
Efficacy and Safety of Chemotherapy in Elderly Patients with Unresectable Pancreatic Cancer
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
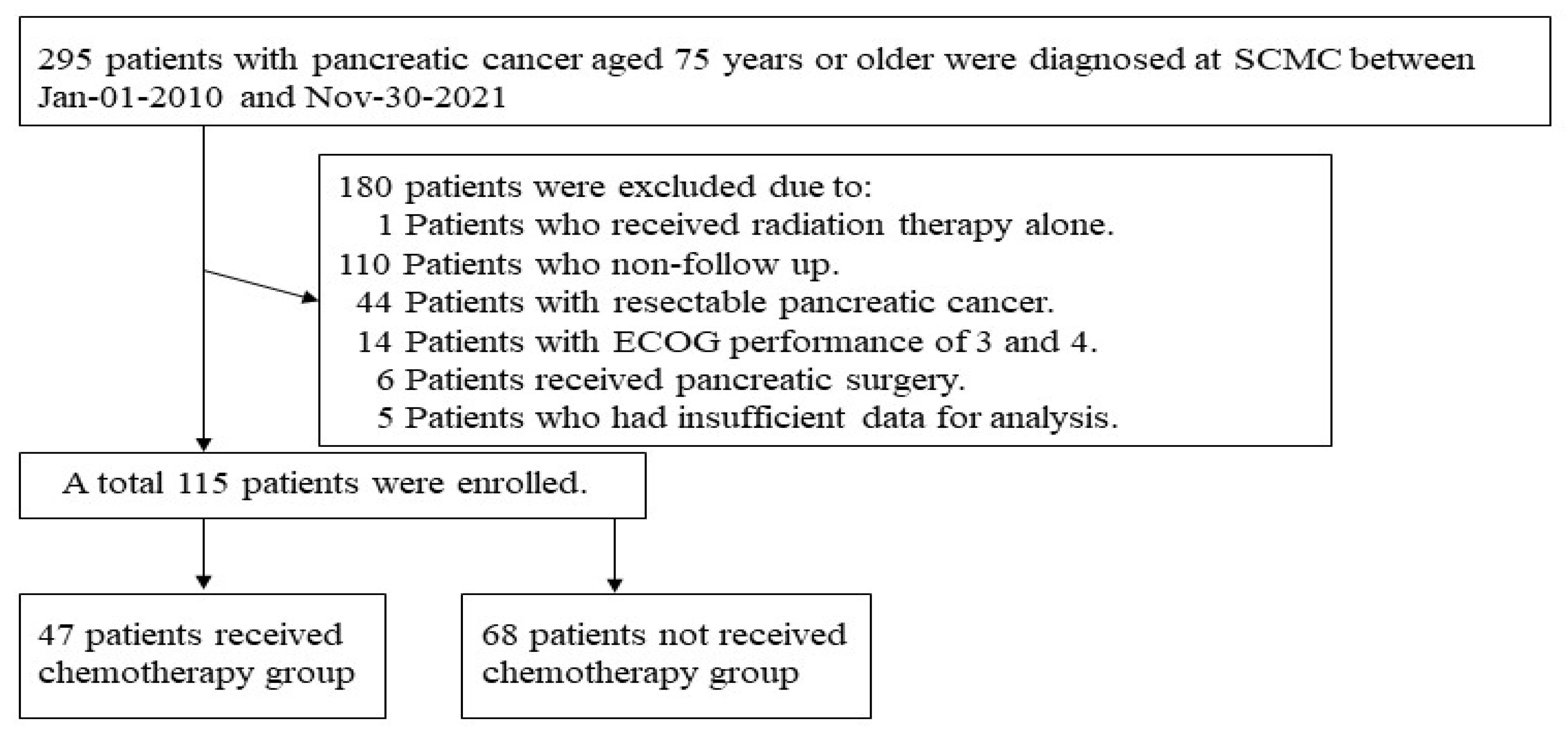
2.1. Study Design and Study Population
2.2. Data Collection
2.3. Outcomes
2.4. Statistical Analysis
2.5. Ethics
3. Results
3.1. Patient Baseline Characteristics before and after PSM
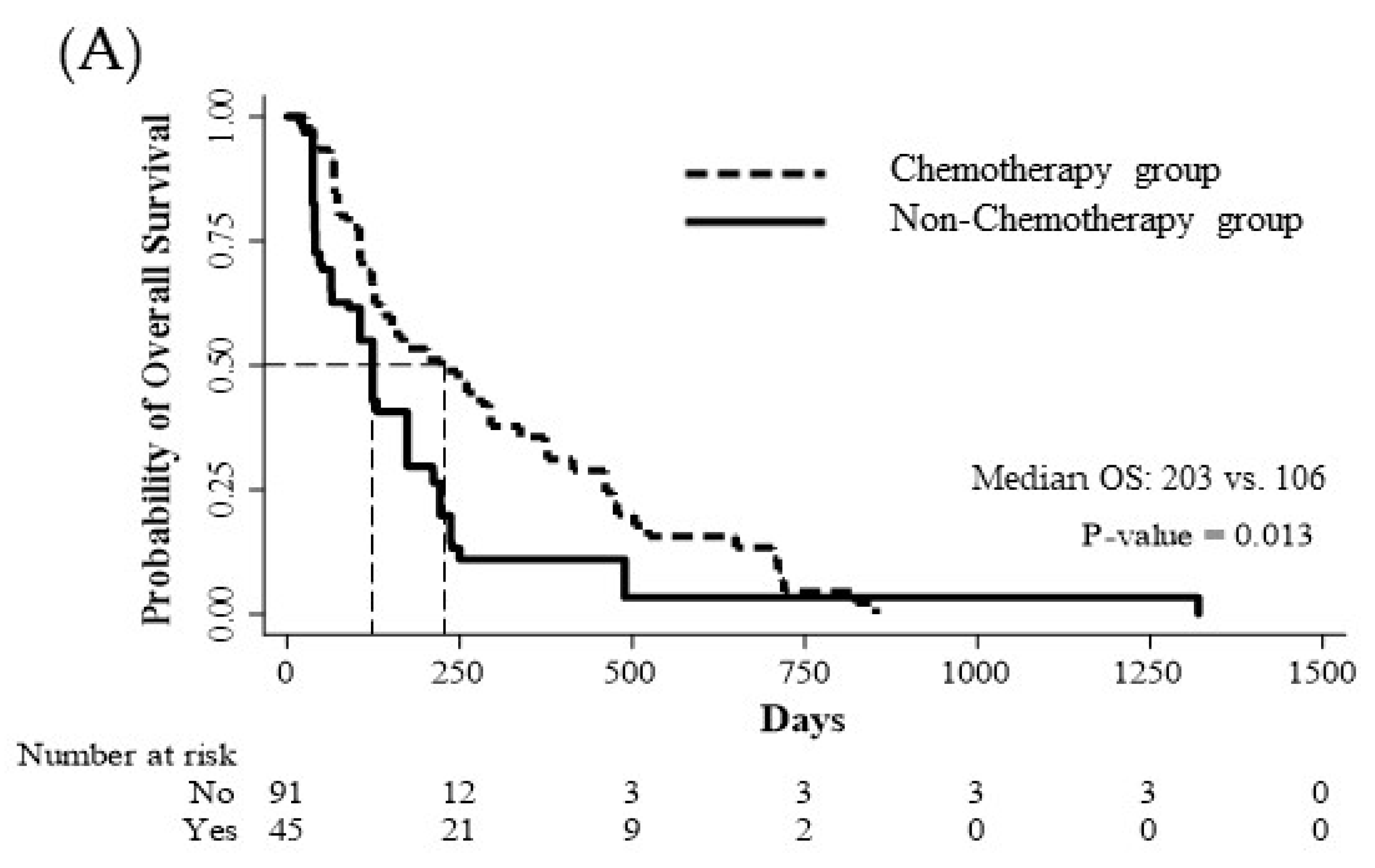
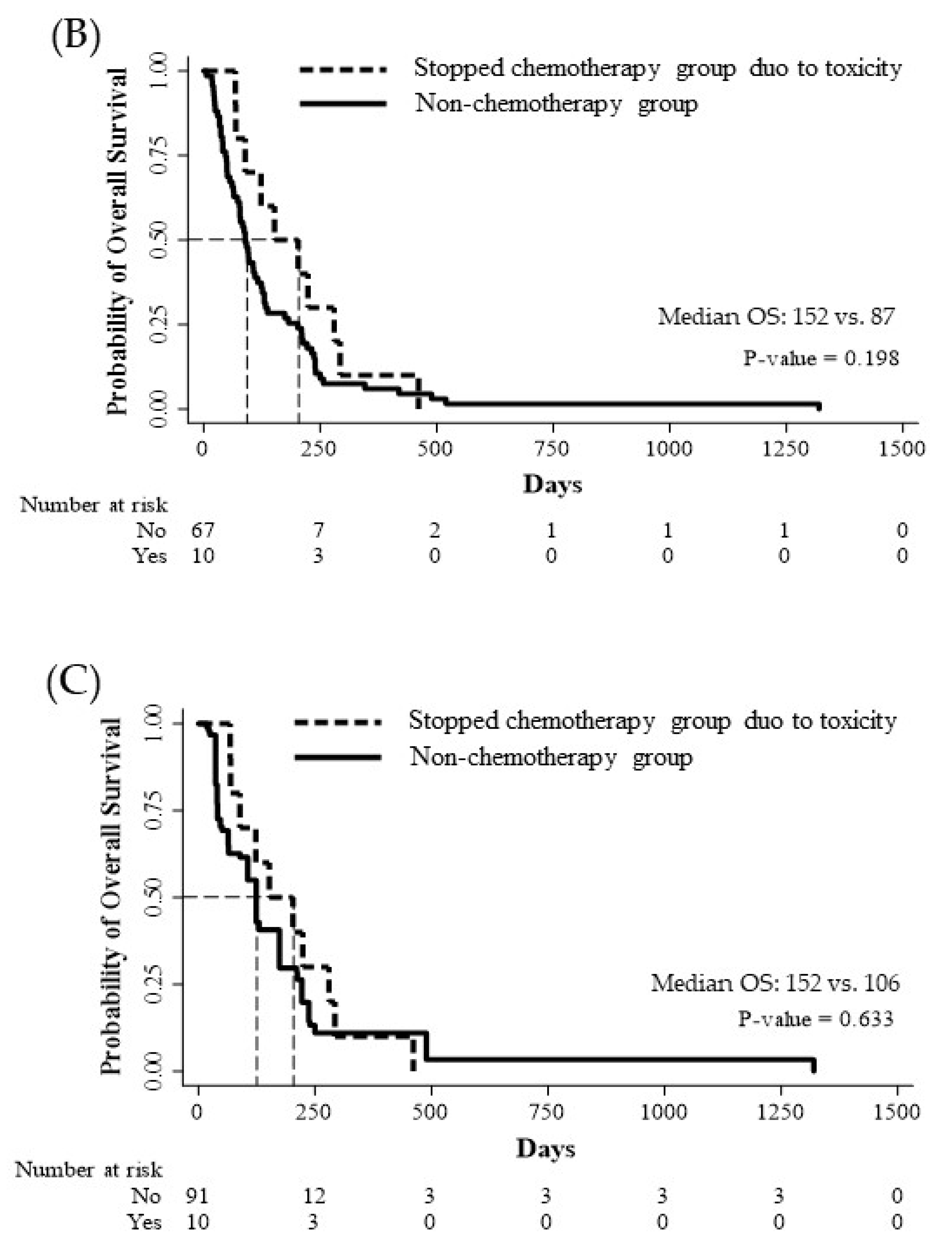
3.2. Efficacy of Chemotherapy and Factors Affecting Survival in Elderly Patients with Unresectable PC after PSM
3.3. Safety of Chemotherapy in Elderly Patients with Unresectable PC after PSM
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Pineros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.; Won, Y.J.; Park, Y.R.; Jung, K.W.; Kong, H.J.; Lee, E.S.; Community of Population-Based Regional Cancer Registries. Cancer statistics in Korea: Incidence, mortality, survival, and prevalence in 2017. Cancer Res. Treat. 2020, 52, 335–350. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Lok, V.; Ngai, C.H.; Zhang, L.; Yuan, J.; Lao, X.Q.; Ng, K.; Chong, C.; Zheng, Z.J.; Wong, M.C.S. Worldwide burden of, risk factors for, and trends in pancreatic cancer. Gastroenterology 2021, 160, 744–754. [Google Scholar] [CrossRef] [PubMed]
- Sehgal, R.; Alsharedi, M.; Larck, C.; Edwards, P.; Gress, T. Pancreatic cancer survival in elderly patients treated with chemotherapy. Pancreas 2014, 43, 306–310. [Google Scholar] [CrossRef]
- Tas, F.; Sen, F.; Keskin, S.; Kilic, L.; Yildiz, I. Prognostic factors in metastatic pancreatic cancer: Older patients are associated with reduced overall survival. Mol. Clin. Oncol. 2013, 1, 788–792. [Google Scholar] [CrossRef]
- Parmar, A.D.; Vargas, G.M.; Tamirisa, N.P.; Sheffield, K.M.; Riall, T.S. Trajectory of care and use of multimodality therapy in older patients with pancreatic adenocarcinoma. Surgery 2014, 156, 280–289. [Google Scholar] [CrossRef]
- Van Der Geest, L.G.M.; Mohammad, N.H.; Besselink, M.G.H.; Lemmens, V.; Portielje, J.E.A.; Van Laarhoven, H.W.M.; Wilmink, J.H.W.; Dutch Pancreatic Cancer Group. Nationwide trends in chemotherapy use and survival of elderly patients with metastatic pancreatic cancer. Cancer Med. 2017, 6, 2840–2849. [Google Scholar] [CrossRef]
- Lamont, E.B.; Schilsky, R.L.; He, Y.; Muss, H.; Cohen, H.J.; Hurria, A.; Meilleur, A.; Kindler, H.L.; Venook, A.; Lilenbaum, R.; et al. Generalizability of trial results to elderly Medicare patients with advanced solid tumors (Alliance 70802). J. Natl. Cancer Inst. 2015, 107, 336. [Google Scholar] [CrossRef]
- McGuigan, A.; Kelly, P.; Turkington, R.C.; Jones, C.; Coleman, H.G.; McCain, R.S. Pancreatic cancer: A review of clinical diagnosis, epidemiology, treatment and outcomes. World J. Gastroenterol. 2018, 24, 4846–4861. [Google Scholar] [CrossRef]
- Burris, H.A.; Moore, M.J.; Andersen, J.; Green, M.R.; Rothenberg, M.L.; Modiano, M.R.; Cripps, M.C.; Portenoy, R.K.; Storniolo, A.M.; Tarassoff, P.; et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: A randomized trial. J. Clin. Oncol. 1997, 15, 2403–2413. [Google Scholar] [CrossRef]
- Vaccaro, V.; Sperduti, I.; Milella, M. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2011, 365, 768–769. [Google Scholar] [CrossRef]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef]
- Kim, J.-j.; Kim, J. A study of health care system housing and environment of the elderly. J. Korea Inst. Electron. Commun. Sci. 2012, 7, 925–930. [Google Scholar]
- Alterovitz, S.S.; Mendelsohn, G.A. Relationship goals of middle-aged, young-old, and old-old internet daters: An analysis of online personal ads. J. Aging Stud. 2013, 27, 159–165. [Google Scholar] [CrossRef]
- Mizrahi, J.D.; Rogers, J.E.; Hess, K.R.; Wolff, R.A.; Varadhachary, G.R.; Javle, M.M.; Shroff, R.T.; Ho, L.; Fogelman, D.R.; Raghav, K.P.S.; et al. Modified FOLFIRINOX in pancreatic cancer patients age 75 or older. Pancreatology 2020, 20, 501–504. [Google Scholar] [CrossRef]
- Macchini, M.; Chiaravalli, M.; Zanon, S.; Peretti, U.; Mazza, E.; Gianni, L.; Reni, M. Chemotherapy in elderly patients with pancreatic cancer: Efficacy, feasibility and future perspectives. Cancer Treat. Rev. 2019, 72, 1–6. [Google Scholar] [CrossRef]
- Li, X.; Huang, D.B.; Zhang, Q.; Guo, C.X.; Fu, Q.H.; Zhang, X.C.; Tang, T.Y.; Su, W.; Chen, Y.W.; Chen, W.; et al. The efficacy and toxicity of chemotherapy in the elderly with advanced pancreatic cancer. Pancreatology 2020, 20, 95–100. [Google Scholar] [CrossRef]
- Kuroda, T.; Kumagi, T.; Yokota, T.; Azemoto, N.; Hasebe, A.; Seike, H.; Nishiyama, M.; Inada, N.; Shibata, N.; Miyata, H. Efficacy of chemotherapy in elderly patients with unresectable pancreatic cancer: A multicenter review of 895 patients. BMC Gastroenterol. 2017, 17, 66. [Google Scholar] [CrossRef]
- Yamagishi, Y.; Higuchi, H.; Izumiya, M.; Sakai, G.; Iizuka, H.; Nakamura, S.; Adachi, M.; Hozawa, S.; Takaishi, H.; Hibi, T. Gemcitabine as first-line chemotherapy in elderly patients with unresectable pancreatic carcinoma. J. Gastroenterol. 2010, 45, 1146–1154. [Google Scholar] [CrossRef]
- Bockhorn, M.; Uzunoglu, F.G.; Adham, M.; Imrie, C.; Milicevic, M.; Sandberg, A.A.; Asbun, H.J.; Bassi, C.; Buchler, M.; Charnley, R.M.; et al. Borderline resectable pancreatic cancer: A consensus statement by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2014, 155, 977–988. [Google Scholar] [CrossRef] [PubMed]
- Isaji, S.; Mizuno, S.; Windsor, J.A.; Bassi, C.; Fernández-del Castillo, C.; Hackert, T.; Hayasaki, A.; Katz, M.H.; Kim, S.-W.; Kishiwada, M. International consensus on definition and criteria of borderline resectable pancreatic ductal adenocarcinoma 2017. Pancreatology 2018, 18, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE) Version 4; U.S. Department of Health and Human Services: Washington, DC, USA, 2009.
- Hentic, O.; Dreyer, C.; Rebours, V.; Zappa, M.; Lévy, P.; Raymond, E.; Ruszniewski, P.; Hammel, P. Gemcitabine in elderly patients with advanced pancreatic cancer. World J. Gastroenterol. WJG 2011, 17, 3497. [Google Scholar] [CrossRef]
- Ohwada, S.; Todaka, A.; Nakase, H.; Shirasu, H.; Kawakami, T.; Hamauchi, S.; Tsushima, T.; Yokota, T.; Onozawa, Y.; Yasui, H. Effectiveness and safety of gemcitabine plus nab-paclitaxel in elderly patients with advanced pancreatic cancer: A single-center retrospective cohort study. Investig. New Drugs 2022, 40, 1106–1116. [Google Scholar] [CrossRef]
- Dell’Aquila, E.; Fulgenzi, C.A.M.; Minelli, A.; Citarella, F.; Stellato, M.; Pantano, F.; Russano, M.; Cursano, M.C.; Napolitano, A.; Zeppola, T. Prognostic and predictive factors in pancreatic cancer. Oncotarget 2020, 11, 924–941. [Google Scholar] [CrossRef]
- Le, N.; Sund, M.; Vinci, A.; Gems Collaborating Group of Pancreas. Prognostic and predictive markers in pancreatic adenocarcinoma. Dig. Liver Dis. 2016, 48, 223–230. [Google Scholar] [CrossRef]
- Majumder, K.; Gupta, A.; Arora, N.; Singh, P.P.; Singh, S. Premorbid obesity and mortality in patients with pancreatic cancer: A systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 2016, 14, 355–368.e2; quiz e332. [Google Scholar] [CrossRef]
- Cho, I.R.; Kang, H.; Jo, J.H.; Lee, H.S.; Chung, M.J.; Park, J.Y.; Park, S.W.; Song, S.Y.; An, C.; Park, M.S.; et al. FOLFIRINOX vs gemcitabine/nab-paclitaxel for treatment of metastatic pancreatic cancer: Single-center cohort study. World J. Gastrointest. Oncol. 2020, 12, 182–194. [Google Scholar] [CrossRef]
- Wedding, U.; Honecker, F.; Bokemeyer, C.; Pientka, L.; Höffken, K. Tolerance to chemotherapy in elderly patients with cancer. Cancer Control J. Moffitt Cancer Cent. 2007, 14, 44–56. [Google Scholar] [CrossRef]
- Hwang, I.G.; Kwon, M.; Kim, J.W.; Kim, S.H.; Lee, Y.-G.; Kim, J.Y.; Koh, S.-J.; Ko, Y.H.; Shin, S.H.; Hong, S. Prevalence and predictive factors for upfront dose reduction of the first cycle of first-line chemotherapy in older adults with metastatic solid cancer: Korean cancer study group (KCSG) multicenter study. Cancers 2021, 13, 331. [Google Scholar] [CrossRef]
- Berger, A.K.; Haag, G.M.; Ehmann, M.; Byl, A.; Jäger, D.; Springfeld, C. Palliative chemotherapy for pancreatic adenocarcinoma: A retrospective cohort analysis of efficacy and toxicity of the FOLFIRINOX regimen focusing on the older patient. BMC Gastroenterol. 2017, 17, 143. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total Patient (n = 115) | Chemotherapy | p Value | ||
|---|---|---|---|---|
| Yes (n = 47) | No (n = 68) | |||
| Age, years | 83.4 ± 5.1 | 80.9 ± 3.9 | 85.1 ± 5.1 | <0.001 |
| Sex, Female | 64 (55.7) | 22 (46.9) | 42 (61.8) | 0.112 |
| BMI, kg/m2 | 21.3 ± 3.0 | 21.9 ± 3.0 | 20.9 ± 3.0 | 0.087 |
| Charlson comorbidity index | 9.7 ± 1.6 | 9.5 ± 1.9 | 9.8 ± 1.4 | 0.312 |
| MI | 10 (8.7) | 7 (14.9) | 3 (4.4) | 0.088 |
| CHF | 2 (1.7) | 1 (2.1) | 1 (1.5) | >0.999 |
| CVA | 9 (7.8) | 5 (10.6) | 4 (5.9) | 0.483 |
| COPD | 3 (2.6) | 2 (4.3) | 1 (1.5) | 0.566 |
| Connective tissue disease | 3 (2.6) | 1 (2.1) | 2 (2.9) | >0.999 |
| PUD | 1 (0.9) | 1 (2.1) | 0 (0.0) | 0.409 |
| Liver disease, severe | 2 (1.7) | 1 (2.1) | 1 (1.5) | >0.999 |
| DM | 0.158 | |||
| Uncomplicated | 15 (13.0) | 9 (19.2) | 6 (8.8) | |
| End-organ damage | 1 (0.9) | 0 (0.0) | 1 (1.5) | |
| CKD | 2 (1.7) | 1 (2.1) | 1 (1.5) | >0.999 |
| ECOG performance | 0.001 | |||
| 0 | 32 (27.8) | 21 (44.7) | 11 (16.2) | |
| 1 | 50 (43.5) | 19 (40.4) | 31 (45.6) | |
| 2 | 33 (28.7) | 7 (14.9) | 26 (38.2) | |
| Biliary drainage, yes | 53 (46.1) | 19 (40.4) | 34 (50.0) | 0.311 |
| Location of pancreatic cancer | 0.049 | |||
| Head or uncinate | 64 (55.7) | 21 (44.7) | 43 (63.2) | |
| Body or tail | 51 (44.3) | 26 (55.3) | 25 (36.8) | |
| Resectability of pancreatic cancer | 0.486 | |||
| Locally advanced | 21 (18.3) | 10 (21.3) | 11 (16.2) | |
| Metastatic | 94 (81.7) | 37 (78.7) | 57 (83.8) | |
| PET-CT | 62 (53.9) | 35 (74.5) | 27 (39.7) | <0.001 |
| Histologic diagnosis | <0.001 | |||
| None | 23 (20.0) | 0 (0.0) | 23 (33.8) | |
| EUS-FNA | 56 (48.7) | 35 (74.5) | 21 (30.9) | |
| ERCP & Endoscopic route * | 15 (13.0) | 3 (6.4) | 12 (17.7) | |
| Percutaneous route ** | 16 (13.9) | 5 (10.6) | 11 (16.2) | |
| Unknown | 5 (4.4) | 4 (8.5) | 1 (1.5) | |
| Median Overall survival | 124 (65–250) | 224 (105–461) | 89 (47–202) | <0.001 |
| No. of Patients (%) | |
|---|---|
| Firstline Chemotherapy, regimen | |
| 5-FU | 1 (2.1) |
| Etoposide + cisplatin | 1 (2.1) |
| FOLFIRINOX | 4 (8.5) |
| Gemcitabine | 16 (34.0) |
| Gemcitabine + Cisplatin | 1 (2.1) |
| Gemcitabine + Nab-paclitaxel | 22 (46.8) |
| TS-1 | 2 (4.3) |
| Firstline Chemotherapy, dose | |
| Full dose | 30 (63.8) |
| Adjust dose | 17 (36.2) |
| Firstline Chemotherapy, response * | |
| PR | 10 (21.3) |
| SD | 24 (51.1) |
| PD | 2 (4.3) |
| Not assessed ** | 11 (23.4) |
| Received chemotherapy | |
| First-line | 39 (83.0) |
| Second-line | 5 (10.6) |
| Third-line | 3 (6.4) |
| Second-line chemotherapy, regimen | |
| FOLFIRINOX | 1 (12.5) |
| Gemcitabine | 1 (12.5) |
| Gemcitabine + Erlotinib | 1 (12.5) |
| Capecitabine | 1 (12.5) |
| TS-1 | 4 (50.0) |
| Mean chemotherapy cycle | 6.8 ± 6.4 |
| Total Patient (n = 136) | Chemotherapy | p Value | ||
|---|---|---|---|---|
| Yes (n = 45) | No (n = 91) | |||
| Age, years | 81.0 ± 4.1 | 80.8 ± 3.6 | 81.1 ± 4.3 | 0.698 |
| Sex, Female | 66 (48.5) | 21 (46.7) | 45 (49.5) | 0.760 |
| BMI, kg/m2 | 21.6 ± 3.1 | 21.8 ± 3.0 | 21.6 ± 3.2 | 0.648 |
| Charlson comorbidity index | 9.4 ± 1.6 | 9.4 ± 1.9 | 9.3 ± 1.4 | 0.634 |
| MI | 7 (5.2) | 7 (15.6) | 0 (0.0) | <0.001 |
| CHF | 1 (0.7) | 1 (2.2) | 0 (0.0) | 0.331 |
| CVA | 12 (8.8) | 5 (11.1) | 7 (7.7) | 0.531 |
| COPD | 2 (1.5) | 2 (4.4) | 0 (0.0) | 0.043 |
| Connective tissue disease | 1 (0.7) | 1 (2.2) | 0 (0.0) | 0.153 |
| PUD | 1 (0.7) | 1 (2.2) | 0 (0.0) | 0.153 |
| Liver disease, severe | 1 (0.7) | 1 (2.2) | 0 (0.0) | 0.153 |
| DM, uncomplicated | 19 (14.0) | 9 (20.0) | 10 (11.0) | 0.190 |
| CKD | 4 (2.9) | 0 (0.0) | 4 (4.4) | 0.153 |
| ECOG performance | 0.390 | |||
| 0 | 64 (47.1) | 20 (44.4) | 44 (48.3) | |
| 1 | 58 (42.6) | 18 (40.0) | 40 (44.0) | |
| 2 | 14 (10.3) | 7 (15.6) | 7 (7.7) | |
| Biliary drainage, yes | 59 (43.4) | 18 (40.0) | 41 (45.1) | 0.576 |
| Location of pancreatic cancer | 0.078 | |||
| Head or uncinate | 75 (55.2) | 20 (44.4) | 55 (60.4) | |
| Body or tail | 61 (44.8) | 25 (55.6) | 36 (39.6) | |
| Resectability of pancreatic cancer | 0.051 | |||
| Locally advanced | 19 (14.0) | 10 (22.2) | 9 (9.9) | |
| Metastatic | 117 (86.0) | 35 (77.8) | 82 (90.1) | |
| PET-CT | 47 (34.6) | 11 (24.4) | 36 (39.6) | 0.081 |
| Histologic diagnosis | <0.001 | |||
| None | 16 (11.8) | 0 (0.0) | 16 (17.6) | |
| EUS-FNA | 81 (59.6) | 35 (77.8) | 46 (50.6) | |
| ERCP & Endoscopic route * | 13 (9.6) | 3 (6.7) | 10 (11.0) | |
| Percutaneous route ** | 23 (16.9) | 4 (8.9) | 19 (20.9) | |
| Unknown | 3 (2.2) | 3 (6.7) | 0 (0.0) | |
| Median Overall survival | 126 (64–244) | 224 (105–461) | 124 (41–222) | 0.001 |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Chemotherapy | ||||
| Yes | 0.64 (0.44–0.92) | 0.017 | 0.60 (0.41–0.90) | 0.012 |
| BMI | 1.10 (1.03–1.18) | 0.003 | 1.12 (1.05–1.20) | 0.001 |
| Charlson comorbidity index | 1.13 (1.00–1.27) | 0.056 | ||
| ECOG performance | ||||
| 0 | Reference | Reference | ||
| 1 | 1.51 (1.05–2.18) | 0.028 | 1.42 (0.97–2.08) | 0.070 |
| 2 | 2.61 (1.44–4.73) | 0.001 | 2.34 (1.21–4.52) | 0.012 |
| Biliary drainage, yes | 1.02 (0.72–1.45) | 0.892 | ||
| Location of pancreatic cancer | ||||
| Head or uncinate | reference | |||
| Body or tail | 0.91 (0.64–1.28) | 0.585 | ||
| Resectability of pancreatic cancer | ||||
| Locally advanced | reference | |||
| Metastatic | 1.83 (1.12–2.99) | 0.016 | 1.73 (1.01–2.96) | 0.046 |
| Firstline Chemotherapy regimen | ||||
| 5-FU | reference | |||
| Etoposide + cisplatin | - | |||
| FOLFIRINOX | 0.22 (0.02–3.02) | 0.258 | ||
| Gemcitabine | 1.74 (0.23–13.57) | 0.580 | ||
| Gemcitabine + Cisplatin | 0.25 (0.01–5.01) | 0.364 | ||
| Gemcitabine + Nab-paclitaxel | 2.41 (0.32–18.18) | 0.394 | ||
| TS-1 | 0.67 (0.06–8.25) | 0.758 | ||
| Firstline Chemotherapy dose | ||||
| Full dose | reference | |||
| Adjust dose | 1.38 (0.45–2.56) | 0.305 | ||
| Firstline Chemotherapy response * | ||||
| PR | reference | |||
| SD | 1.18 (0.54–2.58) | 0.680 | ||
| PD | 7.30 (1.40–37.94) | 0.018 | ||
| Adverse Events | ||
|---|---|---|
| Grade 1 or 2 No. of Patients (%) | Grade 3 or 4 No. of Patients (%) | |
| Hematologic | ||
| Neutropenia | 4 (8.5) | 0 (0.0) |
| Febrile-neutropenia | 0 (0.0) | 1 (2.1) |
| Thrombocytopenia | 1 (2.1) | 0 (0.0) |
| Nonhematologic | ||
| Fatigue | 22 (46.8) | 6 (12.8) |
| Anorexia | 8 (17.0) | 0 (0.0) |
| Vomiting | 1 (2.1) | 1 (2.1) |
| Diarrhea | 0 (0.0) | 2 (4.3) |
| Constipation | 3 (6.4) | 0 (0.0) |
| Sensory neuropathy | 2 (4.3) | 0 (0.0) |
| Mucositis | 1 (2.1) | 0 (0.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwan, B.S.; Lee, O.J.; Kim, H.J.; Kim, K.M.; Shim, S.G.; Cho, D.H.; Kong, S.M.; Kim, J.Y.; Ji, J.H. Efficacy and Safety of Chemotherapy in Elderly Patients with Unresectable Pancreatic Cancer. J. Clin. Med. 2023, 12, 3334. https://doi.org/10.3390/jcm12093334
Kwan BS, Lee OJ, Kim HJ, Kim KM, Shim SG, Cho DH, Kong SM, Kim JY, Ji JH. Efficacy and Safety of Chemotherapy in Elderly Patients with Unresectable Pancreatic Cancer. Journal of Clinical Medicine. 2023; 12(9):3334. https://doi.org/10.3390/jcm12093334
Chicago/Turabian StyleKwan, Byung Soo, Ok Jae Lee, Hyun Jin Kim, Kwang Min Kim, Sang Goon Shim, Dae Hyeon Cho, Sung Min Kong, Jun Young Kim, and Jun Ho Ji. 2023. "Efficacy and Safety of Chemotherapy in Elderly Patients with Unresectable Pancreatic Cancer" Journal of Clinical Medicine 12, no. 9: 3334. https://doi.org/10.3390/jcm12093334