
Systemic Congestion as a Determinant of Efficacy in Adaptive Servo-Ventilation Therapy: A Retrospective Observational Study


Abstract
:1. Background
2. Methods
2.1. Patient Selection
2.2. Definition of Heart Failure
2.3. Study Protocol
2.4. PV Estimation
2.5. ASV Therapy
2.6. Mid-Term Clinical Data
2.7. Statistical Analyses
3. Results
3.1. Baseline Characteristics
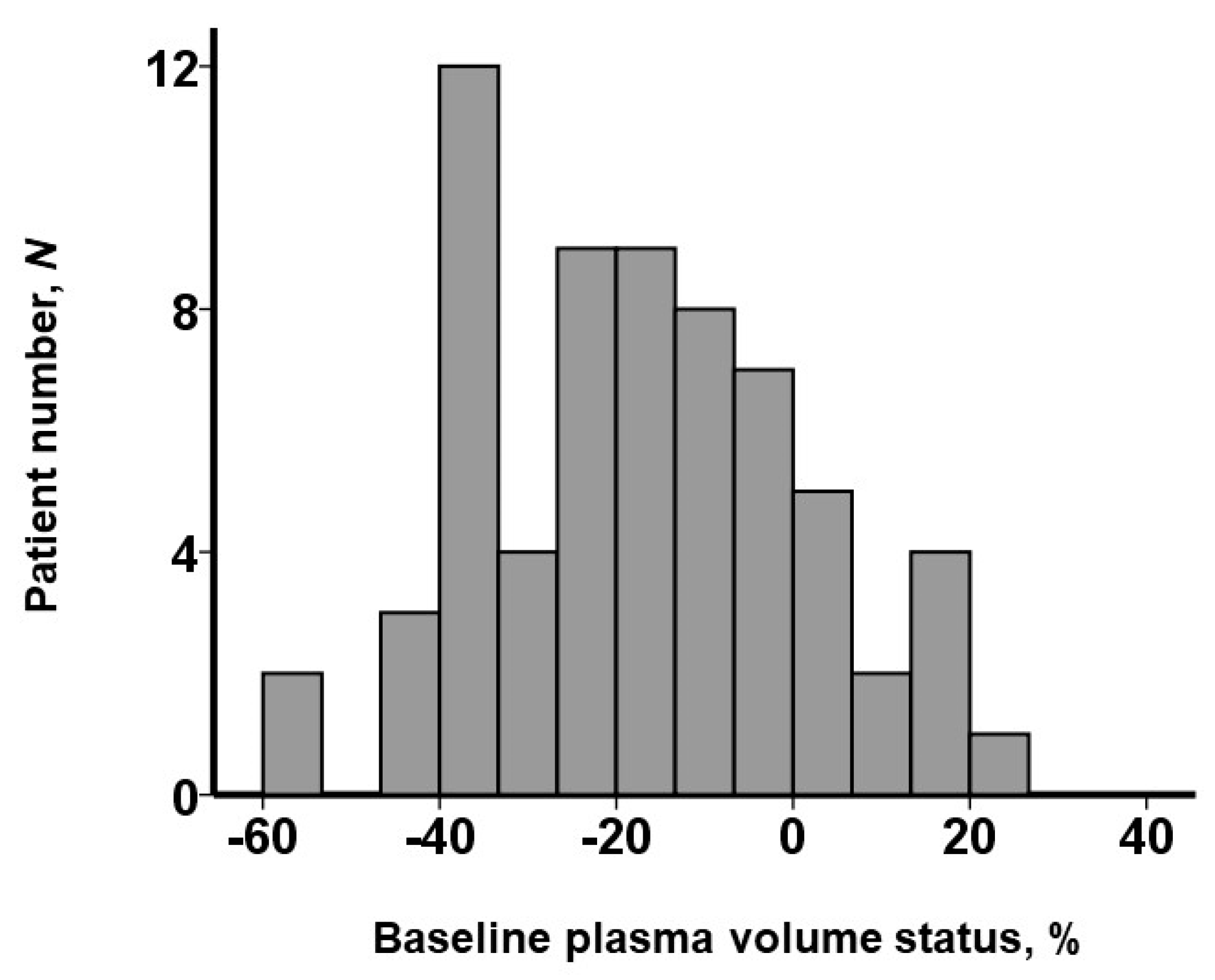
3.2. PV Status
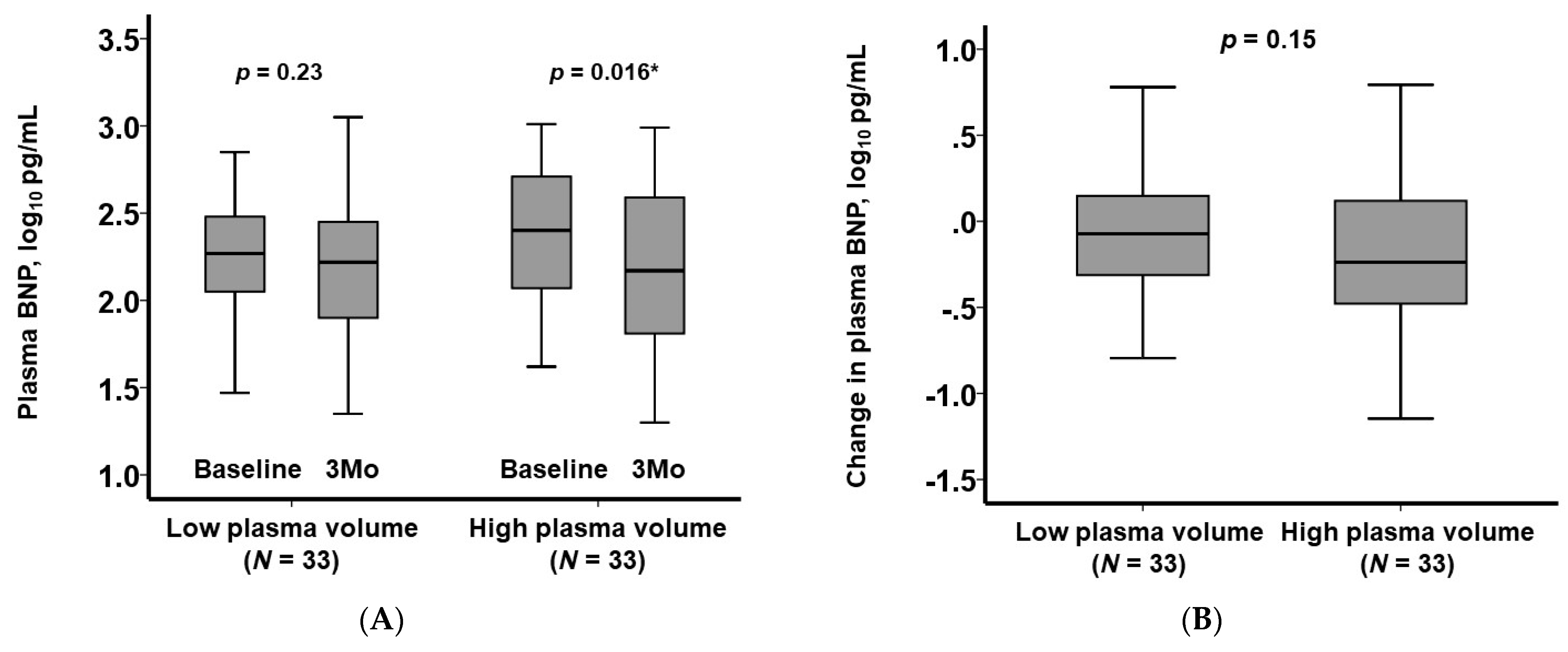
3.3. The Primary Outcome
3.4. Trends in Other Clinical Parameters
4. Discussion
4.1. The Presence of Systemic Congestion
4.2. Impact of ASV on Reducing Plasma BNP Levels
4.3. Clinical Implication of Our Findings
4.4. Strength of This Study
4.5. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tsutsui, H.; Ide, T.; Ito, H.; Kihara, Y.; Kinugawa, K.; Kinugawa, S.; Makaya, M.; Murohara, T.; Node, K.; Saito, Y.; et al. JCS/JHFS 2021 Guideline Focused Update on Diagnosis and Treatment of Acute and Chronic Heart Failure. Circ. J. 2021, 85, 2252–2291. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Aronowitz, P. Congestive Heart Failure. Med. Clin. N. Am. 2022, 106, 447–458. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Perez, I.; Rabiei-Samani, S. What Is Adaptive Servo-Ventilation (ASV)? Am. J. Respir. Crit. Care Med. 2021, 204, P3–P4. [Google Scholar] [PubMed]
- Imamura, T.; Narang, N.; Kinugawa, K. Adaptive Servo-Ventilation as a Novel Therapeutic Strategy for Chronic Heart Failure. J. Clin. Med. 2022, 11, 539. [Google Scholar] [CrossRef]
- Koyama, T.; Watanabe, H.; Kobukai, Y.; Makabe, S.; Munehisa, Y.; Iino, K.; Kosaka, T.; Ito, H. Beneficial effects of adaptive servo ventilation in patients with chronic heart failure. Circ. J. 2010, 74, 2118–2124. [Google Scholar] [CrossRef]
- Kasai, T.; Usui, Y.; Yoshioka, T.; Yanagisawa, N.; Takata, Y.; Narui, K.; Yamaguchi, T.; Yamashina, A.; Momomura, S.I. Effect of flow-triggered adaptive servo-ventilation compared with continuous positive airway pressure in patients with chronic heart failure with coexisting obstructive sleep apnea and Cheyne-Stokes respiration. Circ. Heart Fail. 2010, 3, 140–148. [Google Scholar] [CrossRef]
- Haruki, N.; Takeuchi, M.; Kaku, K.; Yoshitani, H.; Kuwaki, H.; Tamura, M.; Abe, H.; Okazaki, M.; Tsutsumi, A.; Otsuji, Y. Comparison of acute and chronic impact of adaptive servo-ventilation on left chamber geometry and function in patients with chronic heart failure. Eur. J. Heart Fail. 2011, 13, 1140–1146. [Google Scholar] [CrossRef]
- Yoshihisa, A.; Suzuki, S.; Miyata, M.; Yamaki, T.; Sugimoto, K.; Kunii, H.; Nakazato, K.; Suzuki, H.; Saitoh, S.; Takeishi, Y. “A single night” beneficial effects of adaptive servo-ventilation on cardiac overload, sympathetic nervous activity, and myocardial damage in patients with chronic heart failure and sleep-disordered breathing. Circ. J. 2012, 76, 2153–2158. [Google Scholar] [CrossRef]
- Kasai, T.; Kasagi, S.; Maeno, K.; Dohi, T.; Kawana, F.; Kato, M.; Naito, R.; Ishiwata, S.; Ohno, M.; Yamaguchi, T.; et al. Adaptive servo-ventilation in cardiac function and neurohormonal status in patients with heart failure and central sleep apnea nonresponsive to continuous positive airway pressure. JACC Heart Fail. 2013, 1, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Momomura, S.; Seino, Y.; Kihara, Y.; Adachi, H.; Yasumura, Y.; Yokoyama, H. Adaptive servo-ventilation therapy using an innovative ventilator for patients with chronic heart failure: A real-world, multicenter, retrospective, observational study (SAVIOR-R). Heart Vessels. 2015, 30, 805–817. [Google Scholar] [CrossRef]
- Momomura, S.; Seino, Y.; Kihara, Y.; Adachi, H.; Yasumura, Y.; Yokoyama, H.; Wada, H.; Ise, T.; Tanaka, K. Adaptive servo-ventilation therapy for patients with chronic heart failure in a confirmatory, multicenter, randomized, controlled study. Circ. J. 2015, 79, 981–990. [Google Scholar] [CrossRef] [PubMed]
- Cowie, M.R.; Woehrle, H.; Wegscheider, K.; Angermann, C.; d’Ortho, M.P.; Erdmann, E.; Levy, P.; Simonds, A.K.; Somers, V.K.; Zannad, F.; et al. Adaptive Servo-Ventilation for Central Sleep Apnea in Systolic Heart Failure. N. Engl. J. Med. 2015, 373, 1095–1105. [Google Scholar] [CrossRef] [PubMed]
- Yamada, S.; Sakakibara, M.; Yokota, T.; Kamiya, K.; Asakawa, N.; Iwano, H.; Yamada, S.; Oba, K.; Tsutsui, H. Acute hemodynamic effects of adaptive servo-ventilation in patients with heart failure. Circ. J. 2013, 77, 1214–1220. [Google Scholar] [CrossRef] [PubMed]
- Yagi, S.; Akaike, M.; Iwase, T.; Kusunose, K.; Niki, T.; Yamaguchi, K.; Koshiba, K.; Taketani, Y.; Tomita, N.; Yamada, H.; et al. Acute hemodynamic effects of adaptive servo ventilation in patients with pulmonary hypertension. Int. J. Cardiol. 2011, 148, 125–127. [Google Scholar] [CrossRef] [PubMed]
- Yamada, S.; Sakakibara, M.; Matsushima, S.; Saito, A.; Homma, T.; Fukushima, A.; Masaki, Y.; Watanabe, M.; Mitsuyama, H.; Yokoshiki, H.; et al. Successful termination of recurrent ventricular arrhythmias by adaptive servo-ventilation in a patient with heart failure. J. Cardiol. Cases 2011, 3, e57–e61. [Google Scholar] [CrossRef]
- Ling, H.Z.; Flint, J.; Damgaard, M.; Bonfils, P.K.; Cheng, A.S.; Aggarwal, S.; Velmurugan, S.; Mendonca, M.; Rashid, M.; Kang, S.; et al. Calculated plasma volume status and prognosis in chronic heart failure. Eur. J. Heart Fail. 2015, 17, 35–43. [Google Scholar] [CrossRef]
- Kawai, T.; Nakatani, D.; Yamada, T.; Sakata, Y.; Hikoso, S.; Mizuno, H.; Suna, S.; Kitamura, T.; Okada, K.; Dohi, T.; et al. Clinical impact of estimated plasma volume status and its additive effect with the GRACE risk score on in-hospital and long-term mortality for acute myocardial infarction. Int. J. Cardiol. Heart Vasc. 2021, 33, 100748. [Google Scholar] [CrossRef]
- Tamaki, S.; Yamada, T.; Morita, T.; Furukawa, Y.; Iwasaki, Y.; Kawasaki, M.; Kikuchi, A.; Kawai, T.; Seo, M.; Abe, M.; et al. Prognostic Value of Calculated Plasma Volume Status in Patients Admitted for Acute Decompensated Heart Failure—A Prospective Comparative Study with Other Indices of Plasma Volume. Circ. Rep. 2019, 1, 361–371. [Google Scholar] [CrossRef]
- Grodin, J.L.; Philips, S.; Mullens, W.; Nijst, P.; Martens, P.; Fang, J.C.; Drazner, M.H.; Tang, W.H.W.; Pandey, A. Prognostic implications of plasma volume status estimates in heart failure with preserved ejection fraction: Insights from TOPCAT. Eur. J. Heart Fail. 2019, 21, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Martens, P.; Nijst, P.; Dupont, M.; Mullens, W. The Optimal Plasma Volume Status in Heart Failure in Relation to Clinical Outcome. J. Card. Fail. 2019, 25, 240–248. [Google Scholar] [CrossRef] [PubMed]
- McKee, P.A.; Castelli, W.P.; McNamara, P.M.; Kannel, W.B. The natural history of congestive heart failure: The Framingham study. N. Engl. J. Med. 1971, 285, 1441–1446. [Google Scholar] [CrossRef] [PubMed]
- Seino, Y.; Momomura, S.; Kihara, Y.; Adachi, H.; Yasumura, Y.; Yokoyama, H.; SAVIOR-C Investigators. Effects of adaptive servo-ventilation therapy on cardiac function and remodeling in patients with chronic heart failure (SAVIOR-C): Study protocol for a randomized controlled trial. Trials 2015, 16, 14. [Google Scholar] [CrossRef]
- Tsutsui, H.; Isobe, M.; Ito, H.; Ito, H.; Okumura, K.; Ono, M.; Kitakaze, M.; Kinugawa, K.; Kihara, Y.; Goto, Y.; et al. JCS 2017/JHFS 2017 Guideline on Diagnosis and Treatment of Acute and Chronic Heart Failure—Digest Version. Circ. J. 2019, 83, 2084–2184. [Google Scholar] [CrossRef]
- Imamura, T.; Narang, N.; Kinugawa, K. Clinical implications of remote dielectric sensing system to estimate lung fluid levels. J. Cardiol. 2023, 81, 276–282. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (N = 66) | High Plasma Volume (N = 33) | Low Plasma Volume (N = 33) | p-Value | |
|---|---|---|---|---|
| Demographics | ||||
| Age, years | 66 (59, 74) | 73 (65, 78) | 61 (54, 68) | <0.001 * |
| Male sex | 53 (80%) | 23 (70%) | 30 (91%) | 0.030 * |
| Body mass index, kg/m2 | 23.1 (20.0, 26.8) | 20.3 (18.8, 22.6) | 26.8 (24.0, 29.3) | <0.001 * |
| Comorbidity | ||||
| Hypertension | 26 (39%) | 14 (42%) | 12 (36%) | 0.61 |
| Diabetes mellitus | 22 (33%) | 6 (18%) | 16 (48%) | 0.009 * |
| Atrial fibrillation | 30 (45%) | 14 (42%) | 16 (48%) | 0.40 |
| Coronary artery disease | 25 (38%) | 14 (42%) | 11 (33%) | 0.31 |
| History of stroke | 5 (8%) | 3 (9%) | 2 (6%) | 0.64 |
| Peripheral artery disease | 11 (17%) | 6 (18%) | 5 (15%) | 0.74 |
| Laboratory data | ||||
| Hemoglobin, g/dL | 12.9 (11.4, 14.1) | 11.5 (10.3, 12.4) | 14.0 (13.2, 15.4) | <0.001 * |
| Hematocrit, % | 38.7 (35.2, 42.7) | 35.3 (31.1, 37.9) | 42.4 (40.6, 45.9) | <0.001 * |
| Serum albumin, g/dL | 3.9 (3.6, 4.1) | 3.7 (3.4, 3.9) | 4.1 (3.9, 4.3) | <0.001 * |
| Serum sodium, mEq/L | 139 (137, 141) | 138 (135, 141) | 140 (138, 141) | 0.065 |
| Serum potassium, mEq/L | 4.3 (4.0, 4.5) | 4.4 (4.2, 4.7) | 4.2 (4.0, 4.4) | 0.053 |
| Serum total bilirubin, mg/dL | 0.7 (0.5, 0.9) | 0.6 (0.5, 0.8) | 0.8 (0.6, 1.0) | 0.039 * |
| eGFR, mL/min/1.73 m2 | 48.4 (38.5, 59.0) | 41.1 (33.8, 55.3) | 50.9 (45.7, 66.6) | 0.003 * |
| Plasma BNP, log10 pg/mL | 2.24 (2.05, 2.60) | 2.37 (2.06, 2.71) | 2.21 (1.98, 2.53) | 0.26 |
| Echocardiography | ||||
| LVDd, mm | 62 (55, 69) | 58 (52, 69) | 65 (60, 74) | 0.062 |
| LVEF, % | 33 (23, 47) | 34 (24, 54) | 32 (23, 39) | 0.49 |
| Left atrial diameter, mm | 47 (41, 53) | 43 (40, 51) | 49 (43, 53) | 0.028 * |
| Moderate or greater MR | 20 (30%) | 15 (45%) | 5 (15%) | 0.011 * |
| Moderate or greater TR | 16 (24%) | 13 (39%) | 3 (9%) | 0.006 * |
| Medication | ||||
| Beta-blocker | 52(79%) | 25 (76%) | 27 (82%) | 0.38 |
| RAS inhibitor | 58 (88%) | 28 (85%) | 30 (91%) | 0.45 |
| MRA | 38 (58%) | 16 (48%) | 22 (67%) | 0.11 |
| SGLT2 inhibitor | 26 (39%) | 12 (36%) | 14 (42%) | 0.61 |
| Dose of loop diuretics, mg/day | 20 (0, 30) | 20 (0. 40) | 20 (0, 20) | 0.24 |
| Plasma volume status, % | −16.9 (−29.9, −4.5) | −4.7 (−10.8, 3.4) | −34.7 (−38.3, −23.6) | <0.001 * |
| Univariable Analysis | Multivariable Analysis | |||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p-Value | Odds Ratio (95% CI) | p-Value | |
| Age, years | 1.02 (0.98–1.06) | 0.43 | ||
| Atrial fibrillation | 0.58 (0.22–1.56) | 0.28 | ||
| Coronary artery disease | 0.59 (0.21–1.64) | 0.31 | ||
| eGFR, mL/min/1.73 m2 | 0.98 (0.95–1.01) | 0.12 | ||
| Plasma BNP, log10 pg/mL | 2.53 (0.75–8.55) | 0.14 | ||
| LVDd, mm | 1.02 (0.98–1.07) | 0.34 | ||
| LVEF, % | 0.97 (0.94–1.01) | 0.098 | 0.97 (0.94–1.01) | 0.058 |
| Moderate or greater MR | 1.33 (0.46–3.88) | 0.6 | ||
| Moderate or greater TR | 1.30 (0.42–4.07) | 0.65 | ||
| Beta-blocker | 2.32 (0.64–8.33) | 0.2 | ||
| RAS inhibitor | 1.35 (0.30–6.20) | 0.7 | ||
| MRA | 1.08 (0.40–2.89) | 0.88 | ||
| SGLT2 inhibitor | 1.06 (0.42–2.67) | 0.67 | ||
| Dose of loop diuretics, mg/day | 1.01 (0.99–1.02) | 0.33 | ||
| Plasma volume status, % | 1.03 (1.01–1.06) | 0.046 * | 1.036 (1.01–1.07) | 0.032 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nomoto, Y.; Imamura, T.; Kinugawa, K. Systemic Congestion as a Determinant of Efficacy in Adaptive Servo-Ventilation Therapy: A Retrospective Observational Study. J. Clin. Med. 2024, 13, 674. https://doi.org/10.3390/jcm13030674
Nomoto Y, Imamura T, Kinugawa K. Systemic Congestion as a Determinant of Efficacy in Adaptive Servo-Ventilation Therapy: A Retrospective Observational Study. Journal of Clinical Medicine. 2024; 13(3):674. https://doi.org/10.3390/jcm13030674
Chicago/Turabian StyleNomoto, Yu, Teruhiko Imamura, and Koichiro Kinugawa. 2024. "Systemic Congestion as a Determinant of Efficacy in Adaptive Servo-Ventilation Therapy: A Retrospective Observational Study" Journal of Clinical Medicine 13, no. 3: 674. https://doi.org/10.3390/jcm13030674