
Effects of Immersive Virtual Reality on Upper-Extremity Stroke Rehabilitation: A Systematic Review with Meta-Analysis
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Protocol Registration
2.2. Search Strategy and Study Selection
2.3. Eligibility Criteria
2.4. Risk-of-Bias Assessment
2.5. Results Analysis
2.6. Grade and Quality of Evidence
3. Results
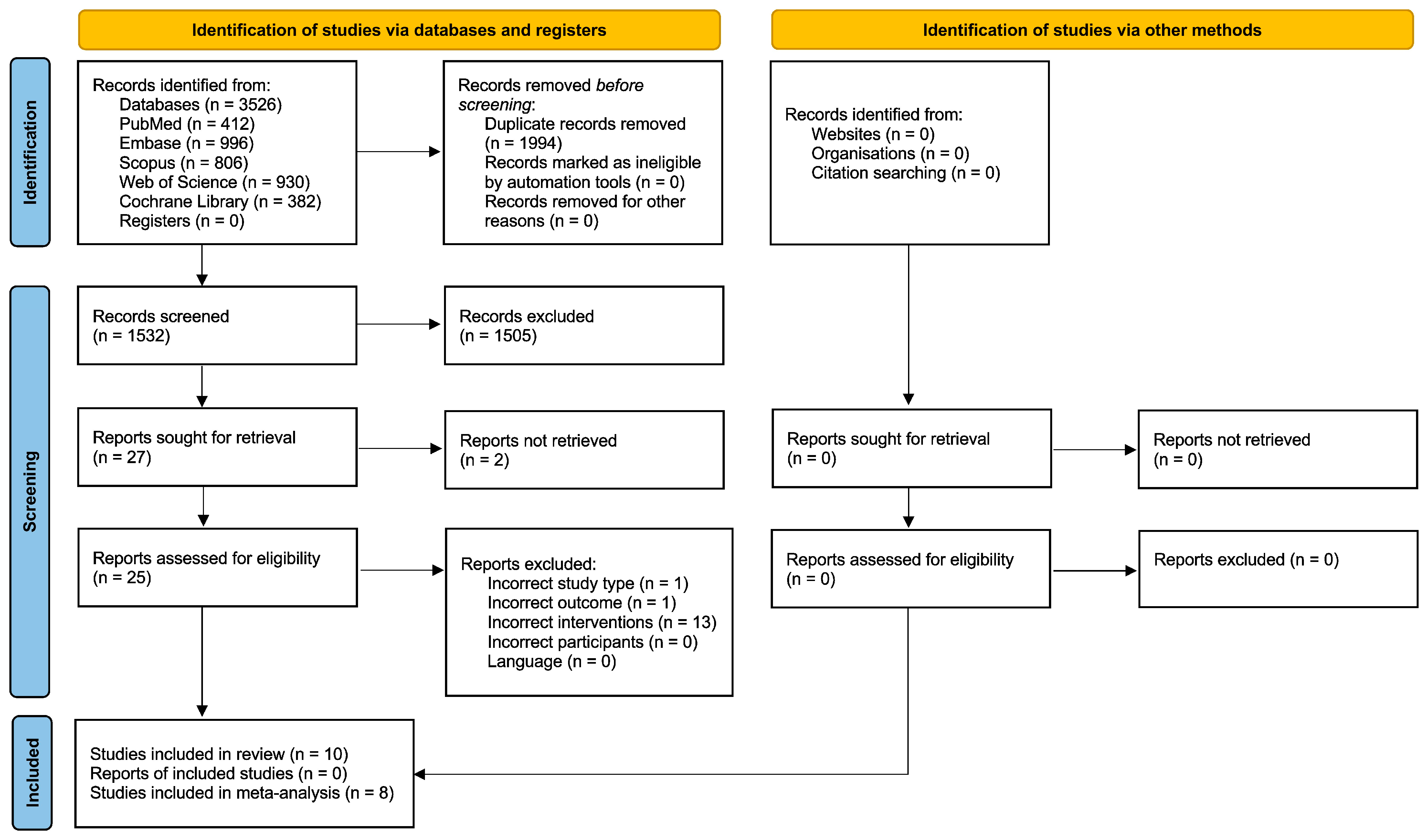
3.1. Study Selection
3.2. Study Characteristics and Results Summary
3.3. Meta-Analysis Results
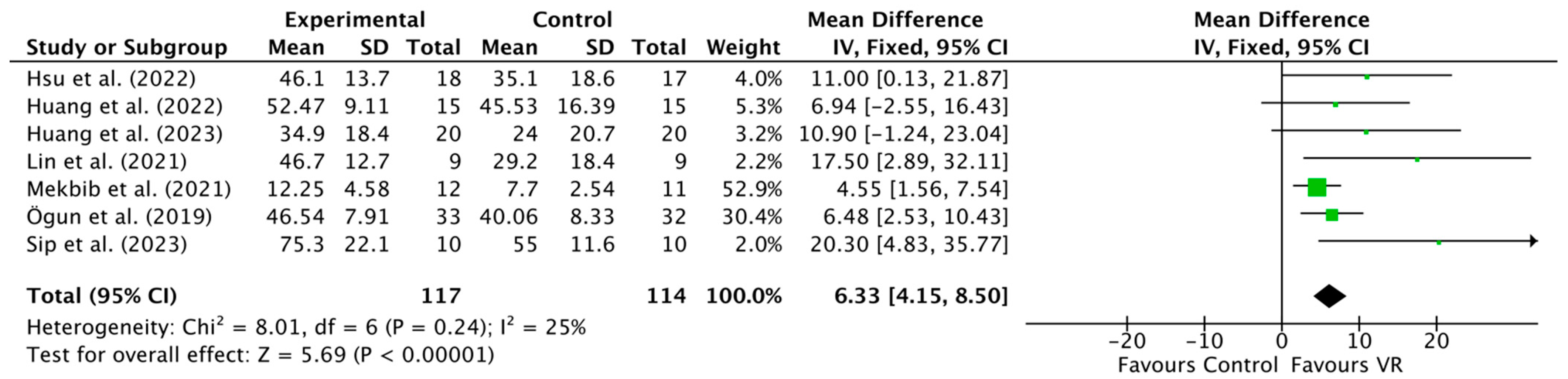
3.3.1. Function Assessed by the Fugl-Meyer Assessment for Upper Extremity
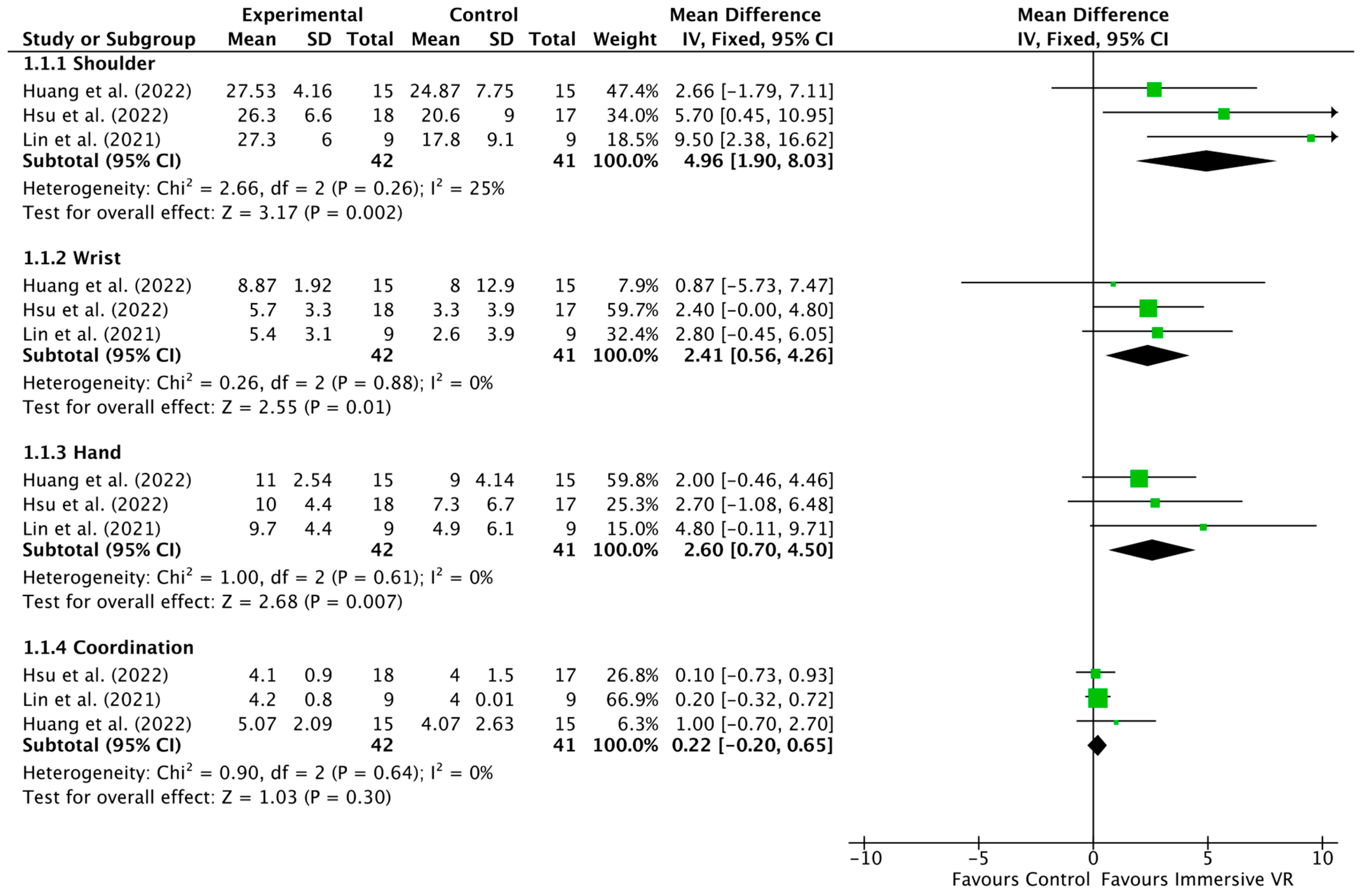
3.3.2. Upper-Extremity Analysis
3.3.3. Activities-of-Daily-Living Analysis
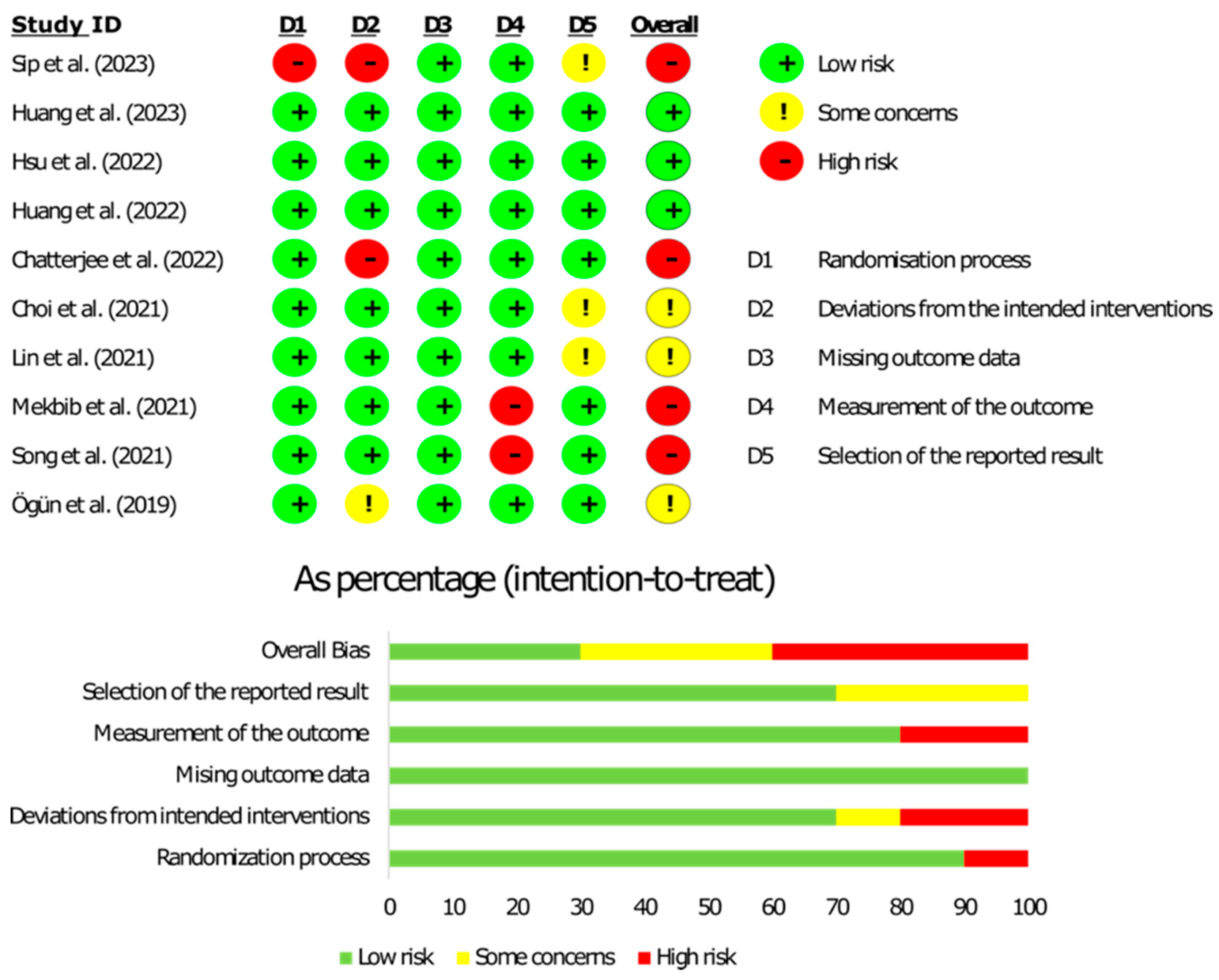
3.4. Risk-of-Bias Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feigin, V.L.; Forouzanfar, M.H.; Krishnamurthi, R.; Mensah, G.A.; Connor, M.; Bennett, D.A.; Moran, A.E.; Sacco, R.L.; Anderson, L.; Truelsen, T.; et al. Global and Regional Burden of Stroke during 1990-2010: Findings from the Global Burden of Disease Study 2010. Lancet 2014, 383, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Teasell, R.W.; Murie Fernandez, M.; McIntyre, A.; Mehta, S. Rethinking the Continuum of Stroke Rehabilitation. Arch. Phys. Med. Rehabil. 2014, 95, 595–596. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.L.; Murray, L.; Richards, L.; Zorowitz, R.D.; Bakas, T.; Clark, P.; Billinger, S.A.; American Heart Association Council on Cardiovascular Nursing and the Stroke Council. Comprehensive Overview of Nursing and Interdisciplinary Rehabilitation Care of the Stroke Patient: A Scientific Statement from the American Heart Association. Stroke 2010, 41, 2402–2448. [Google Scholar] [CrossRef]
- Veerbeek, J.M.; van Wegen, E.; van Peppen, R.; van der Wees, P.J.; Hendriks, E.; Rietberg, M.; Kwakkel, G. What Is the Evidence for Physical Therapy Poststroke? A Systematic Review and Meta-Analysis. PLoS ONE 2014, 9, e87987. [Google Scholar] [CrossRef] [PubMed]
- French, B.; Thomas, L.H.; Coupe, J.; McMahon, N.E.; Connell, L.; Harrison, J.; Sutton, C.J.; Tishkovskaya, S.; Watkins, C.L. Repetitive Task Training for Improving Functional Ability after Stroke. Cochrane Database Syst. Rev. 2016, 11, CD006073. [Google Scholar] [CrossRef] [PubMed]
- Cieślik, B.; Mazurek, J.; Wrzeciono, A.; Maistrello, L.; Szczepańska-Gieracha, J.; Conte, P.; Kiper, P. Examining Technology-Assisted Rehabilitation for Older Adults’ Functional Mobility: A Network Meta-Analysis on Efficacy and Acceptability. NPJ Digit. Med. 2023, 6, 159. [Google Scholar] [CrossRef] [PubMed]
- Riva, G.; Gaggioli, A. Rehabilitation as Empowerment: The Role of Advanced Technologies. Stud. Health Technol. Inf. 2009, 145, 3–22. [Google Scholar]
- Ain, Q.U.; Khan, S.; Ilyas, S.; Yaseen, A.; Tariq, I.; Liu, T.; Wang, J. Additional Effects of Xbox Kinect Training on Upper Limb Function in Chronic Stroke Patients: A Randomized Control Trial. Healthcare 2021, 9, 242. [Google Scholar] [CrossRef]
- Leong, S.C.; Tang, Y.M.; Toh, F.M.; Fong, K.N.K. Examining the Effectiveness of Virtual, Augmented, and Mixed Reality (VAMR) Therapy for Upper Limb Recovery and Activities of Daily Living in Stroke Patients: A Systematic Review and Meta-Analysis. J. Neuroeng. Rehabil. 2022, 19, 93. [Google Scholar] [CrossRef]
- Garay-Sánchez, A.; Suarez-Serrano, C.; Ferrando-Margelí, M.; Jimenez-Rejano, J.J.; Marcén-Román, Y. Effects of Immersive and Non-Immersive Virtual Reality on the Static and Dynamic Balance of Stroke Patients: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 4473. [Google Scholar] [CrossRef]
- Lohre, R.; Warner, J.J.P.; Athwal, G.S.; Goel, D.P. The Evolution of Virtual Reality in Shoulder and Elbow Surgery. JSES Int. 2020, 4, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Ögün, M.N.; Kurul, R.; Yaşar, M.F.; Turkoglu, S.A.; Avci, Ş.; Yildiz, N. Effect of Leap Motion-Based 3D Immersive Virtual Reality Usage on Upper Extremity Function in Ischemic Stroke Patients. Arq. Neuropsiquiatr. 2019, 77, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Patsaki, I.; Dimitriadi, N.; Despoti, A.; Tzoumi, D.; Leventakis, N.; Roussou, G.; Papathanasiou, A.; Nanas, S.; Karatzanos, E. The Effectiveness of Immersive Virtual Reality in Physical Recovery of Stroke Patients: A Systematic Review. Front. Syst. Neurosci. 2022, 16, 880447. [Google Scholar] [CrossRef] [PubMed]
- Demain, S.; Burridge, J.; Ellis-Hill, C.; Hughes, A.-M.; Yardley, L.; Tedesco-Triccas, L.; Swain, I. Assistive Technologies after Stroke: Self-Management or Fending for Yourself? A Focus Group Study. BMC Health Serv. Res. 2013, 13, 334. [Google Scholar] [CrossRef] [PubMed]
- Levin, M.F.; Demers, M. Motor Learning in Neurological Rehabilitation. Disabil. Rehabil. 2021, 43, 3445–3453. [Google Scholar] [CrossRef] [PubMed]
- Bohil, C.J.; Alicea, B.; Biocca, F.A. Virtual Reality in Neuroscience Research and Therapy. Nat. Rev. Neurosci. 2011, 12, 752–762. [Google Scholar] [CrossRef] [PubMed]
- Demeco, A.; Zola, L.; Frizziero, A.; Martini, C.; Palumbo, A.; Foresti, R.; Buccino, G.; Costantino, C. Immersive Virtual Reality in Post-Stroke Rehabilitation: A Systematic Review. Sensors 2023, 23, 1712. [Google Scholar] [CrossRef]
- Berard, C.; Cavalier, M.; Godart, N. Use of Virtual Reality-Based Therapy in the Field of Chronic Stroke Rehabilitation to Improve Hand Function: A Systematic Review. Sport. Tour. Cent. Eur. J. 2022, 5, 115–138. [Google Scholar] [CrossRef]
- Chen, J.; Or, C.K.; Chen, T. Effectiveness of Using Virtual Reality-Supported Exercise Therapy for Upper Extremity Motor Rehabilitation in Patients With Stroke: Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Med. Internet Res. 2022, 24, e24111. [Google Scholar] [CrossRef]
- Luu, W.; Zangerl, B.; Kalloniatis, M.; Kim, J. Effects of Stereopsis on Vection, Presence and Cybersickness in Head-Mounted Display (HMD) Virtual Reality. Sci. Rep. 2021, 11, 12373. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J.; GRADE Working Group. GRADE: An Emerging Consensus on Rating Quality of Evidence and Strength of Recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, K.; Buchanan, A.; Cottrell, K.; Hughes, S.; Day, T.W.; John, N.W. Immersive Virtual Reality for the Cognitive Rehabilitation of Stroke Survivors. IEEE Trans. Neural Syst. Rehabil. Eng. 2022, 30, 719–728. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.-S.; Shin, W.-S.; Bang, D.-H. Application of Digital Practice to Improve Head Movement, Visual Perception and Activities of Daily Living for Subacute Stroke Patients with Unilateral Spatial Neglect: Preliminary Results of a Single-Blinded, Randomized Controlled Trial. Medicine 2021, 100, e24637. [Google Scholar] [CrossRef] [PubMed]
- Hsu, H.-Y.; Kuo, L.-C.; Lin, Y.-C.; Su, F.-C.; Yang, T.-H.; Lin, C.-W. Effects of a Virtual Reality–Based Mirror Therapy Program on Improving Sensorimotor Function of Hands in Chronic Stroke Patients: A Randomized Controlled Trial. Neurorehabilit. Neural Repair 2022, 36, 335–345. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.Y.; Chiang, W.C.; Yeh, Y.C.; Fan, S.C.; Yang, W.H.; Kuo, H.C.; Li, P.C. Effects of Virtual Reality-Based Motor Control Training on Inflammation, Oxidative Stress, Neuroplasticity and Upper Limb Motor Function in Patients with Chronic Stroke: A Randomized Controlled Trial. BMC Neurol. 2022, 22, 21. [Google Scholar] [CrossRef]
- Lin, C.-W.; Kuo, L.-C.; Lin, Y.-C.; Su, F.-C.; Lin, Y.-A.; Hsu, H.-Y. Development and Testing of a Virtual Reality Mirror Therapy System for the Sensorimotor Performance of Upper Extremity: A Pilot Randomized Controlled Trial. IEEE Access 2021, 9, 14725–14734. [Google Scholar] [CrossRef]
- Mekbib, D.B.; Debeli, D.K.; Zhang, L.; Fang, S.; Shao, Y.; Yang, W.; Han, J.; Jiang, H.; Zhu, J.; Zhao, Z.; et al. A Novel Fully Immersive Virtual Reality Environment for Upper Extremity Rehabilitation in Patients with Stroke. Ann. N. Y. Acad. Sci. 2021, 1493, 75–89. [Google Scholar] [CrossRef]
- Song, Y.-H.; Lee, H.-M. Effect of Immersive Virtual Reality-Based Bilateral Arm Training in Patients with Chronic Stroke. Brain Sci. 2021, 11, 1032. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.; Jiang, X.; Jin, Y.; Wu, B.; Vigotsky, A.D.; Fan, L.; Gu, P.; Tu, W.; Huang, L.; Jiang, S. Immersive Virtual Reality-Based Rehabilitation for Subacute Stroke: A Randomized Controlled Trial. J. Neurol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Sip, P.; Kozłowska, M.; Czysz, D.; Daroszewski, P.; Lisiński, P. Perspectives of Motor Functional Upper Extremity Recovery with the Use of Immersive Virtual Reality in Stroke Patients. Sensors 2023, 23, 712. [Google Scholar] [CrossRef] [PubMed]
- Kwah, L.K.; Harvey, L.A.; Diong, J.; Herbert, R.D. Models Containing Age and NIHSS Predict Recovery of Ambulation and Upper Limb Function Six Months after Stroke: An Observational Study. J. Physiother. 2013, 59, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.-F.; Wang, R.H.; Zariffa, J. Recognizing Hand Use and Hand Role at Home after Stroke from Egocentric Video. PLoS Digit. Health 2023, 2, e0000361. [Google Scholar] [CrossRef]
- Fercho, K.A.; Scholl, J.L.; Kc, B.; Bosch, T.J.; Baugh, L.A. Sensorimotor Control of Object Manipulation Following Middle Cerebral Artery (MCA) Stroke. Neuropsychologia 2023, 182, 108525. [Google Scholar] [CrossRef] [PubMed]
- Mollà-Casanova, S.; Llorens, R.; Borrego, A.; Salinas-Martínez, B.; Serra-Añó, P. Validity, Reliability, and Sensitivity to Motor Impairment Severity of a Multi-Touch App Designed to Assess Hand Mobility, Coordination, and Function after Stroke. J. Neuroeng. Rehabil. 2021, 18, 70. [Google Scholar] [CrossRef]
- Bhardwaj, D.; Sureka, D.; Meena, S.; Jain, N. Role of Occupational Therapy in Restoring Fine Motor Skills in Post Stroke Patients-An Analytical Review. EPRA Int. J. Multidiscip. Res. 2021, 7, 22–31. [Google Scholar] [CrossRef]
- Laver, K.E.; Lange, B.; George, S.; Deutsch, J.E.; Saposnik, G.; Crotty, M. Virtual Reality for Stroke Rehabilitation. Cochrane Database Syst. Rev. 2017, 11, CD008349. [Google Scholar] [CrossRef]
- Hao, J.; He, Z.; Yu, X.; Remis, A. Comparison of Immersive and Non-Immersive Virtual Reality for Upper Extremity Functional Recovery in Patients with Stroke: A Systematic Review and Network Meta-Analysis. Neurol. Sci. 2023, 44, 2679–2697. [Google Scholar] [CrossRef]
- Jin, M.; Pei, J.; Bai, Z.; Zhang, J.; He, T.; Xu, X.; Zhu, F.; Yu, D.; Zhang, Z. Effects of Virtual Reality in Improving Upper Extremity Function after Stroke: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Clin. Rehabil. 2022, 36, 573–596. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Certainty Assessment | n of Patients | Effect | Certainty | Importance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n of Studies | Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | iVR | CR | Relative (95% CI) | Absolute (95% CI) | ||
| Upper-limb function improvement (assessed with FMA-UE; scale from 0 to 66) | ||||||||||||
| 7 | RCTs | Serious a | Not serious | Not serious | Serious b | None | 117 | 114 | - | MD 6.33 effect higher (4.15 higher to 8.5 higher) | ⨁⨁◯◯ Low | Important |
| Study ID | Author (Year) | Study Design | Aim | Group Characteristics | Interventions | Outcome Measures | Timepoints | Conclusions |
|---|---|---|---|---|---|---|---|---|
| 1 | Huang et al. (2023) [32] | RCT | To assess the extent to which imVR-based UE rehabilitation could enhance conventional treatment. Additionally, the study aimed to investigate changes in brain functional connectivity associated with the rehabilitation process. | Subjects aged 30 to 85 years old, first stroke event within 1 month prior to enrollment, subacute stage with a subcortical lesion (basal ganglia, internal capsule, corona radiata, or brainstem), starting UL function of Brunnstrom stages II–IV. Exclusion criteria: History of transient ischemic attack, failure of critical organs, previous brain neurosurgery or epilepsy, severe cognitive impairments, or aphasia; subjects not suitable for an MRI scan or enrolled in another clinical trial involving PT or an investigational drug. EG = imVR, age 63.3 (14.3), 13 M, 7 F; CG = conventional rehabilitation, age 65.1 (6.1), 11 M, 9 F. | Both groups received rehabilitation training 5 days/wk for 3 wks. EG = 30′ of conventional rehabilitation + 30′ imVR system rehabilitation (environments: frying dumplings and noodles, popping balloons with a virtual sword, punching dolls in a virtual boxing arena, playing basketball in a virtual court, collecting eggs into a virtual basket, and tidying up a desk in a virtual office). The VR system comprised HMD—HTC Vive-VR; wireless controllers; 2 base stations using steamVR® technology; and computer. CG = 60′ conventional rehabilitation program daily. Design aimed for similar intensity and complexity to the immersive VR group. Program included PT and OT, covering grips, selective finger movements, gross movement, strength training, stretching, and ADLs. | FMA-UE, BI, RS-fMRI, FC, ADL, MRI, TR/TE, FOV, mFD, FLIRT, FNIRT, MNI152 | T0: baseline T1: post-intervention (wk 3) T2: follow-up (12 wks after T1) | ImVR-based rehabilitation is an effective tool that can improve the recovery of UE functional capabilities of subacute stroke patients when added to standard care. |
| 2 | Sip et al. (2023) [33] | RCT | To establish whether immersive VR was worth considering as a form of physical therapy and to assess the advisability of applying it to restore post-stroke hand function impairment. | First episode, maximum of 12 months since stroke diagnosis, age between 40 and 64 years, acquired motor impairment of the hemiplegic UL, functional brain damage specified with Rankin scale 1–4 at the last hospital discharge. Exclusion criteria: requirement for constant, intensive medical surveillance, presence of active comorbidities, severe arterial or pulmonary hypertension, uncontrolled diabetes, or epilepsy. EG: (n = 10) age 54.9 ± 3.98 years; CG: (n = 10) age 59.2 ± 4.34 years. | 18 days, 6 days/wk for 3 consecutive wks for both groups. EG = UL PT using the SciMed system, which incorporates the immersive VR application Virtual Mirror Hand 1.0 with the Oculus Quest 2 VR glasses module. CG = classic mirror therapy treatment relying on a reflection seen in the mirror to facilitate UL rehabilitation. | FMAUE SF-36 | T0: baseline T1: post-treatment (3 wks) | No differences between the two treatments were observed; however, patients undergoing VR therapy reported improvements in pain and multiple subjective sensations. The VR application proves to be intuitive, easily understandable, and accessible from the outset, and it was well received and well tolerated by all participants. |
| 3 | Chatterjee et al. (2022) [25] | RCT | To assess the effects of a custom-built VR environment on cognitive function, ADL recovery, and length of hospital stay in patients with subacute stroke. | Subjects aged ≥18 with unilateral, confirmed stroke (1 day to 3 weeks prior) leading to cognitive impairment. Exclusions: bilateral weakness, dementia, epilepsy, visual acuity < 6/60, or deemed unfit by therapists. Initial protocol excluded patients with (mRS) > 3; EG (n = 30, age: 77.5 ± 13.5, 13 F, 17 M): VR (a serious game with an explicit program for cognitive rehabilitation group) + UC. CG (n = 10, age: 63.5 ± 26.5, 6 F, 4 M): sham VR + UC | UC: PT, OT, SLT (duration not declared). EG: VR: VIRTUE system: customized 3D immersive VR environment reproducing ADLs (cooking, performing house chores, etc.)—5 days per wk up to 2 wks before hospital discharge—duration not declared. Hardware: HMDs (Oculus Rift S). CG: sessions of VR similar to those of the VIRTUE group (a simple task of picking up object with a hand-held controller)—duration not declared. | MoCA At T0 and T2: NEADL HADS EuroQoLS | T0: baseline T1: post-intervention T2: follow-up, 3 months from T1 | This novel immersive VR system had the potential to assist patients with severe cognitive impairment, shorten hospital stays, and supplement the traditional rehabilitation therapy offered by skilled neurotherapy professionals. |
| 4 | Hsu et al. (2022) [27] | RCT | To investigate the differences in the effects of using COT, MT, and VR-MT training on the sensorimotor function of the UL in chronic stroke patients. | Subjects with unilateral cerebral infarction/hemorrhage, >6 months post-stroke, FM-UE: 23–60, MMSE score ≥ 24. Exclusion criteria: presence of neglect, impaired vision, severe aphasia. Three randomized groups: COT (n = 17), age 56.9 ± 13.0, 12 F, 5 M; MT (n = 17), age 56.7 ± 11.5, 7 M, 10 F; VR-MT (n = 18), age 52.9 ± 11.8, 8 M, 10 F. | 20′ of UC for every group + 30′ of the specific intervention (VR-MT, COT, or MT), twice a wk for 9 wks. All participants received OT + PT and SLT if needed. COT = sensorimotor stimulation and skill training for ADLs. MT = mirror therapy, mirror box. VR-MT = personal computer + Leap Motion Controller (LMC)+ Oculus Rift VR headset. | FMA-UE MAL BBT SWM mAS | T0: baseline T1: post-intervention (9 wks) | VR-MT seemed to have potential effects on restoring upper-extremity motor function for chronic stroke patients. |
| 5 | Huang et al. (2022) [28] | RCT | To identify the effects of immersive VR on inflammation, oxidative stress, neuroplasticity, and UL motor function in stroke patients. | Subjects between 20 and 75 yo, stroke onset > 3 months, Brunnstrom stage > 3, diagnosis with computerized tomography or MRI scans, MMSE > 18. Exclusion criteria: participation in other rehabilitation-related or clinical trials within 3 months of the experiment, sensory apraxia, severe impairments in vision or visual perception, receiving warfarin or vitamin K antagonist treatment, high risk of epilepsy, or refusal to undergo the blood test. EG: Immersive VR training group (n = 15), age 50.80 ± 12.32, 9 F, 6 M; CG: COT group (n = 15), age 58.33 ± 11.22. | 16 intervention sessions for 60′/day, 2 to 3 days/wk, while attending regular OT. 6–10 tasks were assigned in each session. COT: UL training with peg board, climbing ladder, and stacking cones. VR: VR UL activities based on twenty VR scenes from commercial games. UL movements in most scenes involved aiming, shooting, hitting, waving arms, punching, and throwing objects. VR headset by HTC VIVE was utilized, consisting of an HMD device, two controllers, and two infrared laser emitter units. | FMA-UE AROM SSQ User experience ad hoc questionnaires; serum biomarkers. | T0: baseline T1: post-intervention, 60 days | HO-1, 8-OHdG, and BDNF might be potential serum biomarkers for VR-based interventions in chronic stroke patients. |
| 6 | Choi et al. (2021) [26] | RCT | To investigate the effects of VR-based digital practice program on USN rehabilitation in patients with subacute stroke. | Individuals recruited 1–6 months post-stroke, MMSE score ≥ 24; exclusion criteria: participation in experimental rehabilitation or drug research, presence of neglect, severely impaired vision, severely impaired sitting posture, limited neck ROM, presence of headache or dizziness with HMD use. EG: DP group (n = 12), age 63.00 ± 10.02, 5 M, 7 F. CG: (n = 12), age 61.58 ± 9.99, 6 M, 6 F. | Both groups: 5 × 1 h therapy session per wk for 4 wks; the training was based on established motor learning and neurodevelopmental treatment. EG: DP group: digital practice (Oculus Rift DK2 and Leap Motion devices while performing exercises in a seated position). CG: conventional USN-specific training (structured visual tracking; reading, and writing, drawing, and copying; and puzzles) for 3 × 30′/wk. | Line bisection test CBS mBI MFVP (Vertical Version) Horizontal head movements | T0: baseline T1: post-intervention, 4 wks | The DP group showed significantly greater improvements in the following:
|
| 7 | Lin et al. (2021) [29] | RCT | To develop a VR-MT system and to analyze the performance of the proposed system. | Chronic (>6 months) stroke survivors with unilateral cerebral infarction or hemorrhage; FMAUE motor assessment: 23–60; MMSE ≥ 24. Exclusion criteria: Wernicke’s or global aphasia. EG: VR-MT group (n = 9), age 49.7 ± 13.4, 7 M, 2 F. CG: MT group (n = 9), age 58.8 ± 9.6, 6 M, 3 F. | Each session lasted 50′, two days a wk for 9 wks. Intensity was equal between groups. CG: MT group: 30′ of traditional MT + 20′ of motor task-specific training. EG: VR-MT group: 30′ of VR-MT + 20′ of regular motor-task-specific training (technology: Leap Motion Controller with a compact USB peripheral device, Oculus Rift VR goggles, In-house VRMT software, developed with Unity). | FMAUE | T0: baseline T1: post-intervention (9 wks) | In general, VR-MT positively affected UL motor function in stroke patients. After training, the total motor score and the hand component of the FMA showed significant differences (p < 0.05) between the two groups and within the VR-MT group. |
| 8 | Mekbib et al. (2021) [30] | RCT | To create a unique, completely immersive VR rehabilitation protocol using commercially available peripheral VR equipment that could stimulate and activate motor neurons to aid post-stroke recovery, as well as investigate the effect of the immersive VR system compared to COT for upper-extremity therapy in stroke patients. | Adults (>18 yo), ≤3 months from first episode of ischemic or hemorrhagic stroke, with moderate-to-severe UE impairments. Normal hearing and vision, MMSE > 16. EG: VR intervention + OT (n = 12), age 52.17 ± 13.26, 9 M, 3 F; CG: OT (n = 11), age 61.00 ± 7.69, 8 M, 3 F. | EG: 1 h of VR + 1 h of OT per day, 4 days a wk for two wks. (Technology: HMD from https://www.vive.com accessed on 21 December 2023; 2 HTC Vive tracking stations; Leap Motion tracking technology; ALIENWARE high graphics laptop. The rehabilitation environment, MNVR-Rehab, was created using the Unity 3D game engine. VR: reaching, grasping.) CG: 2 h OT per day, 4 days a wk for two wks, focusing on minimizing spasticity and normalizing movement patterns. The OT intervention included daily living activities, balance control, gait training, weight shift, and distal and proximal UE functional movements. | FMA-UE BI rs-fMRI) data | T0: baseline T1: post-treatment (2 wks) | The VR group revealed significant improvements in FMA-UE scores compared to the CG. A VR system could provide extra advantages for upper-extremity therapy in patients receiving OT. |
| 9 | Song et al. (2021) [31] | RCT | To determine the effect of a combination of an immersive VR system and bilateral upper-extremity training addressing ADL on UL function and EEG measurements in stroke patients with chronic hemiplegia. | Diagnosis of stroke with hemiplegia persisting for at least 6 months and MMSE-K (Korean) ≥ 24. Exclusion criteria: visual and sensory issues, psychological instability, a history of craniotomy for brain surgery, and concurrent musculoskeletal disease with upper-extremity involvement. EG: VRBAT (n = 5), age 64.20 ± 7.08, 3 M, 2 F. CG: NBAT (n = 5), age 60.00 ± 10.88, 3 M, 2 F. | EG: VRBAT: immersive VR-based bilateral arm training using Tion software (Human IT Solution, Mokpo-si, Republic of Korea). The VR content included ADL tasks, visual-perception-oriented cognitive exercises, and evaluations delivered through Oculus Rift and Rift controller. The interventions lasted 30′ daily, 5 times a wk, for 4 wks (20 sessions), + 1 h conventional rehabilitation per day. CG: similar real-world tasks for bilateral upper-extremity training, with the same intervention frequency and duration, complemented by one hour of conventional rehabilitation per day. | Manual function test (EMG of biceps brachii, triceps brachii, and wrist extensor and flexor muscles on the affected side); Two-Point Discrimination Test; proprioception rest; stereognosis test; UL Muscle Activity (surface EMG signals of biceps brachii, triceps brachii, extensor carpi, and flexor carpi on the affected side); EEG data (only VRBAT) | T0: baseline T1: post-treatment (4 wks) | The following results were obtained in both groups:
|
| 10 | Ögün et al. (2019) [12] | RCT | To investigate the effectiveness of Leap Motion-based 3D immersive VR in the rehabilitation of upper extremities in patients with ischemic stroke. | Stroke onset between 6 and 24 months; MMSE ≥ 25; MAS < 3; UE and hand Brunnstrom score ≥ 4. Exclusion criteria: secondary neurological diseases, recurrent stroke, reduced or lost visual field, or hemorrhagic stroke. EG: VR group (n = 33), age 61.48 ± 10.92, 28 M, 5 F; CG: (n = 34), age 59.75 ± 8.07, 23 M, 9 F. | Both groups: three 1 h sessions per wk over six wks. EG: VR group: 4 games using a VR device to play task-oriented games with movement of the arm and forearm, focused on grasping and handling objects. (Technology: CG: 45′ of conventional therapy with active exercises reproducing the same movements used in the VR group. 15′ of passive VR without the need for extremity interactions). | FMA-UE ARAT FIM PASS-IADL PASS-BADL | T0: baseline T1: post-treatment (6 wks) | Both groups showed significant differences (p < 0.05) after training for all OMs except for the PASS in the CG. The VR group achieved significantly better results in the independent t-test (p < 0.05) than the CG. VR effectively improves UL function and ADLs, but no improvement in independence has been observed. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiper, P.; Godart, N.; Cavalier, M.; Berard, C.; Cieślik, B.; Federico, S.; Kiper, A.; Pellicciari, L.; Meroni, R. Effects of Immersive Virtual Reality on Upper-Extremity Stroke Rehabilitation: A Systematic Review with Meta-Analysis. J. Clin. Med. 2024, 13, 146. https://doi.org/10.3390/jcm13010146
Kiper P, Godart N, Cavalier M, Berard C, Cieślik B, Federico S, Kiper A, Pellicciari L, Meroni R. Effects of Immersive Virtual Reality on Upper-Extremity Stroke Rehabilitation: A Systematic Review with Meta-Analysis. Journal of Clinical Medicine. 2024; 13(1):146. https://doi.org/10.3390/jcm13010146
Chicago/Turabian StyleKiper, Pawel, Nathalie Godart, Manon Cavalier, Charlotte Berard, Błażej Cieślik, Sara Federico, Aleksandra Kiper, Leonardo Pellicciari, and Roberto Meroni. 2024. "Effects of Immersive Virtual Reality on Upper-Extremity Stroke Rehabilitation: A Systematic Review with Meta-Analysis" Journal of Clinical Medicine 13, no. 1: 146. https://doi.org/10.3390/jcm13010146