

Value of Fractional Exhaled Nitric Oxide in Diagnosing Mild Asthma Responsive to Inhaled Corticosteroids
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Pulmonary Function Tests
2.3. FeNO Measurement
2.4. Skin Prick Test
2.5. Statistical Analysis
3. Results
3.1. Study Population
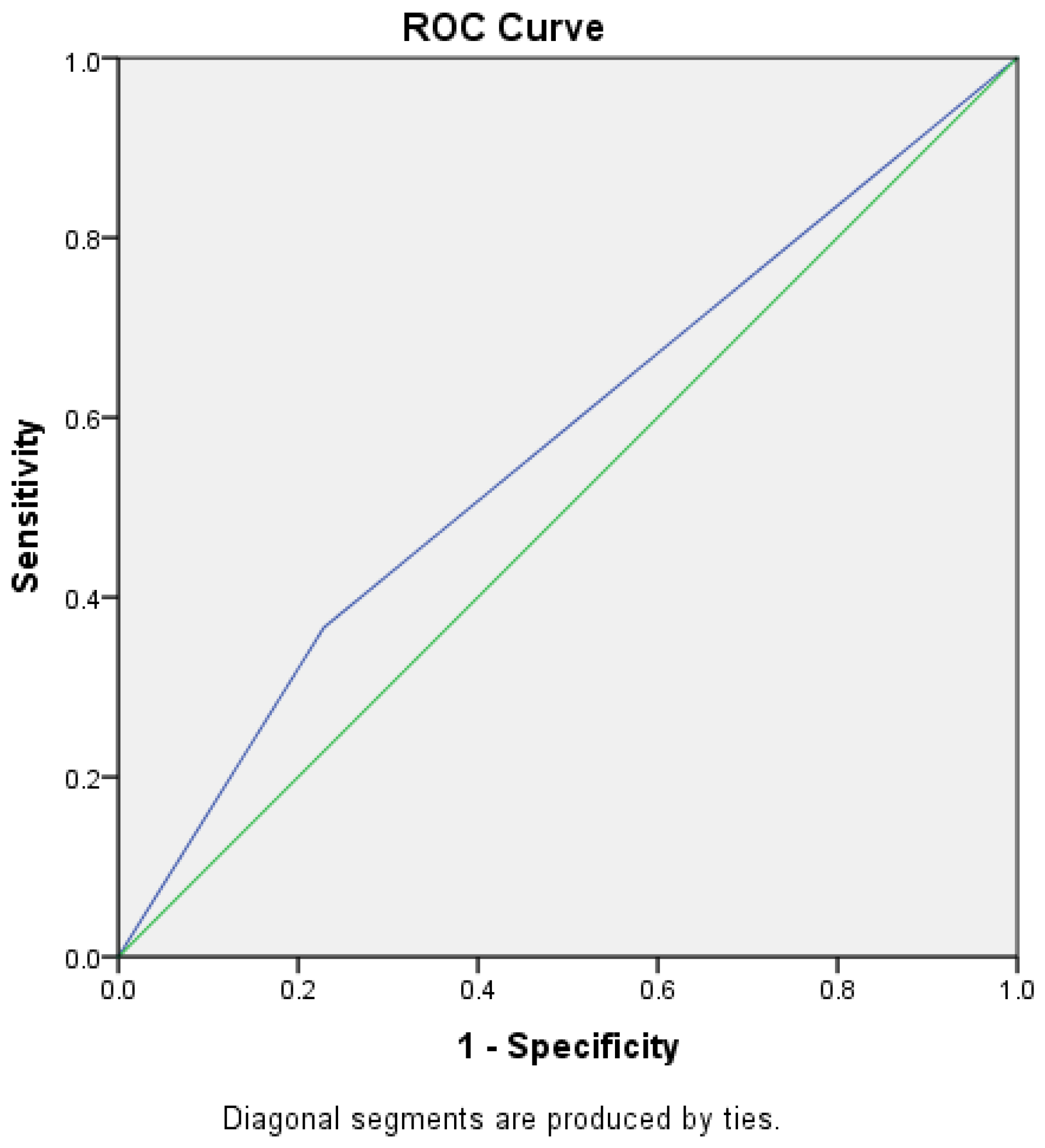
3.2. Sensitivity and Specificity of FeNO in Diagnosis of Mild Asthma
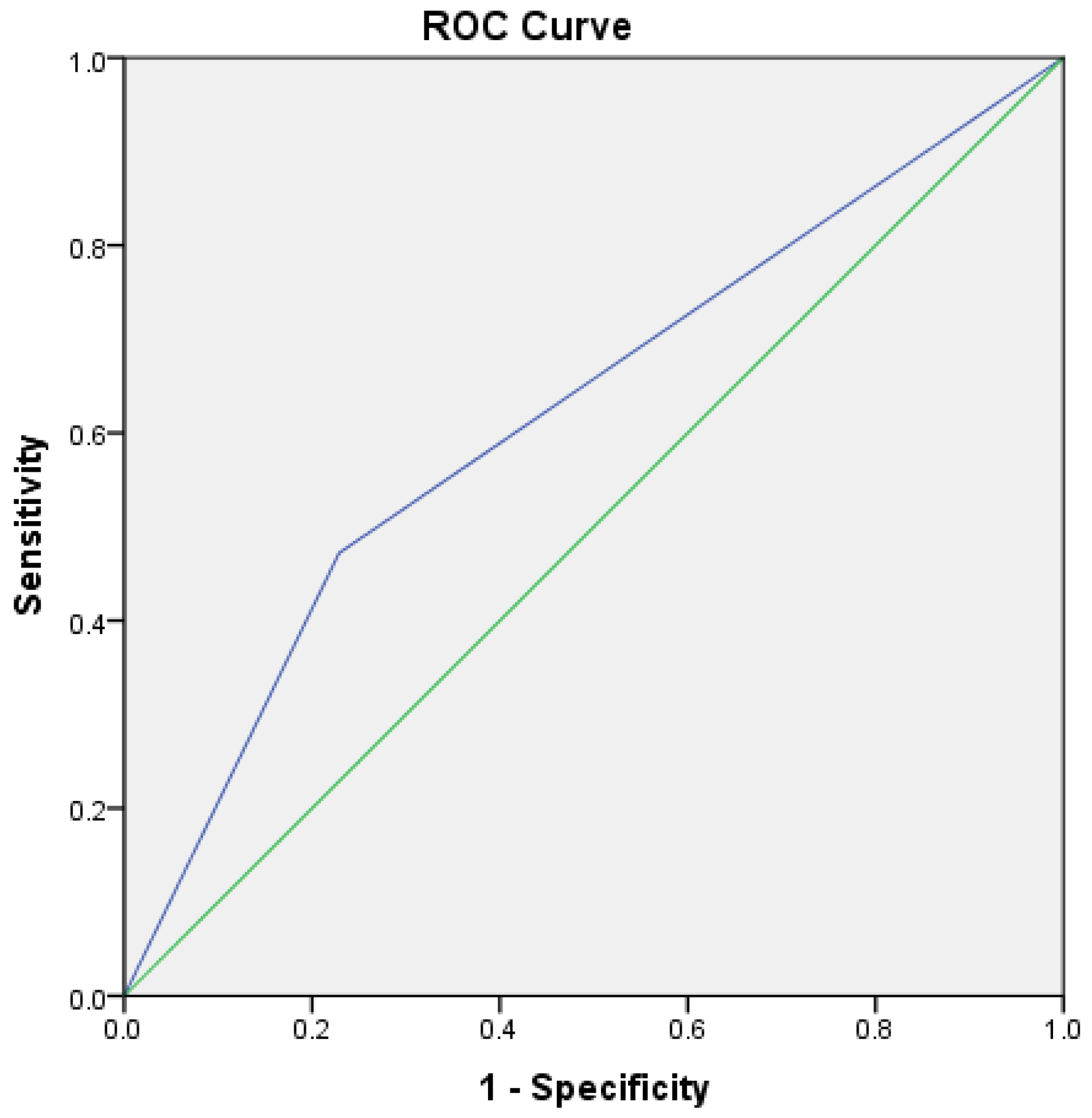
3.3. Sensitivity and Specificity of BPT in Diagnosis of Mild Asthma
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2015 Chronic Respiratory Disease Collaborators. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir. Med. 2017, 5, 691–706. [Google Scholar] [CrossRef] [Green Version]
- Loewenthal, L.; Menzies-Gow, A. FeNO in Asthma. Semin. Respir. Crit Care Med. 2022, 43, 635–645. [Google Scholar] [CrossRef]
- Aaron, S.D.; Vandemheen, K.L.; FitzGerald, J.M.; Ainslie, M.; Gupta, S.; Lemière, C.; Field, S.K.; McIvor, R.A.; Hernandez, P.; Mayers, I.; et al. Reevaluation of diagnosis in adults with physician-diagnosed asthma. JAMA 2017, 317, 269–279. [Google Scholar] [CrossRef]
- Dusser, D.; Montani, D.; Chanez, P.; de Blic, J.; Delacourt, C.; Deschildre, A.; Devillier, P.; Didier, A.; Leroyer, C.; Marguet, C.; et al. Mild asthma: An expert review on epidemiology, clinical characteristics and treatment recommendations. Allergy 2007, 62, 591–604. [Google Scholar] [CrossRef] [PubMed]
- Foucard, T.; Graff-Lonnevig, V. Asthma mortality rate in Swedish children and young adults 1973–88. Allergy 1994, 49, 616–619. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.J.; Campbell, D.A.; Gluyas, P.A.; Coates, J.R.; Ruffin, R.E.; Roder, D.M.; Latimer, K.M.; Luke, C.G.; Frith, P.A.; Yellowlees, P.M.; et al. Characteristics of near-fatal asthma in childhood. Pediatr Pulmonol. 1995, 20, 1–8. [Google Scholar] [CrossRef]
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. Updated 2022. Available online: https://ginasthma.org/gina-reports/URL (accessed on 13 March 2023).
- Goldstein, M.F.; Veza, B.A.; Dunsky, E.H.; Dvorin, D.J.; Belecanech, G.A.; Haralabatos, I.C. Comparisons of peak diurnal expiratory flow variation, postbronchodilator FEV(1) responses, and methacholine inhalation challenges in the evaluation of suspected asthma. Chest 2001, 119, 1001–1010. [Google Scholar] [CrossRef]
- Den Otter, J.J.; Reijnen, G.M.; van den Bosch, W.J.; van Schayck, C.P.; Molema, J.; van Weel, C. Testing bronchial hyper-responsiveness: Provocation or peak expiratory flow variability? Br. J. Gen. Pract. 1997, 47, 487–492. [Google Scholar]
- Cockcroft, D.W.; Davis, B.E. Mechanisms of airway hyperresponsiveness. J. Allergy Clin. Immunol. 2006, 118, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Irwin, R.S.; Baumann, M.H.; Bolser, D.C.; Boulet, L.P.; Braman, S.S.; Brightling, C.E.; Brown, K.K.; Canning, B.J.; Chang, A.B.; Dicpinigaitis, P.V.; et al. Diagnosis and management of cough executive summary: ACCP evidence-based clinical practice guidelines. Chest 2006, 129, 1S–23S. [Google Scholar] [CrossRef] [Green Version]
- Achilleos, A. Evidence-based evaluation and management of chronic cough. Med. Clin. N. Am. 2016, 100, 1033–1045. [Google Scholar] [CrossRef] [PubMed]
- Crapo, R.O.; Casaburi, R.; Coates, A.L.; Enright, P.L.; Hankinson, J.L.; Irvin, C.G.; MacIntyre, N.R.; McKay, R.T.; Wanger, J.S.; Anderson, S.D.; et al. Guidelines for methacholine and exercise challenge testing-1999. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, July 1999. Am. J. Respir. Crit. Care Med. 2000, 161, 309–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kharitonov, S.A.; Yates, D.; Robbins, R.A.; Logan-Sinclair, R.; Shinebourne, E.A.; Barnes, P.J. Increased nitric oxide in exhaled air of asthmatic patients. Lancet 1994, 343, 133–135. [Google Scholar] [CrossRef]
- Alving, K.; Weitzberg, E.; Lundberg, J.M. Increased amount of nitric oxide in exhaled air of asthmatics. Eur. Respir. J. 1993, 6, 1368–1370. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- Ranu, H.; Wilde, M.; Madden, B. Pulmonary function tests. Ulster Med. J. 2011, 80, 84–90. [Google Scholar]
- American Thoracic Society. Lung function testing: Selection of normal values and interpretive strategies. Am. Rev. Respir. Dis. 1991, 144, 1202–1218. [Google Scholar] [CrossRef]
- American Thoracic Society; European Respiratory Society. ATS/ERS recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide, 2005. Am. J. Respir. Crit. Care Med. 2005, 171, 912–930. [Google Scholar] [CrossRef] [Green Version]
- Dweik, R.A.; Boggs, P.B.; Erzurum, S.C.; Irvin, C.G.; Leigh, M.W.; Lundberg, J.O.; Olin, A.C.; Plummer, A.L.; Taylor, D.R. American Thoracic Society Committee on Interpretation of Exhaled Nitric Oxide Levels (FENO) for Clinical Applications. Am. J. Respir. Crit. Care Med. 2011, 184, 602–615. [Google Scholar] [CrossRef] [Green Version]
- Bao, W.; Zhang, X.; Yin, J.; Han, L.; Huang, Z.; Bao, L.; Lv, C.; Hao, H.; Xue, Y.; Zhou, X.; et al. Small-Airway Function Variables in Spirometry, Fractional Exhaled Nitric Oxide, and Circulating Eosinophils Predicted Airway Hyperresponsiveness in Patients with Mild Asthma. J. Asthma Allergy 2021, 14, 415–426. [Google Scholar] [CrossRef]
- Joyce, D.P.; Chapman, K.R.; Kesten, S. Prior diagnosis and treatment of patients with normal results of methacholine challenge and unexplained respiratory symptoms. Chest 1996, 109, 697–701. [Google Scholar] [CrossRef] [Green Version]
- Van Schayck, C.P.; van Der Heijden, F.M.; van Den Boom, G.; Tirimanna, P.R.; van Herwaarden, C.L. Underdiagnosis of asthma: Is the doctor or the patient to blame? The DIMCA project. Thorax 2000, 55, 562–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bai, J.; Peat, J.K.; Berry, G.; Marks, G.B.; Woolcock, A.J. Questionnaire items that predict asthma and other respiratory conditions in adults. Chest 1998, 114, 1343–1348. [Google Scholar] [CrossRef]
- Schneider, A.; Ay, M.; Faderl, B.; Linde, K.; Wagenpfeil, S. Diagnostic accuracy of clinical symptoms in obstructive airway diseases varied within different health care sectors. J. Clin. Epidemiol. 2012, 65, 846–854. [Google Scholar] [CrossRef]
- Appleton, S.L.; Adams, R.J.; Wilson, D.H.; Taylor, A.W.; Ruffin, R.E.; North West Adelaide Cohort Health Study Team. Spirometric criteria for asthma: Adding further evidence to the debate. J. Allergy Clin. Immunol. 2005, 116, 976–982. [Google Scholar] [CrossRef] [PubMed]
- Hunter, C.J.; Brightling, C.E.; Woltmann, G.; Wardlaw, A.J.; Pavord, I.D. A comparison of the validity of different diagnostic tests in adults with asthma. Chest 2002, 121, 1051–1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reddel, H.K.; Busse, W.W.; Pedersen, S.; Tan, W.C.; Chen, Y.Z.; Jorup, C.; Lythgoe, D.; O’Byrne, P.M. Should recommendations about starting inhaled corticosteroid treatment for mild asthma be based on symptom frequency: A post-hoc efficacy analysis of the START study. Lancet 2017, 389, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Selroos, O. Effect of disease duration on dose–response of inhaled budesonide in asthma. Respir. Med. 2008, 102, 1065–1072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enright, P.L.; Lebowitz, M.D.; Cockcroft, D.W. Physiologic measures: Pulmonary function tests. Am. J. Respir. Crit. Care Med. 1994, 149, S9–S18; discussion S19–S20. [Google Scholar] [CrossRef]
- Higgins, B.G.; Britton, J.R.; Chinn, S.; Jones, T.D.; Jenkinson, D.; Burney, P.G.; Tattersfield, A.E. The distribution of peak expiratory flow variability in a population sample. Am. Rev. Respir. Dis. 1989, 140, 1368–1372. [Google Scholar] [CrossRef]
- González-García, M.; Torres-Duque, C.A.; Bustos, A.; Jaramillo, C.; Maldonado, D. Bronchial hyperresponsiveness in women with chronic obstructive pulmonary disease related to wood smoke. Int. J. Chron. Obstruct. Pulmon. Dis. 2012, 7, 367–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aronsson, D.; Tufvesson, E.; Ankerst, J.; Bjermer, L. Allergic rhinitis with hyper-responsiveness differ from asthma in degree of peripheral obstruction during metacholine challenge test. Clin. Physiol. Funct. Imaging 2008, 28, 81–85. [Google Scholar] [CrossRef]
- Boulet, L.P. Asymptomatic airway hyperresponsiveness: A curiosity or an opportunity to prevent asthma? Am. J. Respir. Crit. Care Med. 2003, 167, 371–378. [Google Scholar] [CrossRef]
- Zheng, J. A nationwide questionnaire survey on clinical application of pulmonary function testing in China. Zhonghua Jiehe He Huxi Zazhi 2002, 25, 69–73. [Google Scholar]
- Munakata, M. Exhaled nitric oxide (FeNO) as a non-invasive marker of airway inflammation. Allergol. Int. 2012, 61, 365–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lloyd, C.M.; Snelgrove, R.J. Type 2 immunity: Expanding our view. Sci. Immunol. 2018, 3, eaat1604. [Google Scholar] [CrossRef] [Green Version]
- Lane, C.; Knight, D.; Burgess, S.; Franklin, P.; Horak, F.; Legg, J.; Moeller, A.; Stick, S. Epithelial inducible nitric oxide synthase activity is the major determinant of nitric oxide concentration in exhaled breath. Thorax 2004, 59, 757–760. [Google Scholar] [CrossRef] [Green Version]
- Kobzik, L.; Bredt, D.S.; Lowenstein, C.J.; Drazen, J.; Gaston, B.; Sugarbaker, D.; Stamler, J.S. Nitric oxide synthase in human and rat lung: Immunocytochemical and histochemical localization. Am. J. Respir. Cell Mol. Biol. 1993, 9, 371–377. [Google Scholar] [CrossRef]
- Ricciardolo, F.L.M. Multiple roles of nitric oxide in the airways. Thorax 2003, 58, 175–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papi, A.; Brightling, C.; Pedersen, S.E.; Reddel, H.K. Asthma. Lancet 2018, 391, 783–800. [Google Scholar] [CrossRef]
- Kulkarni, N.S.; Hollins, F.; Sutcliffe, A.; Saunders, R.; Shah, S.; Siddiqui, S.; Gupta, S.; Haldar, P.; Green, R.; Pavord, I.; et al. Eosinophil protein in airway macrophages: A novel biomarker of eosinophilic inflammation in patients with asthma. J. Allergy Clin. Immunol. 2010, 126, 61–69.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kowal, K.; Bodzenta-Lukaszyk, A.; Zukowski, S. Exhaled nitric oxide in evaluation of young adults with chronic cough. J. Asthma 2009, 46, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Sato, S.; Saito, J.; Sato, Y.; Ishii, T.; Xintao, W.; Tanino, Y.; Ishida, T.; Munakata, M. Clinical usefulness of fractional exhaled nitric oxide for diagnosing prolonged cough. Respir. Med. 2008, 102, 1452–1459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, A.D.; Cowan, J.O.; Filsell, S.; McLachlan, C.; Monti-Sheehan, G.; Jackson, P.; Taylor, D.R. Diagnosing asthma: Comparisons between exhaled nitric oxide measurements and conventional tests. Am. J. Respir. Crit. Care Med. 2004, 169, 473–478. [Google Scholar] [CrossRef]
- Louis, R.; Satia, I.; Ojanguren, I.; Schleich, F.; Bonini, M.; Tonia, T.; Rigau, D.; Ten Brinke, A.; Buhl, R.; Loukides, S.; et al. European Respiratory Society Guidelines for the Diagnosis of Asthma in Adults. Eur. Respir. J. 2022, 15, 2101585. [Google Scholar] [CrossRef]
- Schneider, A.; Schwarzbach, J.; Faderl, B.; Welker, L.; Karsch-Völk, M.; Jörres, R.A. FENO measurement and sputum analysis for diagnosing asthma in clinical practice. Respir. Med. 2013, 107, 209–216. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Asthma (n = 142) | Non-Asthma (n = 140) | p-Value | |
|---|---|---|---|
| Age (mean ± SD), year | 34.94 ± 13.81 | 36.25 ± 12.58 | 0.405 |
| BMI (mean ± SD), kg/m2 | 24.5 ± 4.31 | 25.02 ± 4.7 | 0.336 |
| Gender (male/female) | 57/83 | 43/99 | 0.088 |
| Smoker/non-smoker | 16/124 | 17/125 | 1.000 |
| Non-Asthma (n = 140) | Asthma (n = 142) | p-Value | |
|---|---|---|---|
| Basal FEV1 L (mean ± SD) | 3.68 ± 0.88 | 3.36 ± 0.78 | 0.001 |
| Basal FEV1% predicted, mean (range) | 102 (94–110) | 97 (92-107) | 0.015 |
| Post-BDT FEV1 L (mean ± SD) | 3.88 ± 0.92 | 3.59 ± 0.83 | 0.005 |
| Post-BDT FEV1% predicted (mean ± SD) | 105.84 ± 5.03 | 107.3 ± 5.8 | 0.025 |
| FeNO ppb, median (25–75 pct) | 23 (15–50) | 49.5 (25.5–81) | <0.001 |
| <25 ppb n (%) | 73 (52.14) | 35 (24.65) | |
| 25–50 ppb n (%) | 35 (25) | 39 (27.46) | |
| >50 ppb n (%) | 32 (22.86) | 68 (47.89) | <0.001 |
| Skin prick positive test n (%) | 83 (59.3) | 92 (64.79) | 0.407 |
| FeNO ppb median (25–75 pct) | 23 (15-50) | 49.5 (25.5–81) | <0.001 |
| <25 ppb n (%) | 73 (52.14) | 35 (24.65) | |
| 25–50 ppb n (%) | 35 (25) | 39 (27.46) | |
| >50 ppb n (%) | 32 (22.86) | 68 (47.89) | <0.001 |
| Skin prick positive test n (%) | 83 (59.3) | 92 (64.79) | 0.407 |
| FeNO ppb median (25–75 pct) | 23 (15–50) | 49.5 (25.5–81) | <0.001 |
| <25 ppb n (%) | 73 (52.14) | 35 (24.65) | |
| 25–50 ppb n (%) | 35 (25) | 39 (27.46) | |
| >50 ppb n (%) | 32 (22.86) | 68 (47.89) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karamarkovic Lazarusic, N.; Kasap Basioli, E.; Tolic, E.; Dokoza, M.; Pavlisa, G. Value of Fractional Exhaled Nitric Oxide in Diagnosing Mild Asthma Responsive to Inhaled Corticosteroids. J. Clin. Med. 2023, 12, 3330. https://doi.org/10.3390/jcm12093330
Karamarkovic Lazarusic N, Kasap Basioli E, Tolic E, Dokoza M, Pavlisa G. Value of Fractional Exhaled Nitric Oxide in Diagnosing Mild Asthma Responsive to Inhaled Corticosteroids. Journal of Clinical Medicine. 2023; 12(9):3330. https://doi.org/10.3390/jcm12093330
Chicago/Turabian StyleKaramarkovic Lazarusic, Natasa, Eugenija Kasap Basioli, Ena Tolic, Martina Dokoza, and Gordana Pavlisa. 2023. "Value of Fractional Exhaled Nitric Oxide in Diagnosing Mild Asthma Responsive to Inhaled Corticosteroids" Journal of Clinical Medicine 12, no. 9: 3330. https://doi.org/10.3390/jcm12093330