
Cardiac Amyloidosis and Valvular Heart Disease
 , ,
, , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Aim of the Review
2.2. Structure of the Review
2.3. Conduction of Literature Review and Study Appraisal
3. Aortic Stenosis
3.1. Epidemiology
3.2. Pathophysiological Aspects
3.3. Diagnosis and Screening
3.4. Treatment and Outcomes
3.5. Potential Clinical Implications
4. Mitral Regurgitation
4.1. Epidemiology
4.2. Pathophysiological Aspects
4.3. Diagnosis and Screening
4.4. Treatment and Outcomes
4.5. Potential Clinical Implications
5. Tricuspid Regurgitation
5.1. Epidemiology
5.2. Pathophysiological Aspects
5.3. Diagnosis and Screening
5.4. Treatment and Outcomes
5.5. Potential Clinical Implications
6. Mitral and Tricuspid Stenosis
7. Gaps in Knowledge and Recommendations for Future Research
7.1. Aortic Stenosis
7.2. Mitral and Tricuspid Regurgitation
7.3. Considerations in Trial Design for VHD in CA
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
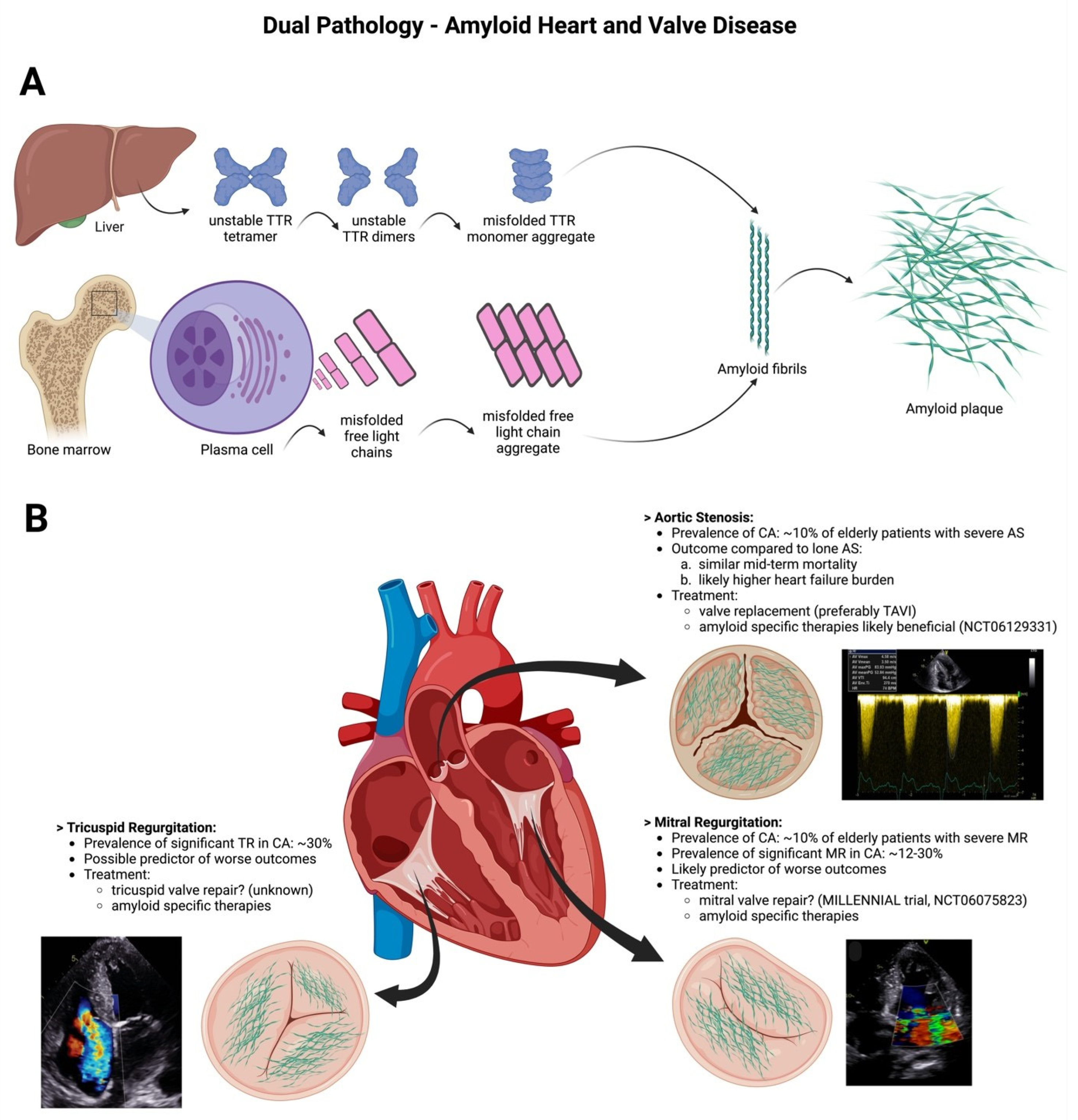
Appendix A. Central Illustration: Dual Pathology—Amyloid Heart and Valve Disease



References
- Ioannou, A.; Patel, R.K.; Razvi, Y.; Porcari, A.; Sinagra, G.; Venneri, L.; Bandera, F.; Masi, A.; Williams, G.E.; O’Beara, S.; et al. Impact of Earlier Diagnosis in Cardiac ATTR Amyloidosis Over the Course of 20 Years. Circulation 2022, 146, 1657–1670. [Google Scholar] [CrossRef] [PubMed]
- Gillmore, J.D.; Maurer, M.S.; Falk, R.H.; Merlini, G.; Damy, T.; Dispenzieri, A.; Wechalekar, A.D.; Berk, J.L.; Quarta, C.C.; Grogan, M.; et al. Nonbiopsy Diagnosis of Cardiac Transthyretin Amyloidosis. Circulation 2016, 133, 2404–2412. [Google Scholar] [CrossRef] [PubMed]
- Longhi, S.; Lorenzini, M.; Gagliardi, C.; Milandri, A.; Marzocchi, A.; Marrozzini, C.; Saia, F.; Ortolani, P.; Biagini, E.; Guidalotti, P.L.; et al. Coexistence of Degenerative Aortic Stenosis and Wild-Type Transthyretin-Related Cardiac Amyloidosis. JACC Cardiovasc. Imaging 2016, 9, 325–327. [Google Scholar] [CrossRef] [PubMed]
- Treibel, T.A.; Fontana, M.; Gilbertson, J.A.; Castelletti, S.; White, S.K.; Scully, P.R.; Roberts, N.; Hutt, D.F.; Rowczenio, D.M.; Whelan, C.J.; et al. Occult Transthyretin Cardiac Amyloid in Severe Calcific Aortic Stenosis: Prevalence and Prognosis in Patients Undergoing Surgical Aortic Valve Replacement. Circ. Cardiovasc. Imaging 2016, 9, e005066. [Google Scholar] [CrossRef] [PubMed]
- Castano, A.; Bokhari, S.; Maurer, M.S. Unveiling wild-type transthyretin cardiac amyloidosis as a significant and potentially modifiable cause of heart failure with preserved ejection fraction. Eur. Heart J. 2015, 36, 2595–2597. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, C.; Aschauer, S.; Kammerlander, A.A.; Schneider, M.; Poschner, T.; Duca, F.; Binder, C.; Koschutnik, M.; Stiftinger, J.; Goliasch, G.; et al. Light-chain and transthyretin cardiac amyloidosis in severe aortic stenosis: Prevalence, screening possibilities, and outcome. Eur. J. Heart Fail. 2020, 22, 1852–1862. [Google Scholar] [CrossRef] [PubMed]
- Dobner, S.; Pilgrim, T.; Hagemeyer, D.; Heg, D.; Lanz, J.; Reusser, N.; Gräni, C.; Afshar-Oromieh, A.; Rominger, A.; Langhammer, B.; et al. Amyloid Transthyretin Cardiomyopathy in Elderly Patients With Aortic Stenosis Undergoing Transcatheter Aortic Valve Implantation. J. Am. Heart Assoc. 2023, 12, e030271. [Google Scholar] [CrossRef]
- Scully, P.R.; Patel, K.P.; Treibel, T.A.; Thornton, G.D.; Hughes, R.K.; Chadalavada, S.; Katsoulis, M.; Hartman, N.; Fontana, M.; Pugliese, F.; et al. Prevalence and outcome of dual aortic stenosis and cardiac amyloid pathology in patients referred for transcatheter aortic valve implantation. Eur. Heart J. 2020, 41, 2759–2767. [Google Scholar] [CrossRef]
- Nitsche, C.; Scully, P.R.; Patel, K.P.; Kammerlander, A.A.; Koschutnik, M.; Dona, C.; Wollenweber, T.; Ahmed, N.; Thornton, G.D.; Kelion, A.D.; et al. Prevalence and Outcomes of Concomitant Aortic Stenosis and Cardiac Amyloidosis. J. Am. Coll. Cardiol. 2021, 77, 128–139. [Google Scholar] [CrossRef]
- Nitsche, C.; Mascherbauer, K.; Wollenweber, T.; Koschutnik, M.; Donà, C.; Dannenberg, V.; Hofer, F.; Halavina, K.; Kammerlander, A.A.; Traub-Weidinger, T.; et al. The Complexity of Subtle Cardiac Tracer Uptake on Bone Scintigraphy. JACC Cardiovasc. Imaging 2022, 15, 1516–1518. [Google Scholar] [CrossRef]
- Arshad, S.; Goldberg, Y.H.; Bhopalwala, H.; Dewaswala, N.; Miceli, N.S.; Birks, E.J.; Vaidya, G.N. High Prevalence of Cardiac Amyloidosis in Clinically Significant Aortic Stenosis: A Meta-Analysis. Cardiol. Res. 2022, 13, 357–371. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, C.; Mascherbauer, K.; Calabretta, R.; Koschutnik, M.; Dona, C.; Dannenberg, V.; Hofer, F.; Halavina, K.; Kammerlander, A.; Traub-Weidinger, T.; et al. Prevalence and outcomes of cardiac amyloidosis in all-comer referrals for bone scintigraphy. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2022, 63, 1906–1911. [Google Scholar] [CrossRef] [PubMed]
- Kristen, A.V.; Schnabel, P.A.; Winter, B.; Helmke, B.M.; Longerich, T.; Hardt, S.; Koch, A.; Sack, F.-U.; Katus, H.A.; Linke, R.P.; et al. High prevalence of amyloid in 150 surgically removed heart valves—A comparison of histological and clinical data reveals a correlation to atheroinflammatory conditions. Cardiovasc. Pathol. 2010, 19, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Singal, A.K.; Bansal, R.; Singh, A.; Dorbala, S.; Sharma, G.; Gupta, K.; Saxena, A.; Bhargava, B.; Karthikeyan, G.; Ramakrishnan, S.; et al. Concomitant Transthyretin Amyloidosis and Severe Aortic Stenosis in Elderly Indian Population: A Pilot Study. JACC CardioOncology 2021, 3, 565–576. [Google Scholar] [CrossRef] [PubMed]
- Marcoux, J.; Mangione, P.P.; Porcari, R.; Degiacomi, M.T.; Verona, G.; Taylor, G.W.; Giorgetti, S.; Raimondi, S.; Sanglier-Cianférani, S.; Benesch, J.L.; et al. A novel mechano-enzymatic cleavage mechanism underlies transthyretin amyloidogenesis. EMBO Mol. Med. 2015, 7, 1337–1349. [Google Scholar] [CrossRef] [PubMed]
- Treibel, T.A.; Lopez, B.; Gonzalez, A.; Menacho, K.; Schofield, R.S.; Ravassa, S.; Fontana, M.; White, S.K.; DiSalvo, C.; Roberts, N.; et al. Reappraising myocardial fibrosis in severe aortic stenosis: An invasive and non-invasive study in 133 patients. Eur. Heart J. 2018, 39, 699–709. [Google Scholar] [CrossRef] [PubMed]
- Jendroska, K.; Poewe, W.; Daniel, S.E.; Pluess, J.; Iwerssen-Schmidt, H.; Paulsen, J.; Barthel, S.; Schelosky, L.; Cervós-Navarro, J.; DeArmond, S.J. Ischemic stress induces deposition of amyloid beta immunoreactivity in human brain. Acta Neuropathol. 1995, 90, 461–466. [Google Scholar] [CrossRef]
- Patel, K.P.; Scully, P.R.; Nitsche, C.; Kammerlander, A.A.; Joy, G.; Thornton, G.; Hughes, R.; Williams, S.; Tillin, T.; Captur, G.; et al. Impact of afterload and infiltration on coexisting aortic stenosis and transthyretin amyloidosis. Heart 2022, 108, 67–72. [Google Scholar] [CrossRef]
- Arbelo, E.; Protonotarios, A.; Gimeno, J.R.; Arbustini, E.; Barriales-Villa, R.; Basso, C.; Bezzina, C.R.; Biagini, E.; Blom, N.A.; de Boer, R.A.; et al. 2023 ESC Guidelines for the management of cardiomyopathies. Eur. Heart J. 2023, 44, 3503–3626. [Google Scholar] [CrossRef]
- Cavalcante, J.L.; Rijal, S.; Abdelkarim, I.; Althouse, A.D.; Sharbaugh, M.S.; Fridman, Y.; Soman, P.; Forman, D.E.; Schindler, J.T.; Gleason, T.G.; et al. Cardiac amyloidosis is prevalent in older patients with aortic stenosis and carries worse prognosis. J. Cardiovasc. Magn. Reson. Off. J. Soc. Cardiovasc. Magn. Reson. 2017, 19, 98. [Google Scholar] [CrossRef]
- Scully, P.R.; Patel, K.P.; Saberwal, B.; Klotz, E.; Augusto, J.B.; Thornton, G.D.; Hughes, R.K.; Manisty, C.; Lloyd, G.; Newton, J.D.; et al. Identifying Cardiac Amyloid in Aortic Stenosis: ECV Quantification by CT in TAVR Patients. JACC Cardiovasc. Imaging 2020, 13, 2177–2189. [Google Scholar] [CrossRef] [PubMed]
- Ternacle, J.; Krapf, L.; Mohty, D.; Magne, J.; Nguyen, A.; Galat, A.; Gallet, R.; Teiger, E.; Côté, N.; Clavel, M.-A.; et al. Aortic Stenosis and Cardiac Amyloidosis: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 74, 2638–2651. [Google Scholar] [CrossRef] [PubMed]
- Rosenblum, H.; Masri, A.; Narotsky, D.L.; Goldsmith, J.; Hamid, N.; Hahn, R.T.; Kodali, S.; Vahl, T.; Nazif, T.; Khalique, O.K.; et al. Unveiling outcomes in coexisting severe aortic stenosis and transthyretin cardiac amyloidosis. Eur. J. Heart Fail. 2021, 23, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Maurer, M.S.; Schwartz, J.H.; Gundapaneni, B.; Elliott, P.M.; Merlini, G.; Waddington-Cruz, M.; Kristen, A.V.; Grogan, M.; Witteles, R.; Damy, T.; et al. Tafamidis Treatment for Patients with Transthyretin Amyloid Cardiomyopathy. N. Engl. J. Med. 2018, 379, 1007–1016. [Google Scholar] [CrossRef] [PubMed]
- Gillmore, J.D.; Garcia-Pavia, P.; Grogan, M.; Hanna, M.A.; Heitner, S.B.; Jacoby, D.; Maurer, M.S.; Rapezzi, C.; Shah, S.J.; Ganju, J.; et al. Abstract 14214: ATTRibute-CM: A Randomized, Double-Blind, Placebo-Controlled, Multi-Center, Global Phase 3 Study of AG10 in Patients With Transthyretin Amyloid Cardiomyopathy (ATTR-CM). Circulation 2019, 140, A14214. [Google Scholar] [CrossRef]
- Nitsche, C.; Koschutnik, M.; Donà, C.; Radun, R.; Mascherbauer, K.; Kammerlander, A.; Heitzinger, G.; Dannenberg, V.; Spinka, G.; Halavina, K.; et al. Reverse Remodeling Following Valve Replacement in Coexisting Aortic Stenosis and Transthyretin Cardiac Amyloidosis. Circ. Cardiovasc. Imaging 2022, 15, e014115. [Google Scholar] [CrossRef] [PubMed]
- Chioncel, O.; Lainscak, M.; Seferovic, P.M.; Anker, S.D.; Crespo-Leiro, M.G.; Harjola, V.-P.; Parissis, J.; Laroche, C.; Piepoli, M.F.; Fonseca, C.; et al. Epidemiology and one-year outcomes in patients with chronic heart failure and preserved, mid-range and reduced ejection fraction: An analysis of the ESC Heart Failure Long-Term Registry. Eur. J. Heart Fail. 2017, 19, 1574–1585. [Google Scholar] [CrossRef]
- Chacko, L.; Karia, N.; Venneri, L.; Bandera, F.; Passo, B.D.; Buonamici, L.; Lazari, J.; Ioannou, A.; Porcari, A.; Patel, R.; et al. Progression of echocardiographic parameters and prognosis in transthyretin cardiac amyloidosis. Eur. J. Heart Fail. 2022, 24, 1700–1712. [Google Scholar] [CrossRef]
- Chacko, L.; Martone, R.; Bandera, F.; Lane, T.; Martinez-Naharro, A.; Boldrini, M.; Rezk, T.; Whelan, C.; Quarta, C.; Rowczenio, D.; et al. Echocardiographic phenotype and prognosis in transthyretin cardiac amyloidosis. Eur. Heart J. 2020, 41, 1439–1447. [Google Scholar] [CrossRef]
- Binder, C.; Duca, F.; Stelzer, P.D.; Nitsche, C.; Rettl, R.; Aschauer, S.; Kammerlander, A.A.; Binder, T.; Agis, H.; Kain, R.; et al. Mechanisms of heart failure in transthyretin vs. light chain amyloidosis. Eur. Heart J.—Cardiovasc. Imaging 2019, 20, 512–524. [Google Scholar] [CrossRef]
- Fagot, J.; Lavie-Badie, Y.; Blanchard, V.; Fournier, P.; Galinier, M.; Carrié, D.; Lairez, O.; Cariou, E.; Toulouse Amyloidosis Research Network collaborators. Impact of tricuspid regurgitation on survival in patients with cardiac amyloidosis. ESC Heart Fail. 2021, 8, 438–446. [Google Scholar] [CrossRef]
- Donà, C.; Nitsche, C.; Koschutnik, M.; Heitzinger, G.; Mascherbauer, K.; Kammerlander, A.A.; Dannenberg, V.; Halavina, K.; Rettl, R.; Duca, F.; et al. Unveiling Cardiac Amyloidosis, its Characteristics, and Outcomes Among Patients With MR Undergoing Transcatheter Edge-to-Edge MV Repair. JACC. Cardiovasc. Interv. 2022, 15, 1748–1758. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.; Godoy Rivas, C.; Rodriguez, E.R.; Tan, C.; Gillinov, A.M.; Harb, S.; Jellis, C.; Griffin, B. Unrecognized Cardiac Amyloidosis at the Time of Mitral Valve Surgery: Incidence and Outcomes. Cardiology 2019, 142, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Masugata, H.; Mizushige, K.; Senda, S.; Kinoshita, A.; Nozaki, S.; Matsuo, H.; Kohno, M. Physical properties of the mitral valve tissue assessed by tissue sound speed in cardiac amyloidosis: Relationship to the severity of mitral regurgitation. Ultrasound Med. Biol. 2000, 26, 1191–1198. [Google Scholar] [CrossRef] [PubMed]
- Nishi, H.; Mitsuno, M.; Ryomoto, M.; Miyamoto, Y. Severe mitral regurgitation due to cardiac amyloidosis--a rare reason for ruptured chordae. Interact. Cardiovasc. Thorac. Surg. 2008, 7, 1199–1200. [Google Scholar] [CrossRef] [PubMed]
- Aimo, A.; Camerini, L.; Fabiani, I.; Morfino, P.; Panichella, G.; Barison, A.; Pucci, A.; Castiglione, V.; Vergaro, G.; Sinagra, G.; et al. Valvular heart disease in patients with cardiac amyloidosis. Heart Fail. Rev. 2023. [Google Scholar] [CrossRef] [PubMed]
- Nemes, A.; Földeák, D.; Kormányos, Á.; Domsik, P.; Kalapos, A.; Borbényi, Z.; Forster, T. Cardiac Amyloidosis Associated with Enlargement and Functional Impairment of the Mitral Annulus: Insights from the Three-Dimensional Speckle Tracking Echocardiographic MAGYAR-Path Study. J. Heart Valve Dis. 2017, 26, 304–308. [Google Scholar]
- El Sabbagh, A.; Reddy, Y.N.V.; Nishimura, R.A. Mitral Valve Regurgitation in the Contemporary Era: Insights Into Diagnosis, Management, and Future Directions. JACC Cardiovasc. Imaging 2018, 11, 628–643. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 43, 561–632. [Google Scholar] [CrossRef]
- Nitsche, C. Echocardiographic tracking of transthyretin cardiomyopathy: Which parameters matter the most? Eur. J. Heart Fail. 2022, 24, 1713–1715. [Google Scholar] [CrossRef]
- Volz, M.J.; Pleger, S.T.; Weber, A.; Geis, N.A.; Hamed, S.; Mereles, D.; Hegenbart, U.; Katus, H.A.; Frey, N.; Raake, P.W.; et al. Initial experience with percutaneous mitral valve repair in patients with cardiac amyloidosis. Eur. J. Clin. Investig. 2021, 51, e13473. [Google Scholar] [CrossRef] [PubMed]
- Benfari, G.; Antoine, C.; Miller, W.L.; Thapa, P.; Topilsky, Y.; Rossi, A.; Michelena, H.I.; Pislaru, S.; Enriquez-Sarano, M. Excess Mortality Associated With Functional Tricuspid Regurgitation Complicating Heart Failure With Reduced Ejection Fraction. Circulation 2019, 140, 196–206. [Google Scholar] [CrossRef] [PubMed]
- Cammalleri, V.; Antonelli, G.; De Luca, V.M.; Carpenito, M.; Nusca, A.; Bono, M.C.; Mega, S.; Ussia, G.P.; Grigioni, F. Functional Mitral and Tricuspid Regurgitation across the Whole Spectrum of Left Ventricular Ejection Fraction: Recognizing the Elephant in the Room of Heart Failure. J. Clin. Med. 2023, 12, 3316. [Google Scholar] [CrossRef] [PubMed]
- Kammerlander, A.A.; Marzluf, B.A.; Graf, A.; Bachmann, A.; Kocher, A.; Bonderman, D.; Mascherbauer, J. Right ventricular dysfunction, but not tricuspid regurgitation, is associated with outcome late after left heart valve procedure. J. Am. Coll. Cardiol. 2014, 64, 2633–2642. [Google Scholar] [CrossRef] [PubMed]
- Topilsky, Y.; Maltais, S.; Medina Inojosa, J.; Oguz, D.; Michelena, H.; Maalouf, J.; Mahoney, D.W.; Enriquez-Sarano, M. Burden of Tricuspid Regurgitation in Patients Diagnosed in the Community Setting. JACC Cardiovasc. Imaging 2019, 12, 433–442. [Google Scholar] [CrossRef]
- Hoerbrand, I.A.; Volz, M.J.; Aus dem Siepen, F.; Aurich, M.; Schlegel, P.; Geis, N.A.; Hegenbart, U.; Konstandin, M.H.; Frey, N.; Raake, P.W. Initial experience with transcatheter tricuspid valve repair in patients with cardiac amyloidosis. ESC Heart Fail. 2023, 10, 1003–1012. [Google Scholar] [CrossRef]
- Randhawa, V.K.; Vakamudi, S.; Phelan, D.M.; Samaras, C.J.; McKenney, J.K.; Hanna, M.; Perez, A.L. Mitral and tricuspid stenosis caused by light chain cardiac amyloid deposition. ESC Heart Fail. 2020, 7, 1130–1135. [Google Scholar] [CrossRef]
- Frumkin, D.; Taube, E.T.; Stangl, K.; Knebel, F. Rapid progression of aortic and mitral stenosis in a patient with AA amyloidosis: A case report. Eur. Heart J.—Case Rep. 2019, 3, ytz051. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duca, F.; Kronberger, C.; Willixhofer, R.; Bartko, P.E.; Bergler-Klein, J.; Nitsche, C. Cardiac Amyloidosis and Valvular Heart Disease. J. Clin. Med. 2024, 13, 221. https://doi.org/10.3390/jcm13010221
Duca F, Kronberger C, Willixhofer R, Bartko PE, Bergler-Klein J, Nitsche C. Cardiac Amyloidosis and Valvular Heart Disease. Journal of Clinical Medicine. 2024; 13(1):221. https://doi.org/10.3390/jcm13010221
Chicago/Turabian StyleDuca, Franz, Christina Kronberger, Robin Willixhofer, Philipp E. Bartko, Jutta Bergler-Klein, and Christian Nitsche. 2024. "Cardiac Amyloidosis and Valvular Heart Disease" Journal of Clinical Medicine 13, no. 1: 221. https://doi.org/10.3390/jcm13010221