

Comparative Analysis of the Visual, Refractive and Aberrometric Outcome with the Use of 2 Intraocular Refractive Segment Multifocal Lenses
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Group and Intraocular Lenses
2.3. Surgical Technique
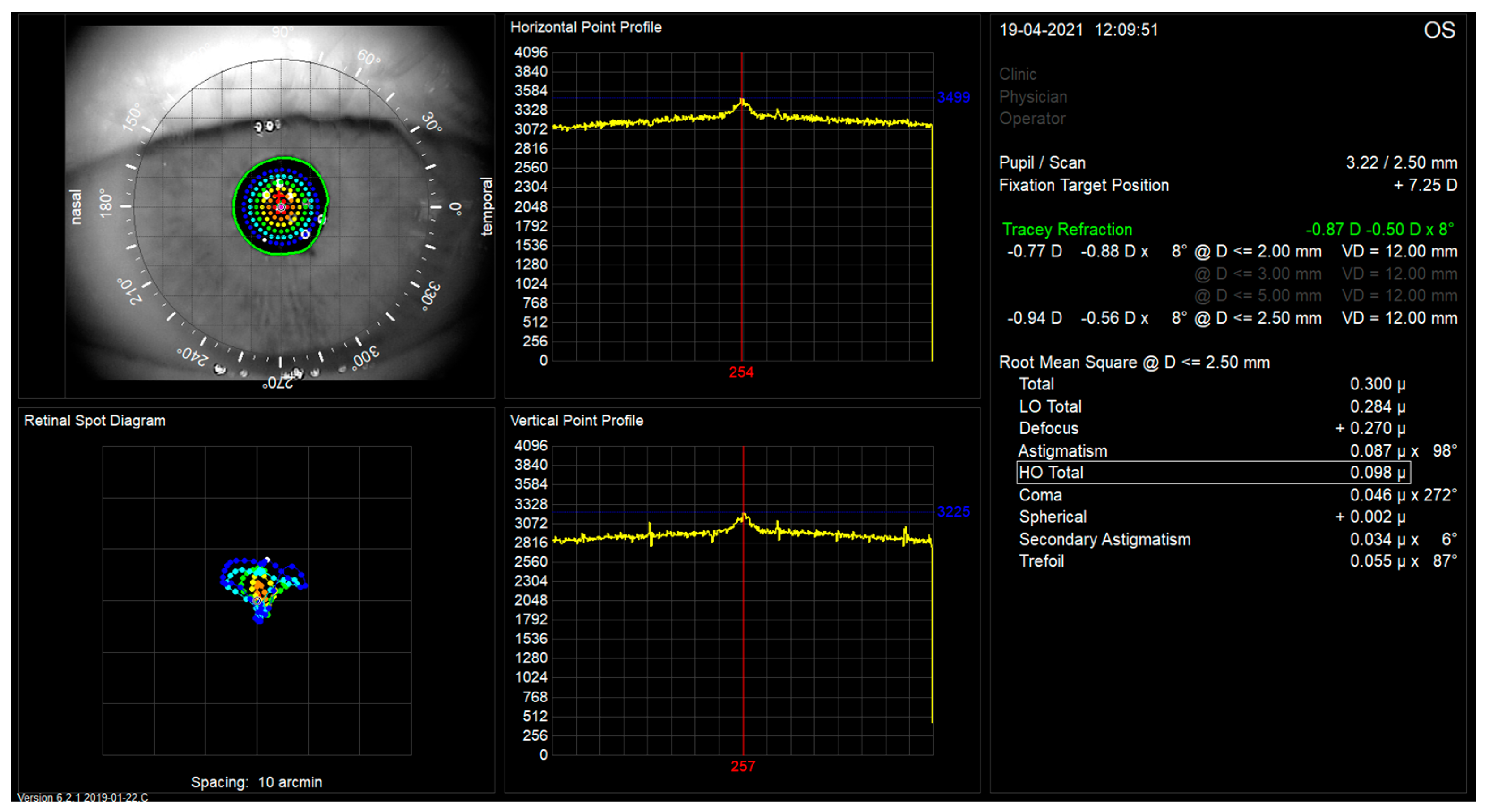
2.4. Examination
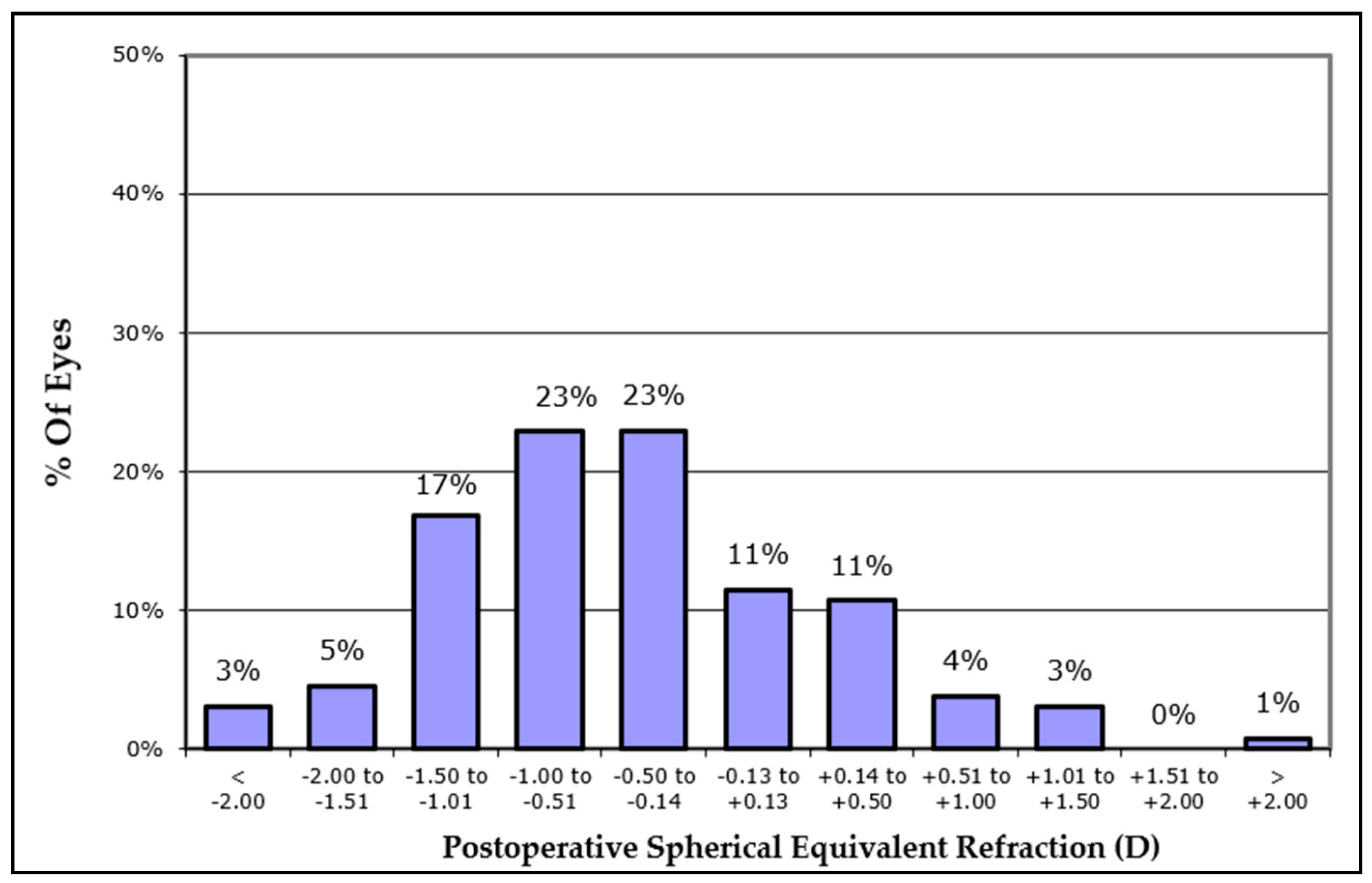
2.5. Spherical Equivalent Refractive Accuracy
3. Results
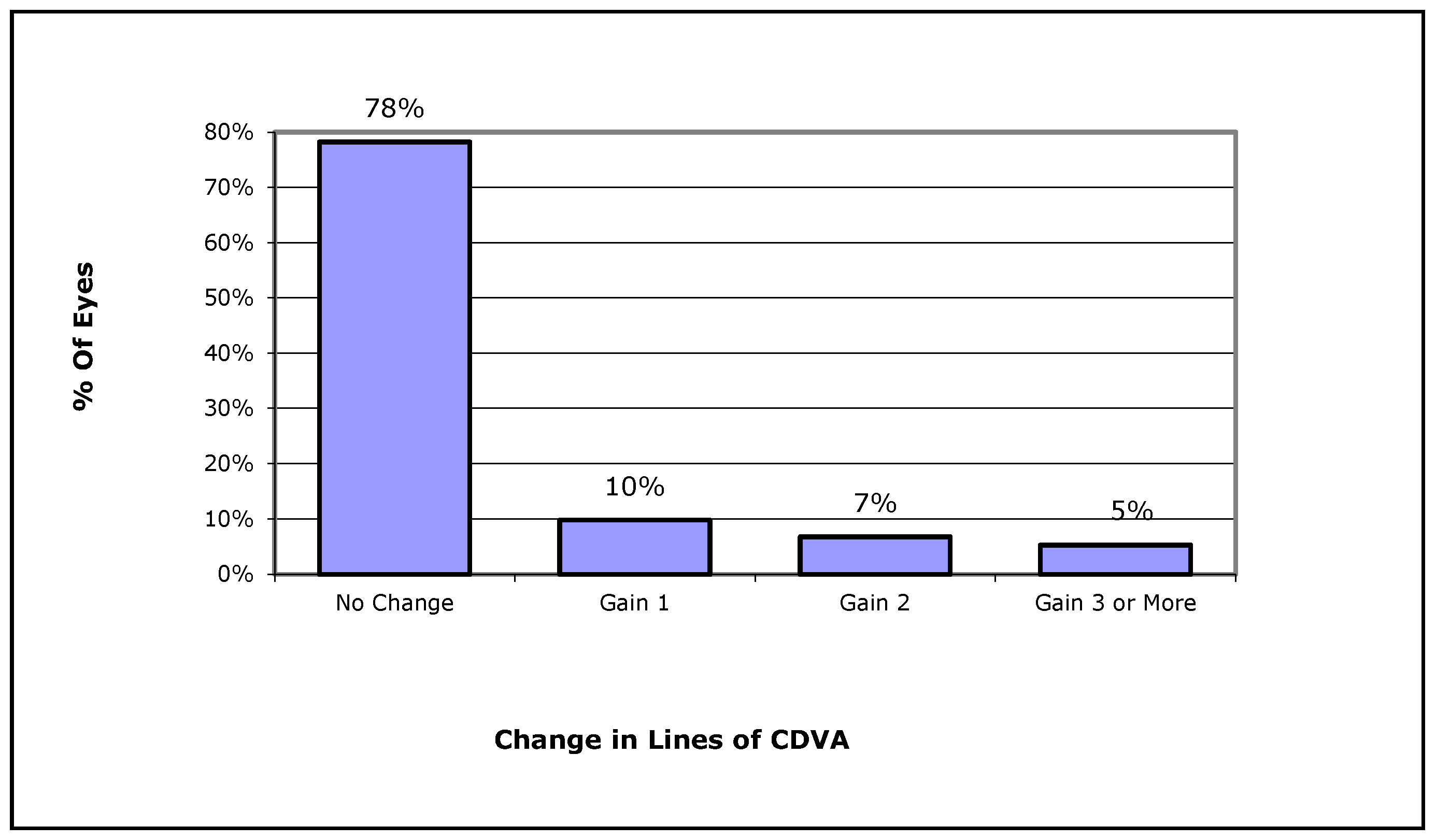
3.1. Visual Acuity and Refraction
3.2. Relationship between Visual Acuity and the Tear Film Break-Up Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alio, J.L.; Plaza-Puche, A.B.; Férnandez-Buenaga, R.; Pikkel, J.; Maldonado, M. Multifocal intraocular lenses: An overview. Surv. Ophthalmol. 2017, 62, 611–634. [Google Scholar] [CrossRef] [PubMed]
- Breyer, D.R.H.; Beckers, L.; Ax, T.; Kaymak, H.; Klabe, K.; Kretz, F.T.A. Aktuelle Übersicht: Multifokale Linsen und Extended-Depth-of-Focus-Intraokularlinsen [Current Review: Multifocal Intraocular Lenses and Extended Depth of Focus Intraocular Lenses]. Klin. Monbl. Augenheilkd. 2020, 237, 943–957. [Google Scholar] [CrossRef] [PubMed]
- Niazi, S.; Gatzioufas, Z.; Dhubhghaill, S.N.; Moshirfar, M.; Faramarzi, A.; Mohammadi, F.; Kheiri, B.; Peyman, A.; Heidari, M.; Doroodgar, F. Association of Patient Satisfaction with Cataract Grading in Five Types of Multifocal IOLs. Adv. Ther. 2023. Published online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Galvis, V.; Escaf, L.C.; Escaf, L.J.; Tello, A.; Rodríguez, L.D.; Lapid-Gortzak, R.; Carreño, N.I.; Berrospi, R.D.; Niño, C.A.; Viberg, A.; et al. Visual and satisfaction results with implantation of the trifocal Panoptix® intraocular lens in cataract surgery. J. Optom. 2022, 15, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Lubiński, W.; Podborączyńska-Jodko, K.; Kirkiewicz, M.; Mularczyk, M.; Post, M. Comparison of visual outcomes after implantation of AtLisa tri 839 MP and Symfony intraocular lenses. Int. Ophthalmol. 2020, 40, 2553–2562. [Google Scholar] [CrossRef] [PubMed]
- Ang, R.E.T. Long-term trifocal toric intraocular lens outcomes in Asian eyes after cataract surgery. J. Cataract. Refract. Surg. 2023, 49, 832–839. [Google Scholar] [CrossRef] [PubMed]
- Karam, M.; Alkhowaiter, N.; Alkhabbaz, A.; Aldubaikhi, A.; Alsaif, A.; Shareef, E.; Alazaz, R.; Alotaibi, A.; Koaik, M.; Jabbour, S.; et al. Extended Depth of Focus Versus Trifocal for Intraocular Lens Implantation: An Updated Systematic Review and Meta-Analysis. Am. J. Ophthalmol. 2023, 251, 52–70. [Google Scholar] [CrossRef]
- Pinero, D.P.; Espinosa, M.J.A.; Alio, J.L. LASIK outcomes following multifocal and monofocal intraocular lens implantation. J. Refract. Surg. 2010, 26, 569–577. [Google Scholar] [CrossRef]
- McNeely, R.N.; Pazo, E.; Spence, A.; Richoz, O.; Nesbit, M.A.; Moore, T.C.; Moore, J.E. Comparison of the visual performance and quality of vision with combined symmetrical inferonasal near addition versus inferonasal and superotemporal placement of rotationally asymmetric refractive multifocal intraocular lenses. J. Cataract. Refract. Surg. 2016, 42, 1721–1729. [Google Scholar] [CrossRef]
- Oshika, T.; Arai, H.; Fujita, Y.; Inamura, M.; Inoue, Y.; Noda, T.; Miyata, K. One-year clinical evaluation of rotationally asymmetric multifocal intraocular lens with +1.5 diopters near addition. Sci. Rep. 2019, 9, 13117. [Google Scholar] [CrossRef]
- Bellucci, R.; Morselli, S.; Pucci, V. Spherical aberration and coma with an aspherical and a spherical intraocular lens in normal age-matched eyes. J. Cataract. Refract. Surg. 2007, 33, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Werner, W.; Roth, E.H. Image properties of spherical as aspheric intraocular lenses. Klin. Mon. Augenheilkd. 1999, 214, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Charman, W.N.; Montés-Micó, R.; Radhakrishnan, H. Problems in the measurement of wavefront aberration for eyes implanted with diffractive bifocal and multifocal intraocular lenses. J. Refract. Surg. 2008, 24, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Fernández, J.; Rocha-de-Lossada, C.; Rodríguez-Vallejo, M. Objective Optical Quality With Multifocal Intraocular Lenses Should Stop to Be Used or Cautiously Interpreted. Asia Pac. J. Ophthalmol. 2022, 11, 569. [Google Scholar] [CrossRef]
- Vega, F.; Faria-Ribeiro, M.; Armengol, J.; Millán, M.S. Pitfalls of Using NIR-Based Clinical Instruments to Test Eyes Implanted with Diffractive Intraocular Lenses. Diagnostics 2023, 13, 1259. [Google Scholar] [CrossRef] [PubMed]
- D’Oria, F.; Scotti, G.; Sborgia, A.; Boscia, F.; Alessio, G. How Reliable Is Pyramidal Wavefront-Based Sensor Aberrometry in Measuring the In Vivo Optical Behaviour of Multifocal IOLs? Sensors 2023, 23, 3534. [Google Scholar] [CrossRef] [PubMed]
- Block, M.I.; Khitin, L.M.; Sade, R.M. Ethical process in human research published in thoracic surgery journals. Ann. Thorac. Surg. 2006, 82, 6–12. [Google Scholar] [CrossRef]
- Cione, F.; De Bernardo, M.; Gioia, M.; Oliviero, M.; Santoro, A.G.; Caputo, A.; Capasso, L.; Pagliarulo, S.; Rosa, N. A No-History Multi-Formula Approach to Improve the IOL Power Calculation after Laser Refractive Surgery: Preliminary Results. J. Clin. Med. 2023, 12, 2890. [Google Scholar] [CrossRef]
- Auffarth, G. Letnis Mplus: An Innovative Multifocal Lens Technology. CRSTEurope 2010. Available online: http://crstodayeurope.com/articles/2010-feb/lentis-mplus-an-innovative-multifocal-lens-technology (accessed on 11 December 2022).
- Matossian, C.; Chang, D.H.; Whitman, J.; Clinch, T.E.; Hu, J.; Ji, L.; Murakami, D.; Wang, Y.; Blackie, C.A. Preoperative Treatment of Meibomian Gland Dysfunction with a Vectored Thermal Pulsation System Prior to Extended Depth of Focus IOL Implantation. Ophthalmol. Ther. 2023, 12, 2427–2439. [Google Scholar] [CrossRef]
- Faria-Correia, F.; Lopes, B.; Monteiro, T.; Franqueira, N.; Ambrósio, R., Jr. Scheimpflug lens densitometry and ocular wavefront aberrations in patients with mild nuclear cataract. J. Cataract. Refract. Surg. 2016, 42, 405–411. [Google Scholar] [CrossRef]
- Alio, J.L.; ElKady, B.; Ortiz, D.; Bernabeu, G. Clinical outcomes and intraocular optical quality of a diffractive multifocal intraocular lens with asymmetrical light distribution. J. Cataract. Refract. Surg. 2008, 34, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Alfonso, J.F.; Fernandez-Vega, L.; Baamonde, M.B. Mont es-Mic o R. Prospective visual evaluation of apodized diffractive intraocular lenses. J. Cataract. Refract. Surg. 2007, 33, 1235–1243. [Google Scholar] [CrossRef] [PubMed]
- Alio, J.L.; ElKady, B.; Ortiz, D.; Bernabeu, G. Microincision multifocal intraocular lens with and without a capsular tension ring; optical quality and clinical outcomes. J. Cataract. Refract. Surg. 2008, 34, 1468–1475. [Google Scholar] [CrossRef] [PubMed]
- Rosen, E.; Alió, J.L.; Dick, H.B.; Dell, S.; Slade, S. Efficacy and safety of multifocal intraocular lenses following cataract and refractive lens exchange: Metaanalysis of peer-reviewed publications. J. Cataract. Refract. Surg. 2016, 42, 310–328. [Google Scholar] [CrossRef] [PubMed]
- Walkow, T.; Klemen, U.M. Patient satisfaction after implantation of diffractive designed multifocal intraocular lenses in dependence on objective parameters. Graefe Arch. Clin. Exp. Ophthalmol. 2001, 239, 683–687. [Google Scholar] [CrossRef] [PubMed]
- Montes-Mico, R.; Alio, J.L. Distance and near contrast sensitivity function after multifocal intraocular lens implantation. J. Cataract. Refract. Surg. 2003, 29, 703–711. [Google Scholar] [CrossRef] [PubMed]
- McNeely, R.N.; Pazo, E.; Spence, A.; Richoz, O.; Nesbit, M.A.; Moore, T.C.; Moore, J.E. Visual outcomes and patient satisfaction 3 and 12 months after implantation of a refractive rotationally asymmetric multifocal intraocular lens. J. Cataract. Refract. Surg. 2017, 43, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Pedrotti, E.; Mastropasqua, R.; Bonetto, J.; Demasi, C.; Aiello, F.; Nucci, C.; Mariotti, C.; Marchini, G. Quality of vision, patient satisfaction and long-term visual function after bilateral implantation of a low addition multifocal intraocular lens. Int. Ophthalmol. 2018, 38, 1709–1716. [Google Scholar] [CrossRef]
- Kim, K.H.; Kim, W.S. Visual outcome and Patient Satisfaction of low-power-added multifocal intraocular lens. Eye Contact Lens 2018, 44, 60–67. [Google Scholar] [CrossRef]
- Rosa, A.M.; Miranda, A.C.; Patricio, M.; McAliden, C.; Silva, F.L.; Murta, J.N.; Castelo-Branco, M. Functional Magnetic Resonance Imaging to Assess the Neurobehavioral Impact of Dysphotopsia with Multifocal Intraocular Lenses. Ophthalmology 2017, 124, 1280–1289. [Google Scholar] [CrossRef]
- Norrby, S. Sources of error in intraocular lens power calculation. J. Cataract. Refract. Surg. 2008, 34, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Langenbucher, A.; Szentmáry, N.; Cayless, A.; Bolz, M.; Hoffmann, P.; Wendelstein, J. Prediction of spectacle refraction uncertainties with discrete IOL power steps and manufacturing tolerances according to ISO using a Monte Carlo model. Br. J. Ophthalmol. 2023, 1–8. [Google Scholar] [CrossRef]
- Langenbucher, A.; Hoffmann, P.; Cayless, A.; Bolz, M.; Wendelstein, J.; Szentmáry, N. Impact of uncertainties in biometric parameters on intraocular lens power formula predicted refraction using a Monte-Carlo simulation. Acta Ophthalmol. 2023, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Kugelberg, M.; Lundström, M. Factors related to the degree of success in achieving target refraction in cataract surgery: Swedish National Cataract Register study. J. Cataract. Refract. Surg. 2008, 34, 1935–1939. [Google Scholar] [CrossRef] [PubMed]
- Hill, W.E.; Abulafia, A.; Wang, L.; Koch, D.D. Pursuing perfection in IOL calculations. II. Measurement foibles: Measurement errors, validation criteria, IOL constants, and lane length. J. Cataract. Refract. Surg. 2017, 43, 869–870. [Google Scholar] [CrossRef] [PubMed]
- D’Oria, F.; Nowrouzi, A.; Alio del Barrio, J.L.; Versaci, F.; Alio, J.L. Retinal Optical Quality of Multifocal Refractive and Monofocal Intraocular Lenses. Photonics 2021, 8, 559. [Google Scholar] [CrossRef]
- Alio, J.L.; D’Oria, F.; Toto, F.; Balgos, J.; Palazon, A.; Versaci, F.; Alio del Barrio, J.L. Retinal image quality with multifocal, EDoF.; and accommodative intraocular lenses as studied by piramidal aberrometry. Eye Vis. 2010, 8, 37. [Google Scholar] [CrossRef]
- Alió, J.L.; Pikkel, J. Multifocal Intraocular Lenses: The Art and the Practice. In Essentials in Ophthalmology; Springer International Publishing: Cham, Switzerland, 2014. [Google Scholar]
- Alio, J.L.; Colecha, J.R.; Pastor, S.; Rodriguez, A.; Artola, A. Symptomatic dry eye treatment with autologous platelet-rich plasma. Ophthalmic. Res. 2007, 39, 124–129. [Google Scholar] [CrossRef]
- De Bernardo, M.; Cione, F.; Rosa, N. Re: Turnbull et al.: Methods for intraocular lens power calculation in cataract surgery after radial keratotomy (Ophthalmology. 2020;127:45-51). Ophthalmology 2020, 127, e87. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tested Parameter | Control Group (Preoperative Measurement) | Patients w/Lentis Mplus15 Lens | Patients w/Lentis Mplus30 Lens | |||
|---|---|---|---|---|---|---|
| Means | SD | Mean | SD | Mean | SD | |
| HOA Total in µm | 0.25 | 0.24 | 0.23 | 0.11 | 0.38 | 0.17 |
| LOA Total in µm | 1.91 | 1.62 | 0.39 | 0.33 | 0.45 | 0.31 |
| Defocus in µm | 0.5 | 2.28 | 0.07 | 0.4 | 0.22 | 0.39 |
| Coma in µm | 0.14 | 0.2 | 0.1 | 0.06 | 0.16 | 0.07 |
| Spherical in µm | 0.02 | 0.09 | 0.05 | 0.03 | 0.02 | 0.06 |
| Trefoil in µm | 0.12 | 0.11 | 0.14 | 0.08 | 0.22 | 0.11 |
| Astigmatism in µm | 0.58 | 0.71 | 0.25 | 0.18 | 0.28 | 0.14 |
| Secondary Astigmatism in µm | 0.04 | 0.04 | 0.04 | 0.03 | 0.06 | 0.04 |
| UDVA EDTRS Letters | 55.57 | 23.96 | 81.24 | 5.55 | 79.81 | 8.24 |
| BCDVA EDTRS Letters | 81.44 | 7.32 | 81.74 | 4.62 | 82.03 | 7.12 |
| UNVA logMAR | 0.35 | 0.29 | 0.05 | 0.07 | 0.03 | 0.1 |
| TBUT in s | 8.31 | 2.42 | 5.62 | 1.48 | 5.1 | 1.96 |
| TraceRef SEQ in dpt | −1.28 | 4.65 | −0.25 | 0.65 | −0.6 | 0.87 |
| DEQ in dpt | 0.81 | 0.40 | 1.21 | 0.68 | ||
| Pupil diameter in mm | 3.85 | 1.04 | 3.19 | 0.84 | 2.89 | 0.70 |
| Group | n | M | SD | Me | Average Rank | H | df | p | |
|---|---|---|---|---|---|---|---|---|---|
| UDVA EDTRS letters | G0 | 103 | 55.57 | 23.96 | 58.90 | 73.39 | 80.95 | 2 | <0.001 |
| G1.5 | 42 | 81.24 | 5.55 | 83.00 | 155.86 | ||||
| G3.0 | 91 | 79.81 | 8.24 | 84.00 | 152.31 | ||||
| UNVA logMAR | G0 | 64 | 0.35 | 0.29 | 0.20 | 142.05 | 71.74 | 2 | <0.001 |
| G1.5 | 42 | 0.05 | 0.07 | 0.00 | 87.52 | ||||
| G3.0 | 91 | 0.03 | 0.10 | 0.00 | 74.02 | ||||
| TBUT in s | G0 | 107 | 8.31 | 2.42 | 8.00 | 165.07 | 81.15 | 2 | <0.001 |
| G1.5 | 42 | 5.62 | 1.48 | 6.00 | 94.56 | ||||
| G3.0 | 91 | 5.10 | 1.96 | 5.00 | 80.06 |
| Patients before surgery (control group) | HOA Total (n = 107) | rho Spearman significance | 0.13 |
| 0.187 | |||
| LOA Total (n = 107) | rho Spearman significance | −0.24 | |
| 0.014 | |||
| Patients with Mplus15 | HOA Total (n = 42) | rho Spearman significance | 0.14 |
| 0.373 | |||
| LOA Total (n = 42) | rho Spearman significance | −0.15 | |
| 0.336 | |||
| Patients with Mplus30 | HOA Total (n = 91) | rho Spearman significance | 0.03 |
| 0.762 | |||
| LOA Total (n = 91) | rho Spearman significance | −0.46 | |
| <0.001 |
| TBUT (s) | |||
|---|---|---|---|
| Patients before surgery (control group) | BCDVA (n = 103) | rho Spearman significance | −0.01 |
| 0.967 | |||
| BCNVA (n = 64) | rho Spearman significance | −0.10 | |
| 0.300 | |||
| Patients with Mplus15 | BCDVA (n = 42) | rho Spearman significance | 0.05 |
| 0.77 | |||
| BCNVA (n = 42) | rho Spearman significance | 0.18 | |
| 0.26 | |||
| Patients with Mplus30 | BCDVA (n = 91) | rho Spearman significance | 0.13 |
| 0.22 | |||
| BCNVA (n = 91) | rho Spearman significance | −0.16 | |
| 0.118 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Markuszewski, B.; Wylęgała, A.; Szentmáry, N.; Langenbucher, A.; Markuszewska, A.; Wylęgała, E. Comparative Analysis of the Visual, Refractive and Aberrometric Outcome with the Use of 2 Intraocular Refractive Segment Multifocal Lenses. J. Clin. Med. 2024, 13, 239. https://doi.org/10.3390/jcm13010239
Markuszewski B, Wylęgała A, Szentmáry N, Langenbucher A, Markuszewska A, Wylęgała E. Comparative Analysis of the Visual, Refractive and Aberrometric Outcome with the Use of 2 Intraocular Refractive Segment Multifocal Lenses. Journal of Clinical Medicine. 2024; 13(1):239. https://doi.org/10.3390/jcm13010239
Chicago/Turabian StyleMarkuszewski, Bartłomiej, Adam Wylęgała, Nóra Szentmáry, Achim Langenbucher, Anna Markuszewska, and Edward Wylęgała. 2024. "Comparative Analysis of the Visual, Refractive and Aberrometric Outcome with the Use of 2 Intraocular Refractive Segment Multifocal Lenses" Journal of Clinical Medicine 13, no. 1: 239. https://doi.org/10.3390/jcm13010239