
Who Can Be Discharged Home after Adult Spinal Deformity Surgery?
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Selection
2.3. Independent Variables
2.4. Outcome Variables
2.5. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Intraoperative and Perioperative Factors
3.3. Radiographic Factors
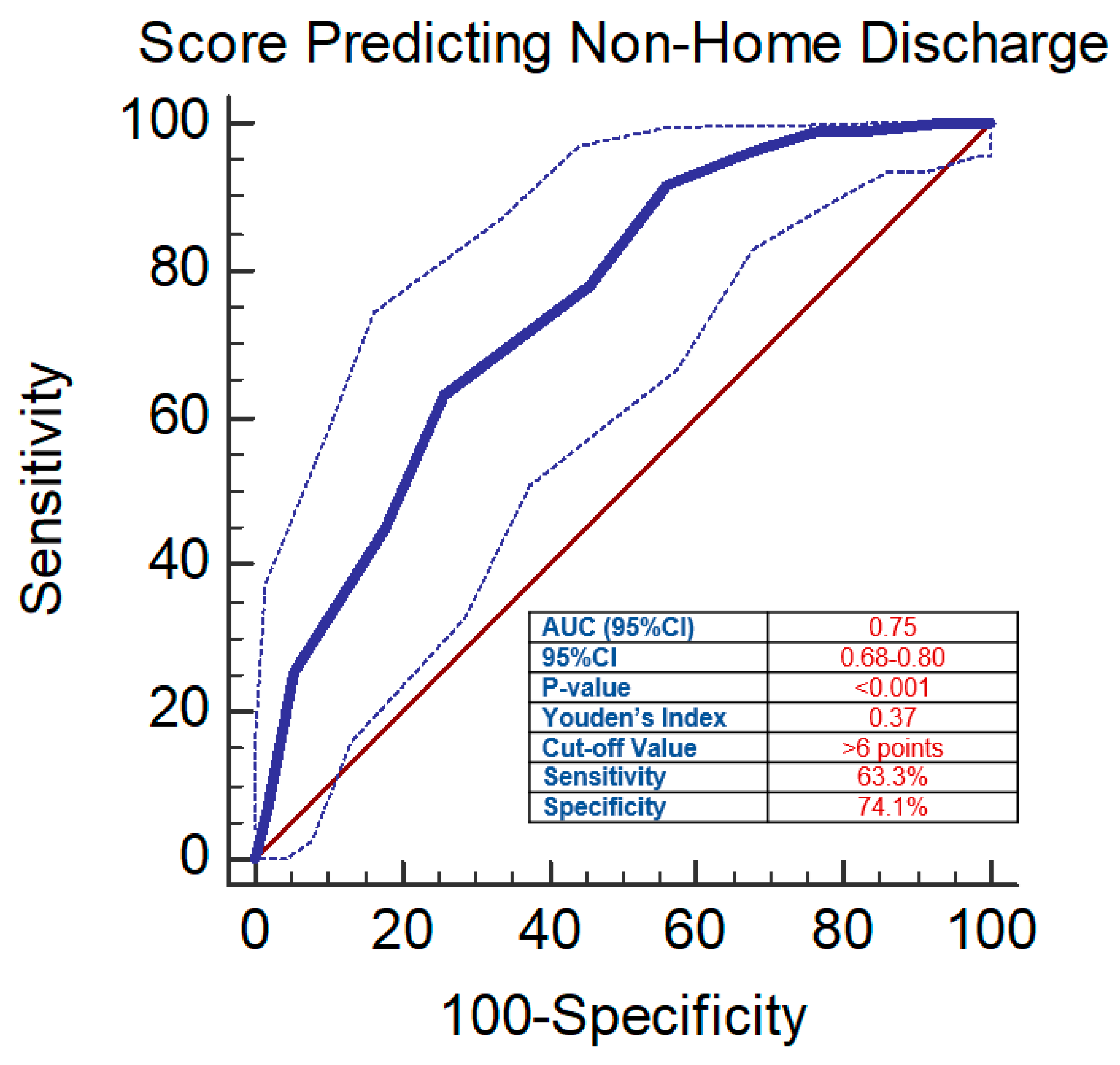
3.4. Scoring System
3.5. Patient-Reported Outcome Measures
3.6. Subanalysis of SNF vs. IPR
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cerpa, M.; Lenke, L.G.; Fehlings, M.G.; Shaffrey, C.I.; Cheung, K.M.C.; Carreon, L.Y. Evolution and Advancement of Adult Spinal Deformity Research and Clinical Care: An Overview of the Scoli-RISK-1 Study. Glob. Spine J. 2019, 9, 8S–14S. [Google Scholar] [CrossRef] [PubMed]
- Safaee, M.M.; Ames, C.P.; Smith, J.S. Epidemiology and Socioeconomic Trends in Adult Spinal Deformity Care. Neurosurgery 2020, 87, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Riley, M.S.; Bridwell, K.H.; Lenke, L.G.; Dalton, J.; Kelly, M.P. Health-related quality of life outcomes in complex adult spinal deformity surgery. J. Neurosurg. Spine 2018, 28, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Daubs, M.D.; Lenke, L.G.; Cheh, G.; Stobbs, G.; Bridwell, K.H. Adult Spinal Deformity Surgery: Complications and Outcomes in Patients Over Age 60. Spine 2007, 32, 2238–2244. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, G.; Boissiere, L.; Larrieu, D.; Bourghli, A.; Vital, J.M.; Gille, O.; Pointillart, V.; Challier, V.; Mariey, R.; Pellisé, F.; et al. Advantages and Disadvantages of Adult Spinal Deformity Surgery and Its Impact on Health-Related Quality of Life. Spine 2017, 42, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Scheer, J.K.; Mundis, G.M.; Klineberg, E.; Hart, R.A.; Deviren, V.; Nguyen, S.; Protopsaltis, T.S.; Gupta, M.; Bess, S.; Shaffrey, C.I.; et al. Postoperative Recovery after Adult Spinal Deformity Surgery: Comparative Analysis of Age in 149 Patients during 2-year Follow-up. Spine 2015, 40, 1505–1515. [Google Scholar] [CrossRef] [PubMed]
- Passias, P.G.; Poorman, G.W.; Bortz, C.A.; Qureshi, R.; Diebo, B.G.; Paul, J.C.; Horn, S.R.; Segreto, F.A.; Pyne, A.; Jalai, C.M.; et al. Predictors of adverse discharge disposition in adult spinal deformity and associated costs. Spine J. 2018, 18, 1845–1852. [Google Scholar] [CrossRef] [PubMed]
- Amin, R.M.; Raad, M.; Jain, A.; Khashan, M.; Hassanzadeh, H.; Frank, S.M.; Kebaish, K.M. Risk factors for nonroutine discharge in adult spinal deformity surgery. Spine J. 2019, 19, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Theologis, A.A.; Lau, D.; Dalle-Ore, C.; Tsu, A.; Deviren, V.; Ames, C.P. Costs and utility of post-discharge acute inpatient rehabilitation following adult spinal deformity surgery. Spine Deform. 2021, 9, 817–822. [Google Scholar] [CrossRef] [PubMed]
- Di Capua, J.; Somani, S.; Lugo-Fagundo, N.; Kim, J.S.; Phan, K.; Lee, N.J.; Kothari, P.; Shin, J.; Cho, S.K. Predictors for Non-Home Patient Discharge Following Elective Adult Spinal Deformity Surgery. Glob. Spine J. 2018, 8, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Eastlack, R.K.; Ledesma, J.B.; Tran, S.; Khalsa, A.; Park, P.; Mummaneni, P.V.; Chou, D.; Kanter, A.S.; Anand, N.; Nunley, P.; et al. Home Versus Rehabilitation: Factors that Influence Disposition After Minimally Invasive Surgery in Adult Spinal Deformity Surgery. World Neurosurg. 2018, 118, e610–e615. [Google Scholar] [CrossRef] [PubMed]
- Stephens, B.F.; Khan, I.; Chotai, S.; Sivaganesan, A.; Devin, C.J. Drivers of Cost in Adult Thoracolumbar Spine Deformity Surgery. World Neurosurg. 2018, 118, e206–e211. [Google Scholar] [CrossRef] [PubMed]
- Montoya, A.; Mody, L.; Sanroma, P.; Muñoz, P.; Mirón-Rubio, M.; Aguilera, A.; Estrada, O.; García, D.; González-Ramallo, V.J.; Pajarón, M.; et al. Common infections in nursing homes: A review of current issues and challenges. Aging Health 2011, 7, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.S.; Ha, J.-K.; Kim, D.G.; Kim, H.; Hwang, C.J.; Lee, D.-H.; Cho, J.H. The clinical importance of sacral slanting in patients with adolescent idiopathic scoliosis undergoing surgery. Spine J. 2015, 15, 834–840. [Google Scholar] [CrossRef] [PubMed]
- Roussouly, P.; Gollogly, S.; Berthonnaud, E.; Dimnet, J. Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine 2005, 30, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Fairbank, J.C.; Couper, J.; Davies, J.B.; O’Brien, J.P. The Oswestry low back pain disability questionnaire. Physiotherapy 1980, 66, 271–273. [Google Scholar] [PubMed]
- The EuroQol Group. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Total Cohort n = 221 | Home Discharge n = 112 | Non-Home Discharge n = 109 | p-Value | |
|---|---|---|---|---|---|
| Preoperative | |||||
| Age, mean ± SD | 63.6 ± 17.6 | 55.7 ± 20.1 | 71.8 ± 9.1 | <0.001 | |
| Female, n (%) | 167 (75.6%) | 83 (74.1%) | 84 (77.1%) | 0.262 | |
| BMI, mean ± SD | 28.9 ± 7.0 | 28.3 ± 7.6 | 29.4 ± 6.3 | 0.088 | |
| Comorbidities, n (%) | 0 | 44 (19.9%) | 33 (29.5%) | 11 (10.1%) | 0.001 |
| 1 | 85 (38.5%) | 36 (32.1%) | 49 (45.0%) | ||
| 2+ | 92 (41.6%) | 43 (38.4%) | 49 (45.0%) | ||
| Diabetes, n (%) | 41 (18.6%) | 17 (15.2%) | 24 (22.0%) | 0.191 | |
| COPD, n (%) | 61 (27.6%) | 31 (27.7%) | 30 (27.5%) | 0.979 | |
| CHF, n (%) | 32 (14.5%) | 13 (11.6%) | 19 (17.4%) | 0.219 | |
| HTN, n (%) | 146 (66.1%) | 64 (57.1%) | 82 (75.2%) | 0.005 | |
| Osteoporosis, n (%) | 43 (24.7%) | 17 (18.9%) | 26 (31.0%) | 0.065 | |
| Prior fusion, n (%) | 77 (34.8%) | 35 (31.2%) | 42 (38.5%) | 0.256 | |
| Intraoperative | |||||
| Total instrumented levels, mean ± SD | 10.5 ± 3.2 | 10.0 ± 3.0 | 11.0 ± 3.4 | 0.030 | |
| Interbody graft at any level, n (%) | 62 (28.0%) | 34 (30.4%) | 28 (25.7%) | 0.127 | |
| Operative time, min, mean ± SD | 421.1 ± 150.0 | 381.4 ± 139.9 | 461.6 ± 149.8 | <0.001 | |
| EBL, mL, mean ± SD | 1416.0 ± 1207.0 | 1101.0 ± 977.8 | 1739.7 ± 1332.9 | <0.001 | |
| LOS, days, mean ± SD | 7.3 ± 10.1 | 5.4 ± 2.8 | 9.3 ± 13.9 | <0.001 | |
| 2-year Postoperative | |||||
| ODI, mean ± SD | 35.2 ± 19.7 | 32.5 ± 22.3 | 37.1 ± 17.4 | 0.158 | |
| NRS-Back pain, mean ± SD | 4.8 ± 2.9 | 4.6 ± 3.0 | 5.0 ± 2.9 | 0.459 | |
| NRS-Leg pain, mean ± SD | 2.8 ± 3.3 | 2.2 ± 2.9 | 3.2 ± 3.4 | 0.092 | |
| EQ-5D, mean ± SD | 0.7 ± 0.2 | 0.7 ± 0.2 | 0.7 ± 0.2 | 0.134 | |
| Univariate | |||
|---|---|---|---|
| Outcome Variable | Independent Variable | OR (95%CI) | p-Value |
| Non-home discharge | Age | 1.10 (1.05–1.12) | <0.001 |
| Comorbidities (2+) | 1.60 (1.11–2.28) | 0.011 | |
| HTN | 2.30 (1.28–4.04) | 0.005 | |
| TIL | 1.09 (1.005–1.19) | 0.037 | |
| Operative time, min | 1.004 (1.002–1.01) | <0.001 | |
| EBL | 1.001 (1.00–1.001) | <0.001 | |
| Preop SVA | 1.01 (1.005–1.014) | <0.001 | |
| Preop PT | 1.03 (1.01–1.06) | 0.007 | |
| Preop T1PA | 1.04 (1.02–1.06) | <0.001 | |
| Predictors of Non-Home Discharge | AUC (95%CI) | Youden’s Index | Cutoff Value | p-Value |
|---|---|---|---|---|
| Age | 0.75 (0.69–0.80) | 0.36 | >56 years | <0.001 |
| TIL | 0.58 (0.51–0.65) | 0.13 | >10 levels | 0.027 |
| Operative time, min | 0.68 (0.62–0.74) | 0.38 | >357 min | <0.001 |
| EBL | 0.67 (0.61–0.73) | 0.28 | >1200 mL | <0.001 |
| Preop SVA | 0.66 (0.59–0.72) | 0.28 | >6.6 cm | <0.001 |
| Preop PT | 0.58 (0.51–0.65) | 0.14 | >33.6° | 0.025 |
| Preop T1PA | 0.64 (0.58–0.71) | 0.23 | >15° | >0.001 |
| Predictors of Non-Home Discharge | Score (10 Points) |
|---|---|
| Age > 56 years | 1 |
| Comorbidities (2+) | 1 |
| Hypertension | 2 |
| TIL > 10 levels | 1 |
| Operative time, > 357 min | 1 |
| EBL > 1200 mL | 1 |
| Preop SVA > 6.6 cm | 1 |
| Preop PT > 33.6° | 1 |
| Preop T1PA > 15° | 1 |
| Validation | |
| Logistic regression | OR = 1.55, 95%CI = 1.34–1.78, p < 0.001 |
| AUC (95%CI) | AUC = 0.75, 95%CI = 0.68–0.80, p < 0.001 |
| Youden’s Index | 0.37 |
| Cut-off value | 6 points |
| Score > 6 | More likely to be discharged to IPR/SNF |
| Score ≤ 6 | More likely to be discharged home |
| Sensitivity | 63.3% |
| Specificity | 74.1% |
| Variables | Non-Home Discharge n = 109 | IPR (n = 71) | SNF (n = 38) | p-Value | |
|---|---|---|---|---|---|
| Preoperative | |||||
| Age, mean ± SD | 71.8 ± 9.1 | 70.4 ± 9.1 | 74.4 ± 8.6 | 0.029 | |
| Female, n (%) | 84 (77.1%) | 50 (70.4%) | 34 (89.5%) | 0.024 | |
| BMI, mean ± SD | 29.4 ± 6.3 | 28.9 ± 6.0 | 30.4 ± 6.8 | 0.283 | |
| Comorbidities, n (%) | 0 | 11 (10.1%) | 6 (8.5%) | 5 (13.2%) | 0.738 |
| 1 | 49 (45.0%) | 32 (45.1%) | 17 (44.7%) | ||
| 2+ | 49 (45.0%) | 33 (46.5%) | 16 (42.1%) | ||
| Diabetes, n (%) | 24 (22.0%) | 16 (22.5%) | 8 (21.1%) | 0.859 | |
| COPD, n (%) | 30 (27.5%) | 20 (28.2%) | 10 (26.3%) | 0.836 | |
| CHF, n (%) | 19 (17.4%) | 14 (19.7%) | 5 (13.2%) | 0.39 | |
| HTN, n (%) | 82 (75.2%) | 53 (74.6%) | 29 (76.3%) | 0.848 | |
| Osteoporosis, n (%) | 26 (31.0%) | 16 (29.6%) | 10 (33.3%) | 0.725 | |
| Prior fusion, n (%) | 42 (38.5%) | 27 (38.0%) | 15 (39.5%) | 0.885 | |
| Intraoperative | |||||
| Total instrumented levels, mean ± SD | 11.0 ± 3.4 | 10.9 ± 3.6 | 11.0 ± 2.9 | 0.761 | |
| Interbody graft at any level, n (%) | 28 (25.7%) | ||||
| Operative time, min, mean ± SD | 461.6 ± 149.8 | 465.7 ± 158.3 | 453.9 ± 134.3 | 0.954 | |
| EBL, mL, mean ± SD | 1739.7 ± 1332.9 | 1658.2 ± 1226.9 | 1892.1 ± 1517.0 | 0.661 | |
| LOS, days, mean ± SD | 5.4 ± 2.8 | 8.6 ± 8.5 | 10.5 ± 20.5 | 0.664 | |
| 2-year Postoperative | |||||
| ODI, mean ± SD | 37.1 ± 17.4 | 39.9 ± 18.3 | 32.2 ± 14.8 | 0.098 | |
| NRS—Back pain, mean ± SD | 5.0 ± 2.9 | 5.4 ± 2.9 | 4.1 ± 2.8 | 0.065 | |
| NRS—Leg pain, mean ± SD | 3.2 ± 3.4 | 3.7 ± 3.5 | 2.4 ± 3.2 | 0.158 | |
| EQ-5D, mean ± SD | 0.7 ± 0.2 | 0.6 ± 0.2 | 0.8 ± 0.1 | 0.011 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jonzzon, S.; Chanbour, H.; Johnson, G.W.; Chen, J.W.; Metcalf, T.; Lyons, A.T.; Younus, I.; Liles, C.; Abtahi, A.M.; Stephens, B.F.; et al. Who Can Be Discharged Home after Adult Spinal Deformity Surgery? J. Clin. Med. 2024, 13, 1340. https://doi.org/10.3390/jcm13051340
Jonzzon S, Chanbour H, Johnson GW, Chen JW, Metcalf T, Lyons AT, Younus I, Liles C, Abtahi AM, Stephens BF, et al. Who Can Be Discharged Home after Adult Spinal Deformity Surgery? Journal of Clinical Medicine. 2024; 13(5):1340. https://doi.org/10.3390/jcm13051340
Chicago/Turabian StyleJonzzon, Soren, Hani Chanbour, Graham W. Johnson, Jeffrey W. Chen, Tyler Metcalf, Alexander T. Lyons, Iyan Younus, Campbell Liles, Amir M. Abtahi, Byron F. Stephens, and et al. 2024. "Who Can Be Discharged Home after Adult Spinal Deformity Surgery?" Journal of Clinical Medicine 13, no. 5: 1340. https://doi.org/10.3390/jcm13051340