
Intrathecal Morphine and Post-Operative Pain Relief in Robotic Surgeries: A Systematic Review and Meta-Analysis
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection Criteria
2.2. Data Extraction and Quality Assessment
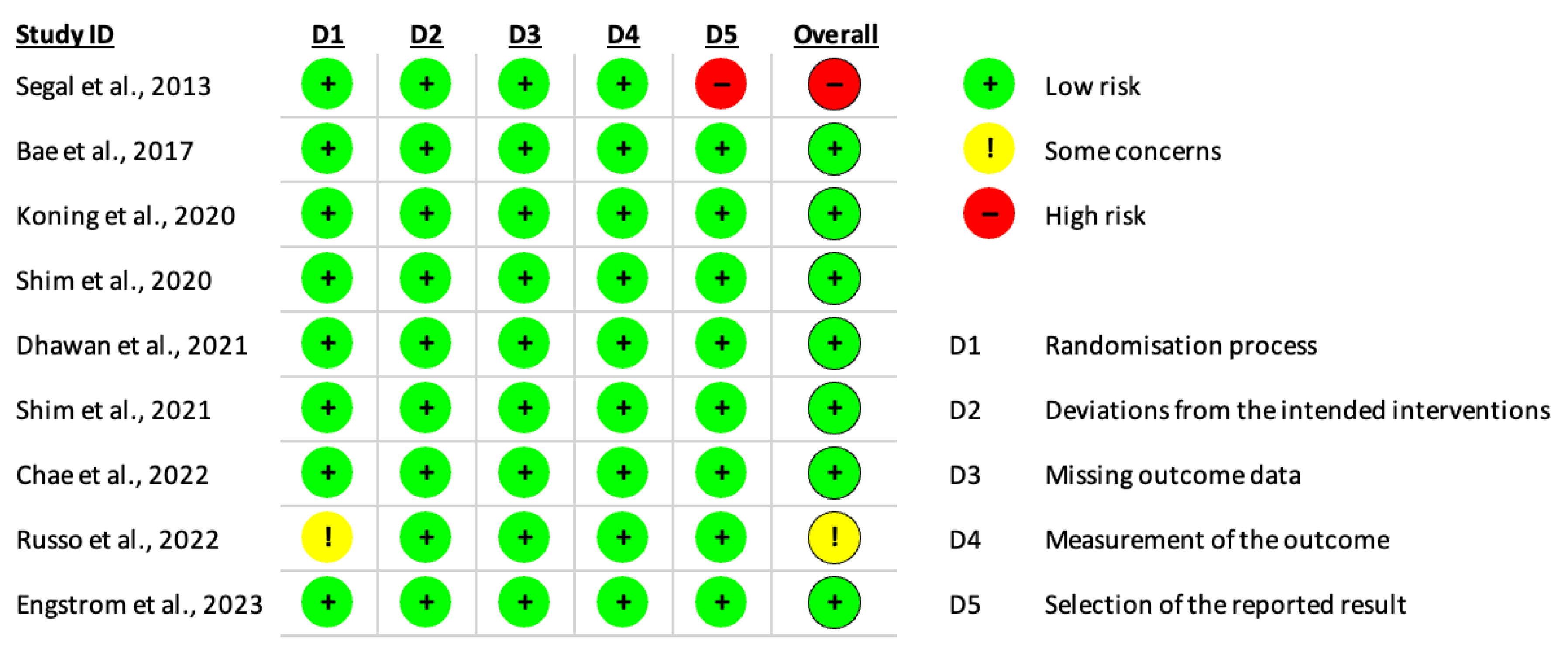
2.3. Risk of Bias Assessment
2.4. Statistical Analysis
3. Results
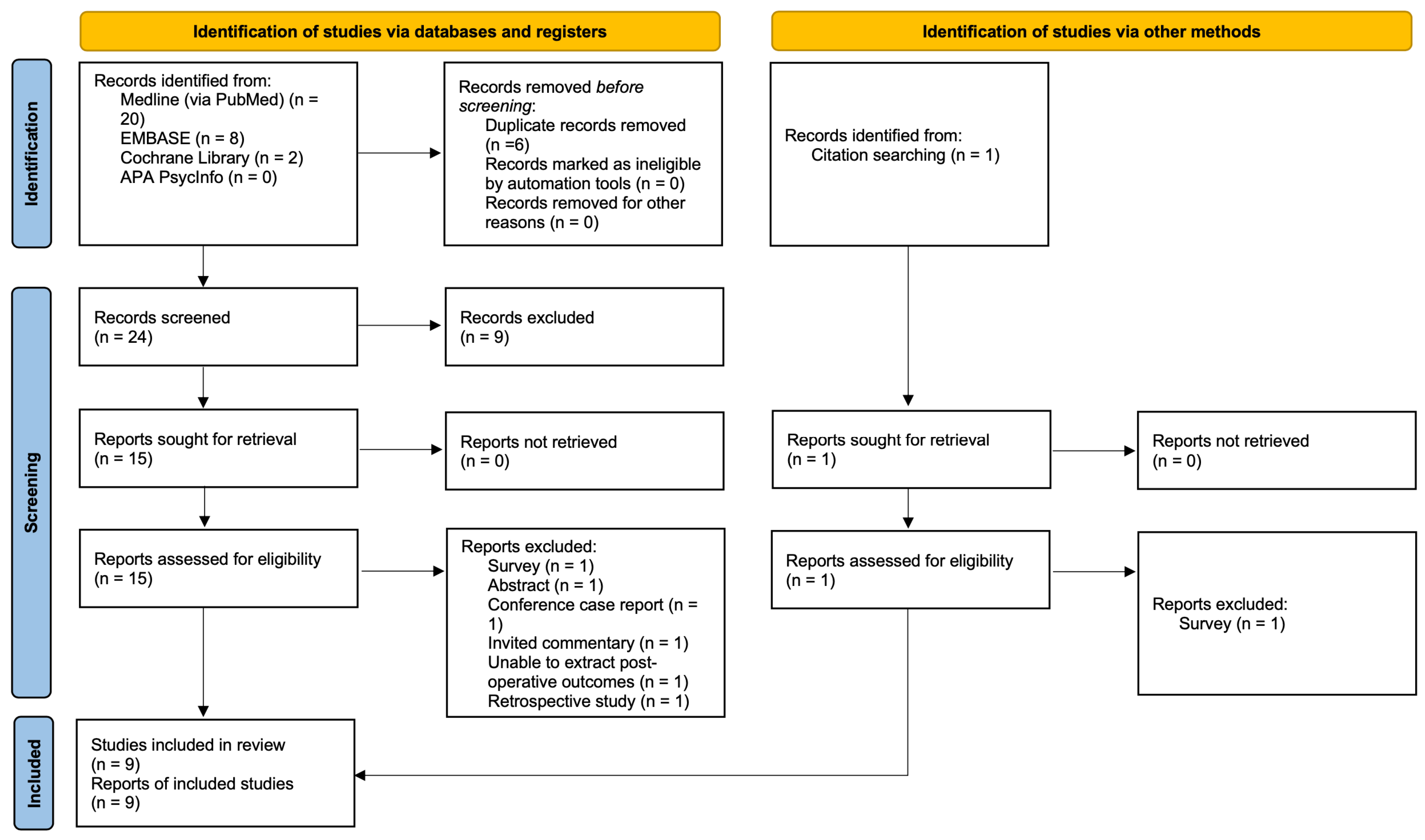
3.1. Search Results
3.2. Study Characteristics
3.3. Primary Outcomes
3.3.1. Pain Scale Methods
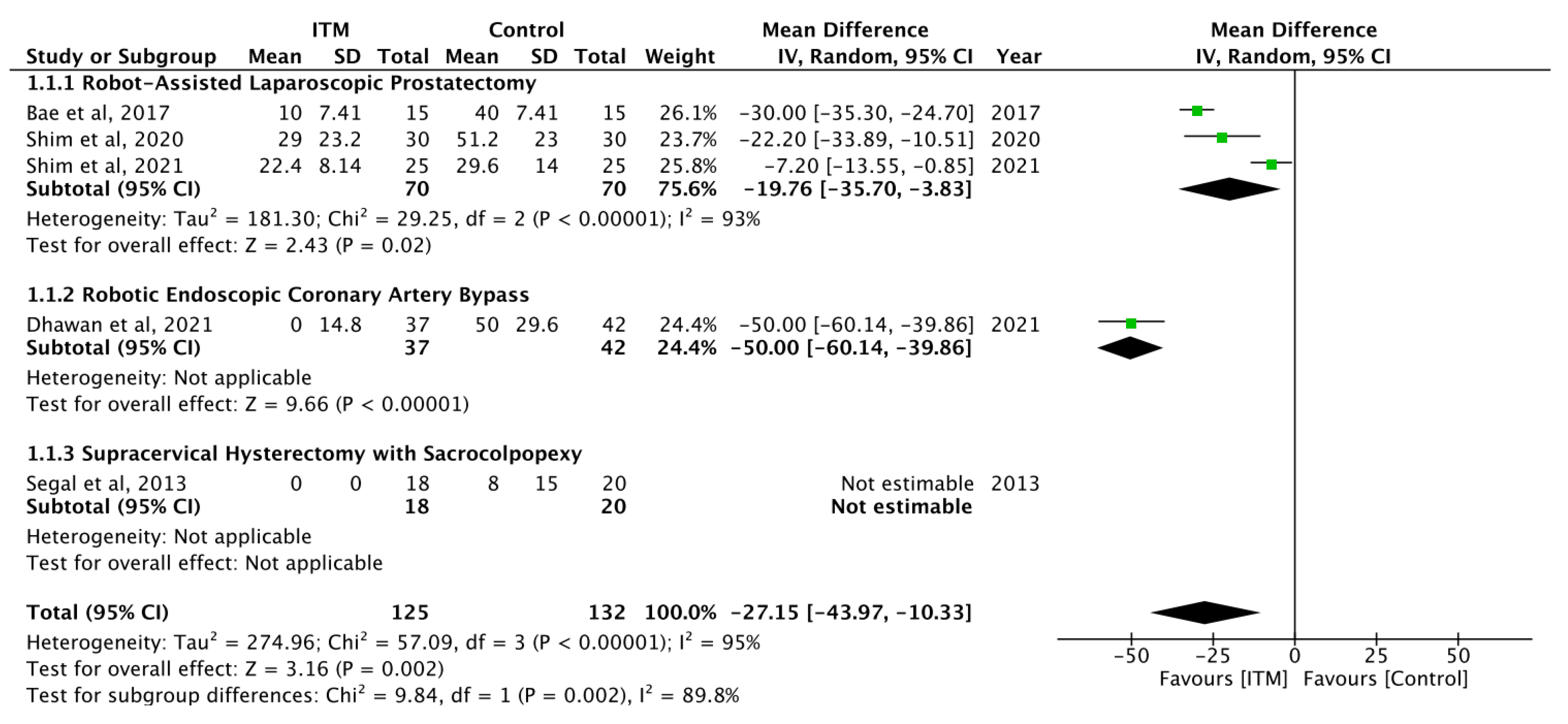
3.3.2. Pain Scores at Rest after Postoperative ITM at 24 h
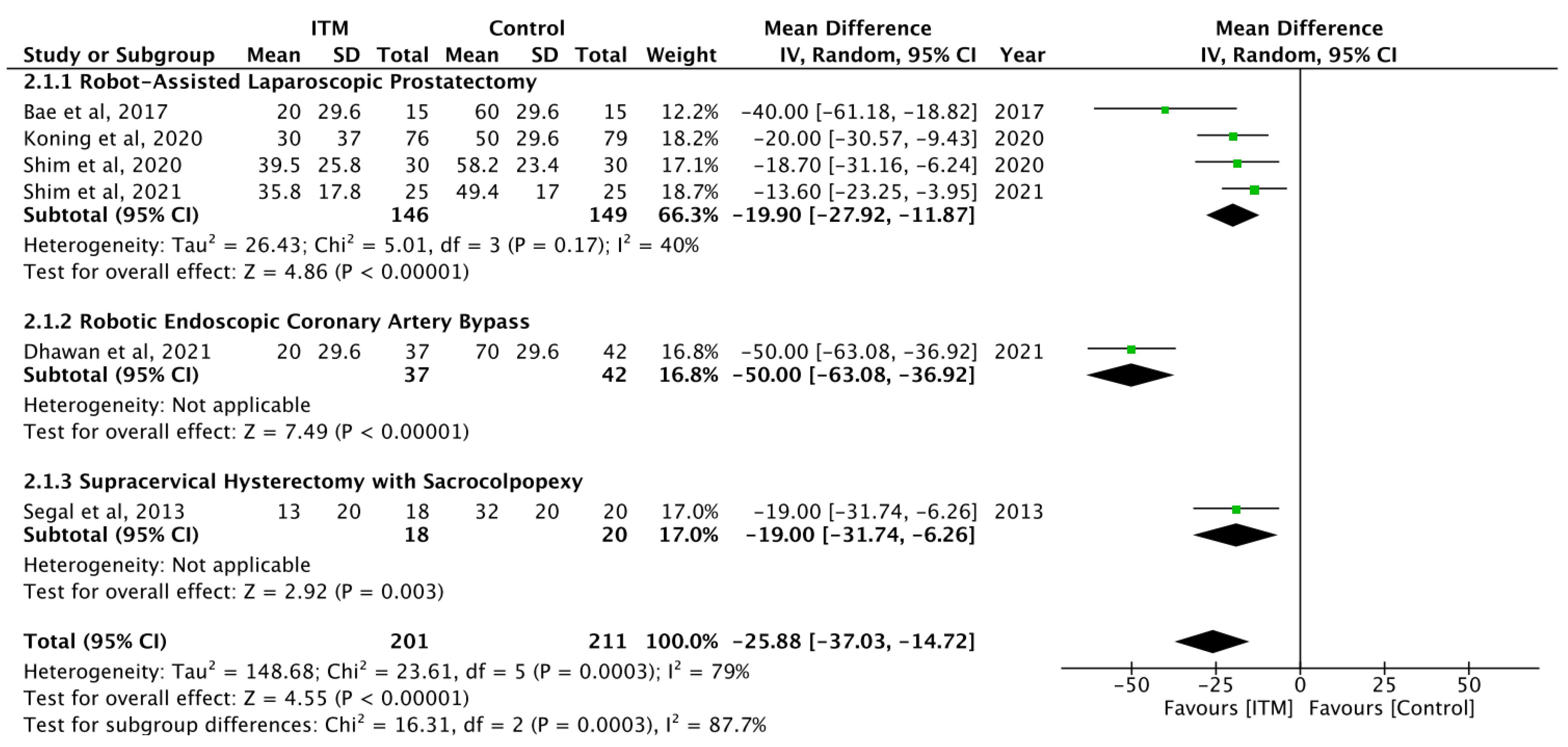
3.3.3. Pain Scores on Exertion after Postoperative ITM at 24 h
3.3.4. Pain Scores on Rest and after Exertion after Postoperative ITM at 48 h
3.3.5. Postoperative Consumption of Equivalent IV Morphine Consumption at 24 h
3.4. Secondary Outcomes
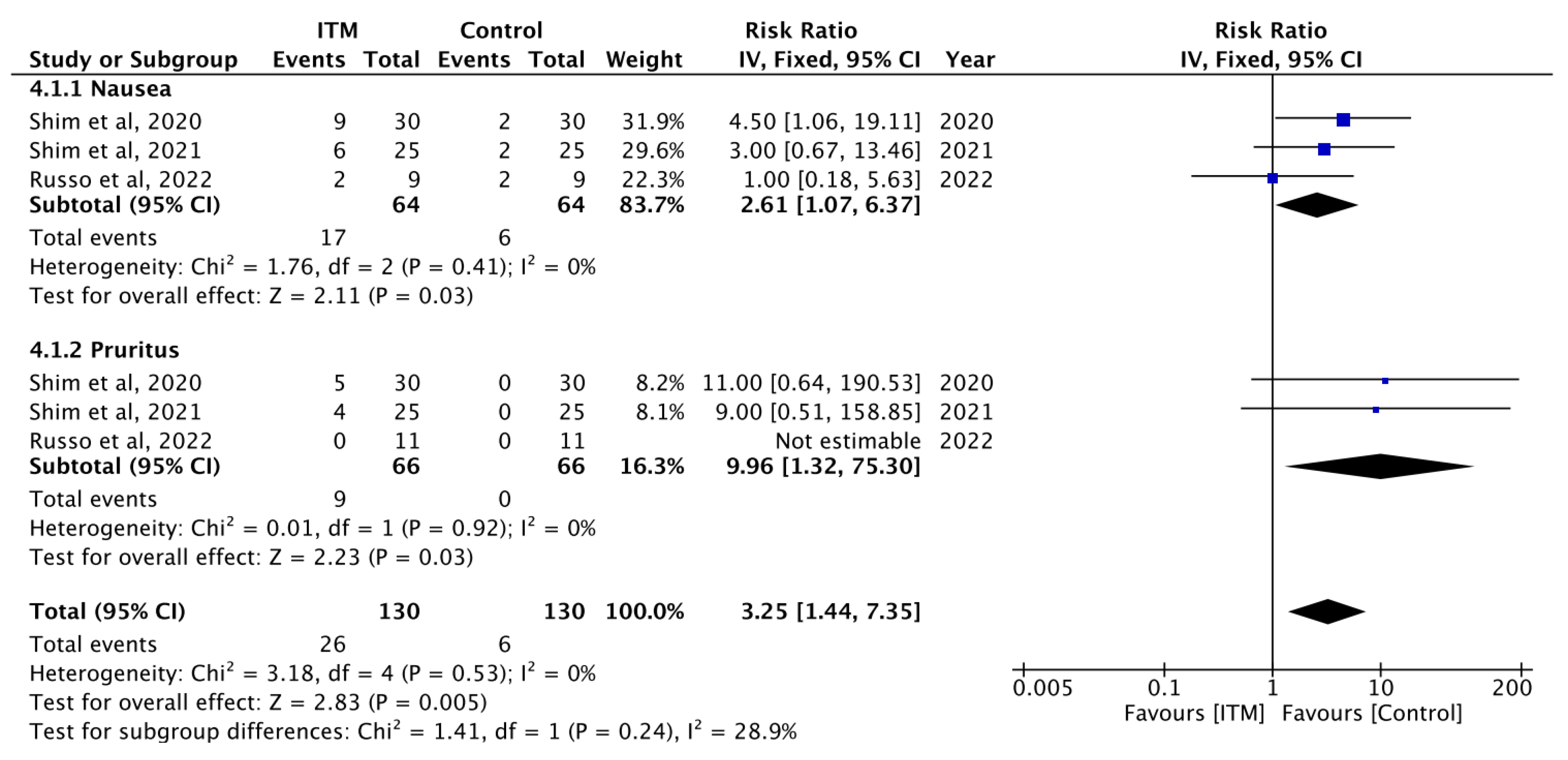
3.4.1. Nausea and Vomiting
3.4.2. Pruritus
3.4.3. Urinary Retention
3.4.4. Respiratory Depression
3.5. Quality Assessment and Risk of Bias
3.6. Test for Statistical Heterogeneity
3.7. Publication Bias
4. Discussion
5. Conclusions
Future Development/Gaps
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Santonocito, C.; Bartolotta, N.; Lanzafame, B.; Morgana, A.; Continella, C.; Cirica, G.; Astuto, M.; Sanfilippo, F. α-2 agonists vs. fentanyl as adjuvants for spinal anesthesia in elective cesarean section: A meta-analysis. Minerva Anestesiol. 2023, 89, 445–454. [Google Scholar]
- Cummings, A.; Orgill, B.D.; Fitzgerald, B.M. Intrathecal Morphine. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK499880/ (accessed on 20 July 2023).
- Aubrun, F.; Mazoit, J.X.; Riou, B. Postoperative intravenous morphine titration. Br. J. Anaesth. 2012, 108, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Olawin, A.M.; Das, J.M. Spinal Anesthesia. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK537299/ (accessed on 20 July 2023).
- Cosgrave, D.; Shanahan, E.; Conlon, N.; Joshi, M. Intrathecal Opioids: Pain Tutorial 347. Available online: https://resources.wfsahq.org/atotw/intrathecal-opioids/ (accessed on 20 July 2023).
- Hayek, S.M.; Hanes, M.C. Intrathecal therapy for chronic pain: Current trends and future needs. Curr. Pain Headache Rep. 2014, 18, 388. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.K.; Nauss, L.A.; Thomas, J.E. Pain relief by intrathecally applied morphine in man. Anesthesiology 1979, 50, 149–151. [Google Scholar] [CrossRef] [PubMed]
- Sharpe, E.E.; Molitor, R.J.; Arendt, K.W.; Torbenson, V.E.; Olsen, D.A.; Johnson, R.L.; Schroeder, D.R.; Jacob, A.K.; Niesen, A.D.; Sviggum, H.P. Intrathecal Morphine versus Intrathecal Hydromorphone for Analgesia after Cesarean Delivery: A Randomized Clinical Trial. Anesthesiology 2020, 132, 1382–1391. [Google Scholar] [CrossRef] [PubMed]
- Koning, M.V.; de Vlieger, R.; Teunissen, A.J.; Gan, M.; Ruijgrok, E.J.; de Graaff, J.C.; Koopman, J.S.; Stolker, R.J. The effect of intrathecal bupivacaine/morphine on quality of recovery in robot-assisted radical prostatectomy: A randomised controlled trial. Anaesthesia 2020, 75, 599–608. [Google Scholar] [CrossRef]
- Ferlito, S.; La Mantia, I.; Caruso, S.; Cammaroto, G.; Chiesa-Estomba, C.M.; Iannella, G.; Nocera, F.; Ingrassia, A.; Cocuzza, S.; Vicini, C.; et al. High Definition Three-Dimensional Exoscope (VITOM 3D) in E.N.T. Surgery: A Systematic Review of Current Experience. J. Clin. Med. 2022, 11, 3639. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- McKenzie, J.E.; Brennan, S.E.; Ryan, R.E.; Thomson, H.J.; Johnston, R.V.; Thomas, J. Chapter 3: Defining the criteria for including studies and how they will be grouped for the synthesis. In Cochrane Handbook for Systematic Reviews of Interventions; Version 6.4 (Updated August 2023); Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: Chichester, UK, 2023; Available online: www.training.cochrane.org/handbook/current/chapter-03 (accessed on 22 July 2023).
- Faculty of Pain Medicine of the Royal College of Anaesthetists, British Pain Society. Outcomes Measures. 2019. Available online: https://fpm.ac.uk/sites/fpm/files/documents/2019-07/Outcome%20measures%202019.pdf (accessed on 20 July 2023).
- Joshi, G.P.; Van de Velde, M.; Kehlet, H.; Pogatzki-Zahn, E.; Schug, S.; Bonnet, F.; Rawal, N.; Delbos, A.; Lavand’homme, P.; PROSPECTWorking Group Collaborators; et al. Development of evidence-based recommendations for procedure-specific pain management: PROSPECT methodology. Anaesthesia 2019, 74, 1298–1304. [Google Scholar] [CrossRef]
- British National Formulary (BNF). Prescribing in Palliative Care. Available online: https://bnf.nice.org.uk/medicines-guidance/prescribing-in-palliative-care/ (accessed on 29 July 2023).
- Faculty of Pain Medicine of the Royal College of Anaesthetists. Dose Equivalents and Changing Opioids. Available online: https://fpm.ac.uk/opioids-aware-structured-approach-opioid-prescribing/dose-equivalents-and-changing-opioids (accessed on 29 July 2023).
- Singh, P.; Yoon, S.S.; Kuo, B. Nausea: A review of pathophysiology and therapeutics. Ther. Adv. Gastroenterol. 2016, 9, 98–112. [Google Scholar] [CrossRef] [PubMed]
- Morra, M.E.; Elshafay, A.; Kansakar, A.R.; Mehyar, G.M.; Dang, N.P.H.; Mattar, O.M.; Iqtadar, S.; Mostafa, M.R.; Hai, V.N.; Vu, T.L.H.; et al. Definition of “persistent vomiting” in current medical literature: A systematic review. Medicine 2017, 96, e8025. [Google Scholar] [CrossRef] [PubMed]
- Tivoli, Y.A.; Rubenstein, R.M. Pruritus: An updated look at an old problem. J. Clin. Aesthetic Dermatol. 2009, 2, 30–36. [Google Scholar]
- Serlin, D.C.; Heidelbaugh, J.J.; Stoffel, J.T. Urinary Retention in Adults: Evaluation and Initial Management. Am. Fam. Physician 2018, 98, 496–503. [Google Scholar] [PubMed]
- National Institute of Diabetes and Digestive and Kidney Diseases. Definition & Facts for Constipation. Available online: https://www.niddk.nih.gov/health-information/digestive-diseases/constipation/definition-facts (accessed on 12 July 2023).
- Ko, S.; Goldstein, D.H.; VanDenKerkhof, E.G. Definitions of “respiratory depression” with intrathecal morphine postoperative analgesia: A review of the literature. Can. J. Anesth. 2003, 50, 679. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G.; Cochrane Statistical Methods Group. Chapter 10: Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions; Version 6.4 (updated August 2023); Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: Chichester, UK, 2023; Available online: www.training.cochrane.org/handbook/current/chapter-10 (accessed on 25 July 2023).
- Carlisle, J.B. Systematic reviews: How they work and how to use them. Anaesthesia 2007, 62, 702–707. [Google Scholar] [CrossRef]
- Bae, J.; Kim, H.C.; Hong, D.M. Intrathecal morphine for postoperative pain control following robot-assisted prostatectomy: A prospective randomized trial. J. Anesth. 2017, 31, 565–571. [Google Scholar] [CrossRef]
- Chae, M.S.; Shim, J.W.; Choi, H.; Hong, S.H.; Lee, J.Y.; Jeong, W.; Lee, B.; Kim, E.; Hong, S.H. Effects of Multimodal Bundle with Remote Ischemic Preconditioning and Intrathecal Analgesia on Early Recovery of Estimated Glomerular Filtration Rate after Robot-Assisted Laparoscopic Partial Nephrectomy for Renal Cell Carcinoma. Cancers 2022, 14, 1985. [Google Scholar] [CrossRef]
- Dhawan, R.; Daubenspeck, D.; Wroblewski, K.E.; Harrison, J.H.; McCrorey, M.; Balkhy, H.H.; Chaney, M.A. Intrathecal Morphine for Analgesia in Minimally Invasive Cardiac surgery: A Randomized, Placebo-controlled, Double-blinded clinical trial. Anesthesiology 2021, 135, 864–876. [Google Scholar] [CrossRef]
- Engström, A.J.E.; Ivarsson, C.A.; Aldergård, Å.; Henningsson, R.N. Analgesic effects of intrathecal morphine and bupivacaine during robotic-assisted surgery: A prospective randomized controlled study. Pain Pract. 2023, 23, 631–638. [Google Scholar] [CrossRef]
- Russo, A.; Romanò, B.; Papanice, D.; Cataldo, A.; Gandi, C.; Vaccarella, L.; Totaro, A.; Sacco, E.; Bassi, P.; Aceto, P.; et al. InTrathecal mORphine, traNsversus Abdominis Plane Block, and tramaDOl Infusion for Catheter-Related Bladder Discomfort in Patients Undergoing Robot-Assisted Laparoscopic Prostatectomy (TORNADO): A Pilot Prospective Controlled Study. J. Clin. Med. 2022, 11, 2136. [Google Scholar] [CrossRef] [PubMed]
- Segal, D.; Awad, N.; Nasir, H.; Mustafa, S.; Lowenstein, L. Combined spinal and general anesthesia vs general anesthesia for robotic sacrocervicopexy: A randomized controlled trial. Int. Urogynecol. J. 2014, 25, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.W.; Cho, Y.J.; Kim, M.; Hong, S.H.; Moon, H.W.; Hong, S.H.; Chae, M.S. Comparison of analgesic efficacy between rectus sheath blockade, intrathecal morphine with bupivacaine, and intravenous patient-controlled analgesia in patients undergoing robot-assisted laparoscopic prostatectomy: A prospective, observational clinical study. BMC Anesthesiol. 2020, 20, 291. [Google Scholar]
- Shim, J.W.; Cho, Y.J.; Moon, H.W.; Park, J.; Lee, H.M.; Kim, Y.S.; Moon, Y.E.; Hong, S.H.; Chae, M.S. Analgesic efficacy of intrathecal morphine and bupivacaine during the early postoperative period in patients who underwent robotic-assisted laparoscopic prostatectomy: A prospective randomized controlled study. BMC Urol. 2021, 21, 30. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Di Luca, M.; Iannella, G.; Montevecchi, F.; Magliulo, G.; De Vito, A.; Cocuzza, S.; Maniaci, A.; Meccariello, G.; Cammaroto, G.; Sgarzani, R.; et al. Use of the transoral robotic surgery to treat patients with recurrent lingual tonsillitis. Int. J. Med. Robot. Comput. Assist. Surg. 2020, 16, e2106. [Google Scholar] [CrossRef] [PubMed]
- Samii, K.; Chauvin, M.; Viars, P. Postoperative spinal analgesia with morphine. Br. J. Anaesth. 1981, 53, 817–820. [Google Scholar] [CrossRef]
- Gehling, M.; Tryba, M. Risks and side-effects of intrathecal morphine combined with spinal anaesthesia: A meta-analysis. Anaesthesia 2009, 64, 643–651. [Google Scholar] [CrossRef]
- Etches, R.C.; Sandler, A.N.; Daley, M.D. Respiratory depression and spinal opioids. Can. J. Anaesth. 1989, 36, 165–185. [Google Scholar] [CrossRef]
- Intuitive. Robotic-Assisted Surgery with da Vinci Systems. Available online: https://www.intuitive.com/en-us/patients/da-vinci-robotic-surgery (accessed on 7 August 2023).
- Sheetz, K.H.; Claflin, J.; Dimick, J.B. Trends in the Adoption of Robotic Surgery for Common Surgical Procedures. JAMA Netw. Open 2020, 3, e1918911. [Google Scholar] [CrossRef]
- Batley, S.E.; Prasad, V.; Vasdev, N.; Mohan, S.G. Post-Operative Pain Management in Patients Undergoing Robotic Urological Surgery. Curr. Urol. 2016, 9, 5–11. [Google Scholar] [CrossRef]
- Alexander, J.I. Pain after laparoscopy. Br. J. Anaesth. 1997, 79, 369–378. [Google Scholar] [CrossRef]
- Katz, N. Design and conduct of confirmatory chronic pain clinical trials. In ACTTION Guide to Clinical Trials of Pain Treatments; Dworkin, R.H., Kerns, R.D., McDermott, M.P., Turk, D.C., Veasley, C., Eds.; Wolters Kluwer Health, Inc. on behalf of the International Association for the Study of Pain: Alphen aan den Rijn, The Netherlands, 2021; pp. 99–133. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Population | Adult patients (≥18 years old) | Paediatric patients |
| Undergoing robot-assisted/robotic surgeries | Any other surgical approach | |
| Intervention | Administration of ITM in patients who have undergone robot-assisted/robotic surgery | Any other intervention |
| Comparisons | Any other analgesia/anaesthetic techniques apart from ITM in postoperative patients | No comparison |
| Placebo/saline control groups in postoperative patients | ||
| Outcomes | Pain scores: verbal rating scale, visual analogue scale and numerical rating scale | No data on pain score |
| Opioid consumption by patients | ||
| Adverse drug reactions: nausea, vomiting, pruritus, urinary retention, constipation and respiratory depression | ||
| Study Type |
|
|
| Author(s) | Country | Publication Year | Study Period | Type of Surgery | ITM Group | Spinal Anaesthesia | Control (n) | Type of Control | |
|---|---|---|---|---|---|---|---|---|---|
| n | Dose (mg) | ||||||||
| Segal et al., 2013 [32] | Israel | 2013 | 2011–2012 | subtotal hysterectomy | 18 | 0.15–0.50 † | 15 mcg fentanyl | 20 | 1–2 mcg/kg IV fentanyl and 1–3 mg/kg propofol |
| Bae et al., 2017 [27] | Korea | 2017 | 2013–2014 | RALP | 15 | 0.30 | NR | 15 | Saline with 1 mcg/mL IV morphine |
| Koning et al., 2020 [9] | Netherlands | 2020 | 2016–v2018 | RALP | 76 | 0.24/0.30 | 12.5/10 mg isobaric bupivacaine | 79 | Sham procedure with 0.1 mg/kg morphine intraoperatively |
| Shim #1 et al., 2020 [33] | Korea | 2020 | May 2020–July 2020 | RALP | 30 | 0.20 | 7.5 mg bupivacaine | 30 | 1000 mcg fentanyl 90 mg ketorolac 0.3 mg ramosetron |
| Dhawan et al., 2021 [29] | USA | 2021 | 2018–2020 | Robotic endoscopic CABG | 37 | 0.07 * | NR | 42 | 1mL saline |
| Shim #2 et al., 2021 [34] | Korea | 2021 | Oct 2019–Dec 2019 | RALP | 25 | 0.20 | 7.5 mg bupivacaine | 25 | 1000 mcg fentanyl 90 mg ketorolac 0.3 mg ramosetron |
| Chae et al., 2022 [28] | Korea | 2022 | 2020–2021 | Robot-assisted laparoscopic partial nephrectomy | 40 | 0.20 | NR | 40 | 0.5 mL saline |
| Russo et al., 2022 [31] | Italy | 2022 | 2020–2021 | RALP | 11 | 0.15 | NR | 22 | 400 mg IV tramadol in 48 mL of 0.9% NaCl solution (n = 11) TAP block with 20 mL 0.2% ropivacaine (n = 11) |
| Engström et al., 2023 [30] | Sweden | 2023 | 2021–2022 | Robotic-assisted laparoscopic hysterectomy | 46 | 0.10 | 15 mg bupivacaine | 48 | 10 mg oxycodone oral |
| ITM Group | Control | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author(s) | Type of Intervention | 24 h (Converted) | 48 h (Converted) | Postoperative IV Morphine Equivalent at 24 h (mg) | Type of Control | 24 h (Converted) | 48 h (Converted) | Postoperative IV Morphine Equivalent at 24 h (mg) | ||||
| At rest | On Exertion | At Rest | On Exertion | At Rest | On Exertion | At Rest | On Exertion | |||||
| Segal et al., 2013 [32] | 15 mcg fentanyl + 0.15–0.5 mg ITM + 1–2 mcg/kg IV fentanyl + 1–3 mg/kg propofol | 0 | 20.0 | 0 | 30.0 | 0.33 * | 1–2 mcg/kg IV fentanyl + 1–3 mg/kg propofol | 15.0 | 20.0 | 0 | 20.0 | 7.59 * |
| Bae et al., 2017 [27] | 0.30 mg ITM + 100 mg morphine + IV-PCA | 7.41 | 29.6 | 7.41 | 25.2 | 8.89 | 100 mg morphine + normal saline (IV-PCA) | 7.41 | 29.6 | 18.7 | 20.0 | 8.89 |
| Koning et al., 2020 [9] | 0.30 mg/5 mL ITM + 12.5 mg bupivacaine OR 0.24 mg/4 mL ITM + 10 mg bupivacaine | NR | 37.0 | NR | NR | Sham procedure with 0.1 mg/kg morphine | NR | 29.6 | NR | NR | ||
| Shim #1 et al., 2020 [33] | 0.20 mg ITM + 7.5 mg bupivacaine + IV-PCA | 23.2 | 25.8 | NR | NR | 1000 mcg fentanyl + 90 mg ketorolac + 0.3 mg ramosetron (IV-PCA) | 23.8 | 21.4 | NR | NR | ||
| Dhawan et al., 2021 [29] | 5 mcg/kg ITM | 14.8 | 29.6 | 11.1 | 25.9 | 22.2 | 1 ml saline | 29.6 | 29.6 | 37.0 | NR | 28.1 |
| Shim #2 et al., 2021 [34] | 0.20 mg ITM + 7.5 mg bupivacaine | 8.14 | 17.8 | NR | 6.81 | 1000 mcg fentanyl + 90 mg ketorolac + 0.3 mg Naseron with 20 mcg fentanyl bolus and 5 mcg fentanyl basal infusion (IV-PCA) | 14.0 | 17.0 | NR | 22.6 | ||
| Chae et al., 2022 [28] | 0.20 mg ITM + 1 mL saline | NR | NR | NR | 0.5 ml saline | NR | NR | NR | ||||
| Russo et al., 2022 [31] | 0.15 mg ITM | NR | NR | 0 * | 400 mg IV tramadol in 48 mL of 0.9% NaCl solution TAP block with 20 mL 0.2% ropivacaine | NR | NR | NR | ||||
| Engström et al., 2023 [30] | 0.10 mg ITM + 15 mg bupivacaine | NR | NR | NR | 10 mg oral oxycodone | NR | NR | NR | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tee, Z.H.; Tsoi, E.H.C.; Lee, Q.; Wong, Y.S.; Gibson, A.; Parsons, N.; Shaikh, S.; Forget, P. Intrathecal Morphine and Post-Operative Pain Relief in Robotic Surgeries: A Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 137. https://doi.org/10.3390/jcm13010137
Tee ZH, Tsoi EHC, Lee Q, Wong YS, Gibson A, Parsons N, Shaikh S, Forget P. Intrathecal Morphine and Post-Operative Pain Relief in Robotic Surgeries: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024; 13(1):137. https://doi.org/10.3390/jcm13010137
Chicago/Turabian StyleTee, Zi Heng, Erica Ho Ching Tsoi, Quinston Lee, Yen Sin Wong, Arron Gibson, Niamh Parsons, Shafaque Shaikh, and Patrice Forget. 2024. "Intrathecal Morphine and Post-Operative Pain Relief in Robotic Surgeries: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 13, no. 1: 137. https://doi.org/10.3390/jcm13010137