Bone Metabolism Markers and Bone Mineral Density in Patients on Long-Term Acenocoumarol Treatment: A Cross-Sectional Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Measurements
2.3. Statistical Methods
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Brown, J.P.; Delmas, P.D.; Malaval, L.; Edouard, C.; Chapuy, M.C.; Meunier, P.J. Serum bone Gla-protein: A specific marker for bone formation in postmenopausal osteoporosis. Lancet 1984, 1, 1091–1093. [Google Scholar] [CrossRef]
- Hauschka, P.V.; Lian, J.B.; Cole, D.E.; Gundberg, C.M. Osteocalcin and matrix Gla protein: Vitamin K-dependent proteins in bone. Physiol. Rev. 1989, 69, 990–1047. [Google Scholar] [CrossRef] [PubMed]
- Price, P.A. Gla-containing proteins of bone. Connect. Tissue. Res. 1989, 21, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Price, P.A.; Otsuka, A.A.; Poser, J.W.; Kristaponis, J.; Raman, N. Characterization of a gamma-carboxyglutamic acid-containing protein from bone. Proc. Natl. Acad. Sci. USA 1976, 73, 1447–1451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hauschka, P.V.; Lian, J.B.; Gallop, P.M. Direct identification of the calcium-binding amino acid, gamma-carboxyglutamate, in mineralized tissue. Proc. Natl. Acad. Sci. USA 1975, 72, 3925–3929. [Google Scholar] [CrossRef] [PubMed]
- Berkner, K.L. Vitamin K-dependent carboxylation. Vitam. Horm. 2008, 78, 131–156. [Google Scholar] [PubMed]
- Booth, S.L.; Centi, A.; Smith, S.R.; Gundberg, C. The role of osteocalcin in human glucose metabolism: Marker or mediator? Nat. Rev. Endocrinol. 2013, 9, 43–55. [Google Scholar] [CrossRef] [PubMed]
- Lacey, D.L.; Timms, E.; Tan, H.L.; Keley, M.J.; Dunstan, C.R.; Burgess, T.; Elliott, R.; Colombero, A.; Elliott, G.; Scully, S.; et al. Osteoprotegerin ligand is a cytokine that regulates osteoclast differentiation and activation. Cell 1998, 93, 165–176. [Google Scholar] [CrossRef]
- Kong, Y.Y.; Feige, U.; Sarosi, I.; Bolon, B.; Tafuri, A.; Morony, S.; Capparelli, C.; Li, J.; Elliott, R.; McCabe, S.; et al. Activated T cells regulate bone loss and joint destruction in adjuvant arthritis through osteoprotegerin ligand. Nature 1999, 402, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Simonet, W.S.; Lacey, D.L.; Dunstan, C.R.; Kelly, M.; Chang, M.S.; Lüthy, R.; Nguyen, H.Q.; Wooden, S.; Bennett, L.; Boone, T.; et al. Osteoprotegerin: A novel secreted protein involved in the regulation of bone density. Cell 1997, 89, 309–319. [Google Scholar] [CrossRef]
- Tan, K.B.; Harrop, J.; Reddy, M.; Young, P.; Terrett, J.; Emery, J.; Moore, G.; Truneh, A. Characterization of a novel TNF-like ligand and recently described TNF ligand and TNF receptor superfamily genes and their constitutive and inducible expression in hematopoietic and non-hematopoietic cells. Gene 1997, 204, 35–46. [Google Scholar] [CrossRef]
- Yun, T.J.; Chaudhary, P.M.; Shu, G.L.; Frazer, J.K.; Ewings, M.K.; Schwartz, S.M.; Pascual, V.; Hood, L.E.; Clark, E.A. OPG/FDCR-1, a TNF receptor family member, is expressed in lymphoid cells and is up-regulated by ligating CD40. J. Immunol. 1998, 161, 6113–6121. [Google Scholar] [PubMed]
- Yasuda, H.; Shima, N.; Nakagawa, N.; Yamaguch, K.; Kinosaki, M.; Mochizuki, S.; Tomoyasu, A.; Yano, K.; Goto, M.; Murakami, A.; et al. Osteoclast differentiation factor is a ligand for osteoprotegerin/osteoclastogenesis-inhibitory factor and is identical to TRANCE/RANKL. Proc. Natl. Acad. Sci. USA 1998, 95, 3597–3602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoppet, M.; Preissner, K.T.; Hofbauer, L.C. RANK ligand and osteoprotegerin: Paracrine regulators of bone metabolism and vascular function. Arterioscler. Thromb. Vasc. Biol. 2002, 22, 549–553. [Google Scholar] [CrossRef] [PubMed]
- Hofbauer, L.C.; Schoppet, M. Clinical implications of the osteoprotegerin/RANKL/RANK system for bone and vascular diseases. JAMA 2004, 292, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Sawicka-Powierza, J.; Konstantynowicz, J.; Jablonska, E.; Zelazowska-Rutkowska, B.; Jelski, W.; Abramowicz, P.; Sasinowski, C.; Chlabicz, S. The association between long-term acenocoumarol treatment and vitamin D deficiency. Front. Endocrinol. (Lausanne) 2018, 9, 226. [Google Scholar] [CrossRef] [PubMed]
- Ducy, P.; Desbois, C.; Boyce, B.; Pinero, G.; Story, B.; Dunstan, C.; Smith, E.; Bonadio, J.; Goldstein, S.; Gundberg, C.; et al. Increased bone formation in osteocalcin-deficient mice. Nature 1996, 382, 448–452. [Google Scholar] [CrossRef] [PubMed]
- Amizuka, N.; Li, M.; Hara, K.; Kobayashi, M.; de Freitas, P.H.; Ubaidus, S.; Oda, K.; Akiyama, Y. Warfarin administration disrupts the assembly of mineralized nodules in the osteoid. J. Electron. Microsc. (Tokyo) 2009, 58, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N.; Bano, G.; Bertozzo, G.; Granziera, S.; Solmi, M.; Manzato, E.; Sergi, G.; Cohen, A.T.; Correll, C.U. Vitamin K antagonists’ use and fracture risk: Results from a systematic review and meta-analysis. J. Thromb. Haemost. 2015, 13, 1665–1675. [Google Scholar] [CrossRef] [PubMed]
- Steffel, J.; Giugliano, R.P.; Braunwald, E.; Murphy, S.A.; Mercuri, M.; Choi, Y.; Aylward, P.; White, H.; Zamorano, J.L.; Antman, E.M.; et al. Edoxaban versus warfarin in atrial fibrillation patients at risk of falling: ENGAGE AF-TIMI 48 analysis. J. Am. Coll. Cardiol. 2016, 68, 1169–1178. [Google Scholar] [CrossRef] [PubMed]
- Lau, W.C.Y.; Chan, E.W.; Cheung, C.L.; Sing, C.W.; Man, K.K.; Lip, G.Y.; Siu, C.W.; Lam, J.K.; Lee, A.C.; Wong, I.C. Association between dabigatran vs warfarin and risk of osteoporotic fractures among patients with nonvalvular atrial fibrillation. JAMA 2017, 317, 1151–1158. [Google Scholar] [CrossRef] [PubMed]
- Poser, J.W.; Price, P.A. A method for decarboxylation of gamma-carboxyglutamic acid in proteins. Properties of the decarboxylated gamma-carboxyglutamic acid protein from calf bone. J. Biol. Chem. 1979, 254, 431–436. [Google Scholar] [PubMed]
- Price, P.A.; Williamson, M.K.; Haba, T.; Dell, R.B.; Jee, W.S. Excessive mineralization with growth plate closure in rats on chronic warfarin treatment. Proc. Natl. Acad. Sci. USA 1982, 79, 7734–7738. [Google Scholar] [CrossRef] [PubMed]
- Binkley, N.; Krueger, D.; Engelke, J.; Suttie, J. Vitamin K deficiency from long-term warfarin anticoagulation does not alter skeletal status in male rhesus monkeys. J. Bone. Miner. Res. 2007, 22, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Obrant, K.J.; Käkönen, S.M.; Astemark, J.; Lilja, H.; Lövgren, T.; Akesson, K.; Pettersson, K. The proportion of carboxylated to total or intact osteocalcin in serum discriminates warfarin-treated patients from control subjects. J. Bone. Miner. Res. 1999, 14, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Knapen, M.H.J.; Hellemons-Boode, B.S.P.; Langenberg-Ledeboer, M.; Knottnerus, J.A.; Hamulyak, K.; Price, P.A.; Vermeer, C. Effect of oral anticoagulant treatment on markers for calcium and bone metabolism. Pathophysiol. Haemost. Thromb. 2000, 30, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Lafforgue, P.; Daver, L.; Monties, J.R.; Chagnaud, C.; De Boissezon, M.C.; Acquaviva, P.C. Bone mineral density in patients given oral vitamin K antagonists. Rev. Rhum. Engl. Ed. 1997, 64, 249–254. [Google Scholar] [PubMed]
- Stenova, E.; Steno, B.; Killinger, Z.; Bagi, L.; Payer, J. Effect of long-term oral anticoagulant therapy on bone mineral density and bone turnover markers: A prospective 12 month study. Bratisl. Lek. Listy 2011, 112, 71–76. [Google Scholar] [PubMed]
- Pastoureau, P.; Vergnaud, P.; Meunier, P.J.; Delmas, P.D. Osteopenia and bone-remodeling abnormalities in warfarin-treated lambs. J. Bone. Miner. Res. 1993, 8, 1417–1426. [Google Scholar] [CrossRef] [PubMed]
- Morishima, Y.; Kamisato, C.; Honda, Y.; Furugohri, T.; Shibano, T. The effects of warfarin and edoxaban, an oral direct factor Xa inhibitor, on gammacarboxylated (Gla-osteocalcin) and undercarboxylated osteocalcin (uc-osteocalcin) in rats. Thromb. Res. 2013, 131, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Resch, H.; Pietschmann, P.; Krexner, E.; Willvonseder, R. Decreased peripheral bone mineral content in patients under anticoagulant therapy with phenprocoumon. Eur. Heart. J. 1991, 12, 439–441. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Honda, Y.; Jun, I. Long-term oral anticoagulation therapy and the risk of hip fracture in patients with previous hemispheric infarction and nonrheumatic atrial fibrillation. Cerebrovasc. Dis. 2010, 29, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Honda, Y.; Kunoh, H.; Oizumi, K. Long-term oral anticoagulation reduces bone mass in patients with previous hemispheric infarction and nonrheumatic atrial fibrillation. Stroke 1997, 28, 2390–2394. [Google Scholar] [CrossRef] [PubMed]
- Fiore, C.E.; Tamburino, C.; Foti, R.; Grmaldi, D. Reduced axial bone mineral content in patients taking an oral anticoagulant. South. Med. J. 1990, 83, 538–542. [Google Scholar] [CrossRef] [PubMed]
- Namba, S.; Yamaoka-Tojo, M.; Hashikata, T.; Ikeda, Y.; Kitasato, L.; Hashimoto, T.; Shimohama, T.; Tojo, T.; Takahira, N.; Masuda, T.; et al. Long-term warfarin therapy and biomarkers for osteoporosis and atherosclerosis. BBA. Clin. 2015, 4, 76–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pluskiewicz, W.; Zurek, J. Quantitative ultrasound and densitometric measurements and laboratory variables in patients on long-term acenocoumarol therapy. Int. J. Clin. Pract. 2007, 61, 1328–1332. [Google Scholar] [CrossRef] [PubMed]
- Arbour, N.C.; Darwish, H.M.; DeLuca, H.F. Transcriptional control of the osteocalcin gene by 1,25-dihydroxyvitamin D-2 and its 24-epimer in rat osteosarcoma cells. Biochim. Biophys. Acta. 1995, 1263, 147–153. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | AC Users (n = 42) | Control Subjects (n = 28) | p Value |
|---|---|---|---|
| Gender (male/female), n (%) | 22 (52.4)/20 (47.6) | 14 (50)/14 (50) | 0.845 |
| Smokers/non-smokers, n (%) | 6 (14.3)/36 (83.7) | 3 (10.7)/25 (89.3) | 0.662 |
| Age, years | 64.67 ± 8.74 (40–81) | 63.29 ± 9.8 (39–84) | 0.54 |
| BMI, kg/m2 | 28.82 ± 5.33 (16.9–41.09) | 26.76 ± 3.6 (19.8–34.2) | 0.078 |
| Time post-menopause, years | 14.05 ± 8.38 (0–28) | 13 ± 11.37 (0–34) | 0.758 |
| Osteocalcin (OC), ng/mL | 4.94 ± 2.22 (1.16–11.8) | 10.68 ± 4.5 (6.03–25) | <0.001 |
| Osteoprotegerin (OPG), pg/mL | 27.53 ± 7.1 (17.93–54.6) | 25.42 ± 5.5 (14.93–36.4) | 0.19 |
| sRANKL log | 4.79 ± 0.53 (3.75–5.63) | 4.67 ± 0.58 (3.75–5.63) | 0.51 |
| sRANKL/OPG log ratio | 3.36 ± 0.54 (2.22–4.29) | 3.31 ± 0.58 (2.32–4.2) | 0.685 |
| Femur neck BMD, g/cm2 | 0.93 ± 0.16 (0.64–1.31) | 0.91 ± 0.1 (0.69–1.2) | 0.6 |
| Femur neck T-score | −0.77 ± 1.28 (−2.86–2.75) | −0.85 ± 1.1 (−2.71–1.6) | 0.78 |
| Femur neck Z-score | 0.15 ± 1.07 (−1.61–3.09) | 0.1 ± 1.0 (−2.06–2) | 0.845 |
| Lumbar spine BMD (L1–L4), g/cm2 | 1.12 ± 0.17 (0.78–1.53) | 1.06 ± 0.17 (0.73–1.4) | 0.091 |
| Lumbar spine BMD T-score | −0.66 ± 1.38 (−3.32–2.61) | −1.25 ± 1.4 (−3.72–1.8) | 0.085 |
| Lumbar spine BMD Z-score | −0.12 ± 1.22 (−2.66–2.42) | −0.53 ± 1.2 (−3.32–1.4) | 0.18 |
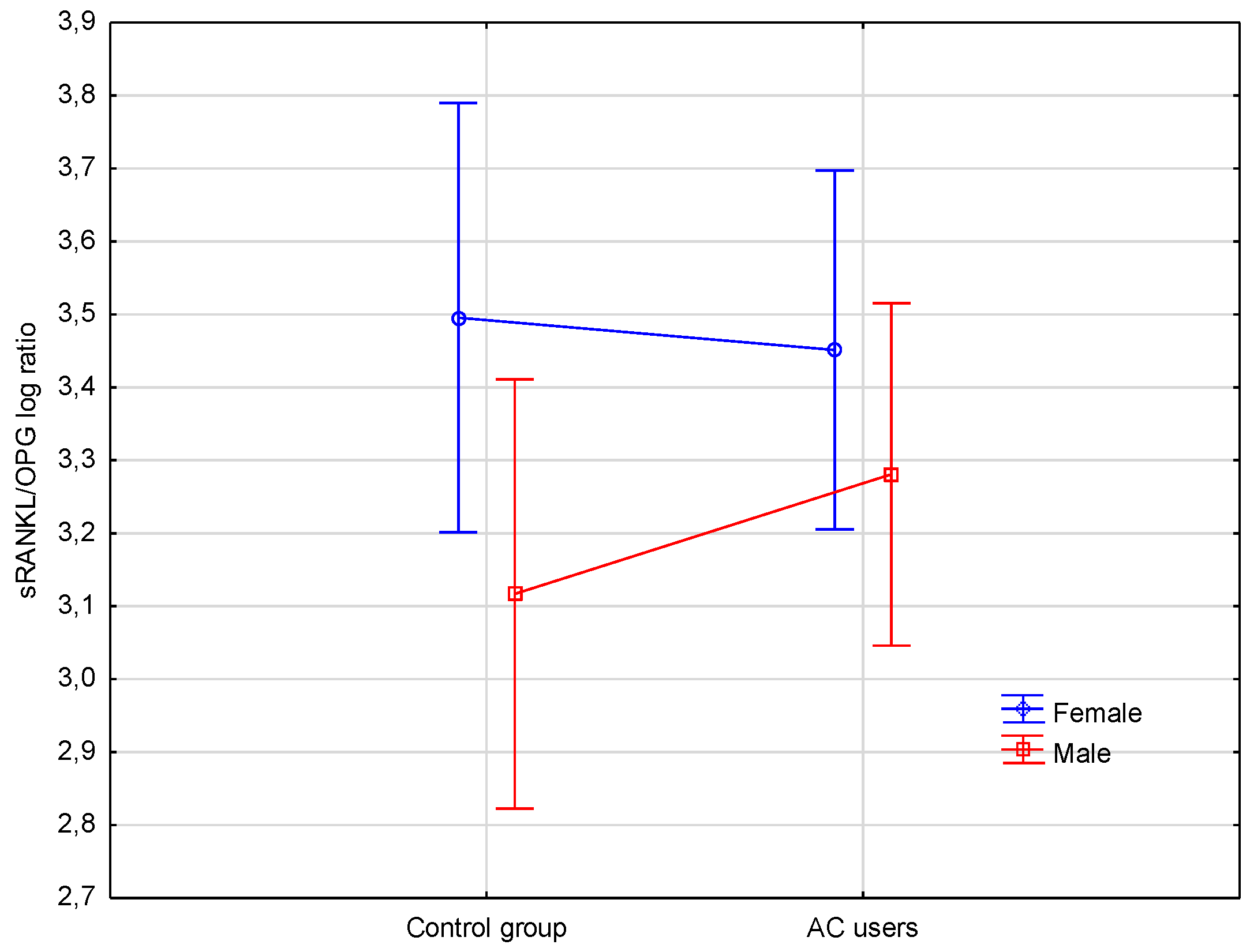
| Variables | Female AC Users | Female Controls | Male AC Users | Male Controls |
|---|---|---|---|---|
| Number | 20 | 14 | 22 | 14 |
| OC, ng/mL | 4.68 ± 2.44 a | 11.42 ± 5.58 | 5.17 ± 2.03 b | 9.94 ± 2.98 |
| OPG, pg/mL | 27.81 ± 7.03 | 24.12 ± 6.26 | 27.27 ± 7.38 | 26.72 ± 4.42 |
| sRANKL log | 4.88 ± 0.48 | 4.86 ± 0.58 | 4.71 ± 0.58 | 4.54 ± 0.52 |
| sRANKL/OPG log ratio | 3.45 ± 0.51 | 3.5 ± 0.59 | 3.28 ± 0.58 | 3.12 ± 0.53 |
| Femur neck BMD, g/cm2 | 0.91 ± 0.18 | 0.86 ± 0.11 | 0.95 ± 0.14 | 0.96 ± 0.11 |
| Lumbar spine BMD (L1–L4), g/cm2 | 1.07 ± 0.17 | 1.0 ± 0.16 | 1.17 ± 0.16 | 1.1 ± 0.17 |
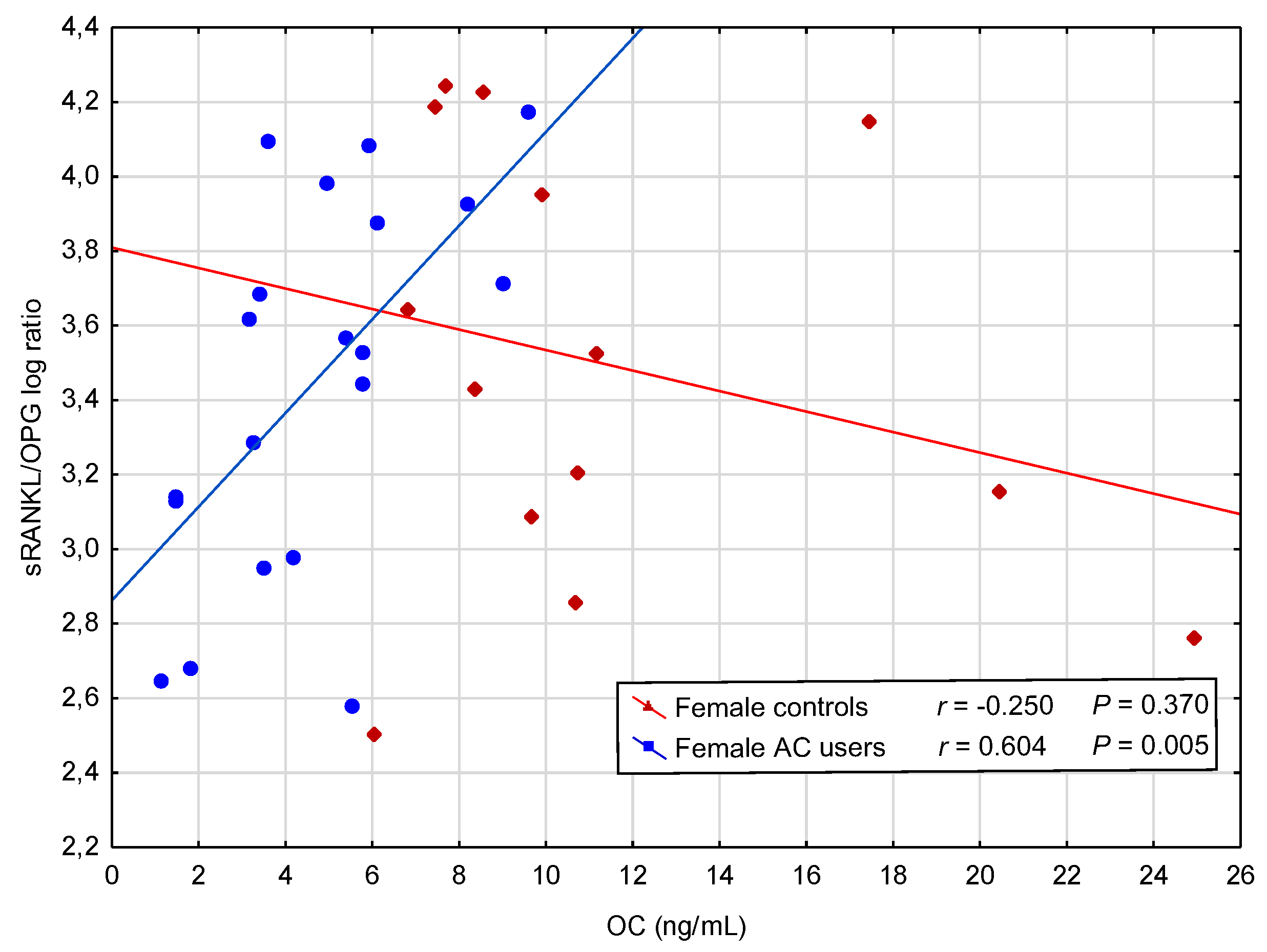
| Variables | Values of Pearson’s Linear Correlation Coefficients | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Female AC Users n = 20 | Female Controls n = 14 | Male AC Users n = 22 | Male Controls n = 14 | ||||||
| r | p | r | p | r | p | r | p | ||
| OC, ng/mL | OPG (pg/mL) | −0.495 | 0.027 | −0.338 | 0.237 | 0.701 | <0.001 | 0.095 | 0.747 |
| sRANKL log | 0.528 | 0.017 | −0.33 | 0.25 | 0.258 | 0.247 | −0.15 | 0.609 | |
| sRANKL/OPG log ratio | 0.604 | 0.005 | −0.25 | 0.37 | 0.148 | 0.513 | −0.161 | 0.582 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sawicka-Powierza, J.; Jablonska, E.; Ratajczak-Wrona, W.; Rogowska-Szadkowska, D.; Garley, M.; Oltarzewska, A.M.; Chlabicz, S.; Konstantynowicz, J. Bone Metabolism Markers and Bone Mineral Density in Patients on Long-Term Acenocoumarol Treatment: A Cross-Sectional Study. J. Clin. Med. 2018, 7, 372. https://doi.org/10.3390/jcm7100372
Sawicka-Powierza J, Jablonska E, Ratajczak-Wrona W, Rogowska-Szadkowska D, Garley M, Oltarzewska AM, Chlabicz S, Konstantynowicz J. Bone Metabolism Markers and Bone Mineral Density in Patients on Long-Term Acenocoumarol Treatment: A Cross-Sectional Study. Journal of Clinical Medicine. 2018; 7(10):372. https://doi.org/10.3390/jcm7100372
Chicago/Turabian StyleSawicka-Powierza, Jolanta, Ewa Jablonska, Wioletta Ratajczak-Wrona, Dorota Rogowska-Szadkowska, Marzena Garley, Alicja M. Oltarzewska, Slawomir Chlabicz, and Jerzy Konstantynowicz. 2018. "Bone Metabolism Markers and Bone Mineral Density in Patients on Long-Term Acenocoumarol Treatment: A Cross-Sectional Study" Journal of Clinical Medicine 7, no. 10: 372. https://doi.org/10.3390/jcm7100372