
Using Augmented Reality Technology to Optimize Transfacet Lumbar Interbody Fusion: A Case Report
 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methodology
2.1. Patient History and Physical Examination
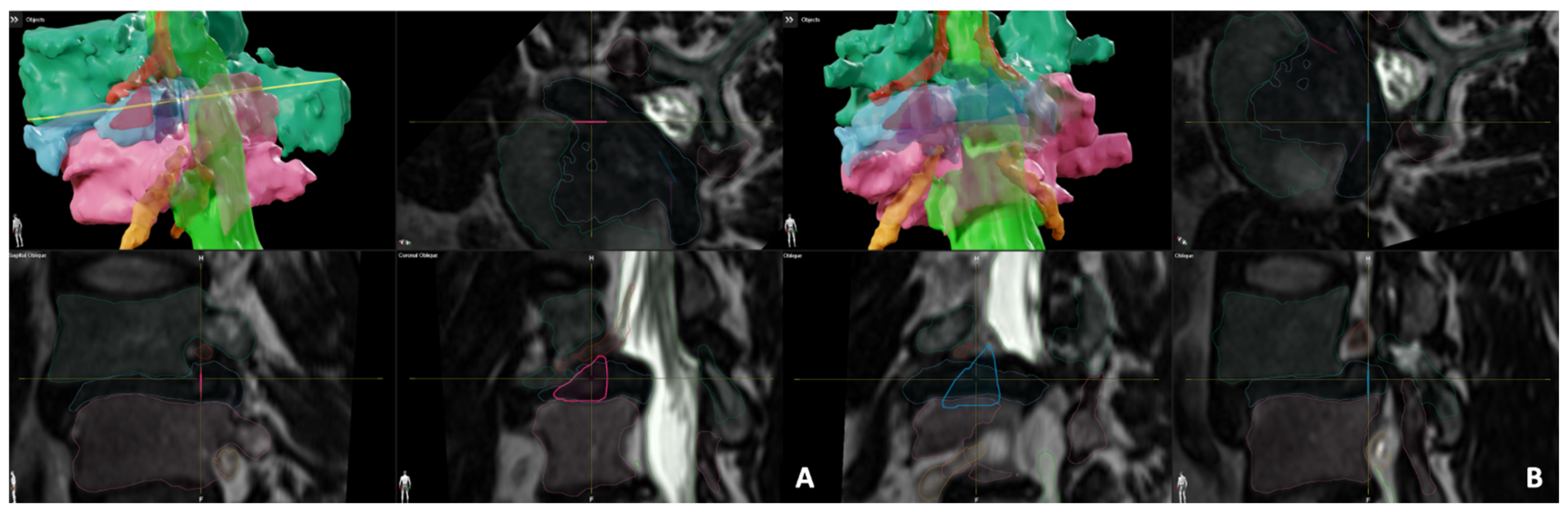
2.2. Kambin’s Triangle and TransFacet Segmentation
2.3. Pre-Operative Measurements
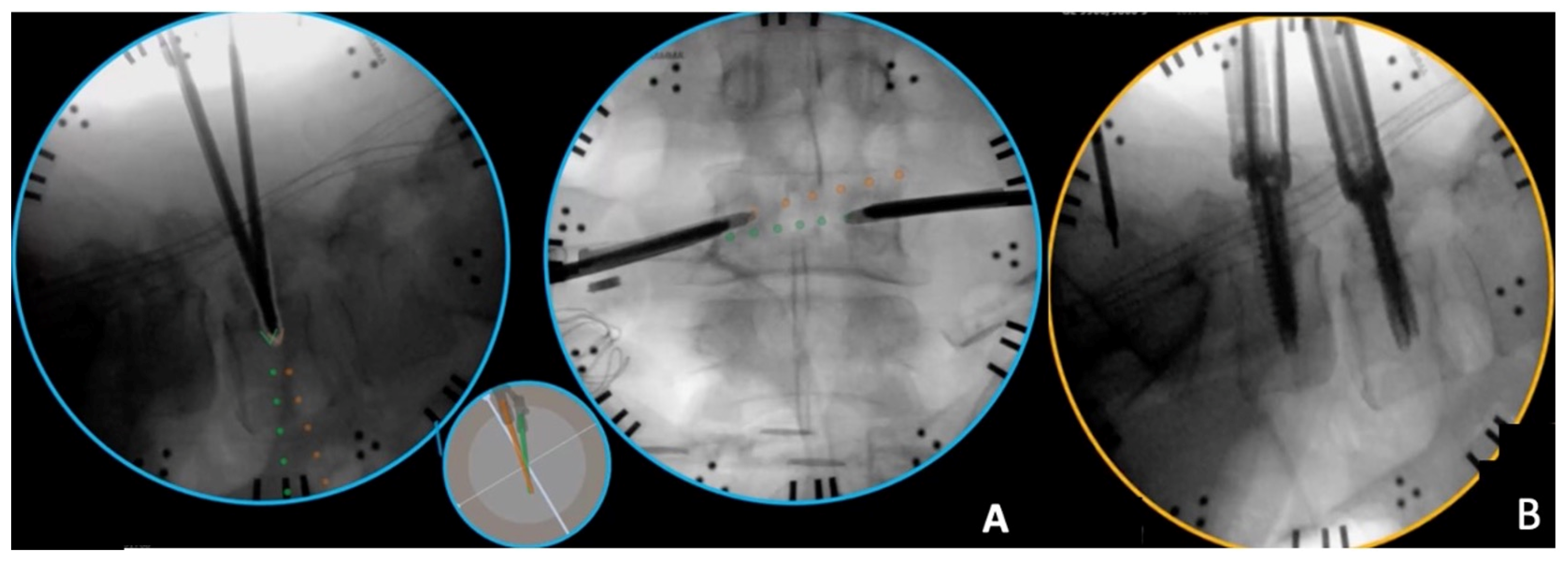
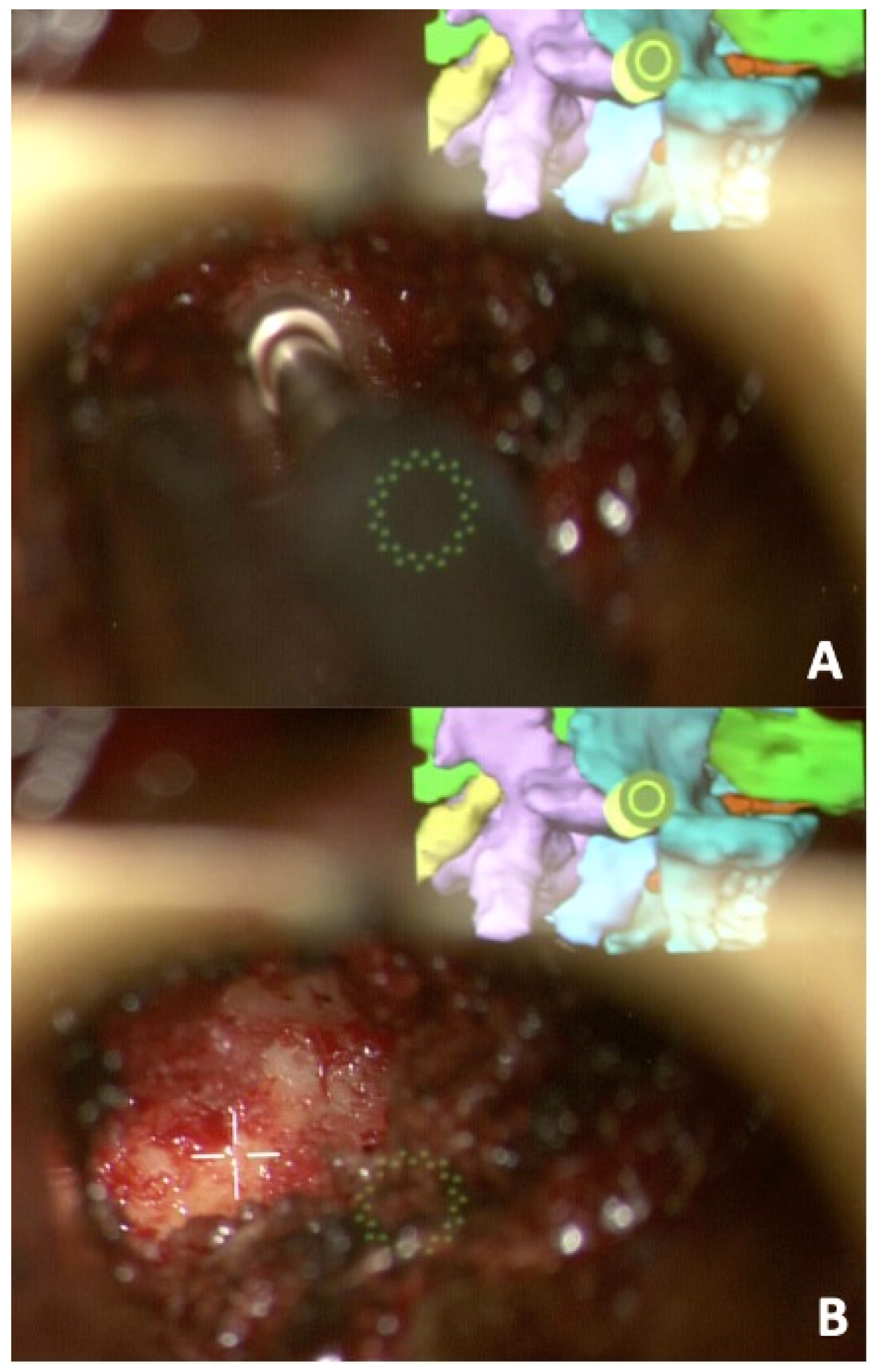
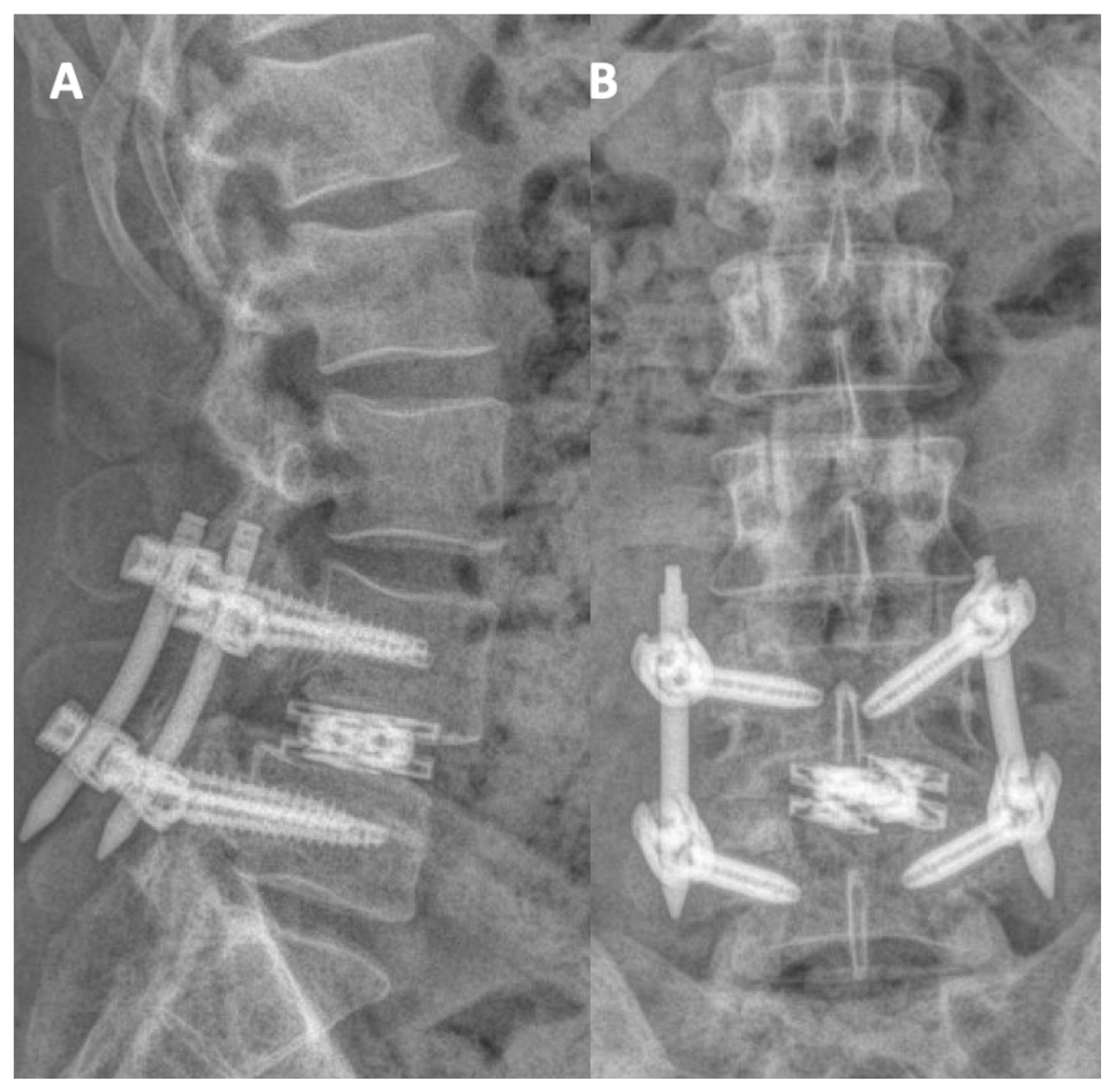
2.4. Intra-Operative Details
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kumar, P.R.; Jha, R.K.; Katti, A. Brain tissue segmentation in neurosurgery: A systematic analysis for quantitative tractography approaches. Acta Neurol. Belg. 2023, 124, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Ren, G.; Yu, K.; Xie, Z.; Wang, P.; Zhang, W.; Huang, Y.; Wang, Y.; Wu, X. Current Applications of Machine Learning in Spine: From Clinical View. Glob. Spine J. 2022, 12, 1827–1840. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Du, Y.; Wei, Z.; Liu, H.; Yang, X.; Zhao, D. Spine Medical Image Segmentation Based on Deep Learning. J. Healthc. Eng. 2021, 2021, 1917946. [Google Scholar] [CrossRef] [PubMed]
- Cheng, P.; Yang, Y.; Yu, H.; He, Y. Automatic vertebrae localization and segmentation in CT with a two-stage Dense-U-Net. Sci. Rep. 2021, 11, 22156. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Jiang, J.L.; Zhang, N.; Zhao, H.; Liu, Z. Automatic Lumbar Vertebra Landmark Localization and Segmentation for Pedicle Screw Placement. In Proceedings of the 2022 26th International Conference on Pattern Recognition (ICPR), Montreal, QC, Canada, 21–25 August 2022; pp. 4263–4269. [Google Scholar]
- Mu, S.; Wang, J.; Gong, S. Mechanical Analysis of Posterior Pedicle Screw System Placement and Internal Fixation in the Treatment of Lumbar Fractures. Comput. Math. Methods Med. 2022, 2022, 6497754. [Google Scholar] [CrossRef] [PubMed]
- Skovrlj, B.; Gilligan, J.; Cutler, H.S.; Qureshi, S.A. Minimally invasive procedures on the lumbar spine. World J. Clin. Cases 2015, 3, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Ham, D.W.; Kwon, B.T.; Park, S.M.; Kim, H.J.; Yeom, J.S. Minimally Invasive Spine Surgery: Techniques, Technologies, and Indications. Asian Spine J. 2020, 14, 694–701. [Google Scholar] [CrossRef] [PubMed]
- Waguia, R.; Gupta, N.; Gamel, K.L.; Ukachukwu, A. Current and Future Applications of the Kambin’s Triangle in Lumbar Spine Surgery. Cureus 2022, 14, e25686. [Google Scholar] [CrossRef]
- Gil, H.Y.; Jeong, S.; Cho, H.; Choi, E.; Nahm, F.S.; Lee, P.B. Kambin’s Triangle Approach versus Traditional Safe Triangle Approach for Percutaneous Transforaminal Epidural Adhesiolysis Using an Inflatable Balloon Catheter: A Pilot Study. J. Clin. Med. 2019, 8, 1996. [Google Scholar] [CrossRef]
- Pairaiturkar, P.P.; Sudame, O.S.; Pophale, C.S. Evaluation of Dimensions of Kambin’s Triangle to Calculate Maximum Permissible Cannula Diameter for Percutaneous Endoscopic Lumbar Discectomy: A 3-Dimensional Magnetic Resonance Imaging Based Study. J. Korean Neurosurg. Soc. 2019, 62, 414–421. [Google Scholar] [CrossRef]
- Tabarestani, T.Q.; Sykes, D.A.; Maquoit, G.; Wang, T.Y.; Ayoub, C.M.; Shaffrey, C.I.; Wiggins, W.F.; Abd-El-Barr, M.M. Novel Merging of CT and MRI to Allow for Safe Navigation into Kambin’s Triangle for Percutaneous Lumbar Interbody Fusion—Initial Case Series Investigating Safety and Efficacy. Oper. Neurosurg. 2023, 24, 331–340. [Google Scholar] [CrossRef]
- Tabarestani, T.Q.; Sykes, D.A.; Kouam, R.W.; Salven, D.S.; Wang, T.Y.; Mehta, V.A.; Shaffrey, C.I.; Wiggins, W.F.; Chi, J.H.; Abd-El-Barr, M.M. Novel Approach to Percutaneous Lumbar Surgeries via Kambin’s Triangle—Radiographic and Surgical Planning Analysis with Nerve Segmentation Technology. World Neurosurg. 2023, 177, e385–e396. [Google Scholar] [CrossRef]
- Khalifeh, J.M.; Dibble, C.F.; Stecher, P.; Dorward, I.; Hawasli, A.H.; Ray, W.Z. Transfacet Minimally Invasive Transforaminal Lumbar Interbody Fusion With an Expandable Interbody Device—Part II: Consecutive Case Series. Oper. Neurosurg. 2020, 19, 518–529. [Google Scholar] [CrossRef]
- Abbasi, H.; Storlie, N.R.; Aya, K.L. Transfacet Oblique Lateral Lumbar Interbody Fusion: Technical Description and Early Results. Cureus 2022, 14, e26533. [Google Scholar] [CrossRef]
- Hiepe, P. Cranial Distortion Correction-Technical Background. 2017. Available online: https://www.researchgate.net/publication/317359164_Cranial_Distortion_Correction_-_Technical_Background?channel=doi&linkId=593694aeaca272fc55739a28&showFulltext=true (accessed on 28 December 2023).
- Godzik, J.; Farber, S.H.; Urakov, T.; Steinberger, J.; Knipscher, L.J.; Ehredt, R.B.; Tumialán, L.M.; Uribe, J.S. “Disruptive Technology” in Spine Surgery and Education: Virtual and Augmented Reality. Oper. Neurosurg. 2021, 21 (Suppl. S1), S85–S93. [Google Scholar] [CrossRef]
- Yuk, F.J.; Maragkos, G.A.; Sato, K.; Steinberger, J. Current innovation in virtual and augmented reality in spine surgery. Ann. Transl. Med. 2021, 9, 94. [Google Scholar] [CrossRef]
- Rush, A.J.; Shepard, N.; Nolte, M.; Siemionow, K.; Phillips, F. Augmented Reality in Spine Surgery: Current State of the Art. Int. J. Spine Surg. 2022, 16, S22–S27. [Google Scholar] [CrossRef] [PubMed]
- Butler, A.J.; Colman, M.W.; Lynch, J.; Phillips, F.M. Augmented reality in minimally invasive spine surgery: Early efficiency and complications of percutaneous pedicle screw instrumentation. Spine J. 2023, 23, 27–33. [Google Scholar] [CrossRef]
- Burström, G.; Persson, O.; Edström, E.; Elmi-Terander, A. Augmented reality navigation in spine surgery: A systematic review. Acta Neurochir. 2021, 163, 843–852. [Google Scholar] [CrossRef] [PubMed]
- Charles, Y.P.; Cazzato, R.L.; Nachabe, R.; Chatterjea, A.; Steib, J.P.; Gangi, A. Minimally Invasive Transforaminal Lumbar Interbody Fusion Using Augmented Reality Surgical Navigation for Percutaneous Pedicle Screw Placement. Clin. Spine Surg. 2021; ahead of print. [Google Scholar] [CrossRef]
- Sommer, F.; Hussain, I.; Kirnaz, S.; Goldberg, J.L.; Navarro-Ramirez, R.; McGrath, L.B., Jr.; Schmidt, F.A.; Medary, B.; Gadjradj, P.S.; Härtl, R. Augmented Reality to Improve Surgical Workflow in Minimally Invasive Transforaminal Lumbar Interbody Fusion—A Feasibility Study with Case Series. Neurospine 2022, 19, 574–585. [Google Scholar] [CrossRef] [PubMed]
- Jamshidi, A.M.; Makler, V.; Wang, M.Y. Augmented Reality Assisted Endoscopic Transforaminal Lumbar Interbody Fusion: 2-Dimensional Operative Video. Oper. Neurosurg. 2021, 21, E563–E564. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Mou, L.; Yan, Q.; Ma, S.; Yue, X.; Zhou, S.; Lin, Z.; Zhang, J.; Liu, J.; Zhao, Y. Automated Segmentation of Trigeminal Nerve and Cerebrovasculature in MR-Angiography Images by Deep Learning. Front. Neurosci. 2021, 15, 744967. [Google Scholar] [CrossRef] [PubMed]
- Gare, B.M.; Hudson, T.; Rohani, S.A.; Allen, D.G.; Agrawal, S.K.; Ladak, H.M. Multi-atlas segmentation of the facial nerve from clinical CT for virtual reality simulators. Int. J. Comput. Assist. Radiol. Surg. 2020, 15, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Fan, G.; Liu, H.; Wang, D.; Feng, C.; Li, Y.; Yin, B.; Zhou, Z.; Gu, X.; Zhang, H.; Lu, Y.; et al. Deep learning-based lumbosacral reconstruction for difficulty prediction of percutaneous endoscopic transforaminal discectomy at L5/S1 level: A retrospective cohort study. Int. J. Surg. 2020, 82, 162–169. [Google Scholar] [CrossRef]
- Choi, I.; Ahn, J.O.; So, W.S.; Lee, S.J.; Choi, I.J.; Kim, H. Exiting root injury in transforaminal endoscopic discectomy: Preoperative image considerations for safety. Eur. Spine J. 2013, 22, 2481–2487. [Google Scholar] [CrossRef]
- Shen, X.; Gao, Y.C.; Zhang, P.; Xuan, W.B.; Song, P.; Gao, Z.X. Transfacet Full-Endoscopic Posterior Lumbar Interbody Fusion for Lumbar Degenerative Diseases: Consecutive Case Series. 2023. Available online: https://assets.researchsquare.com/files/rs-3209596/v1/3f4381c9-256a-411e-9ae2-84598b7ba51d.pdf?c=1690995537 (accessed on 28 December 2023).







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bardeesi, A.; Tabarestani, T.Q.; Bergin, S.M.; Huang, C.-C.; Shaffrey, C.I.; Wiggins, W.F.; Abd-El-Barr, M.M. Using Augmented Reality Technology to Optimize Transfacet Lumbar Interbody Fusion: A Case Report. J. Clin. Med. 2024, 13, 1513. https://doi.org/10.3390/jcm13051513
Bardeesi A, Tabarestani TQ, Bergin SM, Huang C-C, Shaffrey CI, Wiggins WF, Abd-El-Barr MM. Using Augmented Reality Technology to Optimize Transfacet Lumbar Interbody Fusion: A Case Report. Journal of Clinical Medicine. 2024; 13(5):1513. https://doi.org/10.3390/jcm13051513
Chicago/Turabian StyleBardeesi, Anas, Troy Q. Tabarestani, Stephen M. Bergin, Chuan-Ching Huang, Christopher I. Shaffrey, Walter F. Wiggins, and Muhammad M. Abd-El-Barr. 2024. "Using Augmented Reality Technology to Optimize Transfacet Lumbar Interbody Fusion: A Case Report" Journal of Clinical Medicine 13, no. 5: 1513. https://doi.org/10.3390/jcm13051513