

Does Elderly-Onset Inflammatory Bowel Disease Increase Risk of Colorectal Cancer? A Systematic Review and Meta-Analysis
Abstract
:1. Introduction
2. Materials and Methods
2.1. Information Sources and Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection and Data Extraction
2.4. Risk of Bias Assessment
2.5. Study Outcome and Statistical Analysis
3. Results
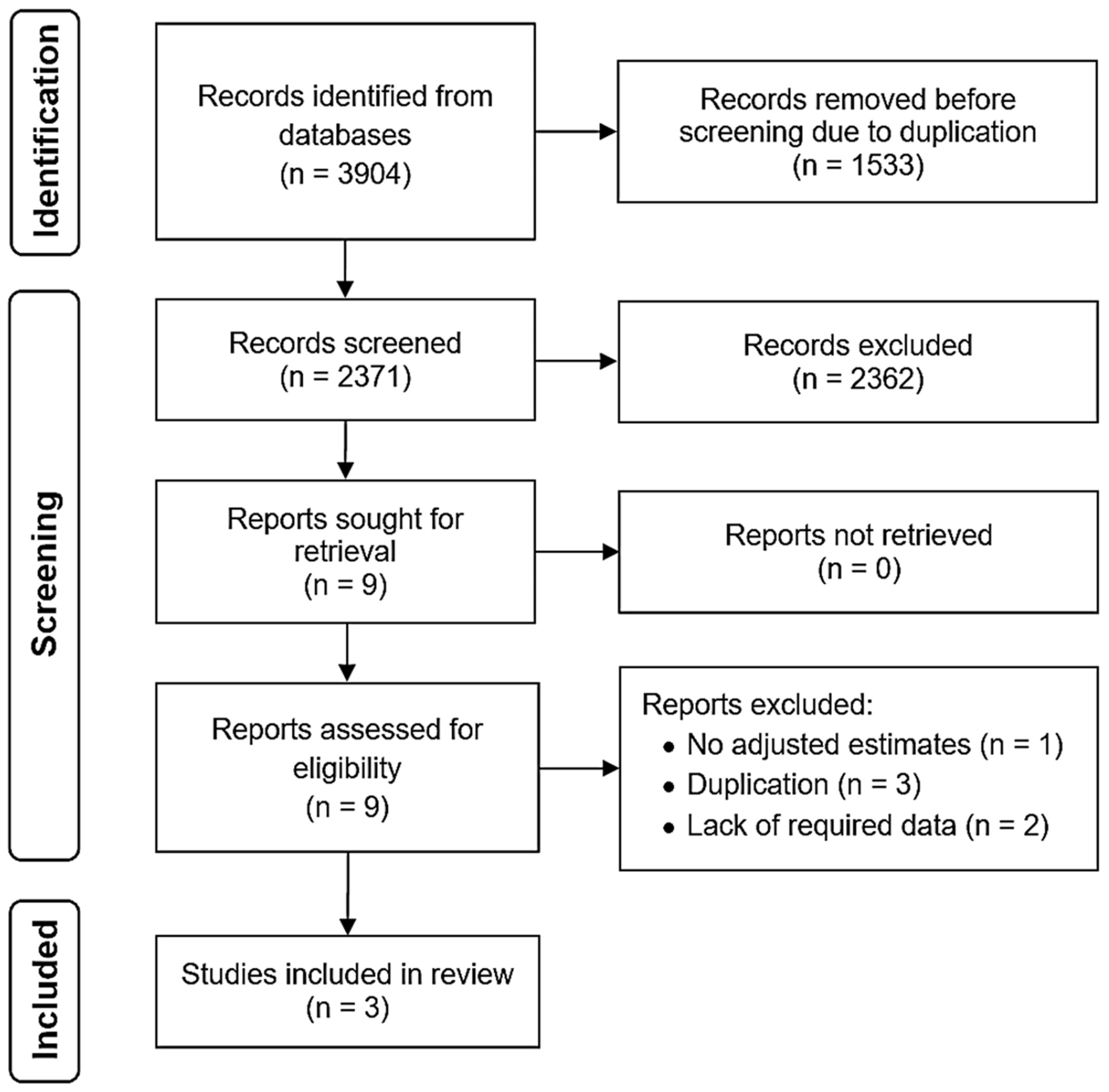
3.1. Search Results, Study Selection, and Characteristics
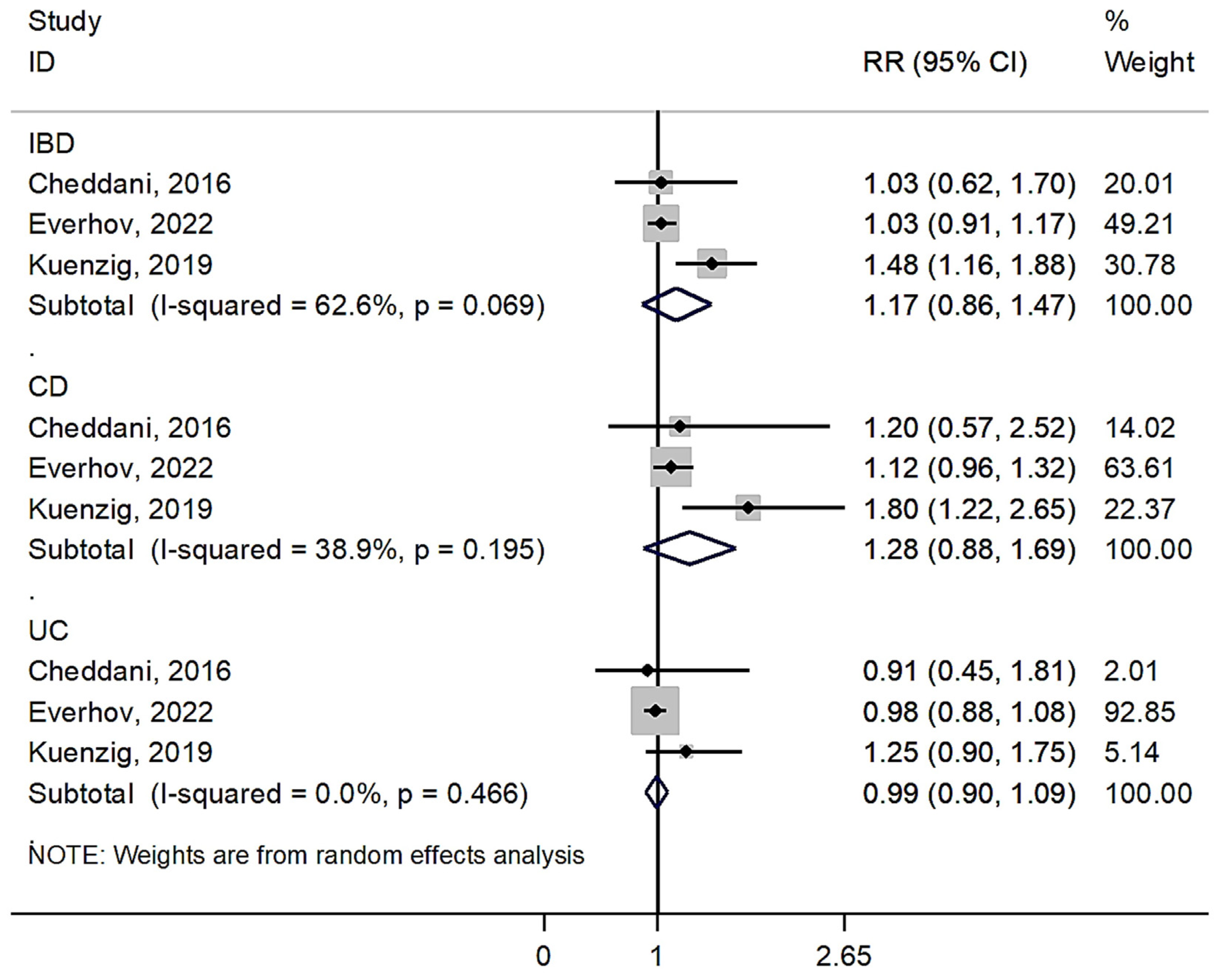
3.2. Overall Risk of Colorectal Cancer
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zamani, M.; Alizadeh-Tabari, S.; Singh, S.; Loomba, R. Meta-analysis: Prevalence of, and risk factors for, non-alcoholic fatty liver disease in patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2022, 55, 894–907. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.C.; Shi, H.Y.; Hamidi, N.; Underwood, F.E.; Tang, W.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Wu, J.C.Y.; Chan, F.K.L.; et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. Lancet 2017, 390, 2769–2778. [Google Scholar] [CrossRef] [PubMed]
- Goethel, A.; Croitoru, K.; Philpott, D.J. The interplay between microbes and the immune response in inflammatory bowel disease. J. Physiol. 2018, 596, 3869–3882. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Burisch, J. Impact of Genes and the Environment on the Pathogenesis and Disease Course of Inflammatory Bowel Disease. Dig. Dis. Sci. 2019, 64, 1759–1769. [Google Scholar] [CrossRef]
- Saez, A.; Herrero-Fernandez, B.; Gomez-Bris, R.; Sánchez-Martinez, H.; Gonzalez-Granado, J.M. Pathophysiology of Inflammatory Bowel Disease: Innate Immune System. Int. J. Mol. Sci. 2023, 24, 1526. [Google Scholar] [CrossRef]
- Seyedian, S.S.; Nokhostin, F.; Malamir, M.D. A review of the diagnosis, prevention, and treatment methods of inflammatory bowel disease. J. Med. Life 2019, 12, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Rogler, G.; Singh, A.; Kavanaugh, A.; Rubin, D.T. Extraintestinal Manifestations of Inflammatory Bowel Disease: Current Concepts, Treatment, and Implications for Disease Management. Gastroenterology 2021, 161, 1118–1132. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.H.; Gweon, T.G.; Kang, S.G.; Jung, S.H.; Lee, K.M.; Kang, S.B. Assessment of Fatigue and Associated Factors in Patients with Inflammatory Bowel Disease: A Questionnaire-Based Study. J. Clin. Med. 2023, 12, 3116. [Google Scholar] [CrossRef]
- Wan, Q.; Zhao, R.; Xia, L.; Wu, Y.; Zhou, Y.; Wang, Y.; Cui, Y.; Shen, X.; Wu, X.T. Inflammatory bowel disease and risk of gastric, small bowel and colorectal cancer: A meta-analysis of 26 observational studies. J. Cancer Res. Clin. Oncol. 2021, 147, 1077–1087. [Google Scholar] [CrossRef]
- Nadeem, M.S.; Kumar, V.; Al-Abbasi, F.A.; Kamal, M.A.; Anwar, F. Risk of colorectal cancer in inflammatory bowel diseases. Semin. Cancer Biol. 2020, 64, 51–60. [Google Scholar] [CrossRef]
- Kamp, K.; Dudley-Brown, S.; Heitkemper, M.; Wyatt, G.; Given, B. Symptoms among emerging adults with inflammatory bowel disease: A descriptive study. Res. Nurs. Health 2020, 43, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Rozich, J.J.; Dulai, P.S.; Fumery, M.; Sandborn, W.J.; Singh, S. Progression of Elderly Onset Inflammatory Bowel Diseases: A Systematic Review and Meta-Analysis of Population-Based Cohort Studies. Clin. Gastroenterol. Hepatol. 2020, 18, 2437–2447.e6. [Google Scholar] [CrossRef] [PubMed]
- Duricova, D.; Burisch, J.; Jess, T.; Gower-Rousseau, C.; Lakatos, P.L. Age-related differences in presentation and course of inflammatory bowel disease: An update on the population-based literature. J. Crohns Colitis 2014, 8, 1351–1361. [Google Scholar] [CrossRef] [PubMed]
- Lutgens, M.W.; van Oijen, M.G.; van der Heijden, G.J.; Vleggaar, F.P.; Siersema, P.D.; Oldenburg, B. Declining risk of colorectal cancer in inflammatory bowel disease: An updated meta-analysis of population-based cohort studies. Inflamm. Bowel Dis. 2013, 19, 789–799. [Google Scholar] [CrossRef] [PubMed]
- Faye, A.S.; Colombel, J.F. Aging and IBD: A New Challenge for Clinicians and Researchers. Inflamm. Bowel Dis. 2022, 28, 126–132. [Google Scholar] [CrossRef]
- Arnott, I.; Rogler, G.; Halfvarson, J. The Management of Inflammatory Bowel Disease in Elderly: Current Evidence and Future Perspectives. Inflamm. Intest. Dis. 2018, 2, 189–199. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- Narula, N.; Chang, N.H.; Mohammad, D.; Wong, E.C.L.; Ananthakrishnan, A.N.; Chan, S.S.M.; Carbonnel, F.; Meyer, A. Food Processing and Risk of Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2023, 21, 2483–2495.e1. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Richardson, M.; Garner, P.; Donegan, S. Interpretation of subgroup analyses in systematic reviews: A tutorial. Clin. Epidemiol. Glob. Health 2019, 7, 192–198. [Google Scholar] [CrossRef]
- Cheddani, H.; Dauchet, L.; Fumery, M.; Charpentier, C.; Marie Bouvier, A.; Dupas, J.L.; Pariente, B.; Peyrin-Biroulet, L.; Savoye, G.; Gower-Rousseau, C. Cancer in Elderly Onset Inflammatory Bowel Disease: A Population-Based Study. Am. J. Gastroenterol. 2016, 111, 1428–1436. [Google Scholar] [CrossRef] [PubMed]
- Everhov, Å.H.; Erichsen, R.; Järås, J.; Pedersen, L.; Halfvarson, J.; Askling, J.; Ekbom, A.; Ludvigsson, J.F.; Sørensen, H.T.; Olén, O. Colorectal cancer in elderly-onset inflammatory bowel disease: A 1969–2017 Scandinavian register-based cohort study. Aliment. Pharmacol. Ther. 2022, 56, 1168–1182. [Google Scholar] [CrossRef] [PubMed]
- Kuenzig, E.; Murthy, S.K.; Stukel, T.A.; Nguyen, G.C.; Kaplan, G.; Talarico, R.; Benchimol, E.I. 207—Increased Incidence of Malignancy in Patients with Elderly-Onset Inflammatory Bowel Disease: A Population-Based Matched Cohort Study. Gastroenterology 2019, 156, S43. [Google Scholar] [CrossRef]
- Ananthakrishnan, A.N.; Nguyen, G.C.; Bernstein, C.N. AGA Clinical Practice Update on Management of Inflammatory Bowel Disease in Elderly Patients: Expert Review. Gastroenterology 2021, 160, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Gisbert, J.P.; Chaparro, M. Systematic review with meta-analysis: Inflammatory bowel disease in the elderly. Aliment. Pharmacol. Ther. 2014, 39, 459–477. [Google Scholar] [CrossRef] [PubMed]
- Olén, O.; Erichsen, R.; Sachs, M.C.; Pedersen, L.; Halfvarson, J.; Askling, J.; Ekbom, A.; Sørensen, H.T.; Ludvigsson, J.F. Colorectal cancer in Crohn’s disease: A Scandinavian population-based cohort study. Lancet Gastroenterol. Hepatol. 2020, 5, 475–484. [Google Scholar] [CrossRef]
- Olén, O.; Erichsen, R.; Sachs, M.C.; Pedersen, L.; Halfvarson, J.; Askling, J.; Ekbom, A.; Sørensen, H.T.; Ludvigsson, J.F. Colorectal cancer in ulcerative colitis: A Scandinavian population-based cohort study. Lancet 2020, 395, 123–131. [Google Scholar] [CrossRef]
- Wetwittayakhlang, P.; Tselekouni, P.; Al-Jabri, R.; Bessissow, T.; Lakatos, P.L. The Optimal Management of Inflammatory Bowel Disease in Patients with Cancer. J. Clin. Med. 2023, 12, 2432. [Google Scholar] [CrossRef]
- Singh, S.; Boland, B.S.; Jess, T.; Moore, A.A. Management of inflammatory bowel diseases in older adults. Lancet Gastroenterol. Hepatol. 2023, 8, 368–382. [Google Scholar] [CrossRef]
- Lucafò, M.; Curci, D.; Franzin, M.; Decorti, G.; Stocco, G. Inflammatory Bowel Disease and Risk of Colorectal Cancer: An Overview From Pathophysiology to Pharmacological Prevention. Front. Pharmacol. 2021, 12, 772101. [Google Scholar] [CrossRef] [PubMed]
- Foster, A.D.; Sivarapatna, A.; Gress, R.E. The aging immune system and its relationship with cancer. Aging Health 2011, 7, 707–718. [Google Scholar] [CrossRef] [PubMed]
- Lian, J.; Yue, Y.; Yu, W.; Zhang, Y. Immunosenescence: A key player in cancer development. J. Hematol. Oncol. 2020, 13, 151. [Google Scholar] [CrossRef] [PubMed]
- Murphy, N.; Moreno, V.; Hughes, D.J.; Vodicka, L.; Vodicka, P.; Aglago, E.K.; Gunter, M.J.; Jenab, M. Lifestyle and dietary environmental factors in colorectal cancer susceptibility. Mol. Asp. Med. 2019, 69, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Kleykamp, B.A.; Heishman, S.J. The older smoker. JAMA 2011, 306, 876–877. [Google Scholar] [CrossRef] [PubMed]
- Govindaraju, T.; Sahle, B.W.; McCaffrey, T.A.; McNeil, J.J.; Owen, A.J. Dietary Patterns and Quality of Life in Older Adults: A Systematic Review. Nutrients 2018, 10, 971. [Google Scholar] [CrossRef]
- Dekker, E.; Rex, D.K. Advances in CRC Prevention: Screening and Surveillance. Gastroenterology 2018, 154, 1970–1984. [Google Scholar] [CrossRef]
- Nimmons, D.; Limdi, J.K. Elderly patients and inflammatory bowel disease. World J. Gastrointest. Pharmacol. Ther. 2016, 7, 51–65. [Google Scholar] [CrossRef]
- Branco, B.C.; Harpaz, N.; Sachar, D.B.; Greenstein, A.J.; Tabrizian, P.; Bauer, J.J.; Greenstein, A.J. Colorectal carcinoma in indeterminate colitis. Inflamm. Bowel Dis. 2009, 15, 1076–1081. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Country | Study Period | Study Design | Patients with Inflammatory Bowel Disease | Adjustment for | ||||
|---|---|---|---|---|---|---|---|---|---|
| Total Patients (n) | Men (%) | Median Age (Years) | Median Follow-Up (Years) | CRC Events (n) | |||||
| Cheddani, 2016 | France | 1990–2006 | Multi-center | IBD = 844 CD = 370 UC = 474 | 51.5 | 70 | 6 | 15 | Sex and age |
| Everhov, 2022 | Sweden and Denmark | 1969–2017 | Multi-center | IBD = 29,093 CD = 7869 UC = 21,224 | 47.4 | 69 | 6 | 569 | Sex, age at IBD diagnosis, birth year, country |
| Kuenzig, 2019 | Canada | 2002–2013 | Single-center | IBD = 5250 CD = 1683 UC = 3195 | NA | NA | 5 | 110 | Sex and age |
| Study | Selection (Out of 4) | Comparability (Out of 2) | Outcome (Out of 3) | Total (Out of 9) |
|---|---|---|---|---|
| Cheddani, 2016 | 4 | 1 | 3 | 8 |
| Everhov, 2022 | 4 | 1 | 3 | 8 |
| Kuenzig, 2019 | 3 | 1 | 3 | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zamani, M.; Alizadeh-Tabari, S. Does Elderly-Onset Inflammatory Bowel Disease Increase Risk of Colorectal Cancer? A Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 148. https://doi.org/10.3390/jcm13010148
Zamani M, Alizadeh-Tabari S. Does Elderly-Onset Inflammatory Bowel Disease Increase Risk of Colorectal Cancer? A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024; 13(1):148. https://doi.org/10.3390/jcm13010148
Chicago/Turabian StyleZamani, Mohammad, and Shaghayegh Alizadeh-Tabari. 2024. "Does Elderly-Onset Inflammatory Bowel Disease Increase Risk of Colorectal Cancer? A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 13, no. 1: 148. https://doi.org/10.3390/jcm13010148