
Association of Prediabetes and Recurrent Stroke in Atrial Fibrillation Patients: A Population-Based Analysis of Hospitalizations and Outcomes
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
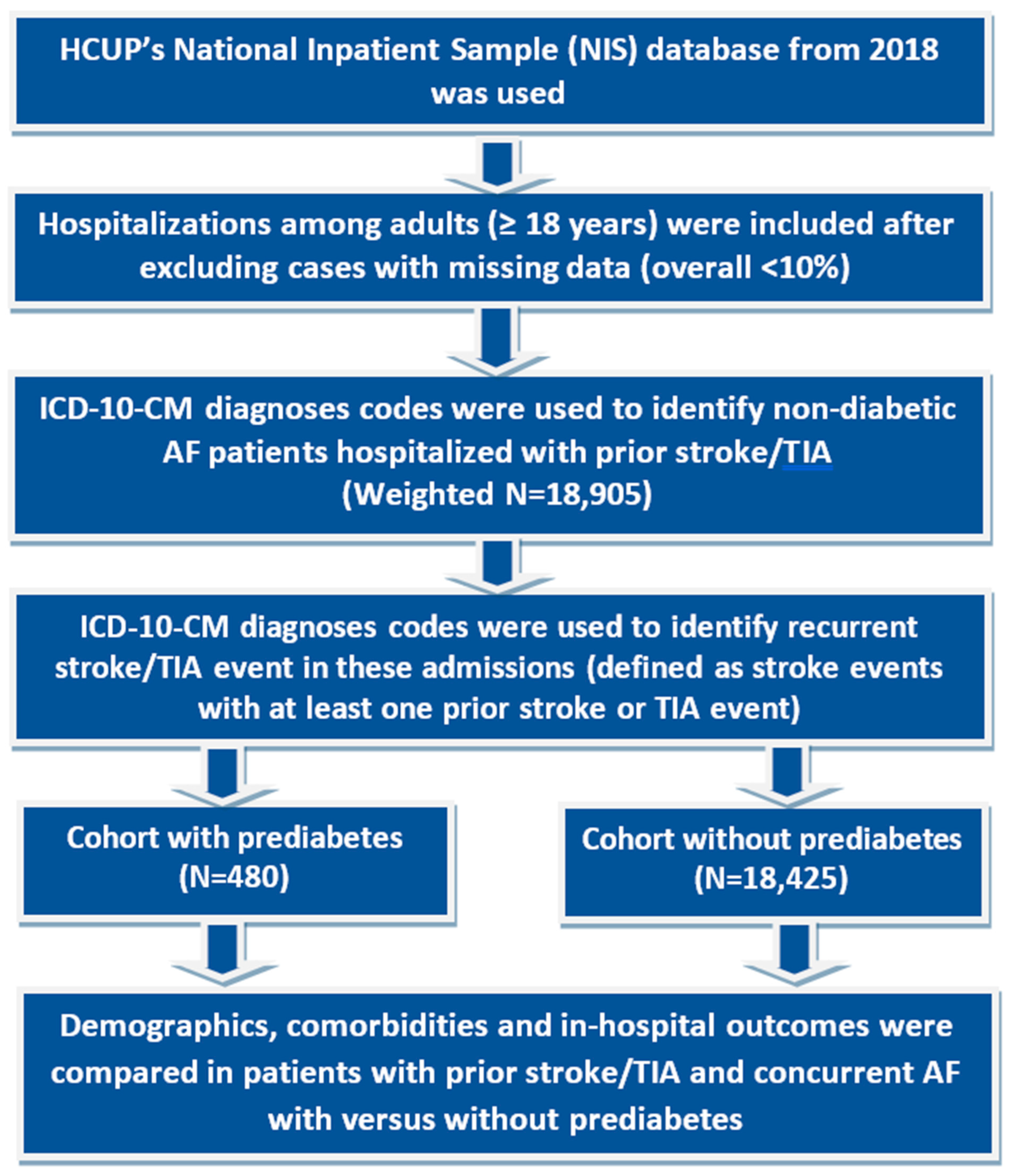
2.1. Data Sources
2.2. Study Participants
2.3. Study Outcomes
2.4. Statistical Analyses
3. Results
3.1. Study Population
3.2. Demographics
3.3. Risk of Recurrent Stroke
3.4. Comorbidities
3.5. Healthcare Utilization
3.6. All-Cause Mortality
4. Discussion
5. Limitations
6. Future Directives
7. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Gaglia, J.L.; Hilliard, M.E.; Isaacs, D.; et al. Classification and Diagnosis of Diabetes: Standards of Care in Diabetes. Diabetes Care 2022, 46 (Suppl. 1), S19–S40. [Google Scholar] [CrossRef] [PubMed]
- Desai, R.; Haque, F.A.; Vasavada, A.; Jain, M.; Desai, R.; Patel, V.; Shawl, S.; Sanikommu, S.; Edusa, S.; Sadum, N.; et al. Abstract 230: Prediabetes In Young Adults and Its Association with Type 1 Myocardial Infarction-related Admissions and Outcomes: A Population-based Analysis In The United States. Circ. Cardiovasc. Qual. Outcomes 2022, 15, A230. [Google Scholar] [CrossRef]
- Kamel, H.; Okin, P.M.; Elkind, M.S.V.; Iadecola, C. Atrial Fibrillation and Mechanisms of Stroke: Time for a New Model. Stroke 2016, 47, 895–900. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Johnsen, S.P.; Guo, Y.; Lip, G.Y. Lip, Epidemiology of Atrial Fibrillation. Card. Electrophysiol. Clin. 2021, 13, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Schlesinger, S.; Neuenschwander, M.; Barbaresko, J.; Lang, A.; Maalmi, H.; Rathmann, W.; Roden, M.; Herder, C. Prediabetes and risk of mortality, diabetes-related complications and comorbidities: Umbrella review of meta-analyses of prospective studies. Diabetologia 2021, 65, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Zeitler, E.P.; Piccini, J.P. Pre-Diabetes and Stroke in Patients with Atrial Fibrillation. J. Am. Coll. Cardiol. 2021, 77, 885–887. [Google Scholar] [CrossRef] [PubMed]
- Overview of the National (Nationwide) Inpatient Sample (NIS), Healthcare Cost and Utilization Project (HCUP) Database. Available online: https://hcup-us.ahrq.gov/nisoverview.jsp (accessed on 24 March 2023).
- Osei, E.; Hertog, H.M.D.; Fonville, S.; Brouwers, P.J.; Mulder, L.J.; Koudstaal, P.J.; Dippel, D.W.; Zandbergen, A.A.; Lingsma, H.F. Prediction of Persistent Impaired Glucose Tolerance in Patients with Minor Ischemic Stroke or Transient Ischemic Attack. J. Stroke Cerebrovasc. Dis. 2020, 29, 104815. [Google Scholar] [CrossRef]
- Karabag, T.; Aydin, M.; Dogan, S.M.; Cetiner, M.A.; Sayin, M.R.; Gudul, N.E.; Kucuk, E. Prolonged P wave dispersion in pre-diabetic patients. Kardiol. Pol. 2011, 69, 566–571. [Google Scholar]
- Hoogwerf, B.J. Prediabetes, Atrial Fibrillation, and Heart Failure: An Intersection of Comorbidities. Diabetes Care 2022, 46, 9–10. [Google Scholar] [CrossRef]
- Hsu, J.-C.; Yang, Y.-Y.; Chuang, S.-L.; Lin, L.-Y.; Chen, T.H.-H. Prediabetes as a risk factor for new-onset atrial fibrillation: The propensity-score matching cohort analyzed using the Cox regression model coupled with the random survival forest. Cardiovasc. Diabetol. 2023, 22, 35. [Google Scholar] [CrossRef]
- Muscari, A.; Falcone, R.; Recinella, G.; Faccioli, L.; Forti, P.; Trossello, M.P.; Puddu, G.M.; Spinardi, L.; Zoli, M. Prognostic significance of diabetes and stress hyperglycemia in acute stroke patients. Diabetol. Metab. Syndr. 2022, 14, 126. [Google Scholar] [CrossRef] [PubMed]
- Stratmann, B.; Tschoepe, D. Diabetes, prediabetes and cardiovascular risk. Der. Internist. 2015, 56, 653–663, quiz 662–663. [Google Scholar] [CrossRef] [PubMed]
- Kezerle, L.; Tsadok, M.A.; Akriv, A.; Senderey, A.B.; Bachrach, A.; Leventer-Roberts, M.; Haim, M. Pre-Diabetes Increases Stroke Risk in Patients with Nonvalvular Atrial Fibrillation. J. Am. Coll. Cardiol. 2021, 77, 875–884. [Google Scholar] [CrossRef] [PubMed]
- Bo, X.W.; Zuo, S.; Jiang, C.; He, L.; Zhao, X.; Li, S.N.; Tang, R.B.; Long, D.Y.; Du, X.; Dong, J.Z.; et al. The relationship between fasting blood glucose level and thromboembolism events in patients with non-valvular atrial fibrillation. Chin. J. Cardiovasc. Dis. 2022, 50, 243–248. [Google Scholar] [CrossRef]
- Decker, J.J.; Norby, F.L.; Rooney, M.R.; Soliman, E.Z.; Lutsey, P.L.; Pankow, J.S.; Alonso, A.; Chen, L.Y. Metabolic Syndrome and Risk of Ischemic Stroke in Atrial Fibrillation: ARIC Study. Stroke 2019, 50, 3045–3050. [Google Scholar] [CrossRef]
- Deng, M.; Su, D.; Xu, S.; Little, P.J.; Feng, X.; Tang, L.; Shen, A. Metformin and Vascular Diseases: A Focused Review on Smooth Muscle Cell Function. Front. Pharmacol. 2020, 11, 635. [Google Scholar] [CrossRef]
- Koskinas, K.; Melmer, A.; Steiner, N.; Gübeli, A.; Wilhelm, M.; Laimer, M. Diagnosis, Prevention and Treatment of Cardiovascular Disease in People with Diabetes and Prediabetes. Praxis 2021, 110, 37–47. [Google Scholar] [CrossRef]
- O’Keefe, E.L.; Sturgess, J.E.; O’Keefe, J.H.; Gupta, S.; Lavie, C.J. Prevention and Treatment of Atrial Fibrillation via Risk Factor Modification. Am. J. Cardiol. 2021, 160, 46–52. [Google Scholar] [CrossRef]
- Oladiran, O.; Nwosu, I. Stroke Risk Stratification in Atrial Fibrillation: A Review of Common Risk Factors. J. Community Hosp. Intern. Med. Perspect. 2019, 9, 113–120. [Google Scholar] [CrossRef]
- Palmisano, P.; Del Greco, M.; Mantica, M.; Moltrasio, M.; Pecora, D.; Pisanò, E.C.; Rovaris, G.; Perego, G.B. Expert Opinion on Continuous Rhythm Monitoring of Patients with Atrial Fibrillation for Candidates or Patients Who Have Already Undergone Ablation. Int. J. Cardiol. 2020, 305, 76–81. [Google Scholar] [CrossRef]
- Rovaris, G.; Ciconte, G.; Schiavone, M.; Mitacchione, G.; Gasperetti, A.; Piazzi, E.; Negro, G.; Montemerlo, E.; Rondine, R.; Pozzi, M.; et al. Second-Generation Laser Balloon Ablation for the Treatment of Atrial Fibrillation Assessed by Continuous Rhythm Monitoring: The LIGHT-AF Study. Europace 2021, 23, 1380–1390. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Prediabetes | Total Recurrent Stroke with AF (Excluding DM) | p-Value | |||
|---|---|---|---|---|---|
| No | Yes | ||||
| n = 18,425 | n = 480 | n = 18,905 | |||
| Age (years) at admission | Median [IQR] | 82 (73–88) | 78 (69–84) | 82 (73–88) | <0.001 |
| Sex | Male | 45.9% | 50.0% | 46.0% | 0.078 |
| Female | 54.1% | 50.0% | 54.0% | ||
| Race | White | 80.7% | 67.7% | 80.3% | <0.001 |
| Black | 9.4% | 15.6% | 9.6% | ||
| Hispanic | 5.6% | 11.5% | 5.7% | ||
| Asian or Pacific Islander | 2.2% | 4.2% | 2.2% | ||
| Median household income national quartile for patient ZIP Code | 0–25th | 24.4% | 25.5% | 24.4% | 0.543 |
| 26–50th | 25.7% | 26.6% | 25.8% | ||
| 51–75th | 25.7% | 26.6% | 25.7% | ||
| 76–100th | 24.2% | 21.3% | 24.1% | ||
| Primary expected payer | Medicare | 85.2% | 78.1% | 85.0% | <0.001 |
| Medicaid | 2.5% | 5.2% | 2.5% | ||
| Private including HMO | 9.7% | 15.6% | 9.8% | ||
| Location/teaching status of hospital | Rural | 6.9% | 6.8% | <0.001 | |
| Urban non-teaching | 19.4% | 15.6% | 19.3% | ||
| Urban teaching | 73.7% | 82.3% | 73.9% | ||
| Region of hospital | Northeast | 16.7% | 19.8% | 16.8% | <0.001 |
| Midwest | 23.4% | 17.7% | 23.3% | ||
| South | 39.5% | 25.0% | 39.2% | ||
| West | 20.3% | 37.5% | 20.7% | ||
| COMORBIDITIES | |||||
| Hypertension | 85.2% | 85.4% | 85.2% | 0.913 | |
| Hyperlipidemia | 59.3% | 74.0% | 59.6% | <0.001 | |
| Smoking | 37.4% | 43.7% | 37.6% | 0.005 | |
| Peripheral vascular disease | 13.0% | 17.7% | 13.1% | 0.003 | |
| Obesity | 8.0% | 18.7% | 8.3% | <0.001 | |
| Renal failure | 19.1% | 20.8% | 19.1% | 0.334 | |
| Prior MI | 10.6% | 8.3% | 10.6% | 0.109 | |
| Prior PCI | 0.9% | 4.2% | 1.0% | <0.001 | |
| Prior CABG | 8.9% | 5.2% | 8.8% | 0.005 | |
| Prior VTE | 7.0% | 3.1% | 6.9% | 0.001 | |
| Cancer | 17.7% | 17.7% | 17.7% | 0.981 | |
| Congestive heart failure | 26.4% | 24.0% | 26.3% | 0.24 | |
| Valvular heart disease | 18.8% | 18.7% | 18.8% | 0.963 | |
| Chronic pulmonary disease | 18.2% | 21.9% | 18.3% | 0.042 | |
| Rheumatoid arthritis/collagen vas | 3.4% | 3.1% | 3.4% | 0.726 | |
| Coagulopathy | 6.3% | 8.3% | 6.3% | 0.071 | |
| Fluid and electrolyte disorders | 26.9% | 22.9% | 26.8% | 0.052 | |
| Deficiency Anaemias | 14.1% | 11.5% | 14.0% | 0.102 | |
| Other neurological disorders | 6.0% | 6.3% | 6.0% | 0.838 | |
| Hypothyroidism | 20.2% | 14.6% | 20.0% | 0.002 | |
| Depression | 10.8% | 11.5% | 10.8% | 0.633 | |
| Outcomes | aOR | 95% LL | 95% UL | p | |
|---|---|---|---|---|---|
| Odds of Recurrent Stroke | Unadjusted odds | 2.14 | 1.72 | 2.66 | <0.001 |
| Odds when adjusted for baseline demographics and hospital level characteristics | 2.13 | 1.69 | 2.69 | <0.001 | |
| Odds when adjusted for baseline demographics and hospital level characteristics plus pre-existing comorbidities | 2.09 | 1.65 | 2.64 | <0.001 | |
| Odds of Subsequent In-hospital Mortality | 0.55 | 0.19 | 1.56 | 0.260 | |
| Prediabetes | |||||
| No | Yes | Total Recurrent Stroke with AF (Excluding DM) | p-Value | ||
| All-cause Mortality | 7.6% | 4.2% | 7.5% | 0.005 | |
| Disposition of patient | Routine | 25.0% | 44.8% | 25.5% | <0.001 |
| Transfers to short term hospitals | 2.5% | 2.5% | |||
| Other transfers incl. SNF, ICF | 47.0% | 26.0% | 46.4% | ||
| Home health care | 17.3% | 22.9% | 17.4% | ||
| Length of stay (days) | Median [IQR] | (2–6) | (2–5) | (2–6) | 0.002 |
| Cost | Median [IQR] | (6657–17,693) | (7590–20,563) | (6661–17,776) | 0.003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Desai, R.; Vasavada, A.; Patel, B.A.; Raval, M.; Mondal, A.; Mahajan, K.; Katukuri, N.; Varma, Y.; Jain, A.; Krishnamoorthy, G. Association of Prediabetes and Recurrent Stroke in Atrial Fibrillation Patients: A Population-Based Analysis of Hospitalizations and Outcomes. J. Clin. Med. 2024, 13, 573. https://doi.org/10.3390/jcm13020573
Desai R, Vasavada A, Patel BA, Raval M, Mondal A, Mahajan K, Katukuri N, Varma Y, Jain A, Krishnamoorthy G. Association of Prediabetes and Recurrent Stroke in Atrial Fibrillation Patients: A Population-Based Analysis of Hospitalizations and Outcomes. Journal of Clinical Medicine. 2024; 13(2):573. https://doi.org/10.3390/jcm13020573
Chicago/Turabian StyleDesai, Rupak, Advait Vasavada, Bhavin A. Patel, Maharshi Raval, Avilash Mondal, Kshitij Mahajan, Nishanth Katukuri, Yash Varma, Akhil Jain, and Geetha Krishnamoorthy. 2024. "Association of Prediabetes and Recurrent Stroke in Atrial Fibrillation Patients: A Population-Based Analysis of Hospitalizations and Outcomes" Journal of Clinical Medicine 13, no. 2: 573. https://doi.org/10.3390/jcm13020573