
Long-Term Functional Limitations on Cardiopulmonary Exercise Testing in Emotion-Triggered Takotsubo Syndrome
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cardiopulmonary Exercise Test
2.2. Statistical Analysis
3. Results
4. Discussion
Study Limitations
5. Future Perspectives
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TTS | Tako-tsubo syndrome |
| AMI | Acute myocardial infarction |
| LVEF | Left ventricular ejection fraction |
| CMR | Cardiac magnetic resonance |
| CPET | Cardiopulmonary exercise testing |
| E-TTS | Emotions-triggered Tako-tsubo syndrome |
| GEIST | German-Italian-Spanish Tako-tsubo registry |
| RER | Respiratory exchange ratio |
| VO2 | Oxygen uptake |
| VCO2 | Carbon dioxide output |
| VE | minute ventilation |
| PETCO2 | end-tidal carbon dioxide partial spressure |
| HR | heart rate |
| VO2/HR | oxygen pulse |
| VCP | Ventilatory compensation point |
| MVV | maximum voluntary ventilation |
| AT | anaerobic threshold |
| HF | heart failure |
| HFrEF | heart failure with reduced ejection fraction |
References
- Templin, C.; Ghadri, J.R.; Diekmann, J.; Napp, L.C.; Bataiosu, D.R.; Jaguszewski, M.; Cammann, V.L.; Sarcon, A.; Geyer, V.; Neumann, C.A.; et al. Clinical Features and Outcomes of Takotsubo (Stress) Cardiomyopathy. N. Engl. J. Med. 2015, 373, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Eitel, I.; von Knobelsdorff-Brenkenhoff, F.; Bernhardt, P.; Carbone, I.; Muellerleile, K.; Aldrovandi, A.; Francone, M.; Desch, S.; Gutberlet, M.; Strohm, O.; et al. Clinical characteristics and cardiovascular magnetic resonance findings in stress (takotsubo) cardiomyopathy. JAMA 2011, 306, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Arcari, L.; Camastra, G.; Ciolina, F.; Limite, L.R.; Danti, M.; Sclafani, M.; Ansalone, G.; Musumeci, M.B.; Nagel, E.; Puntmann, V.; et al. Myocardial oedema contributes to interstitial expansion and associates with mechanical and electrocardiographic changes in takotsubo syndrome: A CMR T1 and T2 mapping study. Eur. Heart J. Cardiovasc. Imaging 2023, 24, 1082–1091. [Google Scholar] [CrossRef] [PubMed]
- Scally, C.; Rudd, A.; Mezincescu, A.; Wilson, H.; Srivanasan, J.; Horgan, G.; Broadhurst, P.; Newby, D.E.; Henning, A.; Dawson, D.K. Persistent Long-Term Structural, Functional, and Metabolic Changes After Stress-Induced (Takotsubo) Cardiomyopathy. Circulation 2018, 137, 1039–1048. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, K.; Ahearn, T.; Srinivasan, J.; Neil, C.J.; Scally, C.; Rudd, A.; Jagpal, B.; Frenneaux, M.P.; Pislaru, C.; Horowitz, J.D.; et al. Alterations in cardiac deformation, timing of contraction and relaxation, and early myocardial fibrosis accompany the apparent recovery of acute stress-induced (takotsubo) cardiomyopathy: An end to the concept of transience. J. Am. Soc. Echocardiogr. 2017, 30, 745–755. [Google Scholar] [CrossRef] [PubMed]
- Uribarri, A.; Núñez-Gil, I.J.; Conty, D.; Vedia, O.; Almendro-Delia, M.; Duran Cambra, A.; Martin-Garcia, A.C.; Barrionuevo-Sánchez, M.; Martínez-Sellés, M.; Raposeiras-Roubín, S.; et al. Short- and long-term prognosis of patients with Takotsubo Syndrome based on different triggers: Importance of the physical nature. J. Am. Heart Assoc. 2019, 8, e013701. [Google Scholar] [CrossRef]
- Ghadri, J.R.; Kato, K.; Cammann, V.L.; Gili, S.; Jurisic, S.; Di Vece, D.; Candreva, A.; Ding, K.J.; Micek, J.; Szawan, K.A.; et al. Long-term prognosis of patients with Takotsubo syndrome. J. Am. Coll. Cardiol. 2018, 72, 874–882. [Google Scholar] [CrossRef] [PubMed]
- Arcari, L.; Cacciotti, L.; Limite, L.R.; Russo, D.; Sclafani, M.; Semeraro, R.; Ansalone, G.; Volpe, M.; Autore, C.; Musumeci, M.B. Clinical characteristics of patients with takotsubo syndrome recurrence: An observational study with long-term follow-up. Int. J. Cardiol. 2021, 329, 23–27. [Google Scholar] [CrossRef]
- Scudiero, F.; Arcari, L.; Cacciotti, L.; De Vito, E.; Marcucci, R.; Passaseo, I.; Limite, L.R.; Musumeci, M.B.; Autore, C.; Citro, R.; et al. Prognostic relevance of GRACE risk score in Takotsubo syndrome. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 721–728. [Google Scholar] [CrossRef]
- Looi, J.L.; Verryt, T.; McLeod, P.; Chan, C.; Pemberton, J.; Webster, M.; To, A.; Lee, M.; Kerr, A.J. Type of Stressor and Medium-Term Outcomes After Takotsubo Syndrome: What Becomes of the Broken Hearted? (ANZACS-QI 59). Heart Lung Circ. 2022, 31, 499–507. [Google Scholar] [CrossRef]
- Laveneziana, P.; Di Paolo, M.; Palange, P. The clinical value of cardiopulmonary exercise testing in the modern era. Eur. Respir. Rev. 2021, 30, 200187. [Google Scholar] [CrossRef]
- Badagliacca, R.; Rischard, F.; Giudice, F.L.; Howard, L.; Papa, S.; Valli, G.; Manzi, G.; Sciomer, S.; Palange, P.; Garcia, J.G.N.; et al. Incremental value of cardiopulmonary exercise testing in intermediate-risk pulmonary arterial hypertension. J. Heart Lung Transplant. 2022, 41, 780–790. [Google Scholar] [CrossRef]
- Ghio, S.; Acquaro, M.; Agostoni, P.; Ambrosio, G.; Carluccio, E.; Castiglione, V.; Colombo, D.; D’Alto, M.; Delle Grottaglie, S.; Dini, F.L.; et al. Right heart failure in left heart disease: Imaging, functional, and biochemical aspects of right ventricular dysfunction. Heart Fail. Rev. 2023, 28, 1009–1022. [Google Scholar] [CrossRef]
- Guazzi, M.; Bandera, F.; Ozemek, C.; Systrom, D.; Arena, R. Cardiopulmonary Exercise Testing: What Is its Value? J. Am. Coll. Cardiol. 2017, 70, 1618–1636. [Google Scholar] [CrossRef]
- Arcari, L.; Núñez Gil, I.J.; Stiermaier, T.; El-Battrawy, I.; Guerra, F.; Novo, G.; Musumeci, M.B.; Cacciotti, L.; Mariano, E.; Caldarola, P.; et al. Gender Differences in Takotsubo Syndrome. J. Am. Coll. Cardiol. 2022, 79, 2085–2093. [Google Scholar] [CrossRef]
- Pätz, T.; Santoro, F.; Cetera, R.; Ragnatela, I.; El-Battrawy, I.; Mezger, M.; Rawish, E.; Andrés-Villarreal, M.; Almendro-Delia, M.; Martinez-Sellés, M.; et al. Trigger-Associated Clinical Implications and Outcomes in Takotsubo Syndrome: Results from the Multicenter GEIST Registry. J. Am. Heart Assoc. 2023, 12, e028511. [Google Scholar] [CrossRef]
- Sclafani, M.; Arcari, L.; Russo, D.; Tini, G.; Limite, L.R.; Cacciotti, L.; Volpe, M.; Autore, C.; Musumeci, M.B. Long-term management of Takotsubo syndrome: A not-so-benign condition. Rev. Cardiovasc. Med. 2021, 22, 597–611. [Google Scholar] [CrossRef]
- Cacciotti, L.; Passaseo, I.; Marazzi, G.; Camastra, G.; Campolongo, G.; Beni, S.; Lupparelli, F.; Ansalone, G. Observational study on Takotsubo-like cardiomyopathy: Clinical features, diagnosis, prognosis and follow-up. BMJ Open 2012, 2, e001165. [Google Scholar] [CrossRef] [PubMed]
- Cramer, S.P. Effects of Beta-Blockers on Maximal Oxygen Consumption. Master’s Theses. 2003. Available online: https://scholarworks.wmich.edu/masters_theses/4681 (accessed on 29 August 2019).
- Sietsema, K.E.; Stringer, W.W.; Sue, D.Y.; Ward, S. Measurements during Integrative Cardiopulmonary Exercise Testing. In Wasserman & Whipp’s Principles of Exercise Testing and Interpretation, 6th ed.; Wolters Kluwer: Alphen aan den Rijn, The Netherlands, 2021; pp. 71–73. [Google Scholar]
- Sietsema, K.E.; Stringer, W.W.; Sue, D.Y.; Ward, S. Approaches to Data Summary and Interpretation. In Wasserman & Whipp’s Principles of Exercise Testing and Interpretation, 6th ed.; Wolters Kluwer: Alphen aan den Rijn, The Netherlands, 2021; pp. 143–144. [Google Scholar]
- Schweiger, V.; Schoenberger, M.; Di Vece, D.; Wuerdinger, M.; Gilhofer, T.; Rajman, K.; Ghadri, J.R.; Cammann, V.L.; Templin, C.; Nierderseer, D. Long-term functional cardiac changes in takotsubo syndrome. Eur. Heart J. 2023, 44, ehad655.2590. [Google Scholar] [CrossRef]
- Wasserman, K.; Zhang, Y.Y.; Gitt, A.; Belardinelli, R.; Koike, A.; Lubarsky, L.; Agostoni, P.G. Lung function and exercise gas exchange in chronic heart failure. Circulation 1997, 96, 2221–2227. [Google Scholar] [CrossRef] [PubMed]
- Sietsema, K.E.; Stringer, W.W.; Sue, D.Y.; Ward, S. Diagnostic Specificity of Exercise Intolerance: A Flowchart Approach. In Wasserman & Whipp’s Principles of Exercise Testing and Interpretation, 6th ed.; Wolters Kluwer: Alphen aan den Rijn, The Netherlands, 2021; pp. 226–227. [Google Scholar]
- Stelken, A.M.; Younis, L.T.; Jennison, S.H.; Miller, D.D.; Miller, L.W.; Shaw, L.J.; Kargl, D.; Chaitman, B.R. Prognostic value of cardiopulmonary exercise testing using percent achieved of predicted peak oxygen uptake for patients with ischemic and dilated cardiomyopathy. J. Am. Coll. Cardiol. 1996, 27, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Chua, T.P.; Ponikowski, P.; Harrington, D.; Anker, S.D.; Webb-Peploe, K.; Clark, A.L.; Poole-Wilson, P.A.; Coats, A.J. Clinical correlates and prognostic significance of the ventilatory response to exercise in chronic heart failure. J. Am. Coll. Cardiol. 1997, 29, 1585–1590. [Google Scholar] [CrossRef] [PubMed]
- Nadruz, W., Jr.; West, E.; Sengeløv, M.; Santos, M.; Groarke, J.D.; Forman, D.E.; Claggett, B.; Skali, H.; Shah, A.M. Prognostic Value of Cardiopulmonary Exercise Testing in Heart Failure with Reduced, Midrange, and Preserved Ejection Fraction. J. Am. Heart Assoc. 2017, 6, e006000. [Google Scholar] [CrossRef]
- Badagliacca, R.; Papa, S.; Poscia, R.; Valli, G.; Pezzuto, B.; Manzi, G.; Torre, R.; Gianfrilli, D.; Sciomer, S.; Palange, P.; et al. The added value of cardiopulmonary exercise testing in the follow-up of pulmonary arterial hypertension. J. Heart Lung Transplant. 2019, 38, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Agostoni, P.; Corrà, U.; Cattadori, G.; Veglia, F.; La Gioia, R.; Scardovi, A.B.; Emdin, M.; Metra, M.; Sinagra, G.; Limongelli, G.; et al. Metabolic exercise test data combined with cardiac and kidney indexes, the MECKI score: A multiparametric approach to heart failure prognosis. Int. J. Cardiol. 2013, 167, 2710–2718. [Google Scholar] [CrossRef]
- Madias, J.E. Takotsubo Cardiomyopathy: Current Treatment. J. Clin. Med. 2021, 10, 3440. [Google Scholar] [CrossRef]
- Santoro, F.; Sharkey, S.; Citro, R.; Miura, T.; Arcari, L.; Urbano-Moral, J.A.; Stiermaier, T.; Nuñez-Gil, I.J.; Silverio, A.; Di Nunno, N.; et al. Beta-blockers and renin-angiotensin system inhibitors for Takotsubo syndrome recurrence: A network meta-analysis. Heart 2023. [Google Scholar] [CrossRef]
- Limite, L.R.; Arcari, L.; Cacciotti, L.; Russo, D.; Musumeci, M.B. Cardiogenic shock in takotsubo syndrome: A clue to unravel what hides behind the curtain? JACC Heart Fail. 2019, 7, 175–176. [Google Scholar] [CrossRef]
- Tini, G.; Arcari, L.; Mistrulli, R.; Follesa, F.; Cianca, A.; Sclafani, M.; Tocci, G.; Spallarossa, P.; Battistoni, A.; Cacciotti, L.; et al. A contemporary update on cancer and takotsubo syndrome. Front. Cardiovasc. Med. 2024, 10, 1301383. [Google Scholar] [CrossRef]
- Zalewska-Adamiec, M.; Małyszko, J.; Bachórzewska-Gajewska, H.; Tomaszuk-Kazberuk, A.; Kożuch, M.; Kralisz, P.; Dobrzycki, S. Takotsubo syndrome and chronic kidney disease: A deadly duet in long-term follow-up. Pol. Arch. Intern. Med. 2018, 128, 518–523. [Google Scholar] [CrossRef]
- Stiermaier, T.; Santoro, F.; El-Battrawy, I.; Möller, C.; Graf, T.; Novo, G.; Santangelo, A.; Mariano, E.; Romeo, F.; Caldarola, P.; et al. Prevalence and Prognostic Impact of Diabetes in Takotsubo Syndrome: Insights from the International, Multicenter GEIST. Regist. Diabetes Care 2018, 41, 1084–1088. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Wang, Y.; Liang, J.; Zuo, X.; Li, Q.; Sherif, A.A.; Zhang, J.; Xu, Y.; Huang, Z.; Dong, M.; et al. Takotsubo syndrome and respiratory diseases: A systematic review. Eur. Heart J. Open 2022, 2, oeac009. [Google Scholar] [CrossRef] [PubMed]
- Rudd, A.E.; Horgan, G.; Khan, H.; Gamble, D.T.; Mcgowan, J.; Sood, A.; Mcgeoch, R.; Irving, J.; Watt, J.; Leslie, S.J.; et al. Cardiovascular and Non-cardiovascular Prescribing and Mortality After Takotsubo—Comparison with Myocardial Infarction and General Population. JACC Adv. 2024. [Google Scholar] [CrossRef]
- Citro, R.; Bellino, M.; Silverio, A. Cardiovascular Mortality in Takotsubo Syndrome: A Mystery Awaiting Solving. JACC Adv. 2024. [Google Scholar] [CrossRef]
- Sun, X.-G.; Hansen, J.E.; Beshai, J.F.; Wasserman, K. Oscillatory breathing and exercise gas exchange abnormalities prognosticate early mortality and morbidity in heart failure. J. Am. Coll. Cardiol. 2010, 55, 1814–1823. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Recovered E-TTS Patients | Matched Control Subjects | p Value | |
|---|---|---|---|
| Peak VO2, mL/min/kg | 17.8 ± 3.6 | 22.1 ± 6.5 | <0.001 |
| % predicted peak VO2 | 76.2 ± 14.1 | 99.9 ± 17.1 | <0.001 |
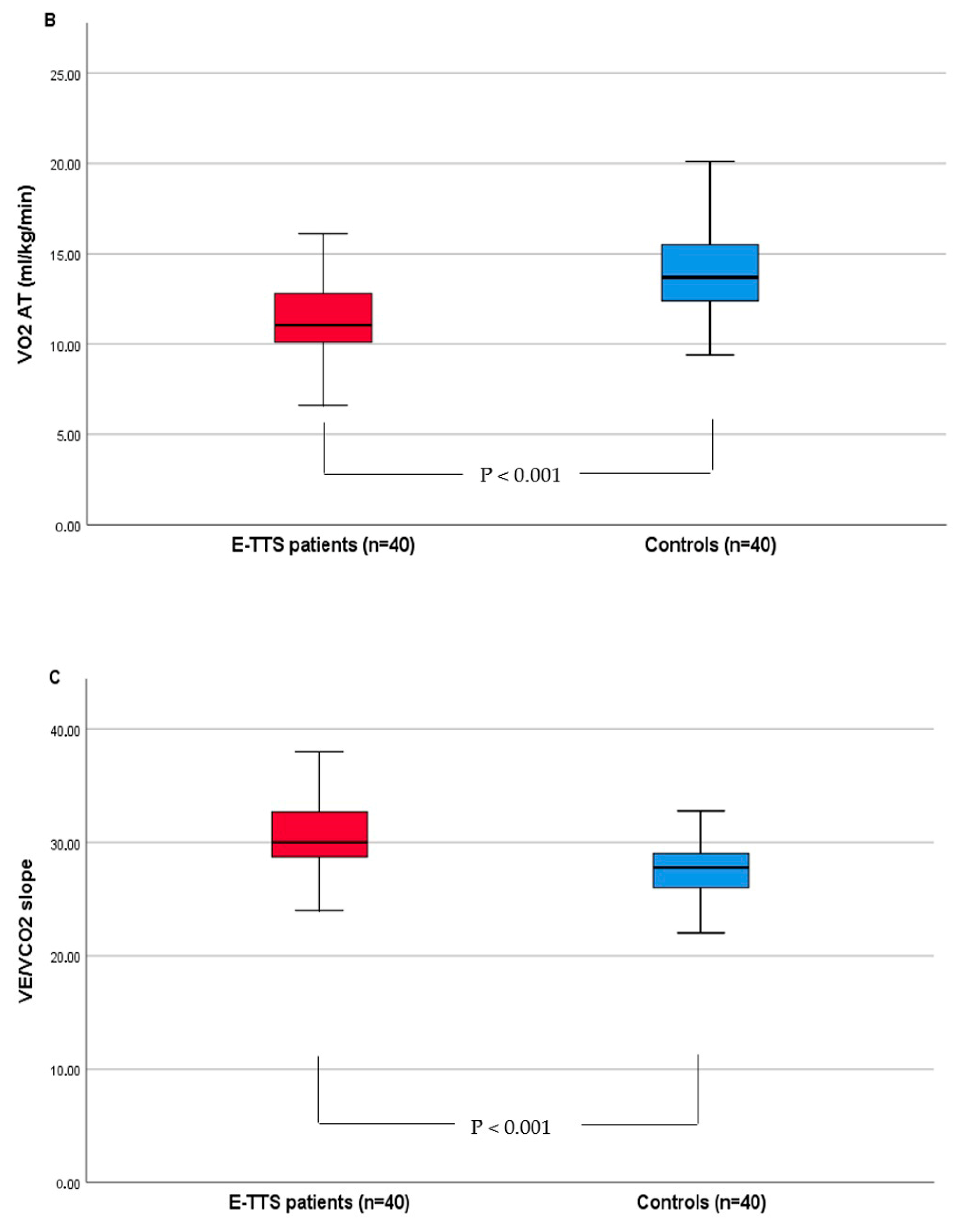
| VO2 at AT, mL/min/kg | 11.5 [10.1–12.9] | 14.4 [12.5–18.7] | <0.001 |
| Peak O2 pulse, mL/beat | 9.8 ± 2.5 | 12.9 ± 3.5 | <0.001 |
| VE/VCO2 slope | 30.5 ± 3.7 | 27.3 ± 3.5 | <0.001 |
| Heart Rate Reserve, beats | 33.3 ± 19.4 | 26.5 ± 13.8 | 0.07 |
| Resting systolic BP, mmHg | 120 [110–130] | 120 [110–130] | 0.98 |
| Resting diastolic BP, mmHg | 80 [70–80] | 80 [70–90] | 0.21 |
| Peak systolic BP, mmHg | 165 [160–180] | 170 [160–180] | 0.46 |
| Peak diastolic BP, mmHg | 100 [90–100] | 100 [90–100] | 0.30 |
| Peak PetCO2, mmHg | 36 ± 4 | 37 ± 5 | 0.40 |
| RER | 1.12 [1.1–1.19] | 1.13 [1.1–1.2] | 0.60 |
| Patients with Prior E-TTS (40) | Control Subjects (40) | p | |
|---|---|---|---|
| Age, y (Mean ± SD) | 65.2 ± 10.6 | 64 ± 11.3 | 0.59 |
| BMI, kg/m2 | 23.6 ± 3.5 | 23.8 ± 2.6 | 0.79 |
| Female, n (%) | 34 (85) | 34 (85) | >0.99 |
| Time since acute TTS event (months) | 30 (12–40) | - | - |
| Comorbidities | |||
| Hypertension, n (%) | 15 (37) | 11(27) | 0.33 |
| Dyslipidemia, n (%) | 13 (37) | 11 (27) | 0.34 |
| Diabetes mellitus, n (%) | 6 (15) | 4 (10) | 0.72 |
| Current smoker, n (%) | 2 (5) | 1 (2) | 0.55 |
| Psychiatric disease | 2 (5) | 0 | 0.32 |
| History of cancer | 2 (5) | 0 | 0.32 |
| Medications | |||
| Beta-blocker | 23 (57) | 16 (40) | 0.11 |
| ARBs/ACE inhibitors | 22 (55) | 13 (32) | 0.056 |
| Statin | 14 (35) | 9 (22) | 0.21 |
| Echocardiography | |||
| LVEF, % | 60 [55–60] | 60 [55–65] | 0.66 |
| Acute E-TTS Event | |
|---|---|
| LV ballooning type, n (%) | |
| Apical | 36 (90) |
| Midventricular | 4 (10) |
| ECG on admission | |
| ST elevation, n (%) | 26 (65) |
| ST depression, n (%) | 6 (15) |
| Negative T wave, n (%) | 7 (17) |
| Presenting symptoms | |
| Angina | 33 (82) |
| Dyspnea | 5 (13) |
| Echocardiography at presentation | |
| Left ventricular EF% (Mean ± SD) | 41 ± 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jabbour, J.P.; Arcari, L.; Cacciotti, L.; Magrì, D.; Recchioni, T.; Valeri, L.; Maggio, E.; Vizza, C.D.; Badagliacca, R.; Papa, S. Long-Term Functional Limitations on Cardiopulmonary Exercise Testing in Emotion-Triggered Takotsubo Syndrome. J. Clin. Med. 2024, 13, 1163. https://doi.org/10.3390/jcm13041163
Jabbour JP, Arcari L, Cacciotti L, Magrì D, Recchioni T, Valeri L, Maggio E, Vizza CD, Badagliacca R, Papa S. Long-Term Functional Limitations on Cardiopulmonary Exercise Testing in Emotion-Triggered Takotsubo Syndrome. Journal of Clinical Medicine. 2024; 13(4):1163. https://doi.org/10.3390/jcm13041163
Chicago/Turabian StyleJabbour, Jean Pierre, Luca Arcari, Luca Cacciotti, Damiano Magrì, Tommaso Recchioni, Livia Valeri, Enrico Maggio, Carmine Dario Vizza, Roberto Badagliacca, and Silvia Papa. 2024. "Long-Term Functional Limitations on Cardiopulmonary Exercise Testing in Emotion-Triggered Takotsubo Syndrome" Journal of Clinical Medicine 13, no. 4: 1163. https://doi.org/10.3390/jcm13041163