

Functional Mitral and Tricuspid Regurgitation across the Whole Spectrum of Left Ventricular Ejection Fraction: Recognizing the Elephant in the Room of Heart Failure
 ,
,
Abstract
:1. Introduction
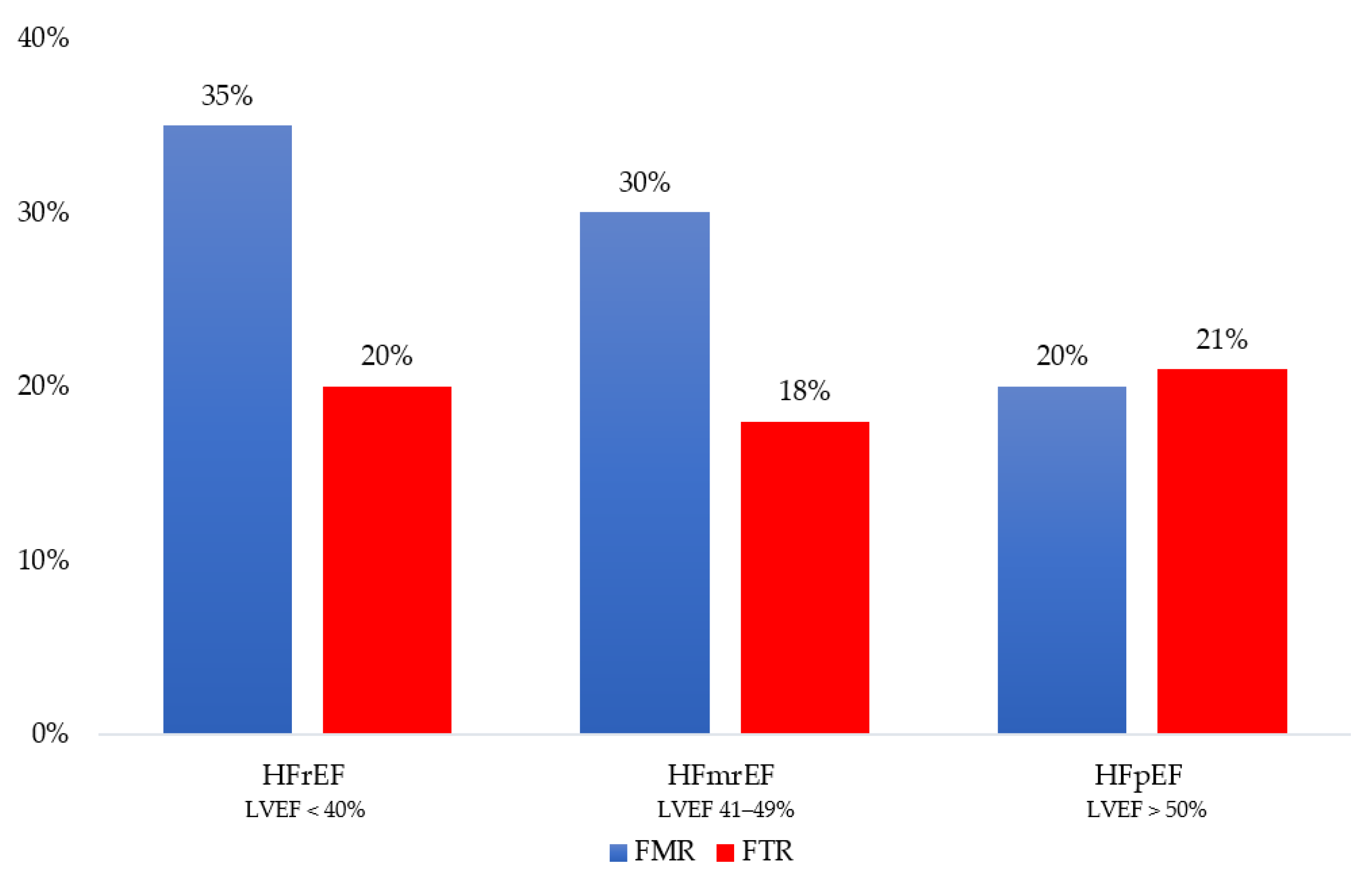
2. Epidemiology
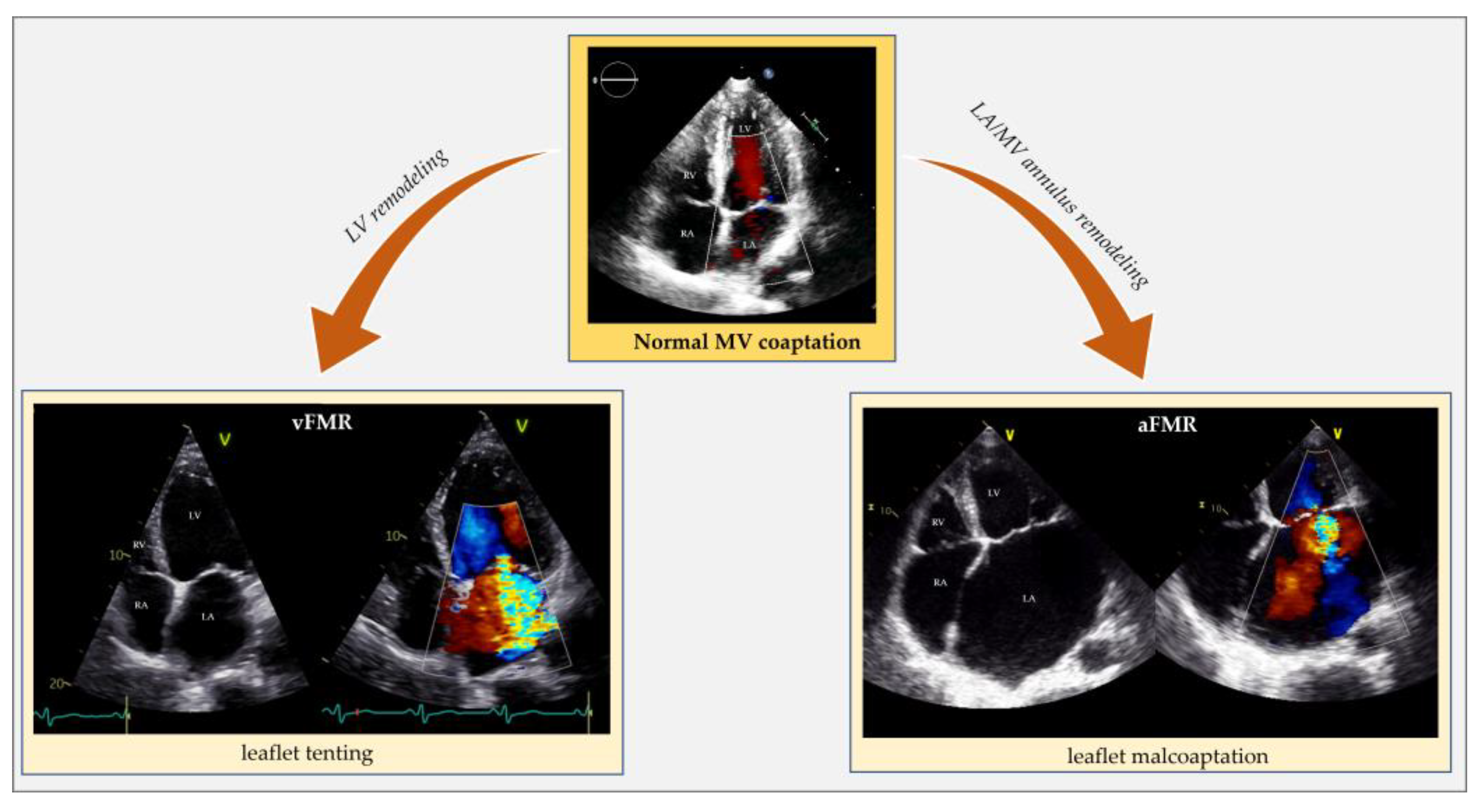
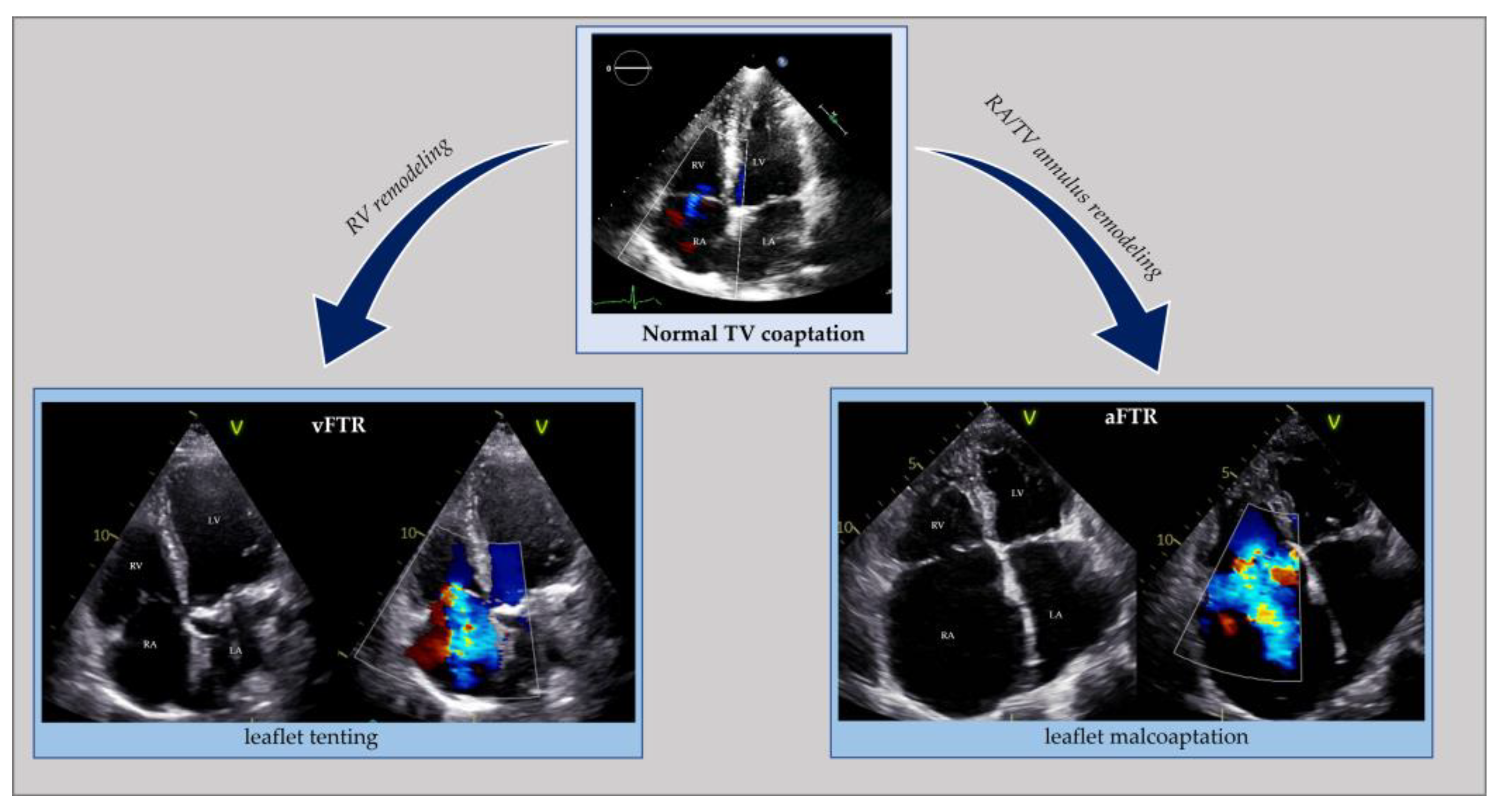
3. Pathophysiology and Prognosis
4. Therapeutic Implications
4.1. Functional Mitral Regurgitation
4.2. Functional Tricuspid Regurgitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kadri, A.N.; Gajulapalli, R.D.; Sammour, Y.M.; Chahine, J.; Nusairat, L.; Gad, M.M.; Al-Khadra, Y.; Hernandez, A.V.; Rader, F.; Harb, S.C.; et al. Impact of Tricuspid Regurgitation in Patients with Heart Failure and Mitral Valve Disease from a Nationwide Cohort Study. Am. J. Cardiol. 2019, 124, 926–931. [Google Scholar] [CrossRef] [PubMed]
- Goliasch, G.; Bartko, P.E.; Pavo, N.; Neuhold, S.; Wurm, R.; Mascherbauer, J.; Lang, I.M.; Strunk, G.; Hülsmann, M. Refining the prognostic impact of functional mitral regurgitation in chronic heart failure. Eur. Heart J. 2018, 39, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Bartko, P.E.; Arfsten, H.; Heitzinger, G.; Pavo, N.; Winter, M.-P.; Toma, A.; Strunk, G.; Hengstenberg, C.; Hülsmann, M.; Goliasch, G. Natural history of bivalvular functional regurgitation. Eur. Heart J.—Cardiovasc. Imaging 2018, 20, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Schlotter, F.; Dietz, M.F.; Stolz, L.; Kresoja, K.-P.; Besler, C.; Sannino, A.; Rommel, K.-P.; Unterhuber, M.; von Roeder, M.; Delgado, V.; et al. Atrial Functional Tricuspid Regurgitation: Novel Definition and Impact on Prognosis. Circ. Cardiovasc. Interv. 2022, 15, 011958. [Google Scholar] [CrossRef] [PubMed]
- Badano, L.P.; Muraru, D.; Enriquez-Sarano, M. Assessment of functional tricuspid regurgitation. Eur. Heart J. 2013, 34, 1875–1885. [Google Scholar] [CrossRef]
- Ennezat, P.V.; Maréchaux, S.; Pibarot, P.; Le Jemtel, T.H. Secondary Mitral Regurgitation in Heart Failure with Reduced or Preserved Left Ventricular Ejection Fraction. Cardiology 2013, 125, 110–117. [Google Scholar] [CrossRef]
- Hoit, B.D. Atrial Functional Mitral Regurgitation: The Left Atrium Gets its Due Respect. J. Am. Coll. Cardiol. 2011, 58, 1482–1484. [Google Scholar] [CrossRef]
- Chioncel, O.; Lainscak, M.; Seferovic, P.M.; Anker, S.D.; Crespo-Leiro, M.G.; Harjola, V.-P.; Parissis, J.; Laroche, C.; Piepoli, M.F.; Fonseca, C.; et al. Epidemiology and one-year outcomes in patients with chronic heart failure and preserved, mid-range and reduced ejection fraction: An analysis of the ESC Heart Failure Long-Term Registry. Eur. J. Heart Fail. 2017, 19, 1574–1585. [Google Scholar] [CrossRef]
- Bursi, F.; Barbieri, A.; Grigioni, F.; Reggianini, L.; Zanasi, V.; Leuzzi, C.; Ricci, C.; Piovaccari, G.; Branzi, A.; Modena, M.G. Prognostic implications of functional mitral regurgitation according to the severity of the underlying chronic heart failure: A long-term outcome study. Eur. J. Heart Fail. 2010, 12, 382–388. [Google Scholar] [CrossRef]
- Patel, J.B.; Borgeson, D.D.; E Barnes, M.; Rihal, C.S.; Daly, R.C.; Redfield, M.M. Mitral regurgitation in patients with advanced systolic heart failure. J. Card. Fail. 2004, 10, 285–291. [Google Scholar] [CrossRef]
- Grigioni, F.; Enriquez-Sarano, M.; Zehr, K.; Bailey, K.; Tajik, A. Ischemic mitral regurgitation. Long-term outcome and prognostic implications with quantitative Doppler assessment. Circulation 2001, 103, 1759–1764. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.; Dini, F.L.; Faggiano, P.; Agricola, E.; Cicoira, M.; Frattini, S.; Simioniuc, A.; Gullace, M.; Ghio, S.; Enriquez-Sarano, M.; et al. Independent prognostic value of functional mitral regurgitation in patients with heart failure. A quantitative analysis of 1256 patients with ischaemic and non-ischaemic dilated cardiomyopathy. Heart 2011, 97, 1675–1680. [Google Scholar] [CrossRef] [PubMed]
- D’Arcy, J.L.; Coffey, S.; Loudon, M.A.; Kennedy, A.; Pearson-Stuttard, J.; Birks, J.; Frangou, E.; Farmer, A.J.; Mant, D.; Wilson, J.; et al. Large-scale community echocardiographic screening reveals a major burden of undiagnosed valvular heart disease in older people: The OxVALVE Population Cohort Study. Eur. Heart J. 2016, 37, 3515–3522. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.P.; Evans, J.C.; Levy, D.; Larson, M.G.; A Freed, L.; Fuller, D.L.; Lehman, B.; Benjamin, E.J. Prevalence and clinical determinants of mitral, tricuspid, and aortic regurgitation (the Framingham Heart Study). Am. J. Cardiol. 1999, 83, 897–902. [Google Scholar] [CrossRef]
- Topilsky, Y.; Maltais, S.; Medina-Inojosa, J.; Oguz, D.; Michelena, H.; Maalouf, J.; Mahoney, D.W.; Enriquez-Sarano, M. Burden of Tricuspid Regurgitation in Patients Diagnosed in the Community Setting. JACC Cardiovasc. Imaging 2019, 12, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Benfari, G.; Antoine, C.; Miller, W.L.; Thapa, P.; Topilsky, Y.; Rossi, A.; Michelena, H.I.; Pislaru, S.; Enriquez-Sarano, M. Excess Mortality Associated with Functional Tricuspid Regurgitation Complicating Heart Failure with Reduced Ejection Fraction. Circulation 2019, 140, 196–206. [Google Scholar] [CrossRef]
- Chorin, E.; Rozenbaum, Z.; Topilsky, Y.; Konigstein, M.; Ziv-Baran, T.; Richert, E.; Keren, G.; Banai, S. Tricuspid regurgitation and long-term clinical outcomes. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 157–165. [Google Scholar] [CrossRef]
- E Bartko, P.; Hülsmann, M.; Hung, J.; Pavo, N.; A Levine, R.; Pibarot, P.; Vahanian, A.; Stone, G.W.; Goliasch, G. Secondary valve regurgitation in patients with heart failure with preserved ejection fraction, heart failure with mid-range ejection fraction, and heart failure with reduced ejection fraction. Eur. Heart J. 2020, 41, 2799–2810. [Google Scholar] [CrossRef]
- Deferm, S.; Bertrand, P.B.; Verbrugge, F.H.; Verhaert, D.; Rega, F.; Thomas, J.D.; Vandervoort, P.M. Atrial Functional Mitral Regurgitation: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 73, 2465–2476. [Google Scholar] [CrossRef]
- Magne, J.; Sénéchal, M.; Dumesnil, J.G.; Pibarot, P. Ischemic Mitral Regurgitation: A Complex Multifaceted Disease. Cardiology 2009, 112, 244–259. [Google Scholar] [CrossRef]
- Lancellotti, P.; Moura, L.; Pierard, L.A.; Agricola, E.; Popescu, B.A.; Tribouilloy, C.; Hagendorff, A.; Monin, J.-L.; Badano, L.; Zamorano, J.L.; et al. European Association of Echocardiography recommendations for the assessment of valvular regurgitation. Part 2: Mitral and tricuspid regurgitation (native valve disease). Eur. Heart J.—Cardiovasc. Imaging 2010, 11, 307–332. [Google Scholar] [CrossRef] [PubMed]
- Kajimoto, K.; Sato, N.; Takano, T.; on behalf of the investigators of the Acute Decompensated Heart Failure Syndromes (ATTEND) registry. Functional mitral regurgitation at discharge and outcomes in patients hospitalized for acute decompensated heart failure with a preserved or reduced ejection fraction. Eur. J. Heart Fail. 2016, 18, 1051–1059. [Google Scholar] [CrossRef] [PubMed]
- Benfari, G.; Antoine, C.; Essayagh, B.; Batista, R.; Maalouf, J.; Rossi, A.; Grigioni, F.; Thapa, P.; Michelena, H.I.; Enriquez-Sarano, M. Functional Mitral Regurgitation Outcome and Grading in Heart Failure With Reduced Ejection Fraction. JACC Cardiovasc. Imaging 2021, 14, 2303–2315. [Google Scholar] [CrossRef] [PubMed]
- Dziadzko, V.; Dziadzko, M.; Medina-Inojosa, J.R.; Benfari, G.; Michelena, H.I.; Crestanello, J.A.; Maalouf, J.; Thapa, P.; Enriquez-Sarano, M. Causes and Mechanisms of Isolated Mitral Regurgitation in the Community: Clinical Context and Outcome. Eur. Heart J. 2019, 40, 2194–2202. [Google Scholar] [CrossRef]
- Gertz, Z.M.; Raina, A.; Saghy, L.; Zado, E.S.; Callans, D.J.; Marchlinski, F.E.; Keane, M.G.; Silvestry, F.E. Evidence of Atrial Functional Mitral Regurgitation Due to Atrial Fibrillation: Reversal With Arrhythmia Control. J. Am. Coll. Cardiol. 2011, 58, 1474–1481. [Google Scholar] [CrossRef]
- Mesi, O.; Gad, M.M.; Crane, A.D.; Ramchand, J.; Puri, R.; Layoun, H.; Miyasaka, R.; Gillinov, M.A.; Wierup, P.; Griffin, B.P.; et al. Severe Atrial Functional Mitral Regurgitation: Clinical and Echocardiographic Characteristics, Management and Outcomes. JACC Cardiovasc. Imaging 2021, 14, 797–808. [Google Scholar] [CrossRef]
- Redfield, M.M.; Jacobsen, S.J.; Borlaug, B.A.; Rodeheffer, R.J.; Kass, D.A. Age- and Gender-Related Ventricular-Vascular Stiffening: A Community-Based Study. Circulation 2005, 112, 2254–2262. [Google Scholar] [CrossRef]
- Lam, C.S.P.; Roger, V.L.; Rodeheffer, R.J.; Bursi, F.; Borlaug, B.A.; Ommen, S.R.; Kass, D.A.; Redfield, M.M. Cardiac Structure and Ventricular–Vascular Function in Persons with Heart Failure and Preserved Ejection Fraction From Olmsted County, Minnesota. Circulation 2007, 115, 1982–1990. [Google Scholar] [CrossRef]
- Kawaguchi, M.; Hay, I.; Fetics, B.; Kass, D.A. Combined Ventricular Systolic and Arterial Stiffening in Patients with Heart Failure and Preserved Ejection Fraction: Implications for Systolic and Diastolic Reserve Limitations. Circulation 2003, 107, 714–720. [Google Scholar] [CrossRef]
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C., Jr.; Ellinor, P.T., Jr.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients with Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration with the Society of Thoracic Surgeons. Circulation 2019, 140, E28. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation Developed in Collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the Diagnosis and Management of Atrial Fibrillation of the European Society of Cardiology (ESC) Developed with the Special Contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 4194. [Google Scholar] [PubMed]
- Manning, W.J.; Silverman, D.I.; Katz, S.E.; Riley, M.F.; Come, P.C.; Doherty, R.M.; Munson, J.T.; Douglas, P.S. Impaired left atrial mechanical function after cardioversion: Relation to the duration of atrial fibrillation. J. Am. Coll. Cardiol. 1994, 23, 1535–1540. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, C.; Okada, A.; Nishimura, K.; Moriuchi, K.; Amano, M.; Takahama, H.; Amaki, M.; Hasegawa, T.; Kanzaki, H.; Fujita, T.; et al. Prognostic comparison of atrial and ventricular functional mitral regurgitation. Open Heart 2021, 8, e001574. [Google Scholar] [CrossRef] [PubMed]
- Enriquez-Sarano, M.; Benfari, G.; Messika-Zeitoun, D.; Grigioni, F.; Michelena, H.I. Functional mitral regurgitation: A proportionate or disproportionate focus of attention? Eur. J. Heart Fail. 2021, 23, 1759–1762. [Google Scholar] [CrossRef]
- Guta, A.C.; Badano, L.P.; Tomaselli, M.; Mihalcea, D.; Bartos, D.; Parati, G.; Muraru, D. The Pathophysiological Link between Right Atrial Remodeling and Functional Tricuspid Regurgitation in Patients with Atrial Fibrillation: A Three-Dimensional Echocardiography Study. J. Am. Soc. Echocardiogr. 2021, 34, 585–594.e1. [Google Scholar] [CrossRef]
- Muraru, D.; Addetia, K.; Guta, A.C.; Ochoa-Jimenez, R.C.; Genovese, D.; Veronesi, F.; Basso, C.; Iliceto, S.; Badano, L.P.; Lang, R.M. Right atrial volume is a major determinant of tricuspid annulus area in functional tricuspid regurgitation: A three-dimensional echocardiographic study. Eur. Heart J.—Cardiovasc. Imaging 2020, 22, 660–669. [Google Scholar] [CrossRef]
- Hahn, R.T.; Badano, L.P.; Bartko, P.E.; Muraru, D.; Maisano, F.; Zamorano, J.L.; Donal, E. Tricuspid regurgitation: Recent advances in understanding pathophysiology, severity grading and outcome. Eur. Heart J.—Cardiovasc. Imaging 2022, 23, 913–929. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2021, 77, 450–500. [Google Scholar] [CrossRef]
- Fagot, J.; Lavie-Badie, Y.; Blanchard, V.; Fournier, P.; Galinier, M.; Carrié, D.; Lairez, O.; Cariou, E.; Alric, L.; Bureau, C.; et al. Impact of tricuspid regurgitation on survival in patients with cardiac amyloidosis. ESC Heart Fail. 2021, 8, 438–446. [Google Scholar] [CrossRef]
- Nusca, A.; Cammalleri, V.; Carpenito, M.; Bono, M.C.; Mega, S.; Grigioni, F.; Ussia, G.P. Percutaneous Repair of Atrial Functional Tricuspid Regurgitation in Cardiac Amyloidosis: Combining Linear with Lateral Thinking. JACC Case Rep. 2023, 5, 101685. [Google Scholar] [CrossRef]
- Mascherbauer, J.; Kammerlander, A.A.; Zotter-Tufaro, C.; Aschauer, S.; Duca, F.; Dalos, D.; Winkler, S.; Schneider, M.; Bergler-Klein, J.; Bonderman, D. Presence of ´isolated´ tricuspid regurgitation should prompt the suspicion of heart failure with preserved ejection fraction. PLoS ONE 2017, 12, e0171542. [Google Scholar] [CrossRef]
- Fender, E.A.; Petrescu, I.; Ionescu, F.; Zack, C.J.; Pislaru, S.V.; Nkomo, V.T.; Cochuyt, J.J.; Hodge, D.O.; Nishimura, R.A. Prognostic Importance and Predictors of Survival in Isolated Tricuspid Regurgitation: A Growing Problem. Mayo Clin. Proc. 2019, 94, 2032–2039. [Google Scholar] [CrossRef] [PubMed]
- Ren, Q.; Li, X.; Fang, J.; Chen, Y.; Wu, M.; Yu, Y.; Liao, S.; Tse, H.; Yiu, K. The prevalence, predictors, and prognosis of tricuspid regurgitation in stage B and C heart failure with preserved ejection fraction. ESC Heart Fail. 2020, 7, 4051–4060. [Google Scholar] [CrossRef] [PubMed]
- Topilsky, Y.; Nkomo, V.T.; Vatury, O.; Michelena, H.I.; Letourneau, T.; Suri, R.M.; Pislaru, S.; Park, S.; Mahoney, D.W.; Biner, S.; et al. Clinical Outcome of Isolated Tricuspid Regurgitation. JACC: Cardiovasc. Imaging 2014, 7, 1185–1194. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.; L’official, G.; Guérin, A.; Dreyfus, J.; Lavie-Badie, Y.; Sportouch, C.; Eicher, J.-C.; Maréchaux, S.; Le Tourneau, T.; Oger, E.; et al. Natural history of functional tricuspid regurgitation: Impact of cardiac output. Eur. Heart J.—Cardiovasc. Imaging 2021, 22, 878–885. [Google Scholar] [CrossRef]
- Hell, M.M.; Emrich, T.; Kreidel, F.; Kreitner, K.-F.; Schoepf, U.J.; Münzel, T.; von Bardeleben, R.S. Computed tomography imaging needs for novel transcatheter tricuspid valve repair and replacement therapies. Eur. Heart J.—Cardiovasc. Imaging 2020, 22, 601–610. [Google Scholar] [CrossRef]
- Bartko, P.E.; Arfsten, H.; Frey, M.; Heitzinger, G.; Pavo, N.; Cho, A.N.N.A.; Neuhold, S.; Tan, T.; Strunk, G.; Hengstenberg, C.; et al. 5937Natural history of functional tricuspid regurgitation: Implications of quantitative doppler assessment. JACC Cardiovasc. Imaging 2019, 12, 389–397. [Google Scholar] [CrossRef]
- Santas, E.; Chorro, F.J.; Miñana, G.; Méndez, J.; Muñoz, J.; Escribano, D.; García-Blas, S.; Valero, E.; Bodí, V.; Núñez, E.; et al. Tricuspid Regurgitation and Mortality Risk Across Left Ventricular Systolic Function in Acute Heart Failure. Circ. J. 2015, 79, 1526–1533. [Google Scholar] [CrossRef]
- Topilsky, Y.; Inojosa, J.M.; Benfari, G.; Vaturi, O.; Maltais, S.; Michelena, H.; Mankad, S.; Enriquez-Sarano, M. Clinical presentation and outcome of tricuspid regurgitation in patients with systolic dysfunction. Eur. Heart J. 2018, 39, 3584–3592. [Google Scholar] [CrossRef]
- Gavazzoni, M.; Heilbron, F.; Badano, L.P.; Radu, N.; Cascella, A.; Tomaselli, M.; Perelli, F.; Caravita, S.; Baratto, C.; Parati, G.; et al. The atrial secondary tricuspid regurgitation is associated to more favorable outcome than the ventricular phenotype. Front. Cardiovasc. Med. 2022, 9, 1022755. [Google Scholar] [CrossRef]
- Dietz, M.F.; Prihadi, E.A.; van der Bijl, P.; Goedemans, L.; Mertens, B.J.; Gursoy, E.; van Genderen, O.S.; Marsan, N.A.; Delgado, V.; Bax, J.J. Prognostic Implications of Right Ventricular Remodeling and Function in Patients with Significant Secondary Tricuspid Regurgitation. Circulation 2019, 140, 836–845. [Google Scholar] [CrossRef] [PubMed]
- Itelman, E.; Vatury, O.; Kuperstein, R.; Ben-Zekry, S.; Hay, I.; Fefer, P.; Barbash, I.; Klempfner, R.; Segev, A.; Feinberg, M.; et al. The Association of Severe Tricuspid Regurgitation with Poor Survival Is Modified by Right Ventricular Pressure and Function: Insights from SHEBAHEART Big Data. J. Am. Soc. Echocardiogr. 2022, 35, 1028–1036. [Google Scholar] [CrossRef] [PubMed]
- Masuda, M.; Sekiya, K.; Asai, M.; Iida, O.; Okamoto, S.; Ishihara, T.; Nanto, K.; Kanda, T.; Tsujimura, T.; Matsuda, Y.; et al. Influence of catheter ablation for atrial fibrillation on atrial and ventricular functional mitral regurgitation. ESC Heart Fail. 2022, 9, 1901–1913. [Google Scholar] [CrossRef] [PubMed]
- Coats, A.J.S.; Anker, S.D.; Baumbach, A.; Alfieri, O.; von Bardeleben, R.S.; Bauersachs, J.; Bax, J.J.; Boveda, S.; Čelutkienė, J.; Cleland, J.G.; et al. The management of secondary mitral regurgitation in patients with heart failure: A joint position statement from the Heart Failure Association (HFA), European Association of Cardiovascular Imaging (EACVI), European Heart Rhythm Association (EHRA), and European Association of Percutaneous Cardiovascular Interventions (EAPCI) of the ESC. Eur. Heart J. 2021, 42, 1254–1269. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 146, E185. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. Corrigendum to: 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 4901. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef]
- Bartko, P.E.; Arfsten, H.; Heitzinger, G.; Pavo, N.; Strunk, G.; Gwechenberger, M.; Hengstenberg, C.; Binder, T.; Hulsmann, M.; Goliasch, G. Papillary Muscle Dyssynchrony-Mediated Functional Mitral Regurgitation: Mechanistic Insights and Modulation by Cardiac Resynchronization. JACC Cardiovasc. Imaging 2019, 12, 1728–1737. [Google Scholar] [CrossRef]
- Onishi, T.; Onishi, T.; Marek, J.J.; Ahmed, M.; Haberman, S.C.; Oyenuga, O.; Adelstein, E.; Schwartzman, D.; Saba, S.; Gorcsan, J. 3rd. Mechanistic features associated with improvement in mitral regurgitation after cardiac resynchronization therapy and their relation to long-term patient outcome. Circ. Heart Fail. 2013, 6, 685–693. [Google Scholar] [CrossRef]
- Van Der Bijl, P.; Vo, N.M.; Leung, M.; Ajmone Marsan, N.; Delgado, V.; Stone, G.W.; Bax, J.J. Impact of Atrial Fibrillation on Improvement of Functional Mitral Regurgitation in Cardiac Resynchronization Therapy. Heart Rhythm. 2018, 15, 1816–1822. [Google Scholar] [CrossRef]
- Dell’Era, G.; Rondano, E.; Franchi, E.; Marino, P. Atrial asynchrony and function before and after electrical cardioversion for persistent atrial fibrillation. Eur. J. Echocardiogr. 2010, 11, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Kihara, T.; Gillinov, A.M.; Takasaki, K.; Fukuda, S.; Song, J.-M.; Shiota, M.; Shiota, T. Mitral Regurgitation Associated with Mitral Annular Dilation in Patients with Lone Atrial Fibrillation: An Echocardiographic Study. Echocardiography 2009, 26, 885–889. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, Y.; Abe, Y.; Sasaki, Y.; Bito, Y.; Morisaki, A.; Nishimura, S.; Shibata, T. Mitral valve repair for atrial functional mitral regurgitation in patients with chronic atrial fibrillation. Interact. Cardiovasc. Thorac. Surg. 2015, 21, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Yousef, S.; Arnaoutakis, G.J.; Gada, H.; Smith, A.J.C.; Sanon, S.; Sultan, I. Transcatheter mitral valve therapies: State of the art. J. Card. Surg. 2021, 37, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Cammalleri, V.; Mega, S.; Ussia, G.P.; Grigioni, F. Mitral and Tricuspid Valves Percutaneous Repair in Patients with Advanced Heart Failure: Panacea, or Pandora’s Box? Heart Fail. Clin. 2021, 17, 607–618. [Google Scholar] [CrossRef]
- Stone, G.W.; Lindenfeld, J.; Abraham, W.T.; Kar, S.; Lim, D.S.; Mishell, J.M.; Whisenant, B.; Grayburn, P.A.; Rinaldi, M.; Kapadia, S.R.; et al. Transcatheter Mitral-Valve Repair in Patients with Heart Failure. N. Engl. J. Med. 2018, 379, 2307–2318. [Google Scholar] [CrossRef]
- Obadia, J.-F.; Messika-Zeitoun, D.; Leurent, G.; Iung, B.; Bonnet, G.; Piriou, N.; Lefèvre, T.; Piot, C.; Rouleau, F.; Carrié, D.; et al. Percutaneous Repair or Medical Treatment for Secondary Mitral Regurgitation. N. Engl. J. Med. 2018, 379, 2297–2306. [Google Scholar] [CrossRef]
- Grayburn, P.A.; Sannino, A.; Packer, M. Proportionate and disproportionate functional mitral regurgitation: A new conceptual framework that reconciles the results of the MITRA-FR and COAPT trials. JACC Cardiovasc. Imaging 2019, 12, 353–362. [Google Scholar] [CrossRef]
- Hagendorff, A.; Doenst, T.; Falk, V. Echocardiographic assessment of functional mitral regurgitation: Opening Pandora’s box? ESC Heart Fail. 2019, 6, 678–685. [Google Scholar] [CrossRef]
- Szerlip, M.; Spargias, K.S.; Makkar, R.; Kar, S.; Kipperman, R.M.; O’neill, W.W.; Ng, M.K.; Smith, R.L.; Fam, N.P.; Rinaldi, M.J.; et al. 2-Year Outcomes for Transcatheter Repair in Patients with Mitral Regurgitation From the CLASP Study. JACC Cardiovasc. Interv. 2021, 14, 1538–1548. [Google Scholar] [CrossRef]
- Gertz, Z.M.; Herrmann, H.C.; Lim, D.S.; Kar, S.; Kapadia, S.R.; Reed, G.W.; Puri, R.; Krishnaswamy, A.; Gersh, B.J.; Weissman, N.J.; et al. Implications of Atrial Fibrillation on the Mechanisms of Mitral Regurgitation and Response to MitraClip in the COAPT Trial. Circ. Cardiovasc. Interv. 2021, 14, E010300. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Sugiura, A.; Öztürk, C.; Vogelhuber, J.; Tabata, N.; Wilde, N.; Zimmer, S.; Nickenig, G.; Weber, M. Transcatheter Edge-to-Edge Repair for Atrial Secondary Mitral Regurgitation. JACC Cardiovasc. Interv. 2022, 15, 1731–1740. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.-H.; Makar, M.; Kar, S.; Chakravarty, T.; Oakley, L.; Sekhon, N.; Koseki, K.; Nakamura, M.; Hamilton, M.; Patel, J.K.; et al. Outcomes After Transcatheter Edge-to-Edge Mitral Valve Repair According to Mitral Regurgitation Etiology and Cardiac Remodeling. J. Am. Coll. Cardiol. Interv. 2022, 15, 1711–1722. [Google Scholar] [CrossRef]
- Sodhi, N.; Asch, F.M.; Ruf, T.; Petrescu, A.; von Bardeleben, S.; Lim, D.S.; Maisano, F.; Kar, S.; Price, M.J. Clinical Outcomes with Transcatheter Edge-to-Edge Repair in Atrial Functional MR From the EXPAND Study. JACC Cardiovasc. Interv. 2022, 15, 1723–1730. [Google Scholar] [CrossRef] [PubMed]
- Schofer, J.; Siminiak, T.; Haude, M.; Herrman, J.P.; Vainer, J.; Wu, J.C.; Levy, W.C.; Mauri, L.; Feldman, T.; Kwong, R.Y.; et al. Percutaneous Mitral Annuloplasty for Functional Mitral Regurgitation: Results of the CARILLON Mitral Annuloplasty Device European Union Study. Circulation 2009, 120, 326–333. [Google Scholar] [CrossRef]
- Nickenig, G.; Hammerstingl, C.; Schueler, R.; Topilsky, Y.; Grayburn, P.A.; Vahanian, A.; Messika-Zeitoun, D.; Urena Alcazar, M.; Baldus, S.; Volker, R.; et al. Transcatheter Mitral Annuloplasty in Chronic Functional Mitral Regurgitation: 6-Month Results with the Cardioband Percutaneous Mitral Repair System. JACC Cardiovasc. Interv. 2016, 9, 2039–2047. [Google Scholar] [CrossRef]
- Gooley, R.P.; Meredith, I.T. The Accucinch transcatheter direct mitral valve annuloplasty system. Eurointervention 2015, 11, W60–W61. [Google Scholar] [CrossRef]
- Houston, B.A.; Brittain, E.L.; Tedford, R.J. Right Ventricular Failure. N. Engl. J. Med. 2023, 388, 1111–1125. [Google Scholar] [CrossRef]
- McCarthy, P.M.; Bhudia, S.K.; Rajeswaran, J.; Hoercher, K.J.; Lytle, B.W.; Cosgrove, D.M.; Blackstone, E.H. Tricuspid valve repair: Durability and risk factors for failure. J. Thorac. Cardiovasc. Surg. 2004, 127, 674–685. [Google Scholar] [CrossRef]
- Fukuda, S.; Song, J.-M.; Gillinov, A.M.; McCarthy, P.M.; Daimon, M.; Kongsaerepong, V.; Thomas, J.D.; Shiota, T. Tricuspid Valve Tethering Predicts Residual Tricuspid Regurgitation after Tricuspid Annuloplasty. Circulation 2005, 111, 975–979. [Google Scholar] [CrossRef]
- Zack, C.J.; Fender, E.A.; Chandrashekar, P.; Reddy, Y.N.; Bennett, C.E.; Stulak, J.M.; Miller, V.M.; Nishimura, R.A. National Trends and Outcomes in Isolated Tricuspid Valve Surgery. J. Am. Coll. Cardiol. 2017, 70, 2953–2960. [Google Scholar] [CrossRef] [PubMed]
- Cammalleri, V.; Carpenito, M.; Bono, M.C.; Mega, S.; Ussia, G.P.; Grigioni, F. Transcatheter Tricuspid Valve Therapy: From Anatomy to Intervention. Front. Cardiovasc. Med. 2021, 8, 778445. [Google Scholar] [CrossRef] [PubMed]
- Praz, F.; Muraru, D.; Kreidel, F.; Lurz, P.; Hahn, R.T.; Delgado, V.; Senni, M.; von Bardeleben, R.S.; Nickenig, G.; Hausleiter, J.; et al. Transcatheter treatment for tricuspid valve disease. Eurointervention 2021, 17, 791–808. [Google Scholar] [CrossRef] [PubMed]
- Taramasso, M.; Alessandrini, H.; Latib, A.; Asami, M.; Attinger-Toller, A.; Biasco, L.; Braun, D.; Brochet, E.; Connelly, K.A.; Denti, P.; et al. Outcomes after Current Transcatheter Tricuspid Valve Intervention: Mid-Term Results from the International Trivalve Registry. JACC Cardiovasc. Interv. 2019, 12, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Taramasso, M.; Benfari, G.; van Der Bijl, P.; Alessandrini, H.; Attinger-Toller, A.; Biasco, L.; Lurz, P.; Braun, D.; Brochet, E.; Connelly, K.A.; et al. Transcatheter versus Medical Treatment of Symptomatic Severe Tricuspid Regurgitation. J. Am. Coll. Cardiol. 2019, 74, 2998–3008. [Google Scholar] [CrossRef] [PubMed]
- Nickenig, G.; Weber, M.; Schüler, R.; Hausleiter, J.; Nabauer, M.; von Bardeleben, R.S.; Sotiriou, E.; Schäfer, U.; Deuschl, F.; Alessandrini, H.; et al. Tricuspid valve repair with the Cardioband system: Two-year outcomes of the multicentre, prospective TRI-REPAIR study. Eurointervention 2021, 16, e1264–e1271. [Google Scholar] [CrossRef]
- Tanaka, T.; Sugiura, A.; Kavsur, R.; Vogelhuber, J.; Öztürk, C.; Becher, M.U.; Zimmer, S.; Nickenig, G.; Weber, M. Leaflet-to-annulus index and residual tricuspid regurgitation following tricuspid transcatheter edge-to-edge repair. Eurointervention 2022, 18, e169–e178. [Google Scholar] [CrossRef]
- Carpenito, M.; Cammalleri, V.; Vitez, L.; De Filippis, A.; Nobile, E.; Bono, M.C.; Mega, S.; Bunc, M.; Grigioni, F.; Ussia, G.P. Edge-to-Edge Repair for Tricuspid Valve Regurgitation. Preliminary Echo-Data and Clinical Implications from the Tricuspid Regurgitation IMAging (TRIMA) Study. J. Clin. Med. 2022, 11, 5609. [Google Scholar] [CrossRef]
- Webb, J.G.; Chuang, A.M.; Meier, D.; von Bardeleben, R.S.; Kodali, S.K.; Smith, R.L.; Hausleiter, J.; Ong, G.; Boone, R.; Ruf, T.; et al. Transcatheter Tricuspid Valve Replacement with the EVOQUE System: 1-Year Outcomes of a Multicenter, First-in-Human Experience. JACC Cardiovasc. Interv. 2022, 15, 481–491. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Intervention | Target Structure | Device | Description | Eligibility Criteria |
|---|---|---|---|---|
| Edge-to-edge | Mitral leaflets | MitraClip (Abbott Vascular, Abbott Park, IL, USA) PASCAL (Edwards Lifesciences, Irvine, CA, USA) | Based on edge-to-edge technique Transfemoral transeptal approach Approved for FMR and DMR | Central A2-P2 (ideal) No calcification Mean gradient < 4 mmHg MVA > 3 cm2 Sufficient leaflet tissue for grasping |
| Direct Annuloplasty | Mitral annulus | Cardioband (Edwards Lifesciences, Irvine, CA, USA) | Implantation of a flexible ring into the posterior annulus Ideal for annular dilatation mainly due to LA enlargement (atrial FMR) Anchoring on the hinge of the annulus Transfemoral transeptal approach | Annular dilatation with functional (or mixed, functional-dominant) etiology |
| Indirect Annuloplasty | Coronary sinus | Carillon (Cardiac Dimensions, Kirkland, WA, USA) | Nitinol anchors placed in the distal and proximal coronary sinus Reduction of MV annulus diameter upon deployment of the device Transjugular approach | Annular dilatation with functional (or mixed, functional-dominant) etiology Coronary sinus proximity and coplanarity |
| Chordal replacement | Papillary muscles | NeoChord (NeoChord, St Louis Park, MN, USA) | Surgical off-pump procedure Implantation of artificial chords Transapical access | Prolapse or flail Leaflet-to-annulus index ≥ 1.25 |
| MV replacement | MV apparatus | Tendyne (Abbott Vascular, Abbott Park, IL, USA) | Self-expanding valve Indicated in suboptimal anatomy for transcatheter repair Transapical approach | MVA 1.0–3.0 cm2 Multisegment disease Commissural disease, perforations, clefts Mean gradients 5–10 mmHg Unlikely LVOT obstruction LVEF ≥ 30% Suboptimal MR reduction expected with transcatheter repair No scar or remodeled LV (transapical access) |
| COAPT | MITRA-FR | CLASP | CLASP (FMR) | |
|---|---|---|---|---|
| Patients enrolled | 614 | 304 | 124 | 85 (single arm) |
| Technical implantation success | 98% | 96% | 96% | 96% |
| Atrial fibrillation/Flutter | 57.3% | 34.5% | 53.4% | 45% |
| LVEF | 31 ± 9% | 33 ± 7% | 44 ± 14% | 37 ± 10% |
| EROA | 41 ± 15 mm2 | 31 ± 10 mm2 | 38 ± 15 mm2 | 34 ± 11 mm2 |
| LVEDV | 101 ± 34 mL/m2 | 135 ± 35 mL/m2 | 181 ± 61 mL | 199 ± 59 mL |
| Mortality at 1 y and 2 y | 19% and 29% | 23% and 34% | 9% and 20% | 12% and 28% |
| MR ≥ 3+ at discharge → 12 mo → 24 mo | 7.4% → 5% → 0.9% | 8% → 17% → not recorded | 4% * → 0% → 3% | 4% * → 0% → 5% |
| Type of Intervention | Target Structure | Device | Description | Eligibility Criteria |
|---|---|---|---|---|
| Edge-to-edge | Tricuspid leaflets | TriClip (Abbott Vascular, Abbott Park, IL, USA) PASCAL (Edwards Lifesciences, Irvine, CA, USA) | Based on edge-to-edge technique Approximation of the septal and anterior leaflets or septal and posterior leaflets | Small septolateral gap ≤ 7 mm Anteroseptal jet location Trileaflet morphology Diffusely degenerated leaflets and pacemaker lead impingement are unfavorable anatomic conditions |
| Direct Annuloplasty | Tricuspid annulus | Cardioband (Edwards Lifesciences, Irvine, CA, USA) | Implantation of a flexible ring with multiple anchors on the hinge of the annulus Challenging procedure Distance between RCA and annulus may be a limitation | Annular dilatation as primary mechanism of TR Mild tethering (tenting height <0.76 cm, tenting area < 1.63 cm2, tenting volume < 2.3 mL) Central jet location Sufficient landing zone for anchoring |
| Heterotopic replacement | Superior and inferior caval veins | TricValve (Orbus Vienna AU, Wien, Austria) | Self-expanding valves Indicated in patients with significant backflow in the IVC and/or SVC Palliative care in unfavorable anatomy for transcatheter repair Irrespective of the TR etiology | Appropriate caval diameters (and intercaval distance) Contraindicated in severe RV dysfunction and pulmonary hypertension |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cammalleri, V.; Antonelli, G.; De Luca, V.M.; Carpenito, M.; Nusca, A.; Bono, M.C.; Mega, S.; Ussia, G.P.; Grigioni, F. Functional Mitral and Tricuspid Regurgitation across the Whole Spectrum of Left Ventricular Ejection Fraction: Recognizing the Elephant in the Room of Heart Failure. J. Clin. Med. 2023, 12, 3316. https://doi.org/10.3390/jcm12093316
Cammalleri V, Antonelli G, De Luca VM, Carpenito M, Nusca A, Bono MC, Mega S, Ussia GP, Grigioni F. Functional Mitral and Tricuspid Regurgitation across the Whole Spectrum of Left Ventricular Ejection Fraction: Recognizing the Elephant in the Room of Heart Failure. Journal of Clinical Medicine. 2023; 12(9):3316. https://doi.org/10.3390/jcm12093316
Chicago/Turabian StyleCammalleri, Valeria, Giorgio Antonelli, Valeria Maria De Luca, Myriam Carpenito, Annunziata Nusca, Maria Caterina Bono, Simona Mega, Gian Paolo Ussia, and Francesco Grigioni. 2023. "Functional Mitral and Tricuspid Regurgitation across the Whole Spectrum of Left Ventricular Ejection Fraction: Recognizing the Elephant in the Room of Heart Failure" Journal of Clinical Medicine 12, no. 9: 3316. https://doi.org/10.3390/jcm12093316