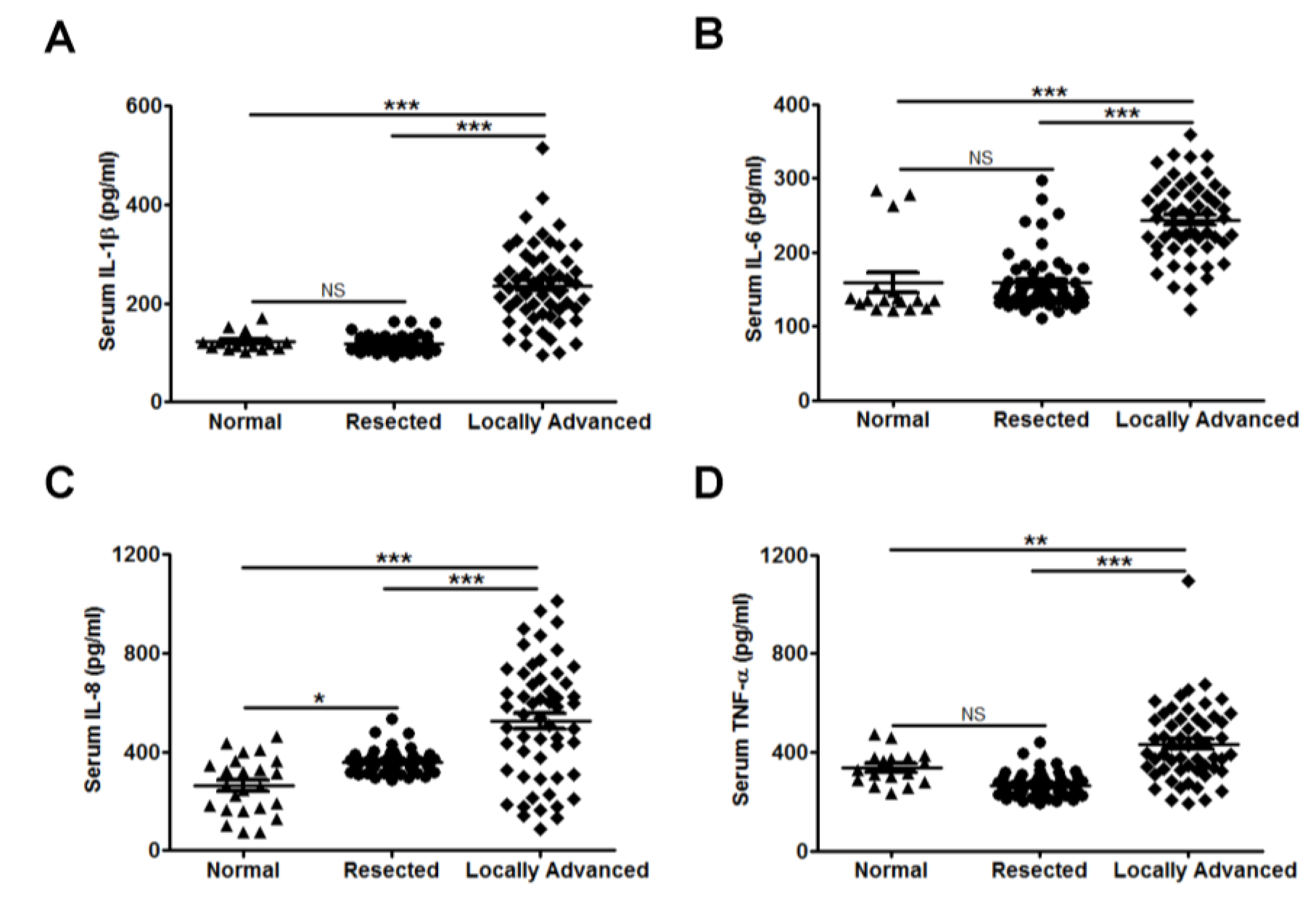
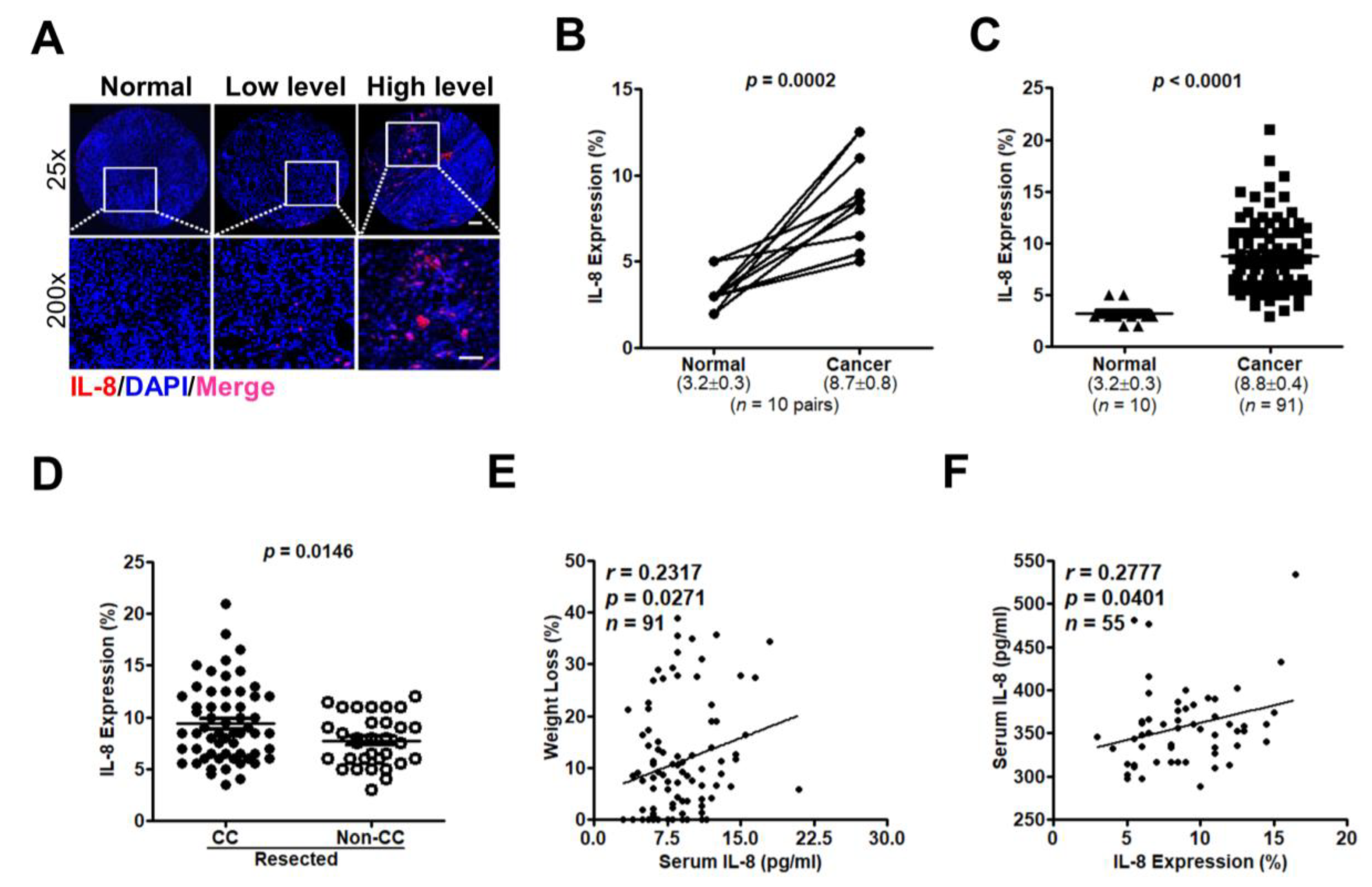
3.2. Interleukin (IL-8) Is an Applicable Diagnostic Indicator for CC Status
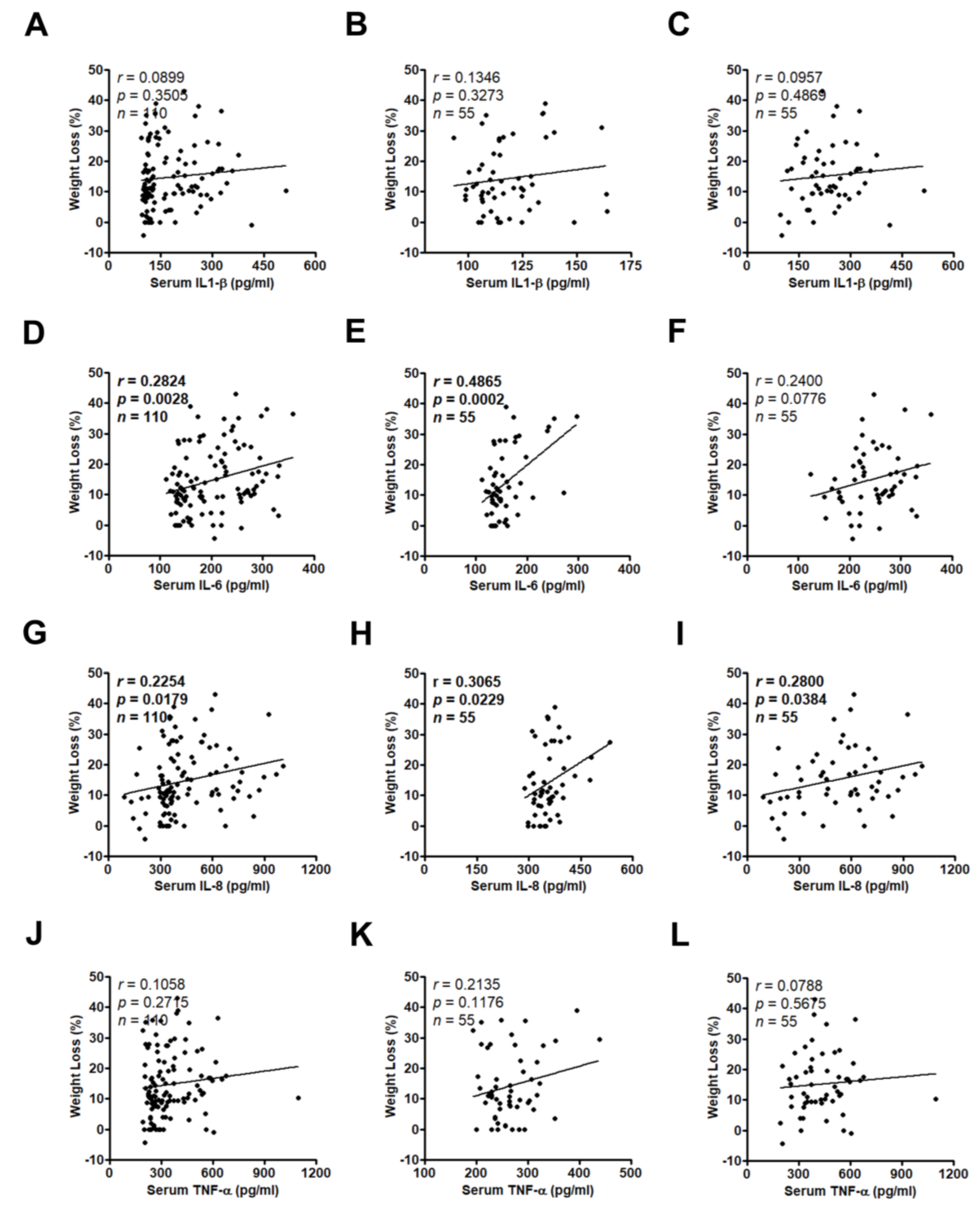
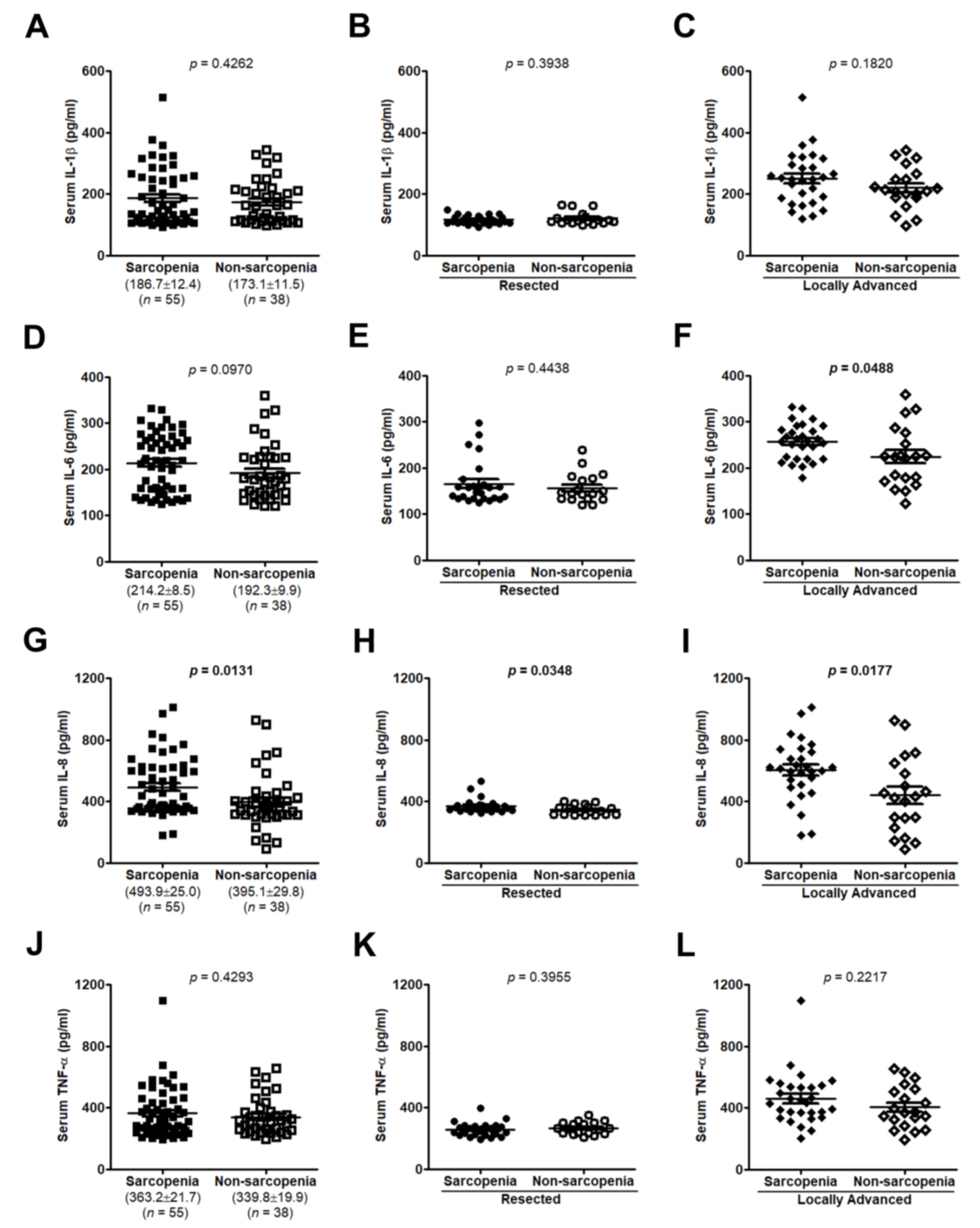
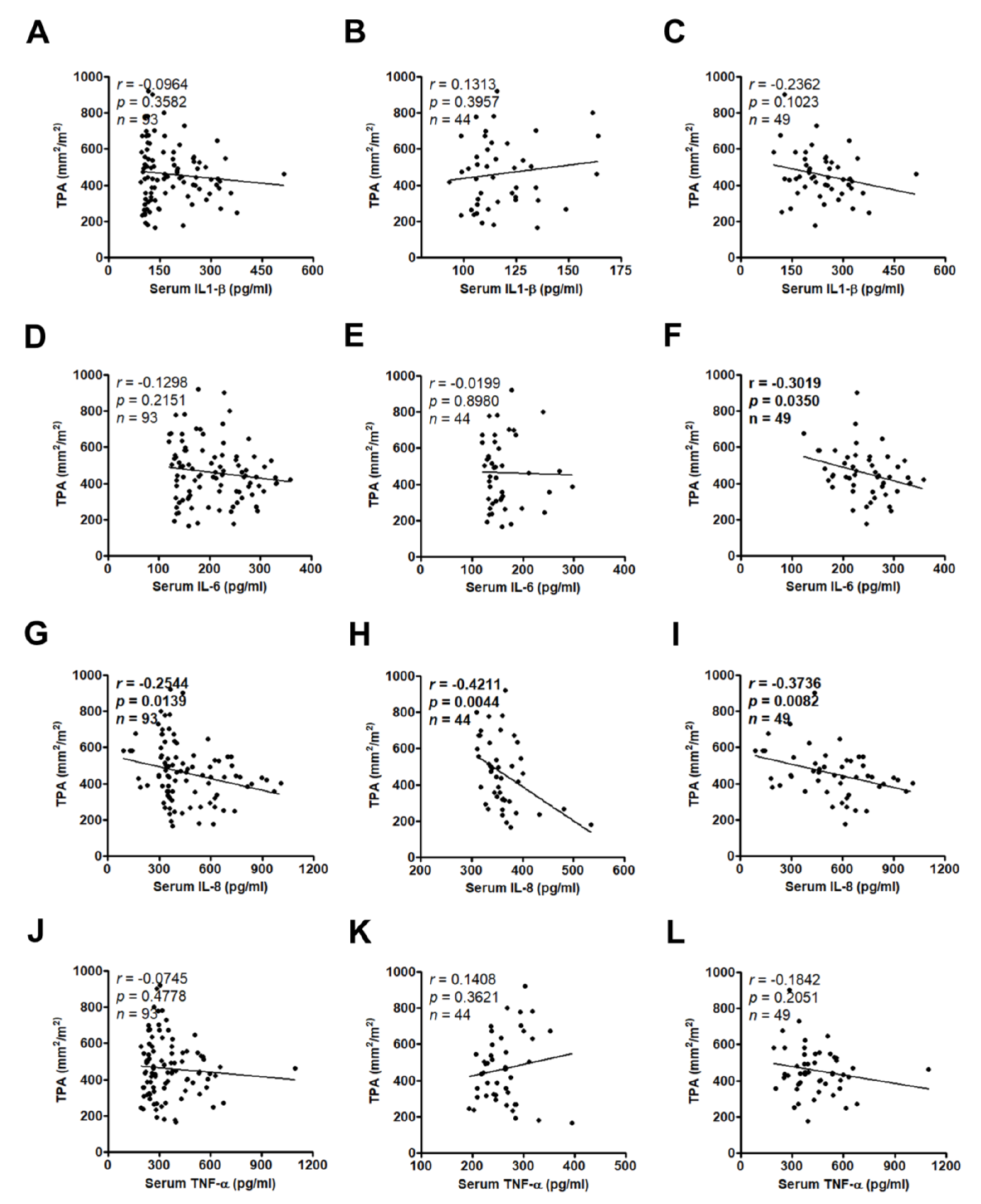
3.3. High Serum IL-8 Level Commonly Occurs in Patients Exhibiting Weight Loss and Muscle Wasting
3.4. IL-8 Expression Are Related to CC Symptoms and Disease Progression in PC
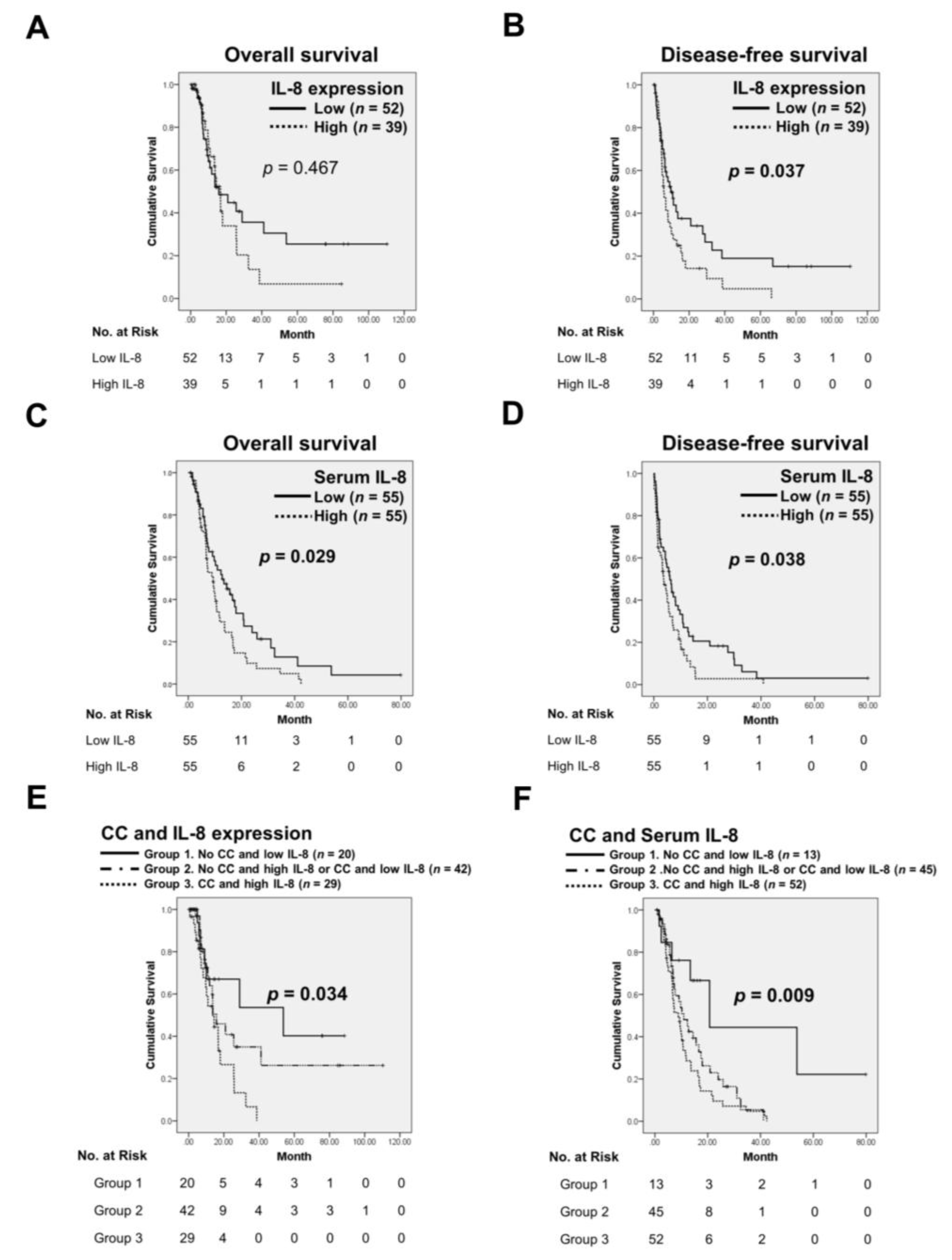
3.5. The Combination of IL-8 with CC Predicts Poor Prognosis of PC
4. Discussion
Author Contributions
Funding
Acknowledgements
Conflicts of Interest
Abbreviations
| CC | cancer cachexia |
| PC | pancreatic cancer |
| IL-1β | Interleukin-1 beta |
| IL-6 | Interleukin-6 |
| IL-8 | Interleukin-8 |
| TNF-α | tumor necrosis factor-α |
| BMI | body-mass index |
| CRP | C-reactive protein |
| ELISA | enzyme-linked immunosorbent assay |
| PACS | pictures archiving and cmmunication system |
| TPA | total psoas area |
| TMAs | tissue microarrays |
| DAPI | 4’,6-diamidino-2-phenylindole |
| OS | overall survival |
| DFS | disease-free survival |
| HRs | hazard ratios |
| CIs | confidence intervals |
| CaP | cachectic prostate carcinoma |
References
- Fearon, K.; Strasser, F.; Anker, S.D.; Bosaeus, I.; Bruera, E.; Fainsinger, R.L.; Jatoi, A.; Loprinzi, C.; MacDonald, N.; Mantovani, G.; et al. Definition and classification of cancer cachexia: An international consensus. Lancet Oncol. 2011, 12, 489–495. [Google Scholar] [CrossRef]
- Evans, W.J.; Morley, J.E.; Argiles, J.; Bales, C.; Baracos, V.; Guttridge, D.; Jatoi, A.; Kalantar-Zadeh, K.; Lochs, H.; Mantovani, G.; et al. Cachexia: A new definition. Clin. Nutr. 2008, 27, 793–799. [Google Scholar] [CrossRef] [PubMed]
- Ronga, I.; Gallucci, F.; Riccardi, F.; Uomo, G. Anorexia-cachexia syndrome in pancreatic cancer: Recent advances and new pharmacological approach. Adv. Med. Sci. 2014, 59, 1–6. [Google Scholar] [CrossRef]
- Mueller, T.C.; Burmeister, M.A.; Bachmann, J.; Martignoni, M.E. Cachexia and pancreatic cancer: Are there treatment options? World J. Gastroenterol. 2014, 20, 9361–9373. [Google Scholar] [CrossRef]
- Tan, C.R.; Yaffee, P.M.; Jamil, L.H.; Lo, S.K.; Nissen, N.; Pandol, S.J.; Tuli, R.; Hendifar, A.E. Pancreatic cancer cachexia: A review of mechanisms and therapeutics. Front. Physiol. 2014, 5, 88. [Google Scholar] [CrossRef]
- Aslani, A.; Gill, A.J.; Roach, P.J.; Allen, B.J.; Smith, R.C. Preoperative body composition is influenced by the stage of operable pancreatic adenocarcinoma but does not predict survival after Whipple’s procedure. HPB 2010, 12, 325–333. [Google Scholar] [CrossRef] [PubMed]
- Paez, D.; Labonte, M.J.; Lenz, H.J. Pancreatic cancer: Medical management (novel chemotherapeutics). Gastroenterol. Clin. N. Am. 2012, 41, 189–209. [Google Scholar] [CrossRef] [PubMed]
- Fearon, K.C.; Baracos, V.E. Cachexia in pancreatic cancer: New treatment options and measures of success. HPB 2010, 12, 323–324. [Google Scholar] [CrossRef]
- Chen, Y.; Shi, M.; Yu, G.Z.; Qin, X.R.; Jin, G.; Chen, P.; Zhu, M.H. Interleukin-8, a promising predictor for prognosis of pancreatic cancer. World J. Gastroenterol. 2012, 18, 1123–1129. [Google Scholar] [CrossRef]
- Donohoe, C.L.; Ryan, A.M.; Reynolds, J.V. Cancer cachexia: Mechanisms and clinical implications. Gastroenterol. Res. Pract. 2011, 2011, 601434. [Google Scholar] [CrossRef]
- Lenk, K.; Schuler, G.; Adams, V. Skeletal muscle wasting in cachexia and sarcopenia: Molecular pathophysiology and impact of exercise training. J. Cachexia Sarcopenia Muscle 2010, 1, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Scheede-Bergdahl, C.; Watt, H.L.; Trutschnigg, B.; Kilgour, R.D.; Haggarty, A.; Lucar, E.; Vigano, A. Is IL-6 the best pro-inflammatory biomarker of clinical outcomes of cancer cachexia? Clin. Nutr. 2012, 31, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Laviano, A.; Meguid, M.M.; Inui, A.; Muscaritoli, M.; Rossi-Fanelli, F. Therapy insight: Cancer anorexia-cachexia syndrome—When all you can eat is yourself. Nat. Clin. Pract. Oncol. 2005, 2, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Ballehaninna, U.K.; Chamberlain, R.S. Serum CA 19-9 as a biomarker for pancreatic cancer—A comprehensive review. Indian J. Surg. Oncol. 2011, 2, 88–100. [Google Scholar] [CrossRef] [PubMed]
- Prado, C.M.; Lieffers, J.R.; McCargar, L.J.; Reiman, T.; Sawyer, M.B.; Martin, L.; Baracos, V.E. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: A population-based study. Lancet Oncol. 2008, 9, 629–635. [Google Scholar] [CrossRef]
- Hou, Y.C.; Chao, Y.J.; Tung, H.L.; Wang, H.C.; Shan, Y.S. Coexpression of CD44-positive/CD133-positive cancer stem cells and CD204-positive tumor-associated macrophages is a predictor of survival in pancreatic ductal adenocarcinoma. Cancer 2014, 120, 2766–2777. [Google Scholar] [CrossRef] [Green Version]
- Argiles, J.M.; Meijsing, S.H.; Pallares-Trujillo, J.; Guirao, X.; Lopez-Soriano, F.J. Cancer cachexia: A therapeutic approach. Med. Res. Rev. 2001, 21, 83–101. [Google Scholar] [CrossRef]
- Argiles, J.M.; Busquets, S.; Stemmler, B.; Lopez-Soriano, F.J. Cancer cachexia: Understanding the molecular basis. Nat. Rev. Cancer 2014, 14, 754–762. [Google Scholar] [CrossRef]
- Tsoli, M.; Robertson, G. Cancer cachexia: Malignant inflammation, tumorkines, and metabolic mayhem. Trends Endocrinol. Metab. 2013, 24, 174–183. [Google Scholar] [CrossRef]
- Suzuki, H.; Asakawa, A.; Amitani, H.; Nakamura, N.; Inui, A. Cancer cachexia—Pathophysiology and management. J. Gastroenterol. 2013, 48, 574–594. [Google Scholar] [CrossRef]
- Alves, M.J.; Figueredo, R.G.; Azevedo, F.F.; Cavallaro, D.A.; Neto, N.I.; Lima, J.D.; Matos-Neto, E.; Radloff, K.; Riccardi, D.M.; Camargo, R.G.; et al. Adipose tissue fibrosis in human cancer cachexia: The role of TGFβ pathway. BMC Cancer 2017, 17, 190. [Google Scholar] [CrossRef] [PubMed]
- Pfitzenmaier, J.; Vessella, R.; Higano, C.S.; Noteboom, J.L.; Wallace, D., Jr.; Corey, E. Elevation of cytokine levels in cachectic patients with prostate carcinoma. Cancer 2003, 97, 1211–1216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujiwara, Y.; Kobayashi, T.; Chayahara, N.; Imamura, Y.; Toyoda, M.; Kiyota, N.; Mukohara, T.; Nishiumi, S.; Azuma, T.; Yoshida, M.; et al. Metabolomics evaluation of serum markers for cachexia and their intra-day variation in patients with advanced pancreatic cancer. PLoS ONE 2014, 9, e113259. [Google Scholar] [CrossRef] [PubMed]
- Tazaki, E.; Shimizu, N.; Tanaka, R.; Yoshizumi, M.; Kamma, H.; Imoto, S.; Goya, T.; Kozawa, K.; Nishina, A.; Kimura, H. Serum cytokine profiles in patients with prostate carcinoma. Exp. Ther. Med. 2011, 2, 887–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, B.; Zhang, D.; Wang, S.; Zheng, H.; Wang, X. Association of interleukin-8 with cachexia from patients with low-third gastric cancer. Comp. Funct. Genom. 2009, 212345. [Google Scholar] [CrossRef] [PubMed]
- Baltgalvis, K.A.; Berger, F.G.; Pena, M.M.; Davis, J.M.; White, J.P.; Carson, J.A. Muscle wasting and interleukin-6-induced atrogin-I expression in the cachectic Apc (Min/+) mouse. Pflugers Arch. 2009, 457, 989–1001. [Google Scholar] [CrossRef]
- Haddad, F.; Zaldivar, F.; Cooper, D.M.; Adams, G.R. IL-6-induced skeletal muscle atrophy. J. Appl. Physiol. 2005, 98, 911–917. [Google Scholar] [CrossRef] [Green Version]
- Bonetto, A.; Aydogdu, T.; Jin, X.; Zhang, Z.; Zhan, R.; Puzis, L.; Koniaris, L.G.; Zimmers, T.A. JAK/STAT3 pathway inhibition blocks skeletal muscle wasting downstream of IL-6 and in experimental cancer cachexia. Am. J. Physiol. Endocrinol. Metab. 2012, 303, 410–421. [Google Scholar] [CrossRef]
- Ando, K.; Takahashi, F.; Motojima, S.; Nakashima, K.; Kaneko, N.; Hoshi, K.; Takahashi, K. Possible role for tocilizumab, an anti-interleukin-6 receptor antibody, in treating cancer cachexia. J. Clin. Oncol. 2013, 31, 69–72. [Google Scholar] [CrossRef]
- Hirata, H.; Tetsumoto, S.; Kijima, T.; Kida, H.; Kumagai, T.; Takahashi, R.; Otani, Y.; Inoue, K.; Kuhara, H.; Shimada, K.; et al. Favorable responses to tocilizumab in two patients with cancer-related cachexia. J. Pain Symptom Manag. 2013, 46, 9–13. [Google Scholar] [CrossRef]
- Bayliss, T.J.; Smith, J.T.; Schuster, M.; Dragnev, K.H.; Rigas, J.R. A humanized anti-IL-6 antibody (ALD518) in non-small cell lung cancer. Expert Opin. Biol. Ther. 2011, 11, 1663–1668. [Google Scholar] [CrossRef] [PubMed]
- Acharyya, S.; Ladner, K.J.; Nelsen, L.L.; Damrauer, J.; Reiser, P.J.; Swoap, S.; Guttridge, D.C. Cancer cachexia is regulated by selective targeting of skeletal muscle gene products. J. Clin. Investig. 2004, 114, 370–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, J.P.; Phillips, B.E.; Smith, K.; Atherton, P.J.; Rankin, D.; Selby, A.L.; Liptrot, S.; Lund, J.; Larvin, M.; Rennie, M.J. Effect of tumor burden and subsequent surgical resection on skeletal muscle mass and protein turnover in colorectal cancer patients. Am. J. Clin. Nutr. 2012, 96, 1064–1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orditura, M.; De Vita, F.; Catalano, G.; Infusino, S.; Lieto, E.; Martinelli, E.; Morgillo, F.; Castellano, P.; Pignatelli, C.; Galizia, G. Elevated serum levels of interleukin-8 in advanced non-small cell lung cancer patients: Relationship with prognosis. J. Interferon Cytokine Res. 2002, 22, 1129–1135. [Google Scholar] [CrossRef] [PubMed]
- Welling, T.H.; Fu, S.; Wan, S.; Zou, W.; Marrero, J.A. Elevated serum IL-8 is associated with the presence of hepatocellular carcinoma and independently predicts survival. Cancer Investig. 2012, 30, 689–697. [Google Scholar] [CrossRef] [PubMed]
- Konno, H.; Ohta, M.; Baba, M.; Suzuki, S.; Nakamura, S. The role of circulating IL-8 and VEGF protein in the progression of gastric cancer. Cancer Sci. 2003, 94, 735–740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanmamed, M.F.; Carranza-Rua, O.; Alfaro, C.; Onate, C.; Martin-Algarra, S.; Perez, G.; Landazuri, S.F.; Gonzalez, A.; Gross, S.; Rodriguez, I.; et al. Serum interleukin-8 reflects tumor burden and treatment response across malignancies of multiple tissue origins. Clin. Cancer Res. 2014, 20, 5697–5707. [Google Scholar] [CrossRef]
- Bachmann, J.; Ketterer, K.; Marsch, C.; Fechtner, K.; Krakowski-Roosen, H.; Buchler, M.W.; Friess, H.; Martignoni, M.E. Pancreatic cancer related cachexia: Influence on metabolism and correlation to weight loss and pulmonary function. BMC Cancer 2009, 9, 255. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Resected | Locally Advanced | p-Value | Resected | Locally Advanced | ||||
|---|---|---|---|---|---|---|---|---|---|
| Non-CC | CC | p-Value | Non-CC | CC | p-Value | ||||
| Number of Patients | 91 | 55 | 32 | 59 | 4 | 51 | |||
| Age, Median (Range) | 66 (37–85) | 67 (41–87) | |||||||
| Sex | |||||||||
| Male | 59 (64.8) | 31 (56.4) | 0.308 | 20 (62.5) | 39 (66.1) | 0.731 | 3 (75.0) | 21 (41.2) | 0.189 |
| Female | 32 (35.2) | 24 (43.6) | 12 (37.5) | 20 (33.9) | 1 (25.0) | 30 (58.8) | |||
| Tumor Location | |||||||||
| Head | 56 (61.5) | 27 (49.1) | 0.002 | 16 (50.0) | 40 (67.8) | 0.415 | 1 (25.0) | 26 (51.0) | 0.502 |
| Neck | 6 (6.6) | 4 (7.3) | 3 (9.4) | 3 (5.1) | 1 (25.0) | 3 (5.9) | |||
| Body/tail | 16 (17.6) | 16 (29.1) | 7 (21.9) | 9 (15.3) | 1 (25.0) | 15 (29.4) | |||
| Uncinate process | 13 (14.3) | 2 (3.6) | 6 (18.8) | 7 (11.9) | 0 (0.0) | 2 (3.9) | |||
| unknown | 0 (0.0) | 6 (10.9) | 0 (0.0) | 0 (0.0) | 1 (25.0) | 5 (9.8) | |||
| Tumor Size | |||||||||
| <3 cm | 34 (37.4) | 12 (37.5) | 22 (37.3) | 0.984 | |||||
| ≥3 cm | 57 (62.6) | 20 (62.5) | 37 (62.7) | ||||||
| Lymph Nodes | |||||||||
| Negative | 46 (50.5) | 15 (46.9) | 31 (52.5) | 0.606 | |||||
| Positive | 45 (49.5) | 17 (53.1) | 28 (47.5) | ||||||
| Margin Status | |||||||||
| R0 | 65 (71.4) | 23 (71.9) | 42 (71.2) | 0.184 | |||||
| R1 | 22 (24.2) | 6 (18.8) | 16 (27.1) | ||||||
| R2 | 4 (4.4) | 3 (9.4) | 1 (1.7) | ||||||
| Tumor Grade | |||||||||
| Poorly diff. | 17 (18.7) | 1 (3.1) | 16 (27.1) | 0.011 | |||||
| Moderate diff. | 48 (52.7) | 18 (56.2) | 30 (50.8) | ||||||
| Well diff. | 26 (28.6) | 13 (40.6) | 13 (22.0) | ||||||
| Stage | |||||||||
| I | 11 (12.1) | 5 (15.6) | 6 (10.2) | 0.814 | |||||
| II | 74 (81.3) | 25 (78.1) | 49 (83.1) | ||||||
| III | 4 (4.4) | 1 (3.1) | 3 (5.1) | ||||||
| IV | 2 (2.2) | 1 (3.1) | 1 (1.7) | ||||||
| CA19-9 | |||||||||
| <100 U/mL | 37 (40.7) | 12 (21.8) | 0.019 | 12 (37.5) | 25 (42.4) | 0.651 | 1 (25.0) | 11 (21.6) | 0.873 |
| >100 U/mL | 54 (59.3) | 43 (78.2) | 20 (62.5) | 34 (57.6) | 3 (75.0) | 40 (78.4) | |||
| Adjuvant Therapy | |||||||||
| Yes | 36 (39.6) | 45 (81.8) | 0.000 | 14 (43.8) | 22 (37.3) | 0.547 | 2 (50.0) | 43 (84.3) | 0.087 |
| No | 55 (60.4) | 10 (18.2) | 18 (56.2) | 37 (62.7) | 2 (50.0) | 8 (15.7) | |||
| Diabetes Mellitus | |||||||||
| Yes | 63 (69.2) | 32 (58.2) | 0.175 | 9 (28.1) | 19 (32.2) | 0.687 | 1 (25.0) | 22 (43.1) | 0.479 |
| No | 28 (30.8) | 23 (41.8) | 23 (71.9) | 40 (67.8) | 3 (75.0) | 29 (56.9) | |||
| Survival | |||||||||
| Yes | 47 (51.6) | 1 (1.8) | 0.000 | 24 (75.0) | 23 (39.0) | 0.001 | 1 (25.0) | 0 (0.0) | 0.000 |
| No | 44 (48.4) | 54 (98.2) | 8 (25.0) | 36 (61.0) | 3 (75.0) | 51 (100.0) | |||
| Cancer Cachexia | |||||||||
| Yes | 59 (64.8) | 51 (92.7) | 0.000 | ||||||
| No | 32 (35.2) | 4 (7.3) | |||||||
| Weight Loss | |||||||||
| <5% | 32 (35.2) | 8 (14.5) | 0.007 | 32 (100.0) | 0 (0.0) | 0.000 | 4 (100.0) | 4 (7.8) | 0.000 |
| >5% | 59 (64.8) | 47 (85.5) | 0 (0.0) | 59 (100.0) | 0 (0.0) | 47 (92.2) | |||
| BMI | |||||||||
| ≤20 kg/m2 | 53 (58.2) | 33 (60.0) | 0.542 | 18 (56.2) | 35 (60.3) | 0.623 | 0 (0.0) | 33 (64.7) | 0.000 |
| >20 kg/m2 | 32 (35.2) | 21 (38.2) | 13 (40.6) | 19 (32.8) | 3 (75.0) | 18 (35.3) | |||
| Unknown | 5 (5.6) | 1 (1.8) | 1 (3.1) | 4 (6.9) | 1 (25.0) | 0 (0.0) | |||
| Fatigue | |||||||||
| Yes | 37 (40.7) | 35 (63.6) | 0.007 | 8 (25.0) | 29 (49.2) | 0.025 | 0 (0.0) | 35 (68.6) | 0.006 |
| No | 54 (59.3) | 20 (36.4) | 24 (75.0) | 30 (50.8) | 4 (100.0) | 16 (31.4) | |||
| Anorexia | |||||||||
| Yes | 38 (41.8) | 34 (61.8) | 0.019 | 9 (28.1) | 29 (49.2) | 0.052 | 0 (0.0) | 34 (66.7) | 0.008 |
| No | 53 (58.2) | 21 (38.2) | 23 (71.9) | 30 (50.8) | 4 (100.0) | 17 (33.3) | |||
| CRP | |||||||||
| <5 mg/L | 16 (17.6) | 6 (10.9) | 0.208 | 8 (25.0) | 8 (13.6) | 0.374 | 0 (0.0) | 6 (11.8) | 0.548 |
| >5 mg/L | 71 (78.0) | 43 (78.2) | 23 (71.9) | 48 (81.4) | 4 (100.0) | 39 (76.5) | |||
| Unknown | 4 (4.4) | 6 (10.9) | 1 (3.1) | 3 (5.1) | 0 (0.0) | 6 (11.8) | |||
| Hemoglobin | |||||||||
| <12 g/dL | 36 (39.6) | 24 (43.6) | 0.149 | 12 (37.5) | 24 (40.7) | 0.767 | 2 (50.0) | 22 (43.1) | 0.903 |
| >12 g/dL | 55 (60.4) | 29 (52.7) | 20 (62.5) | 35 (59.3) | 2 (50.0) | 27 (52.9) | |||
| Unknown | 0 (0.0) | 2 (3.6) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (3.9) | |||
| Albumin | |||||||||
| <3.2 g/dL | 18 (19.8) | 11 (20.0) | 0.060 | 8 (25.0) | 10 (16.9) | 0.515 | 2 (50.0) | 9 (17.6) | 0.273 |
| >3.2 g/dL | 72 (79.1) | 39 (70.9) | 24 (75.0) | 48 (81.4) | 2 (50.0) | 37 (72.5) | |||
| Unknown | 1 (1.1) | 5 (9.1) | 0 (0.0) | 1 (1.7) | 0 (0.0) | 5 (9.8) | |||
| Characteristic | Tissue Expression (%) | ||
|---|---|---|---|
| Low (n = 52) | High (n = 39) | p-Value | |
| Sex | |||
| Male | 33 (63.5) | 26 (66.7) | 0.751 |
| Female | 19 (36.5) | 13 (33.3) | |
| Tumor Location | |||
| Head | 32 (61.5) | 24 (61.5) | 0.789 |
| Neck | 4 (7.7) | 2 (5.1) | |
| Body/tail | 10 (19.2) | 6 (15.4) | |
| Uncinate process | 6 (11.5) | 7 (17.9) | |
| unknown | 0 (0.0) | 0 (0.0) | |
| Tumor Size | |||
| <3 cm | 24 (46.2) | 10 (25.6) | 0.045 |
| ≥3 cm | 28 (53.8) | 29 (74.4) | |
| Lymph Nodes | |||
| Negative | 25 (48.1) | 21 (53.8) | 0.586 |
| Positive | 27 (51.9) | 18 (46.2) | |
| Margin Status | |||
| R0 | 37 (71.2) | 28 (71.8) | 0.747 |
| R1 | 12 (23.1) | 10 (25.6) | |
| R2 | 3 (5.8) | 1 (2.6) | |
| Tumor Grade | |||
| Poorly diff. | 9 (17.3) | 8 (20.5) | 0.542 |
| Moderate diff. | 30 (57.7) | 18 (46.2) | |
| Well diff. | 13 (25.0) | 13 (33.3) | |
| Stage | |||
| I | 7 (13.5) | 4 (10.3) | 0.956 |
| II | 42 (80.8) | 32 (82.1) | |
| III | 2 (3.8) | 2 (5.1) | |
| IV | 1 (1.9) | 1 (2.6) | |
| CA19-9 | |||
| <37 U/mL | 15 (28.8) | 4 (10.3) | 0.031 |
| >37 U/mL | 37 (71.2) | 35 (89.7) | |
| Adjuvant Therapy | |||
| Yes | 18 (34.6) | 18 (46.2) | 0.265 |
| No | 34 (65.4) | 21 (53.8) | |
| Diabetes Mellitus | |||
| Yes | 20 (38.5) | 8 (20.5) | 0.066 |
| No | 32 (61.5) | 31 (79.5) | |
| BMI | |||
| <20 kg/m2 | 26 (50.0) | 27 (71.1) | 0.120 |
| >20 kg/m2 | 22(42.3) | 10 (26.3) | |
| unknown | 4 (7.7) | 1 (2.6) | |
| Fatigue | |||
| Yes | 20 (38.5) | 17 (43.6) | 0.622 |
| No | 32 (61.5) | 22 (56.4) | |
| Anorexia | |||
| Yes | 15 (28.8) | 23 (59.0) | 0.004 |
| No | 37 (71.2) | 16 (41.0) | |
| CRP | |||
| <5 mg/L | 8 (15.4) | 8 (20.5) | 0.307 |
| >5 mg/L | 43 (82.7) | 28 (71.8) | |
| unknown | 1 (1.9) | 3 (3.3) | |
| Hemoglobin | |||
| <12 g/dL | 20 (38.5) | 16 (41.0) | 0.804 |
| >12 g/dL | 32 (61.5) | 23 (59.0) | |
| unknown | 0 (0.0) | 0 (0.0) | |
| Albumin | |||
| <3.2 g/dL | 10 (19.2) | 8 (20.5) | 0.498 |
| >3.2 g/dL | 42 (80.8) | 30 (76.9) | |
| unknown | 0 (0.0) | 1 (2.6) | |
| Variable | No. of Patients | Overall Survival | Disease-Free Survival | ||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | ||
| Cancer Cachexia | |||||||
| No | 36 | 1 | 5.390–64.382 | 0.000 | 1 | 1.092–2.685 | 0.019 |
| Yes | 110 | 18.629 | 1.712 | ||||
| Weight Loss | |||||||
| <5% | 40 | 1 | 2.617–22.544 | 0.000 | 1 | 1.027–2.433 | 0.038 |
| >5% | 106 | 7.682 | 1.581 | ||||
| BMI | |||||||
| ≤20 kg/m2 | 86 | 1 | 0.113–1.037 | 0.058 | 1 | 0.766–1.748 | 0.489 |
| >20 kg/m2 | 54 | 0.342 | 1.157 | ||||
| Unknown | 6 | ||||||
| Fatigue | |||||||
| No | 74 | 1 | 0.829–2.058 | 0.250 | 1 | 0.877–1.839 | 0.207 |
| Yes | 72 | 1.306 | 1.269 | ||||
| Anorexia | |||||||
| No | 74 | 1 | 1.359–3.757 | 0.002 | 1 | 0.959–2.065 | 0.081 |
| Yes | 72 | 2.260 | 1.407 | ||||
| CRP | |||||||
| <5 mg/L | 22 | 1 | 0.989–3.435 | 0.054 | 1 | 0.645–1.717 | 0.837 |
| >5 mg/L | 114 | 1.843 | 1.053 | ||||
| Unknown | 10 | ||||||
| Hemoglobin | |||||||
| <12 g/dL | 60 | 1 | 0424–1.236 | 0.236 | 1 | 0.081–1.612 | 0.182 |
| >12 g/dL | 84 | 0.724 | 0.362 | ||||
| Unknown | 2 | ||||||
| Albumin | |||||||
| <3.2 g/dL | 29 | 1 | 0.404–1.138 | 0.141 | 1 | 0.179–1.388 | 0.183 |
| >3.2 g/dL | 111 | 0.678 | 0.498 | ||||
| Unknown | 6 | ||||||
| IL-8 expression | |||||||
| Low | 50 | 1 | 0.825–2.742 | 0.183 | 1 | 1.080–2.843 | 0.023 |
| High | 41 | 1.504 | 1.752 | ||||
| Serum IL-8 | |||||||
| Low | 55 | 1 | 1.045–2.495 | 0.031 | 1 | 1.021–2.319 | 0.040 |
| High | 55 | 1.615 | 1.539 | ||||
| CC and IL-8 expression | |||||||
| Group 1 | 20 | 1 | Reference | 1 | Reference | ||
| Group 2 | 42 | 1.742 | 0.727–4.170 | 0.213 | 1.508 | 0.784–2.902 | 0.219 |
| Group 3 | 29 | 2.555 | 1.042–6.261 | 0.040 | 1.996 | 1.008–3.954 | 0.047 |
| CC and Serum IL-8 | |||||||
| Group 1 | 13 | 1 | Reference | 1 | Reference | ||
| Group 2 | 45 | 2.911 | 1.117–7.585 | 0.029 | 1.423 | 0.723–2.821 | 0.307 |
| Group 3 | 52 | 3.840 | 1.508–9.777 | 0.005 | 1.928 | 0.990–3.755 | 0.045 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hou, Y.-C.; Wang, C.-J.; Chao, Y.-J.; Chen, H.-Y.; Wang, H.-C.; Tung, H.-L.; Lin, J.-T.; Shan, Y.-S. Elevated Serum Interleukin-8 Level Correlates with Cancer-Related Cachexia and Sarcopenia: An Indicator for Pancreatic Cancer Outcomes. J. Clin. Med. 2018, 7, 502. https://doi.org/10.3390/jcm7120502
Hou Y-C, Wang C-J, Chao Y-J, Chen H-Y, Wang H-C, Tung H-L, Lin J-T, Shan Y-S. Elevated Serum Interleukin-8 Level Correlates with Cancer-Related Cachexia and Sarcopenia: An Indicator for Pancreatic Cancer Outcomes. Journal of Clinical Medicine. 2018; 7(12):502. https://doi.org/10.3390/jcm7120502
Chicago/Turabian StyleHou, Ya-Chin, Chih-Jung Wang, Ying-Jui Chao, Hao-Yun Chen, Hao-Chen Wang, Hui-Ling Tung, Jung-Ting Lin, and Yan-Shen Shan. 2018. "Elevated Serum Interleukin-8 Level Correlates with Cancer-Related Cachexia and Sarcopenia: An Indicator for Pancreatic Cancer Outcomes" Journal of Clinical Medicine 7, no. 12: 502. https://doi.org/10.3390/jcm7120502