
The Effect of Sodium–Glucose Cotransporter-2 Inhibitors on COVID-19 Patients with Type 2 Diabetes Mellitus: A Retrospective Cohort Study Using the Common Data Model

Abstract
:1. Introduction
2. Materials and Methods
2.1. Definitions and Outcomes
2.2. Statistical Analysis
3. Results
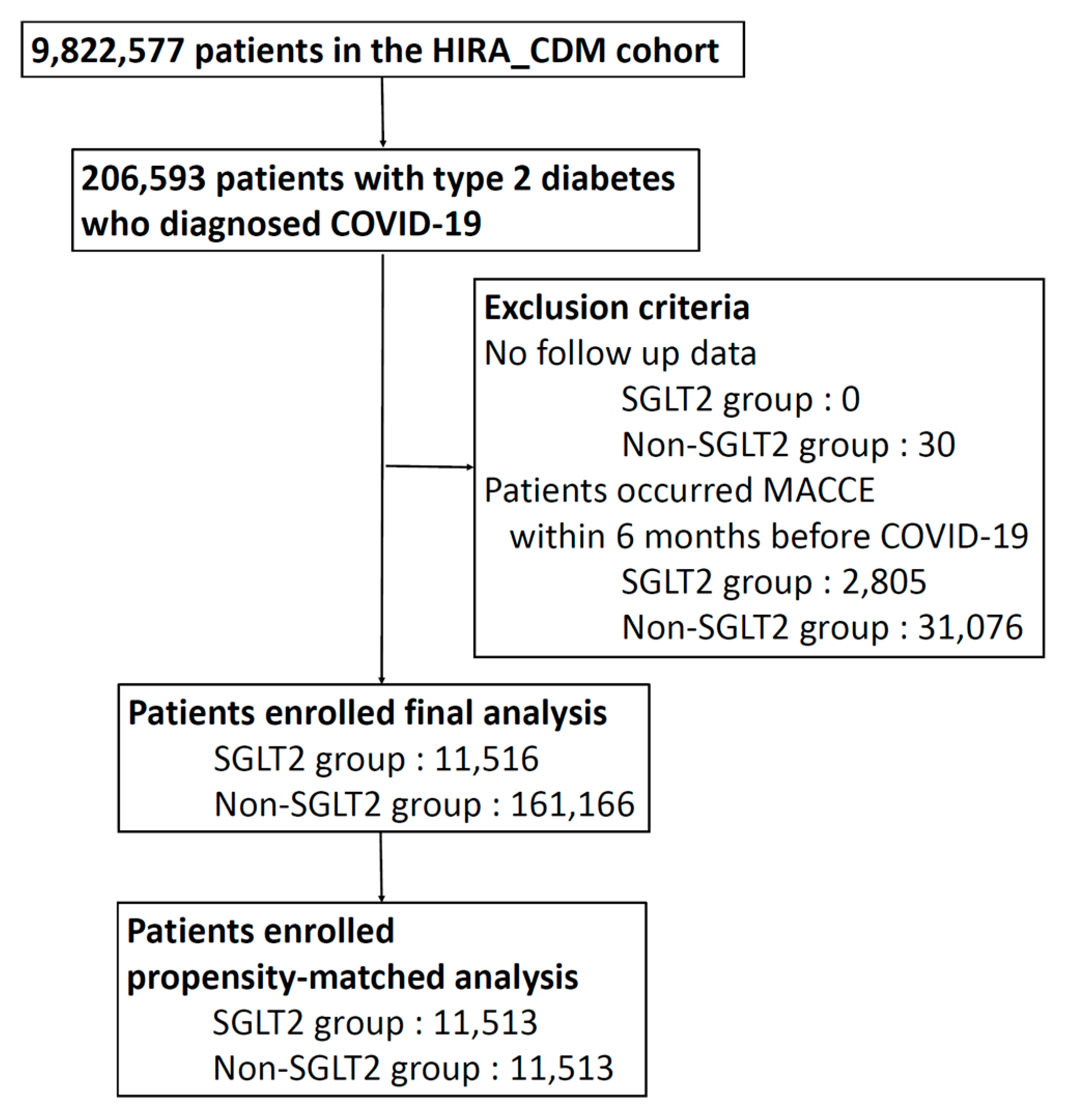
3.1. Cohort Characteristics
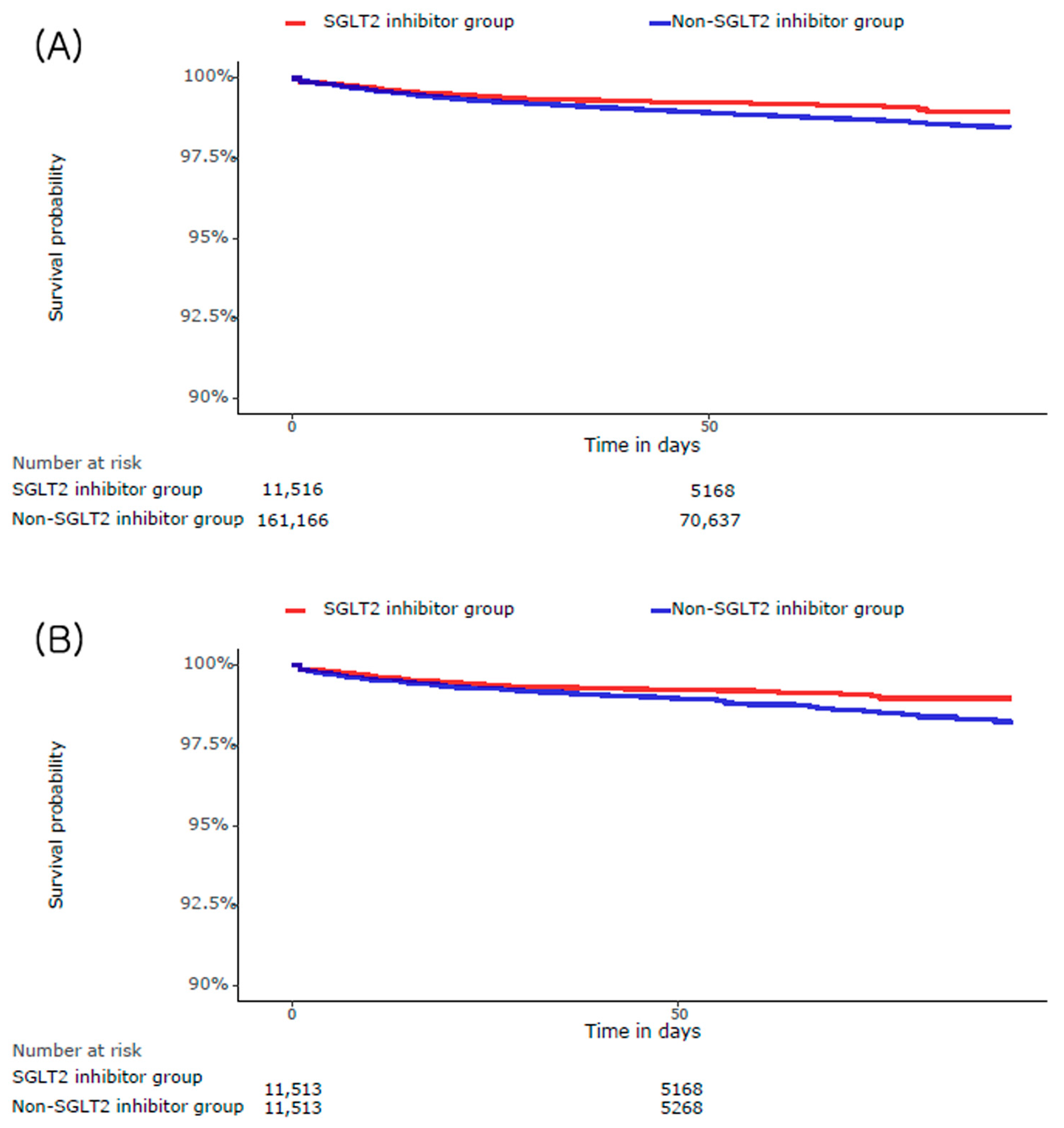
3.2. Clinical Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| COVID | Coronavirus disease |
| SGLT2 | Sodium glucose cotransporter 2 |
| DM | Diabetes mellitus |
| HIRA | Health Insurance Review and Assessment Service of Korea |
| OMOP | Observational Medical Outcomes Partnership |
| CDM | Common data model |
| OHDSI | Observational Health Data Sciences and Informatics |
| MACCEs | Major adverse cardiac and cerebrovascular events |
References
- The Lancet. Long COVID: 3 Years in. Lancet 2023, 401, 795. [CrossRef] [PubMed]
- Gupta, R.; Hussain, A.; Misra, A. Diabetes and COVID-19: Evidence, Current Status and Unanswered Research Questions. Eur. J. Clin. Nutr. 2020, 74, 864–870. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.Y.; Ma, Y.T.; Zhang, J.Y.; Xie, X. COVID-19 and the Cardiovascular System. Nat. Rev. Cardiol. 2020, 17, 259–260. [Google Scholar] [CrossRef] [PubMed]
- Fedorchenko, Y.; Zimba, O. Comorbidities in the COVID-19 Pandemic: Scopus-Based Bibliometric Analysis. J. Korean Med. Sci. 2023, 38, e93. [Google Scholar] [CrossRef] [PubMed]
- Raisi-Estabragh, Z.; Cooper, J.; Salih, A.; Raman, B.; Lee, A.M.; Neubauer, S.; Harvey, N.C.; Petersen, S.E. Cardiovascular Disease and Mortality Sequelae of COVID-19 in the UK Biobank. Heart 2022, 109, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Xu, E.; Bowe, B.; Al-Aly, Z. Long-Term Cardiovascular Outcomes of COVID-19. Nat. Med. 2022, 28, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Braunwald, E. SGLT2 Inhibitors: The Statins of the 21st Century. Eur. Heart J. 2022, 43, 1029–1030. [Google Scholar] [CrossRef]
- Zelniker, T.A.; Wiviott, S.D.; Raz, I.; Im, K.; Goodrich, E.L.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Furtado, R.H.M.; et al. SGLT2 Inhibitors for Primary and Secondary Prevention of Cardiovascular and Renal Outcomes in Type 2 Diabetes: A Systematic Review and Meta-Analysis of Cardiovascular Outcome Trials. Lancet 2019, 393, 31–39. [Google Scholar] [CrossRef]
- Sainsbury, C.; Wang, J.; Gokhale, K.; Acosta-Mena, D.; Dhalla, S.; Byne, N.; Chandan, J.S.; Anand, A.; Cooper, J.; Okoth, K.; et al. Sodium-Glucose Co-Transporter-2 Inhibitors and Susceptibility to COVID-19: A Population-Based Retrospective Cohort Study. Diabetes Obes. Metab. 2021, 23, 263–269. [Google Scholar] [CrossRef]
- Vitale, R.J.; Valtis, Y.K.; McDonnell, M.E.; Palermo, N.E.; Fisher, N.D.L. Euglycemic Diabetic Ketoacidosis with COVID-19 Infection in Patients with Type 2 Diabetes Taking SGLT2 Inhibitors. AACE Clin. Case Rep. 2021, 7, 10–13. [Google Scholar] [CrossRef]
- Kosiborod, M.N.; Esterline, R.; Furtado, R.H.M.; Oscarsson, J.; Gasparyan, S.B.; Koch, G.G.; Martinez, F.; Mukhtar, O.; Verma, S.; Chopra, V.; et al. Dapagliflozin in Patients with Cardiometabolic Risk Factors Hospitalised with COVID-19 (DARE-19): A Randomised, Double-Blind, Placebo-Controlled, Phase 3 Trial. Lancet Diabetes Endocrinol. 2021, 9, 586–594. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Kim, C.; Kim, K.H.; Lee, Y.; Yu, D.H.; Yun, J.; Baek, H.; Park, R.W.; You, S.C. Scalable Infrastructure Supporting Reproducible Nationwide Healthcare Data Analysis toward FAIR Stewardship. Sci. Data 2023, 10, 674. [Google Scholar] [CrossRef] [PubMed]
- Jiang, G.; Kiefer, R.C.; Sharma, D.K.; Prud’hommeaux, E.; Solbrig, H.R. A Consensus-Based Approach for Harmonizing the OHDSI Common Data Model with HL7 FHIR. Stud. Health Technol. Inform. 2017, 245, 887–891. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-las-Peñas, C.; Palacios-Ceña, D.; Gómez-Mayordomo, V.; Florencio, L.L.; Cuadrado, M.L.; Plaza-Manzano, G.; Navarro-Santana, M. Prevalence of Post-COVID-19 Symptoms in Hospitalized and Non-Hospitalized COVID-19 Survivors: A Systematic Review and Meta-Analysis. Eur. J. Intern. Med. 2021, 92, 55–70. [Google Scholar] [CrossRef] [PubMed]
- Elze, M.C.; Gregson, J.; Baber, U.; Williamson, E.; Sartori, S.; Mehran, R.; Nichols, M.; Stone, G.W.; Pocock, S.J. Comparison of Propensity Score Methods and Covariate Adjustment: Evaluation in 4 Cardiovascular Studies. J. Am. Coll. Cardiol. 2017, 69, 345–357. [Google Scholar] [CrossRef] [PubMed]
- Khunti, K.; Valabhji, J.; Misra, S. Diabetes and the COVID-19 Pandemic. Diabetologia 2023, 66, 255–266. [Google Scholar] [CrossRef]
- Unsworth, R.; Wallace, S.; Oliver, N.S.; Yeung, S.; Kshirsagar, A.; Naidu, H.; Kwong, R.M.W.; Kumar, P.; Logan, K.M. New-Onset Type 1 Diabetes in Children during COVID-19: Multicenter Regional Findings in the U.K. Diabetes Care 2020, 43, e170–e171. [Google Scholar] [CrossRef]
- Kamrath, C.; Mönkemöller, K.; Biester, T.; Rohrer, T.R.; Warncke, K.; Hammersen, J.; Holl, R.W. Ketoacidosis in Children and Adolescents with Newly Diagnosed Type 1 Diabetes during the COVID-19 Pandemic in Germany. JAMA 2020, 324, 801. [Google Scholar] [CrossRef]
- Maayah, Z.H.; Ferdaoussi, M.; Takahara, S.; Soni, S.; Dyck, J.R.B. Empagliflozin Suppresses Inflammation and Protects against Acute Septic Renal Injury. Inflammopharmacology 2021, 29, 269–279. [Google Scholar] [CrossRef]
- Lee, H.-F.; Chan, Y.-H.; Chuang, C.; Li, P.-R.; Yeh, Y.-H.; Hsiao, F.-C.; Peng, J.-R.; See, L.-C. Cardiovascular, Renal, and Lower Limb Outcomes in Patients with Type 2 Diabetes after Percutaneous Coronary Intervention and Treated with Sodium–Glucose Cotransporter 2 Inhibitors vs. Dipeptidyl Peptidase-4 Inhibitors. Eur. Heart J. Cardiovasc. Pharmacother. 2023, 9, 301. [Google Scholar] [CrossRef]
- Tereshchenko, L.G.; Bishop, A.; Fisher-Campbell, N.; Levene, J.; Morris, C.C.; Patel, H.; Beeson, E.; Blank, J.A.; Bradner, J.N.; Coblens, M.; et al. Risk of Cardiovascular Events after COVID-19. Am. J. Cardiol. 2022, 179, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Fox, S.E.; Li, G.; Akmatbekov, A.; Harbert, J.L.; Lameira, F.S.; Brown, J.Q.; Heide, R.S.V. Unexpected Features of Cardiac Pathology in COVID-19 Infection. Circulation 2020, 142, 1123–1125. [Google Scholar] [CrossRef] [PubMed]
- McGonagle, D.; Plein, S.; O’Donnell, J.S.; Sharif, K.; Bridgewood, C. Increased Cardiovascular Mortality in African Americans with COVID-19. Lancet Respir. Med. 2020, 8, 649–651. [Google Scholar] [CrossRef] [PubMed]
- Cowie, M.R.; Fisher, M. SGLT2 Inhibitors: Mechanisms of Cardiovascular Benefit beyond Glycaemic Control. Nat. Rev. Cardiol. 2020, 17, 761–772. [Google Scholar] [CrossRef]
- Wu, M.-Z.; Chandramouli, C.; Wong, P.-F.; Chan, Y.-H.; Li, H.-L.; Yu, S.-Y.; Tse, Y.-K.; Ren, Q.-W.; Yu, S.-Y.; Tse, H.-F.; et al. Risk of Sepsis and Pneumonia in Patients Initiated on SGLT2 Inhibitors and DPP-4 Inhibitors. Diabetes Metab. 2022, 48, 101367. [Google Scholar] [CrossRef]
- Bossi, A.C.; Forloni, F.; Colombelli, P.L. Lack of Efficacy of SGLT2-i in Severe Pneumonia Related to Novel Coronavirus (NCoV) Infection: No Little Help from Our Friends. Diabetes Ther. 2020, 11, 1605–1606. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Before PS Adjustment | After PS Adjustment | |||||
|---|---|---|---|---|---|---|
| SGLT2 Inhibitor | Non-SGLT2 Inhibitor | SMD | SGLT2 Inhibitor | Non-SGLT2 Inhibitor | SMD | |
| (n = 11,516) | (n = 161,166) | (n = 11,513) | (n = 11,513) | |||
| Age group | ||||||
| 15–19 | 0.1 | 0.6 | −0.09 | 0.1 | 0.2 | −0.03 |
| 20–24 | 0.6 | 0.9 | −0.04 | 0.7 | 0.6 | 0 |
| 25–29 | 0.9 | 1.4 | −0.04 | 1 | 0.9 | 0.01 |
| 30–34 | 1.7 | 2 | −0.03 | 1.7 | 1.5 | 0.02 |
| 35–39 | 3.6 | 3.3 | 0.02 | 3.7 | 3.6 | 0.01 |
| 45–49 | 8.2 | 6 | 0.09 | 8.4 | 8.1 | 0.01 |
| 50–54 | 11 | 8.6 | 0.08 | 11.3 | 11 | 0.01 |
| 60–64 | 17 | 15.1 | 0.05 | 17 | 17 | 0 |
| 65–69 | 14 | 14.3 | −0.01 | 13.9 | 13.7 | 0.01 |
| 70–74 | 10.4 | 11.3 | −0.03 | 10.2 | 10.2 | 0 |
| 75–79 | 6.4 | 8.2 | −0.07 | 6.1 | 6.5 | −0.01 |
| 80–84 | 3.9 | 6.7 | −0.13 | 3.5 | 3.7 | −0.01 |
| 85–89 | 1.6 | 3.9 | −0.14 | 1.4 | 1.5 | −0.01 |
| 90–94 | 0.4 | 1.5 | −0.1 | 0.4 | 0.5 | −0.02 |
| 95–99 | 0.1 | 0.3 | −0.06 | 0.1 | 0.2 | −0.04 |
| Female sex | 47.7 | 54.1 | −0.13 | 47.9 | 46.8 | 0.02 |
| Medical history | ||||||
| Acute respiratory disease | 79.8 | 79.4 | 0.01 | 80.2 | 79.5 | 0.02 |
| Chronic liver disease | 8.2 | 7.4 | 0.03 | 8.1 | 8.3 | −0.01 |
| Chronic obstructive lung disease | 2.6 | 2.7 | −0.01 | 2.3 | 2.6 | −0.02 |
| Crohn’s disease | 0.1 | 0.1 | −0.01 | 0.1 | 0.1 | 0 |
| Dementia | 5.5 | 9.3 | −0.14 | 4.8 | 5.1 | −0.01 |
| Depressive disorder | 12.7 | 14.5 | −0.05 | 12.1 | 11.7 | 0.01 |
| Gastroesophageal reflux disease | 41.4 | 40.8 | 0.01 | 40.8 | 40.6 | 0 |
| Gastrointestinal hemorrhage | 3 | 3.3 | −0.01 | 2.8 | 2.8 | 0 |
| Hyperlipidemia | 83.8 | 68.3 | 0.37 | 83.7 | 84.9 | −0.03 |
| Hypertensive disorder | 66.9 | 56.8 | 0.21 | 65.9 | 67.2 | −0.03 |
| Lesion of liver | 5.1 | 4.7 | 0.02 | 5 | 5.3 | −0.01 |
| Obesity | 0.7 | 0.3 | 0.06 | 0.8 | 0.6 | 0.02 |
| Osteoarthritis | 23.3 | 24.1 | −0.02 | 23.1 | 22.6 | 0.01 |
| Pneumonia | 5.6 | 5.7 | −0.01 | 5 | 4.9 | 0 |
| Psoriasis | 1.4 | 1 | 0.04 | 1.4 | 1.1 | 0.02 |
| Schizophrenia | 1 | 1.4 | −0.03 | 1 | 1.2 | −0.02 |
| Urinary tract infectious disease | 7.2 | 7.1 | 0 | 6.6 | 6.3 | 0.01 |
| Visual system disorder | 51.6 | 47.8 | 0.08 | 51.4 | 50.9 | 0.01 |
| Cardiovascular disease | ||||||
| Atrial fibrillation | 3.5 | 2.2 | 0.07 | 3.1 | 3 | 0.01 |
| Cerebrovascular disease | 8.9 | 7.8 | 0.04 | 8.4 | 8.5 | 0 |
| Coronary arteriosclerosis | 4.8 | 2.2 | 0.14 | 4.6 | 4.4 | 0.01 |
| Heart disease | 30.7 | 22.2 | 0.19 | 29.2 | 30.1 | −0.02 |
| Heart failure | 12.7 | 8.3 | 0.14 | 11.5 | 11.6 | 0 |
| Ischemic heart disease | 20.1 | 12.8 | 0.2 | 19.2 | 20.1 | −0.02 |
| Peripheral vascular disease | 25.5 | 18.8 | 0.16 | 24.9 | 25.3 | −0.01 |
| Pulmonary embolism | 0.7 | 0.7 | 0 | 0.5 | 0.6 | −0.01 |
| Venous thrombosis | 1.5 | 1.5 | 0 | 1.4 | 1.3 | 0.01 |
| Neoplasms | ||||||
| Hematologic neoplasm | 0.5 | 0.6 | −0.01 | 0.5 | 0.7 | −0.02 |
| Malignant lymphoma | 0.1 | 0.2 | −0.02 | 0.1 | 0.2 | −0.02 |
| Malignant neoplasm of anorectum | 0.3 | 0.3 | −0.01 | 0.3 | 0.4 | −0.03 |
| Malignant neoplastic disease | 8.1 | 8.4 | −0.01 | 7.9 | 8.3 | −0.01 |
| Malignant tumor of breast | 0.8 | 0.8 | 0 | 0.8 | 0.7 | 0.01 |
| Malignant tumor of colon | 0.6 | 0.7 | 0 | 0.6 | 0.7 | −0.01 |
| Malignant tumor of lung | 0.3 | 0.4 | −0.01 | 0.3 | 0.4 | −0.03 |
| Malignant tumor of urinary bladder | 0.2 | 0.3 | −0.02 | 0.2 | 0.3 | −0.02 |
| Malignant neoplasm of prostate | 0.9 | 1 | −0.01 | 0.8 | 0.9 | 0 |
| Before PS Adjustment | After PS Adjustment | |||||
|---|---|---|---|---|---|---|
| SGLT2 Inhibitor | Non-SGLT2 Inhibitor | SMD | SGLT2 Inhibitor | Non-SGLT2 Inhibitor | SMD | |
| (n = 12,401) | (n = 164,471) | (n = 12,400) | (n = 11,513) | |||
| Age group | ||||||
| 15–19 | 0.1 | 0.6 | −0.09 | 0.1 | 0.2 | −0.03 |
| 20–24 | 0.6 | 0.9 | −0.04 | 0.7 | 0.7 | 0.01 |
| 25–29 | 0.9 | 1.4 | −0.04 | 1 | 0.8 | 0.02 |
| 30–34 | 1.7 | 2 | −0.03 | 1.7 | 1.4 | 0.03 |
| 35–39 | 3.6 | 3.3 | 0.02 | 3.6 | 3.3 | 0.01 |
| 40–44 | 6.8 | 5.4 | 0.06 | 7.1 | 7 | 0 |
| 45–49 | 8.2 | 6 | 0.09 | 8.6 | 8.6 | 0 |
| 50–54 | 11 | 8.6 | 0.08 | 11.6 | 11.6 | 0 |
| 55–59 | 13.3 | 10.1 | 0.1 | 13.9 | 14 | 0 |
| 60–64 | 17 | 15.1 | 0.05 | 17.2 | 16.9 | 0.01 |
| 65–69 | 14 | 14.3 | −0.01 | 13.8 | 13.7 | 0 |
| 70–74 | 10.4 | 11.3 | −0.03 | 9.8 | 9.9 | 0 |
| 75–79 | 6.4 | 8.2 | −0.07 | 5.8 | 6.1 | −0.01 |
| 80–84 | 3.9 | 6.7 | −0.13 | 3.4 | 3.5 | −0.01 |
| 85–89 | 1.6 | 3.9 | −0.14 | 1.3 | 1.5 | −0.02 |
| 90–94 | 0.4 | 1.5 | −0.1 | 0.3 | 0.4 | −0.02 |
| Female sex | 47.7 | 54.1 | −0.13 | 46.8 | 46.2 | 0.01 |
| Medical history: General | ||||||
| Acute respiratory disease | 79.8 | 79.4 | 0.01 | 79.7 | 78.8 | 0.02 |
| Chronic liver disease | 8.2 | 7.4 | 0.03 | 8 | 8.4 | −0.02 |
| Chronic obstructive lung disease | 2.6 | 2.7 | −0.01 | 1.8 | 2.2 | −0.03 |
| Crohn’s disease | 0.1 | 0.1 | −0.01 | 0.1 | 0.1 | −0.01 |
| Dementia | 5.5 | 9.3 | −0.14 | 4.3 | 4.6 | −0.01 |
| Depressive disorder | 12.7 | 14.5 | −0.05 | 11.2 | 10.9 | 0.01 |
| Gastroesophageal reflux disease | 41.4 | 40.8 | 0.01 | 39.7 | 39.5 | 0 |
| Gastrointestinal hemorrhage | 3 | 3.3 | −0.01 | 2.7 | 2.5 | 0.01 |
| Hyperlipidemia | 83.8 | 68.3 | 0.37 | 83.8 | 85.6 | −0.05 |
| Hypertensive disorder | 66.9 | 56.8 | 0.21 | 65.8 | 67.7 | −0.04 |
| Lesion of liver | 5.1 | 4.7 | 0.02 | 5.1 | 5.3 | −0.01 |
| Obesity | 0.7 | 0.3 | 0.06 | 0.7 | 0.6 | 0.02 |
| Osteoarthritis | 23.3 | 24.1 | −0.02 | 22.5 | 22.2 | 0.01 |
| Pneumonia | 5.6 | 5.7 | −0.01 | 1.9 | 1.6 | 0.02 |
| Psoriasis | 1.4 | 1 | 0.04 | 1.4 | 1.2 | 0.02 |
| Renal impairment | 6.5 | 5.4 | 0.04 | 5.6 | 5.7 | −0.01 |
| Rheumatoid arthritis | 2.4 | 2.9 | −0.03 | 2.2 | 2.2 | 0 |
| Schizophrenia | 1 | 1.4 | −0.03 | 0.9 | 1.2 | −0.03 |
| Ulcerative colitis | 0.1 | 0.2 | −0.01 | 0.1 | 0.1 | −0.01 |
| Urinary tract infectious disease | 7.2 | 7.1 | 0 | 6.5 | 6 | 0.02 |
| Visual system disorder | 51.6 | 47.8 | 0.08 | 50.9 | 50.4 | 0.01 |
| Medical history: Cardiovascular disease | −0.02 | |||||
| Atrial fibrillation | 3.5 | 2.2 | 0.07 | 3 | 3 | 0 |
| Cerebrovascular disease | 8.9 | 7.8 | 0.04 | 8.2 | 8.3 | 0 |
| Coronary arteriosclerosis | 4.8 | 2.2 | 0.14 | 4.6 | 4.4 | 0.01 |
| Heart disease | 30.7 | 22.2 | 0.19 | 28.8 | 29.9 | −0.02 |
| Heart failure | 12.7 | 8.3 | 0.14 | 11.2 | 11.4 | −0.01 |
| Ischemic heart disease | 20.1 | 12.8 | 0.2 | 18.8 | 19.8 | −0.02 |
| Peripheral vascular disease | 25.5 | 18.8 | 0.16 | 24.6 | 24.9 | −0.01 |
| Pulmonary embolism | 0.7 | 0.7 | 0 | 0.5 | 0.5 | 0 |
| Venous thrombosis | 1.5 | 1.5 | 0 | 1.4 | 1.3 | 0.01 |
| Medical history: Neoplasms | ||||||
| Hematologic neoplasm | 0.5 | 0.6 | −0.01 | 0.5 | 0.7 | −0.03 |
| Malignant lymphoma | 0.1 | 0.2 | −0.02 | 0.1 | 0.1 | −0.01 |
| Malignant neoplasm of anorectum | 0.3 | 0.3 | −0.01 | 0.3 | 0.5 | −0.03 |
| Malignant neoplastic disease | 8.1 | 8.4 | −0.01 | 7.7 | 8.1 | −0.02 |
| Malignant tumor of breast | 0.8 | 0.8 | 0 | 0.8 | 0.8 | 0 |
| Malignant tumor of colon | 0.6 | 0.7 | 0 | 0.6 | 0.7 | −0.01 |
| Malignant tumor of lung | 0.3 | 0.4 | −0.01 | 0.2 | 0.3 | −0.02 |
| Malignant tumor of urinary bladder | 0.2 | 0.3 | −0.02 | 0.2 | 0.3 | −0.01 |
| Malignant neoplasm of prostate | 0.9 | 1 | −0.01 | 0.9 | 0.8 | 0 |
| Crude Population | Propensity Score-Matched Population | |||||||
|---|---|---|---|---|---|---|---|---|
| MACCE | SGLT2 inhibitor (n = 11,516) | Non-SGLT2 inhibitor (n = 161,166) | Unadjusted HR (95% CI) | p value | SGLT2 inhibitor (n = 11,513) | Non-SGLT2 inhibitor (n = 11,513) | Adjusted HR (95% CI) | p value |
| 103 (0.89) | 2057 (1.28) | 0.70 (0.57–0.85) | <0.01 | 103 (0.89) | 151 (1.31) | 0.71 (0.53–0.94) | 0.02 | |
| All-cause death | SGLT2 inhibitor (n = 14,319) | Non-SGLT2 inhibitor (n = 192,216) | Unadjusted HR (95% CI) | p value | SGLT2 inhibitor (n = 14,313) | Non-SGLT2 inhibitor (n = 14,313) | Adjusted HR (95% CI) | p value |
| 157 (1.10) | 2901 (1.51) | 0.72 (0.61–0.84) | <0.01 | 157 (1.10) | 193 (1.35) | 0.80 (0.64–1.01) | 0.06 | |
| Myocardial infarction | SGLT2 inhibitor (n = 13,591) | Non-SGLT2 inhibitor (n = 187,149) | Unadjusted HR (95% CI) | p value | SGLT2 inhibitor (n = 13,589) | Non-SGLT2 inhibitor (n = 13,589) | Adjusted HR (95% CI) | p value |
| 16 (0.12) | 223 (0.12) | 0.98 (0.57–1.58) | 0.95 | 16 (0.12) | 26 (0.19) | 0.68 (0.35–1.30) | 0.26 | |
| Stroke | SGLT2 inhibitor (n = 12,435) | Non-SGLT2 inhibitor (n = 167,593) | Unadjusted HR (95% CI) | p value | SGLT2 inhibitor (n = 12,426) | Non-SGLT2 inhibitor (n = 12,426) | Adjusted HR (95% CI) | p value |
| 23 (0.18) | 395 (0.24) | 0.78 (0.50–1.16) | 0.25 | 23 (0.18) | 44 (0.35) | 0.62 (0.32–1.18) | 0.16 | |
| Heart failure | SGLT2 inhibitor (n = 11,671) | Non-SGLT2 inhibitor (n = 166,606) | Unadjusted HR (95% CI) | p value | SGLT2 inhibitor (n = 11,670) | Non-SGLT2 inhibitor (n = 11,670) | Adjusted HR (95% CI) | p value |
| 81 (0.70) | 1257 (0.75) | 0.92 (0.73–1.44) | 0.44 | 81 (0.70) | 125 (1.07) | 0.65 (0.45–0.89) | 0.01 | |
| Crude Population | Propensity Score-Matched Population | |||||||
|---|---|---|---|---|---|---|---|---|
| Pneumonia | SGLT2 inhibitor (n = 12,401) | Non-SGLT2 inhibitor (n = 164,471) | Unadjusted HR (95% CI) | p value | SGLT2 inhibitor (n = 12,400) | Non-SGLT2 inhibitor (n = 12,400) | Adjusted HR (95% CI) | p value |
| 552 (4.45) | 6915 (4.20) | 1.06 (0.97–1.15) | 0.20 | 552 (4.45) | 544 (4.39) | 1.03 (0.91–1.16) | 0.62 | |
| Sepsis | SGLT2 inhibitor (n = 14,068) | Non-SGLT2 inhibitor (n = 188,432) | Unadjusted HR (95% CI) | p value | SGLT2 inhibitor (n = 14,063) | Non-SGLT2 inhibitor (n = 14,063) | Adjusted HR (95% CI) | p value |
| 33 (0.23) | 575 (0.31) | 0.76 (0.53–1.07) | 0.13 | 33 (0.23) | 39 (0.28) | 0.78 (0.46–1.31) | 0.36 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, K.R.; Chun, K.J.; Kim, B.S.; Lee, S. The Effect of Sodium–Glucose Cotransporter-2 Inhibitors on COVID-19 Patients with Type 2 Diabetes Mellitus: A Retrospective Cohort Study Using the Common Data Model. J. Clin. Med. 2024, 13, 431. https://doi.org/10.3390/jcm13020431
Lim KR, Chun KJ, Kim BS, Lee S. The Effect of Sodium–Glucose Cotransporter-2 Inhibitors on COVID-19 Patients with Type 2 Diabetes Mellitus: A Retrospective Cohort Study Using the Common Data Model. Journal of Clinical Medicine. 2024; 13(2):431. https://doi.org/10.3390/jcm13020431
Chicago/Turabian StyleLim, Kyoung Ree, Kwang Jin Chun, Bum Sung Kim, and Seunghwa Lee. 2024. "The Effect of Sodium–Glucose Cotransporter-2 Inhibitors on COVID-19 Patients with Type 2 Diabetes Mellitus: A Retrospective Cohort Study Using the Common Data Model" Journal of Clinical Medicine 13, no. 2: 431. https://doi.org/10.3390/jcm13020431