
Analysis of Pain Management after Anatomic VATS Resection in Austrian Thoracic Surgery Units
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Regional Anesthesia
3.2. Opioid Usage
3.3. Postoperative Pain Medication
3.4. Discharge Medication
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goto, T. What is the best pain control after thoracic surgery? J. Thorac. Dis. 2018, 10, 1335–1338. [Google Scholar] [CrossRef] [PubMed]
- Mercieri, M.; D’andrilli, A.; Arcioni, R. Improving postoperative pain management after video-assisted thoracic surgery lung resection contributes to enhanced recovery, but guidelines are still lacking. J. Thorac. Dis. 2018, 10, S983–S987. [Google Scholar] [CrossRef] [PubMed]
- Elmore, B.; Nguyen, V.; Blank, R.; Yount, K.; Lau, C. Pain Management Following Thoracic Surgery. Thorac. Surg. Clin. 2015, 25, 393–409. [Google Scholar] [CrossRef] [PubMed]
- Allain, P.-A.; Carella, M.; Agrafiotis, A.C.; Burey, J.; Assouad, J.; Hafiani, E.-M.; Ynineb, Y.; Bonnet, F.; Garnier, M.; Quesnel, C. Comparison of several methods for pain management after video-assisted thoracic surgery for pneumothorax: An observational study. BMC Anesthesiol. 2019, 19, 120. [Google Scholar] [CrossRef] [PubMed]
- Batchelor, T.J.P.; Rasburn, N.J.; Abdelnour-Berchtold, E.; Brunelli, A.; Cerfolio, R.J.; Gonzalez, M.; Ljungqvist, O.; Petersen, R.H.; Popescu, W.M.; Slinger, P.D.; et al. Guidelines for enhanced recovery after lung surgery: Recommendations of the Enhanced Recovery after Surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS). Eur. J. Cardio-Thorac. Surg. 2019, 55, 91–115. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, D.; Stamer, U.M.; Pogatzki-Zahn, E.; Zaslansky, R.; Tanase, N.V.; Perruchoud, C.; Kranke, P.; Komann, M.; Lehman, T.; Meissner, W. Chronic postsurgical pain in Europe: An observational study. Eur. J. Anaesthesiol. 2015, 32, 725–734. [Google Scholar] [CrossRef] [PubMed]
- Guimaraes-Pereira, L.; Valdoleiros, I.; Reis, P.; Abelha, F. Evaluating Persistent Postoperative Pain in One Tertiary Hospital: Incidence, Quality of Life, Associated Factors, and Treatment. Anesthesiol. Pain Med. 2016, 6, e36461. [Google Scholar] [CrossRef] [PubMed]
- Chou, R.; Gordon, D.B.; de Leon-Casasola, O.A.; Rosenberg, J.M.; Bickler, S.; Brennan, T.; Carter, T.; Cassidy, C.L.; Chittenden, E.H.; Degenhardt, E.; et al. Management of Postoperative Pain: A Clinical Practice Guideline from the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J. Pain 2016, 17, 131–157. [Google Scholar] [CrossRef]
- Thompson, C.; French, D.G.; Costache, I. Pain management within an enhanced recovery program after thoracic surgery. J. Thorac. Dis. 2018, 10 (Suppl. S32), S3773–S3780. [Google Scholar] [CrossRef]
- Ziarnik, E.; Grogan, E.L. Post-lobectomy early complications. Thorac. Surg. Clin. 2015, 25, 355–364. [Google Scholar] [CrossRef]
- Karcz, M.; Papadakos, P.J. Respiratory complications in the postanesthesia care unit: A review of pathophysiological mechanisms. Can. J. Respir. Ther. 2013, 49, 21–29. [Google Scholar] [PubMed]
- Blanco, C.; Wiley, T.R.A.; Lloyd, J.J.; Lopez, M.F.; Volkow, N.D. America’s opioid crisis: The need for an integrated public health approach. Transl. Psychiatry 2020, 10, 167. [Google Scholar] [CrossRef] [PubMed]
- Bendixen, M.; Jørgensen, O.D.; Kronborg, C.; Andersen, C.; Licht, P.B. Postoperative pain and quality of life after lobectomy via video-assisted thoracoscopic surgery or anterolateral thoracotomy for early stage lung cancer: A randomised controlled trial. Lancet Oncol. 2016, 17, 836–844. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, M.-J.; Wang, K.-C.; Liu, H.-P.; Gonzalez-Rivas, D.; Wu, C.-Y.; Liu, Y.-H.; Wu, Y.-C.; Chao, Y.-K.; Wu, C.-F. Management of acute postoperative pain with continuous intercostal nerve block after single port video-assisted thoracoscopic anatomic resection. J. Thorac. Dis. 2016, 8, 3563–3571. [Google Scholar] [CrossRef] [PubMed]
- Ponholzer, F.; Ng, C.; Maier, H.; Dejaco, H.; Schlager, A.; Lucciarini, P.; Öfner, D.; Augustin, F. Intercostal Catheters for Postoperative Pain Management in VATS Reduce Opioid Consumption. J. Clin. Med. 2021, 10, 372. [Google Scholar] [CrossRef] [PubMed]
- Wildgaard, K.; Petersen, R.H.; Hansen, H.J.; Møller-Sørensen, H.; Ringsted, T.K.; Kehlet, H. Multimodal analgesic treatment in video-assisted thoracic surgery lobectomy using an intraoperative intercostal catheter. Eur. J. Cardio-Thorac. Surg. 2012, 41, 1072–1077. [Google Scholar] [CrossRef] [PubMed]
- Andrade, S.; Bartels, D.B.; Lange, R.; Sandford, L.; Gurwitz, J. Safety of metamizole: A systematic review of the literature. J. Clin. Pharm. Ther. 2016, 41, 459–477. [Google Scholar] [CrossRef] [PubMed]
- Kötter, T.; da Costa, B.R.; Fässler, M.; Blozik, E.; Linde, K.; Jüni, P.; Reichenbach, S.; Scherer, M. Metamizole-Associated Adverse Events: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0122918. [Google Scholar] [CrossRef]
- Hoffmann, F.; Bantel, C.; von Rosen, F.T.; Jobski, K. Regional Differences in Prescribing Patterns of Metamizole in Germany Based on Data from 70 Million Persons. Int. J. Environ. Res. Public Health 2020, 17, 3892. [Google Scholar] [CrossRef]
- Shah, R.R. Metamizole (dipyrone)-induced agranulocytosis: Does the risk vary according to ethnicity? J. Clin. Pharm. Ther. 2019, 44, 129–133. [Google Scholar] [CrossRef]
- Gostin, L.O.; Hodge, J.G.; Noe, S.A. Reframing the Opioid Epidemic as a National Emergency. JAMA 2017, 318, 1539–1540. [Google Scholar] [CrossRef] [PubMed]
- Guertin, J.R.; Pagé, M.G.; Tarride, J.-É.; Talbot, D.; Watt-Watson, J.; Choinière, M. Just how much does it cost? A cost study of chronic pain following cardiac surgery. J. Pain Res. 2018, 11, 2741–2759. [Google Scholar] [CrossRef] [PubMed]
- Tong, Y.; Wei, P.; Wang, S.; Sun, Q.; Cui, Y.; Ning, N.; Chen, S.; He, X. Characteristics of Postoperative Pain After VATS and Pain-Related Factors: The Experience in National Cancer Center of China. J. Pain Res. 2020, 13, 1861–1867. [Google Scholar] [CrossRef] [PubMed]
- Bayman, E.O.; Parekh, K.R.; Keech, J.; Selte, A.; Brennan, T.J. A Prospective Study of Chronic Pain after Thoracic Surgery. Anesthesiology 2017, 126, 938–951. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhou, R.; Hou, B.; Tang, S.; Hao, J.; Gu, X.; Ma, Z.; Zhang, J. Incidence and risk factors for chronic postsurgical pain following video-assisted thoracoscopic surgery: A retrospective study. BMC Surg. 2022, 22, 76. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Li, S.; Liang, N.; Liu, W.; Liu, H.; Liu, H. Postoperative pain experiences in Chinese adult patients after thoracotomy and video-assisted thoracic surgery. J. Clin. Nurs. 2017, 26, 2744–2754. [Google Scholar] [CrossRef]
- Flor, H. Painful memories. Can we train chronic pain patients to ‘forget’ their pain? EMBO Rep. 2002, 3, 288–291. [Google Scholar] [CrossRef]
- Babar, L.; Modi, P.; Anjum, F. Lung Cancer Screening; StatPearls: Treasure Island, FL, USA, 2023. [Google Scholar]
- Indini, A.; Rijavec, E.; Bareggi, C.; Grossi, F. Novel treatment strategies for early-stage lung cancer: The oncologist’s perspective. J. Thorac. Dis. 2020, 12, 3390–3398. [Google Scholar] [CrossRef]


{kind=link}
| Do You Use Regional Anesthesia Procedures as a Standard for VATS Lobectomies? | Yes: 9, No: 0 |
|---|---|
| - Intercostal nerve block (ICNB; single-shot intraoperative) | 5 |
| - Peridural/epidural anesthesia (PDA) | 2 |
| - Intercostal catheter (ICC) | 3 |
| - Thoracic paravertebral block (TPVB) | 1 |
| - Serratus plane block | 0 |
| - Others: | 0 |
| If regional anesthesia procedures are used, is a continuous flow rate or patient-controlled analgesia (PCA) used? | |
| - Continuous | 0 |
| - PCA | 0 |
| - Continuous with patient-controlled bolus delivery | 6 |
| Does your department have a standard for pain management in patients after VATS lobectomies? | |
| - Yes | 9 |
| - No | 0 |
| Which of the following pain medications do your patients receive as standard therapy during their inpatient stay after VATS lobectomy? If medication is administered at VAS, please specify from which VAS range. | |
| - Paracetamol | 5/9 |
| - Fixed schedule or at VAS | 4 vs. 1 |
| - Mode of administration: oral intravenous | both in 5/5 |
| - Ibuprofen | 1/9 |
| - Fixed schedule or at VAS | 1 vs. 0 |
| - Mode of administration: oral intravenous | oral |
| - Dexibuprofen | 0/9 |
| - Fixed schedule or at VAS | n.a. |
| - Metamizole | 8/9 |
| - Fixed schedule or at VAS | 6 vs. 2 |
| - Mode of administration: oral intravenous | both in 8/8 |
| - Diclofenac | 3/9 |
| - Fixed schedule or at VAS | 2 vs. 1 |
| - Mode of administration: oral intravenous | both in 3/3 |
| - Gabapentin | 0/9 |
| - Fixed schedule or at VAS | n.a. |
| - Mode of administration: oral intravenous | n.a. |
| - Piritramide | 6/9 |
| - Fixed schedule or at VAS | 0 vs. 6 |
| - Mode of administration: intravenous subcutaneous | both in 6/6 |
| - Hydromorphone hydrochloride | 4/9 |
| - Fixed schedule or at VAS | 1 vs. 3 |
| - Mode of administration: oral intravenous subcutaneous | oral in 4/4 |
| - Tramadol hydrochloride | 1/9 |
| - Fixed schedule or at VAS | 0 vs. 1 |
| - Mode of administration: oral intravenous subcutaneous | oral in 1/1 |
| - Others: - Lornoxicam, Oxycodon, Oxycodon/Naloxon, Diclofenac/Orphenadrin | one each, 3 on a fixed schedule, Oxycodon depending on VAS |
| How restrictively are opiates used for postoperative pain management in your practice? | |
| - Opioids are prescribed for every patient | 2/9 |
| - According to VAS. If so, from which VAS: | 5/9 |
| - Rather restrictive/attempt opiate-free analgesia | 2/9 |
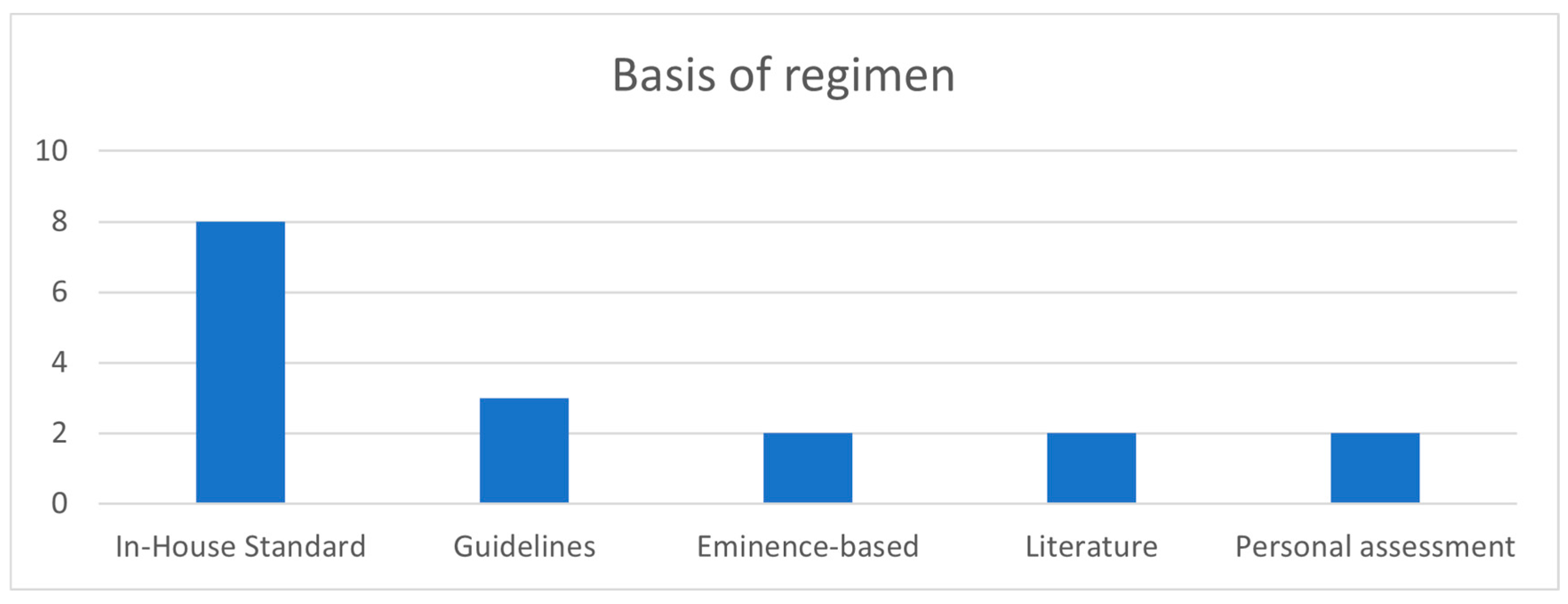
| Which of the following is your pain medication regimen based on? (multiple answers possible) | |
| - Guidelines | 3 |
| - Literature | 2 |
| - “Eminence-based” | 2 |
| - In-house standard | 8 |
| - Personal assessment | 2 |
| - Other: | 0 |
| What pain medication do your patients receive at discharge and for how long? | Metamizole in 5/9, NSAID in 5/9, Paracetamol in 3/9, Duration based on symptoms in 9/9 |
| Do you use any other procedures for analgesia during or after the patient’s inpatient stay, which have not yet been explained in the above questions? | No: 9/9 |
| Are your patients regularly surveyed regarding their pain? | |
| - No | 0 |
| - Yes. If so: at what times? | 9/9, median 3 times/24 h, range 3–6 times/24 h |
| How many anatomical minimally invasive resections are performed at your center per year? | median 100/y, range 32–250/y |
| Do you use a uniportal or multiportal (two or more ports) approach? | multiport approach n = 8, uniportal n = 1 |
| Do you use a digital thoracic drainage system? | Yes: 7, No: 2 |
| Please describe your chest drain management with regard to criteria for drain removal: | |
| - Do you look at the quality of the fluid? | Yes: 9 |
| - Maximum drainage amount over 24 h? | median 300 mL/24 h, range 100–400 mL/24 h |
| - If a digital thoracic drainage system is used: | |
| ○ Maximum air flow in mL/min? | median 20 mL/min, range 0–40 mL/min |
| Technique | Usage (%) | By Surgeons | By Anesthesiologists |
|---|---|---|---|
| SSINB | 5 out of 9 (55.6) | X | |
| ICC | 3 out of 9 (33.3) | X | |
| EA | 2 out of 9 (22.2) | X | |
| TPVB | 1 out of 9 (11.1) | X | X |
| Medication | Fixed Schedule | Depending on VAS | Overall Usage |
|---|---|---|---|
| Metamizole | 6 | 2 | 8 out of 9 |
| Piritramide | 0 | 6 | 6 out of 9 |
| Paracetamol | 4 | 1 | 5 out of 9 |
| Hydromorphone | 1 | 3 | 4 out of 9 |
| Diclofenac * | 2 | 1 | 3 out of 9 |
| Ibuprofen | 1 | 0 | 1 out of 9 |
| Tramadol | 0 | 1 | 1 out of 9 |
| Lornoxicam | 1 | 0 | 1 out of 9 |
| Oxycodon | 0 | 1 | 1 out of 9 |
| Oxycodon/Naloxon | 1 | 0 | 1 out of 9 |
| Diclofenac/Orphenadrin | 1 | 0 | 1 out of 9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ponholzer, F.; Schweiger, T.; Ghanim, B.; Maier, H.; Hutter, J.; Tomaselli, F.; Krause, A.; Müller, M.; Lindenmann, J.; Spruk, G.; et al. Analysis of Pain Management after Anatomic VATS Resection in Austrian Thoracic Surgery Units. J. Clin. Med. 2024, 13, 80. https://doi.org/10.3390/jcm13010080
Ponholzer F, Schweiger T, Ghanim B, Maier H, Hutter J, Tomaselli F, Krause A, Müller M, Lindenmann J, Spruk G, et al. Analysis of Pain Management after Anatomic VATS Resection in Austrian Thoracic Surgery Units. Journal of Clinical Medicine. 2024; 13(1):80. https://doi.org/10.3390/jcm13010080
Chicago/Turabian StylePonholzer, Florian, Thomas Schweiger, Bahil Ghanim, Herbert Maier, Jörg Hutter, Florian Tomaselli, Axel Krause, Michael Müller, Jörg Lindenmann, Gero Spruk, and et al. 2024. "Analysis of Pain Management after Anatomic VATS Resection in Austrian Thoracic Surgery Units" Journal of Clinical Medicine 13, no. 1: 80. https://doi.org/10.3390/jcm13010080