
Augmentation Rhinoplasty and Centrofacial Lipofilling: Our Experience (ARCL)
 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
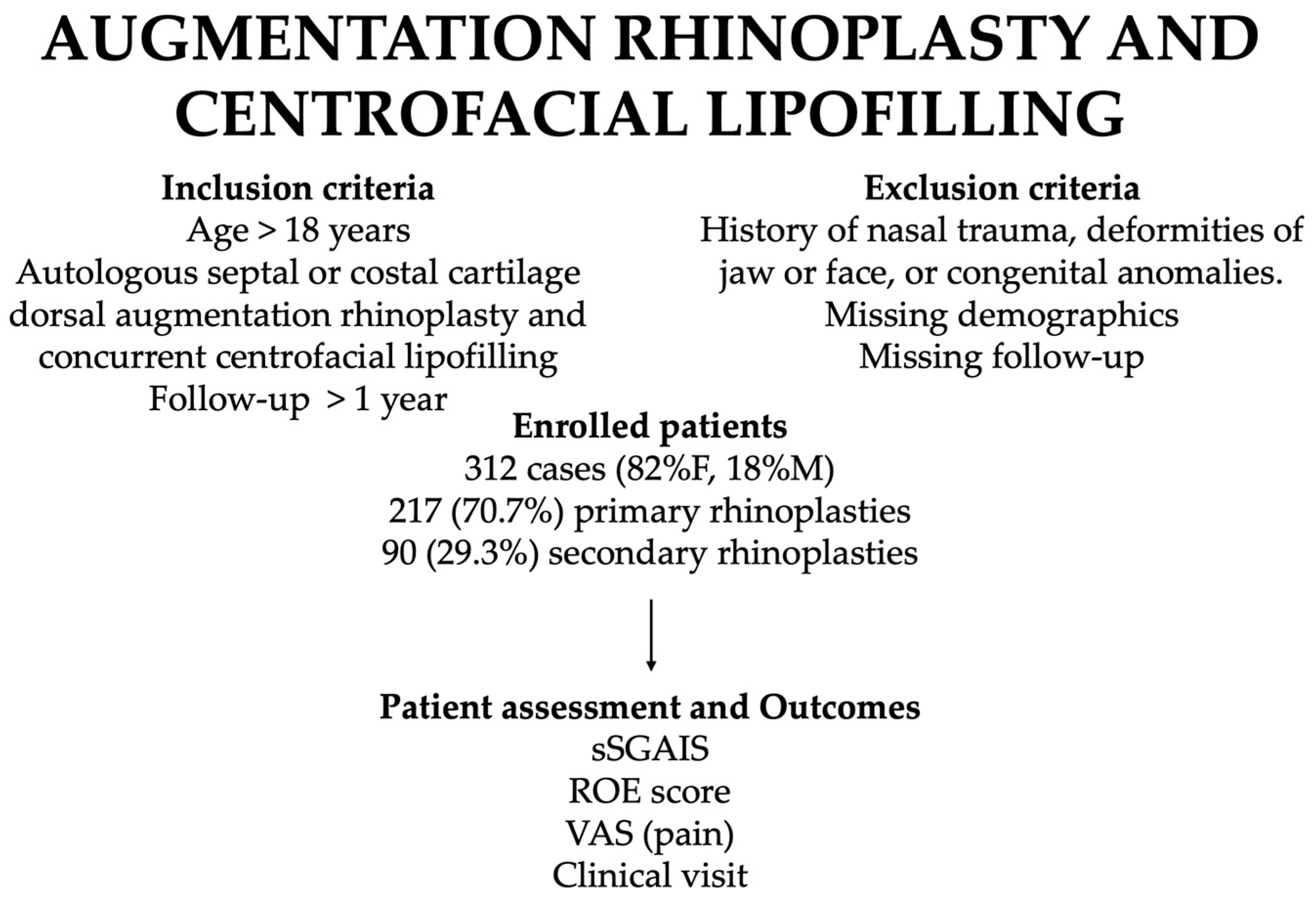
2.1. Study Design
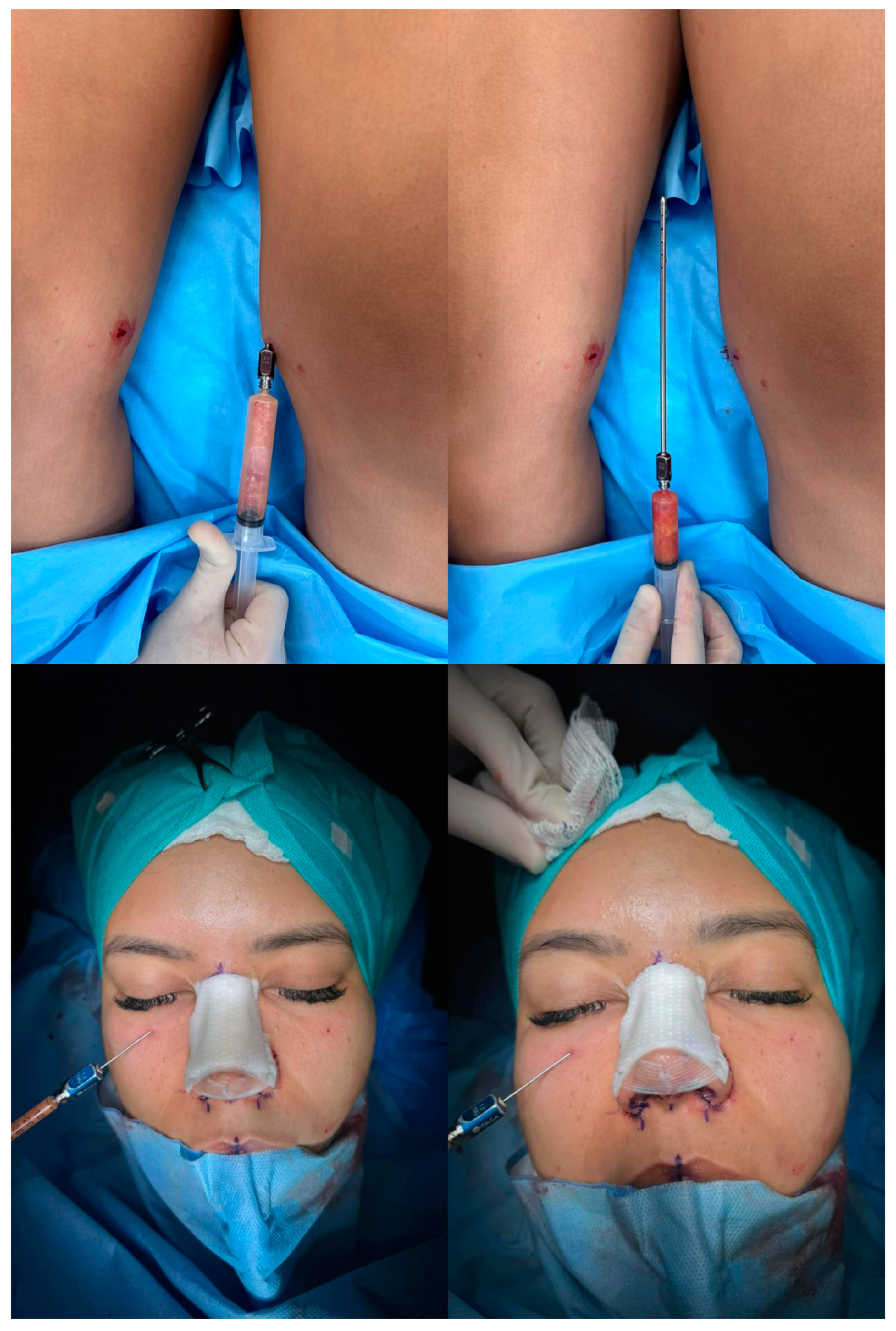
2.2. Operative Technique
2.3. Rhinoplasty
2.4. Centrofacial Lipofilling
3. Results
3.1. Study Population
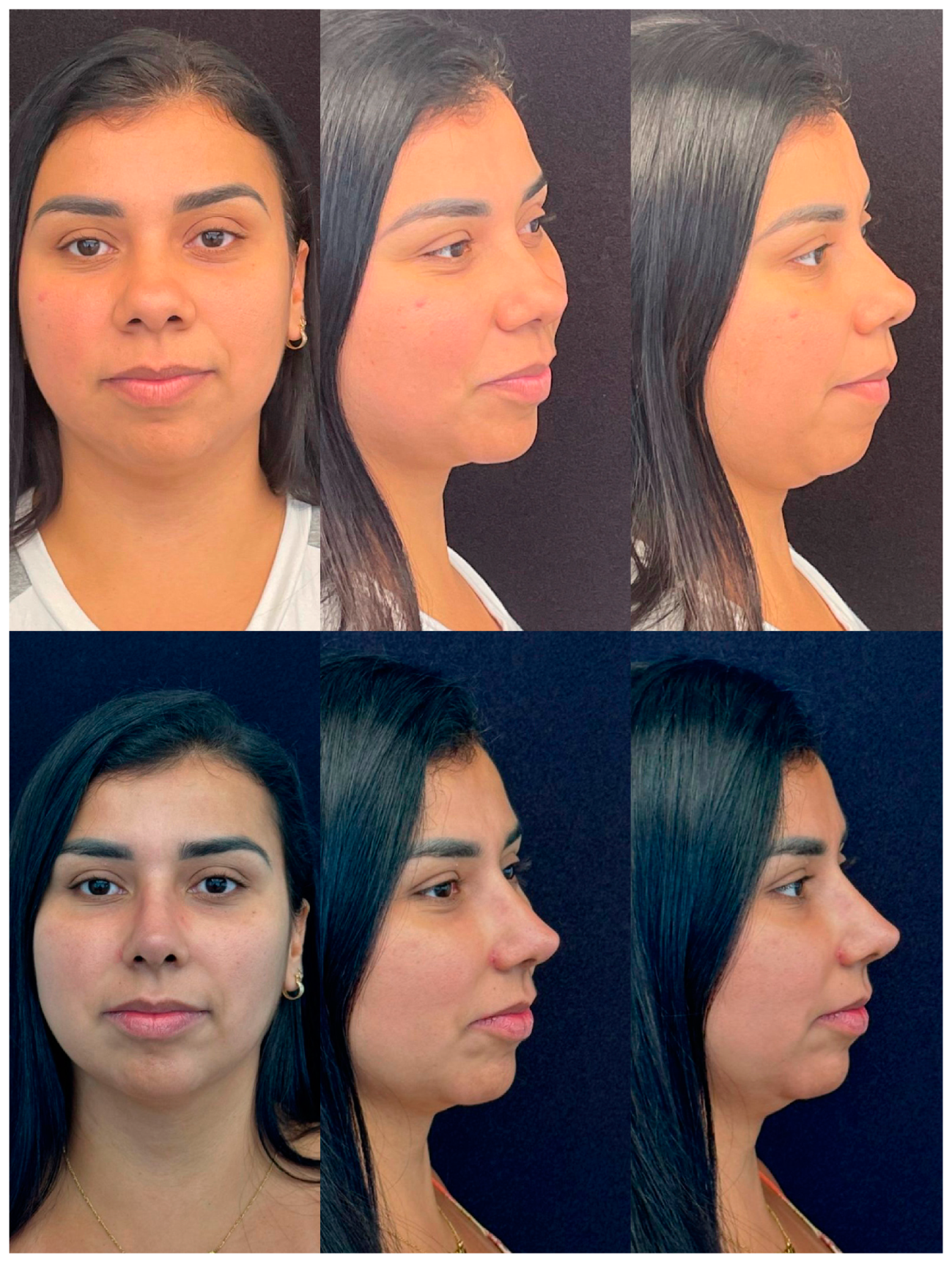
3.2. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- ASPS_Plastic_Surgery_Statistics. 2022. Available online: https://www.plasticsurgery.org/documents/News/Statistics/2022/plastic-surgery-statistics-report-2022.pdf (accessed on 31 December 2023).
- Matory, W.E., Jr.; Matory, W.E. Definitions of beauty in the ethnic patient. In Ethnic Considerations in Facial Aesthetic Surgery; Lippincott-Raven Publishers: Philadelphia, PA, USA, 1998; pp. 61–83. [Google Scholar]
- Hoefflin, S. Hoefflin, Ethnic Rhinoplasty; Springer: New York, NY, USA, 1998. [Google Scholar] [CrossRef]
- Powell, N.; Humphreys, B. Proportions of the Aesthetic Face; American Academy of Facial Plastic and Reconstructive Surgery Series; Thieme-Stratton New York: New York, NY, USA, 1984. [Google Scholar]
- Cobo, R. Ethnic Rhinoplasty. Facial Plast. Surg. 2019, 35, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Cerrati, E.W.; Thomas, J.R. The multicultural evolution of beauty in facial surgery. Braz. J. Otorhinolaryngol. 2017, 83, 373–374. [Google Scholar] [CrossRef] [PubMed]
- Psychological Evaluation of Patients Seeking Rhinoplasty. Available online: http://www.eajm.org/en/psychological-evaluation-of-patients-seeking-rhinoplasty-132888 (accessed on 26 December 2023).
- Pozzi, M.; Fadel, C.; Bolletta, A.; Cuomo, R.; Roxo, C.W. Ethnic rhinoplasty: Preliminary results of our technique in the pursuit of the harmonious nose. J. Plast. Reconstr. Aesthet. Surg. 2023, 87, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Yaremchuk, M.J.; Vibhakar, D. Pyriform Aperture Augmentation as An Adjunct to Rhinoplasty. Clin. Plast. Surg. 2016, 43, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Sykes, J.M.; Suarez, G.A. Chin Advancement, Augmentation, and Reduction as Adjuncts to Rhinoplasty. Clin. Plast. Surg. 2016, 43, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Carvas, M.; Tonnard, P.; Verpaele, A. Rhinoplasty Combined With Centrofacial Lipofilling to Optimize Facial Proportions. Aesthet. Surg. J. Open Forum 2020, 2, ojz034. [Google Scholar] [CrossRef] [PubMed]
- Lindenblatt, N.; van Hulle, A.; Verpaele, A.M.; Tonnard, P.L. The Role of Microfat Grafting in Facial Contouring. Aesthet. Surg. J. 2015, 35, 763–771. [Google Scholar] [CrossRef] [PubMed]
- Krastev, T.K.; Beugels, J.; Hommes, J.; Piatkowski, A.; Mathijssen, I.; van der Hulst, R. Efficacy and Safety of Autologous Fat Transfer in Facial Reconstructive Surgery: A Systematic Review and Meta-analysis. JAMA Facial Plast. Surg. 2018, 20, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Daniel, R.K.; Kosins, A.M. Current Trends in Preservation Rhinoplasty. Aesthet. Surg. J. Open Forum 2020, 2, ojaa003. [Google Scholar] [CrossRef]
- Chan, D.; Shipchandler, T.Z. Update on the evidence for functional rhinoplasty techniques. Curr. Opin. Otolaryngol. Head Neck Surg. 2015, 23, 265–271. [Google Scholar] [CrossRef]
- Romo, T., 3rd; Abraham, M.T. The ethnic nose. Facial Plast. Surg. 2003, 19, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.R.; Won, T.B. Rhinoplasty in the Asian Patient. Clin. Plast. Surg. 2016, 43, 265–279. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.H.; Jang, Y.J. Rib cartilage in Asian rhinoplasty: New trends. Curr. Opin. Otolaryngol. Head Neck Surg 2019, 27, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Hwang, N.H.; Dhong, E.S. Septal Extension Graft in Asian Rhinoplasty. Facial Plast. Surg. Clin. N. Am. 2018, 26, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Wan, R.; Weissman, J.P.; Ullrich, P.J.; Joshi, C.; Williams, T.; Galiano, R.D. The Utilization of Fresh Frozen Cartilage in Asian Rhinoplasty: A New Approach. Plast. Reconstr. Surg. Glob. Open 2023, 11, e4903. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.N.; Most, S.P. Concepts of Facial Aesthetics When Considering Ethnic Rhinoplasty. Otolaryngol. Clin. N. Am. 2020, 53, 195–208. [Google Scholar] [CrossRef] [PubMed]
- Porter, J.P.; Olson, K.L. Anthropometric facial analysis of the African American woman. Arch. Facial Plast. Surg. 2001, 3, 191–197. [Google Scholar] [CrossRef]
- Leong, S.C.; White, P.S. A comparison of aesthetic proportions between the healthy Caucasian nose and the aesthetic ideal. J. Plast. Reconstr. Aesthet. Surg. 2006, 59, 248–252. [Google Scholar] [CrossRef]
- Millard, D.R. Adjuncts in Augmentation Mentoplasty and Corrective Rhinoplasty. Plast. Reconstr. Surg. 1965, 36, 48–61. [Google Scholar] [CrossRef]
- Park, Y.J.; Cha, J.H.; Han, S.E. Maximizing Thread Usage for Facial Rejuvenation: A Preliminary Patient Study. Aesthetic Plast. Surg. 2021, 45, 528–535. [Google Scholar] [CrossRef]
- Bueller, H. Ideal Facial Relationships and Goals. Facial Plast. Surg. 2018, 34, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Honn, M.; Goz, G. The ideal of facial beauty: A review. J. Orofac. Orthop. 2007, 68, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Cortese, A.; D’Alessio, G.; Brongo, S.; Amato, M.; Sarno, M.R.; Claudio, P.P. New Techniques in Relation to New Concepts of the Aesthetic of the Face: Technical Considerations and Aesthetic Evaluation. J. Craniofac. Surg. 2016, 27, e693–e695. [Google Scholar] [CrossRef] [PubMed]
- Grinfeld, A.; Betelli, R.; Arruda, G.; Almeida, W. How to Harmonize the Ethnic Nose. Facial Plast. Surg. 2016, 32, 620–624. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| modified 5-points Global Aesthetic Improvement Scale (S-GAIS) | |
| 1 = very much improved, 2 = much improved, 3 = improved, 4 = no change, 5 = worse | |
| Facial harmony | 1.3 (range 1–3) |
| Profile vision | 1.2 (range 1–2) |
| Femininity | 2.4 (range 1–4) |
| Attractiveness | 2.2 (range 1–4) |
| Youthfulness | 1.8 (range 1–2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pozzi, M.; Susini, P.; di Seclì, D.; Schettino, M.; Grimaldi, L.; Cuomo, R.; Roxo, C.W. Augmentation Rhinoplasty and Centrofacial Lipofilling: Our Experience (ARCL). J. Clin. Med. 2024, 13, 1965. https://doi.org/10.3390/jcm13071965
Pozzi M, Susini P, di Seclì D, Schettino M, Grimaldi L, Cuomo R, Roxo CW. Augmentation Rhinoplasty and Centrofacial Lipofilling: Our Experience (ARCL). Journal of Clinical Medicine. 2024; 13(7):1965. https://doi.org/10.3390/jcm13071965
Chicago/Turabian StylePozzi, Mirco, Pietro Susini, Davide di Seclì, Michela Schettino, Luca Grimaldi, Roberto Cuomo, and Carlos Weck Roxo. 2024. "Augmentation Rhinoplasty and Centrofacial Lipofilling: Our Experience (ARCL)" Journal of Clinical Medicine 13, no. 7: 1965. https://doi.org/10.3390/jcm13071965