
Effectiveness of a Manual Therapy Protocol in Women with Pelvic Pain Due to Endometriosis: A Randomized Clinical Trial

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Randomization, Blinding, and Masking
2.4. Interventions
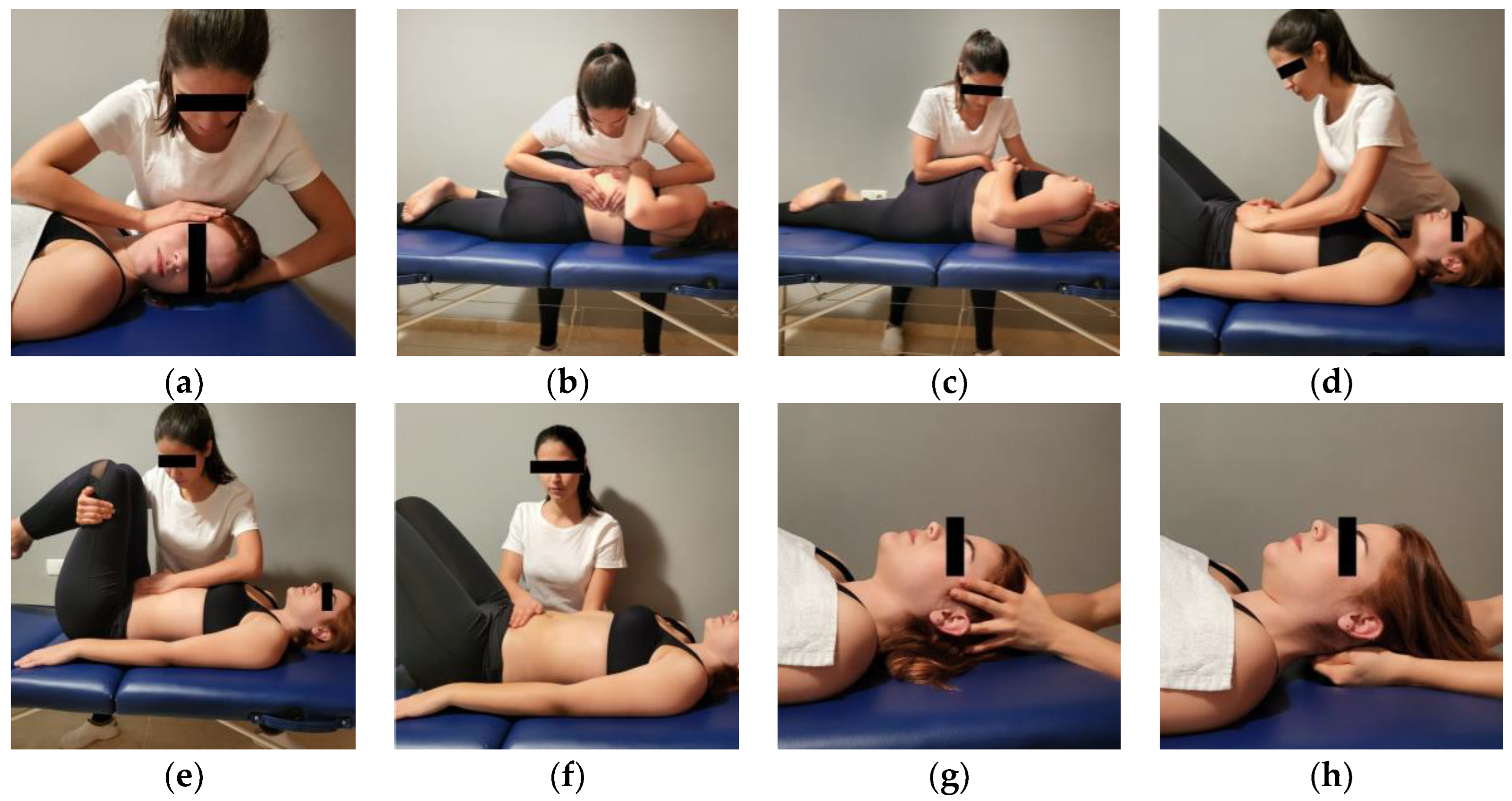
2.4.1. Manual Therapy Protocol
2.4.2. Placebo Treatment
2.5. Main Outcome Measures
2.5.1. Clinical Characteristics
2.5.2. Clinical Features Related to Quality of Life
2.5.3. Emotional Condition
2.5.4. Patient’s Perception of Change after the Intervention
2.6. Statistics
2.7. Sample Size Calculation
3. Results
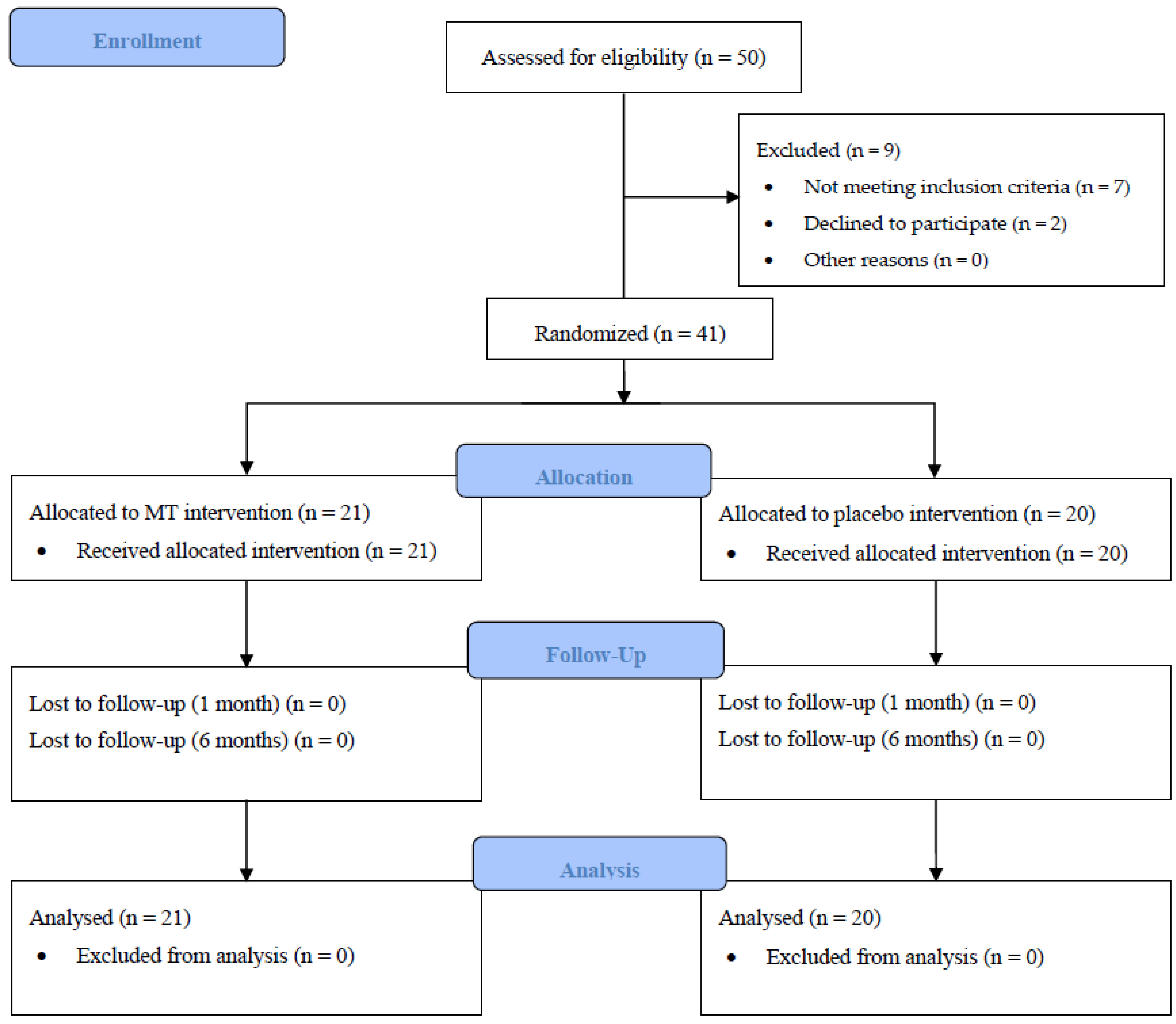
3.1. Participants
3.2. Effect of the Treatment on Pelvic Pain and Lumbar Mobility
3.3. Effect of the Treatment on Clinical Features Related to Quality of Life
3.4. Effect of the Treatment on Emotional Condition
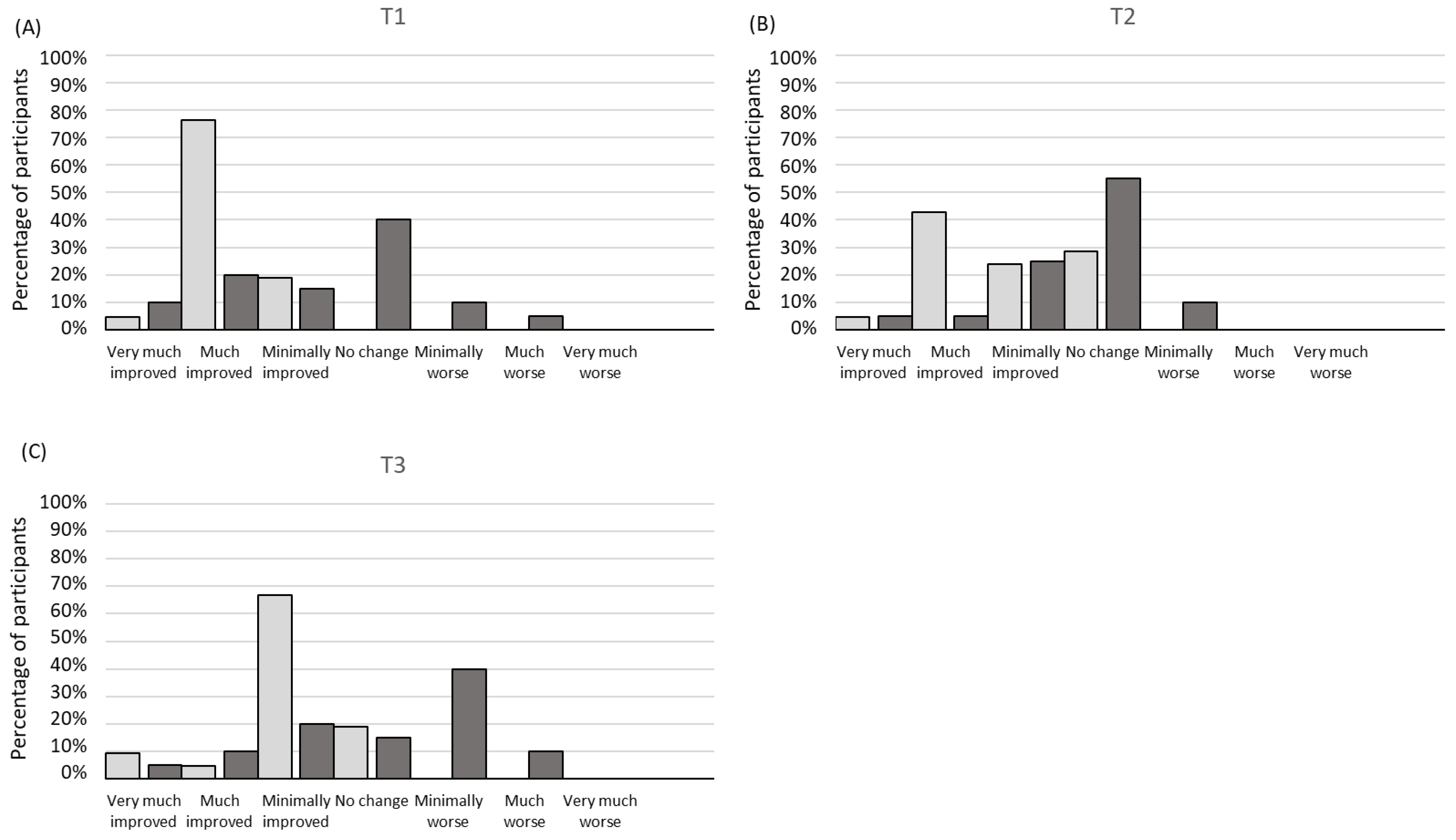
3.5. Patient’s Perception of Change after Treatment
3.6. Patients’ Perception of Group Assignment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zullo, F.; Spagnolo, E.; Saccone, G.; Acunzo, M.; Xodo, S.; Ceccaroni, M.; Berghella, V. Endometriosis and obstetrics complications: A systematic review and meta-analysis. Fertil. Steril. 2017, 108, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Vercellini, P.; Fedele, L.; Aimi, G.; Pietropaolo, G.; Consonni, D.; Crosignani, P.G. Association between endometriosis stage, lesion type, patient characteristics and severity of pelvic pain symptoms: A multivariate analysis of over 1000 patients. Hum. Reprod. 2007, 22, 266–271. [Google Scholar] [CrossRef]
- Triolo, O.; Laganà, A.S.; Sturlese, E. Chronic Pelvic Pain in Endometriosis: An Overview. J. Clin. Med. Res. 2013, 5, 153–163. [Google Scholar] [CrossRef]
- Nnoaham, K.E.; Hummelshoj, L.; Webster, P.; d’Hooghe, T.; de Cicco Nardone, F.; de Cicco Nardone, C.; Jenkinson, C.; Kennedy, S.H.; Zondervan, K.T.; World Endometriosis Research Foundation Global Study of Women’s Health Consortium. Impact of endometriosis on quality of life and work productivity: A multicenter study across ten countries. Fertil. Steril. 2011, 96, 366–373.e8. [Google Scholar] [CrossRef]
- Carbone, M.G.; Campo, G.; Papaleo, E.; Marazziti, D.; Maremmani, I. The importance of a multi-disciplinary approach to the endometriotic patients: The relationship between endometriosis and psychic vulnerability. J. Clin. Med. 2021, 10, 1616. [Google Scholar] [CrossRef] [PubMed]
- Karp, B.I.; Stratton, P. Endometriosis-associated chronic pelvic pain. Med 2023, 4, 143–146. [Google Scholar] [CrossRef]
- Chaichian, S.; Kabir, A.; Mehdizadehkashi, A.; Rahmani, K.; Moghimi, M.; Moazzami, B. Comparing the efficacy of surgery and medical therapy for pain management in endometriosis: A systematic review and meta-analysis. Pain Physician 2017, 20, 185–195. [Google Scholar] [PubMed]
- Becker, C.M.; Gattrell, W.T.; Gude, K.; Singh, S.S. Reevaluating response and failure of medical treatment of endometriosis: A systematic review. Fertil. Steril. 2017, 108, 125–136. [Google Scholar] [CrossRef]
- Fitzcharles, M.-A.; Cohen, S.P.; Clauw, D.J.; Littlejohn, G.; Usui, C.; Häuser, W. Nociplastic pain: Towards an understanding of prevalent pain conditions. Lancet 2021, 397, 2098–2110. [Google Scholar] [CrossRef]
- Baranowski, A.P. Chronic pelvic pain. Best Pract. Res. Clin. Gastroenterol. 2009, 23, 593–610. [Google Scholar] [CrossRef]
- Aredo, J.V.; Heyrana, K.J.; Karp, B.I.; Shah, J.P.; Stratton, P. Relating chronic pelvic pain and endometriosis to signs of sensitization and myofascial pain and dysfunction. Semin. Reprod. Med. 2017, 35, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Lara-Ramos, A.; Álvarez-Salvago, F.; Fernández-Lao, C.; Galiano-Castillo, N.; Ocón-Hernández, O.; Mazheika, M.; Salinas-Asensio, M.M.; Mundo-López, A.; Arroyo-Morales, M.; Cantarero-Villanueva, I.; et al. Widespread pain hypersensitivity and lumbopelvic impairments in women diagnosed with endometriosis. Pain Med. 2021, 22, 1970–1981. [Google Scholar] [CrossRef] [PubMed]
- Berghmans, B. Physiotherapy for pelvic pain and female sexual dysfunction: An untapped resource. Int. Urogynecol. J. 2018, 29, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Physical Therapy. Cologne, Germany: Institute for Quality and Efficiency in Health Care (IQWiG). 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK561514/ (accessed on 27 April 2023).
- Arribas-Romano, A.; Fernández-Carnero, J.; Molina-Rueda, F.; Angulo-Diaz-Parreño, S.; Navarro-Santana, M.J. Efficacy of physical therapy on nociceptive pain processing alterations in patients with chronic musculoskeletal pain: A systematic review and meta-analysis. Pain Med. 2020, 21, 2502–2517. [Google Scholar] [CrossRef] [PubMed]
- Ruffini, N.; D’Alessandro, G.; Pimpinella, A.; Galli, M.; Galeotti, T.; Cerritelli, F.; Tramontano, M. The role of osteopathic care in gynaecology and obstetrics: An updated systematic review. Healthcare 2022, 10, 1566. [Google Scholar] [CrossRef]
- Smith, A.R. Manual therapy: The historical, current, and future role in the treatment of pain. ScientificWorldJournal 2007, 7, 109–120. [Google Scholar] [CrossRef]
- Muñoz-Gómez, E.; Inglés, M.; Aguilar-Rodríguez, M.; Mollà-Casanova, S.; Sempere-Rubio, N.; Serra-Añó, P.; Espí-López, G. Effect of a craniosacral therapy protocol in people with migraine: A randomized controlled trial. J. Clin. Med. 2022, 11, 759. [Google Scholar] [CrossRef]
- Muñoz-Gómez, E.; Inglés, M.; Serra-Añó, P.; Espí-López, G.V. Effectiveness of a manual therapy protocol based on articulatory techniques in migraine patients. A randomized controlled trial. Musculoskelet. Sci. Pract. 2021, 54, 102386. [Google Scholar] [CrossRef]
- Muñoz-Gómez, E.; Serra-Añó, P.; Mollà-Casanova, S.; Sempere-Rubio, N.; Aguilar-Rodríguez, M.; Espí-López, G.V.; Inglés, M. Potential add-on effects of manual therapy techniques in migraine patients: A randomised controlled trial. J. Clin. Med. 2022, 11, 4686. [Google Scholar] [CrossRef]
- Daraï, C.; Deboute, O.; Zacharopoulou, C.; Laas, E.; Canlorbe, G.; Belghiti, J.; Zilberman, S.; Ballester, M.; Daraï, E. Impact of osteopathic manipulative therapy on quality of life of patients with deep infiltrating endometriosis with colorectal involvement: Results of a pilot study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 188, 70–73. [Google Scholar] [CrossRef]
- Sillem, M.; Juhasz-Böss, I.; Klausmeier, I.; Mechsner, S.; Siedentopf, F.; Solomayer, E. Osteopathy for endometriosis and chronic pelvic pain—A pilot study. Geburtshilfe Frauenheilkd. 2016, 76, 960–963. [Google Scholar] [CrossRef] [PubMed]
- Goyal, K.; Goyal, M.; Narkeesh, K.; John Samuel, A.; Sharma, S.; Chatterjee, S.; Arumugam, N. The effectiveness of osteopathic manipulative treatment in an abnormal uterine bleeding related pain and health related quality of life (HR-QoL)—A case report. J. Bodyw. Mov. Ther. 2017, 21, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Fryette, H.H. Occiput-Atlas-Axis. J. Am. Osteopath. Assoc. 1936, 35, 353–354. [Google Scholar]
- Oliva Pascual-Vaca, Á.; Punzano-Rodríguez, R.; Escribá-Astaburuaga, P.; Fernández-Domínguez, J.C.; Ricard, F.; Franco-Sierra, M.A.; Rodríguez-Blanco, C. Short-term changes in algometry, inclinometry, stabilometry, and urinary pH analysis after a thoracolumbar junction manipulation in patients with kidney stones. J. Altern. Complement. Med. 2017, 23, 639–647. [Google Scholar] [CrossRef]
- Méndez-Sánchez, R.; González-Iglesias, J.; Sánchez-Sánchez, J.L.; Puente-González, A.S. Immediate effects of bilateral sacroiliac joint manipulation on plantar pressure distribution in asymptomatic participants. J. Altern. Complement. Med. 2014, 20, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Espí-López, G.V.; Inglés, M.; Soliva-Cazabán, I.; Serra-Añó, P. Effect of the soft-tissue techniques in the quality of life in patients with Crohn’s disease. Medicine 2018, 97, e13811. [Google Scholar] [CrossRef]
- Arnadottir, T.S.; Sigurdardottir, A.K. Is craniosacral therapy effective for migraine? Tested with HIT-6 Questionnaire. Complement. Ther. Clin. Pract. 2013, 19, 11–14. [Google Scholar] [CrossRef]
- Cabrera-Martos, I.; Valenza, M.C.; Valenza-Demet, G.; Benítez-Feliponi, A.; Robles-Vizcaíno, C.; Ruiz-Extremera, A. Effects of manual therapy on treatment duration and motor development in infants with severe nonsynostotic plagiocephaly: A randomised controlled pilot study. Child’s Nerv. Syst. 2016, 32, 2211–2217. [Google Scholar] [CrossRef]
- Sutherland, W. The Cranial Bowl; Free Press Co.: Mankato, MN, USA, 1939. [Google Scholar]
- Bang, H.; Flaherty, S.P.; Kolahi, J.; Park, J. Blinding assessment in clinical trials: A review of statistical methods and a proposal of blinding assessment protocol. Clin. Res. Regul. Aff. 2010, 27, 42–51. [Google Scholar] [CrossRef]
- Bijur, P.E.; Silver, W.; Gallagher, E.J. Reliability of the visual analog scale for measurement of acute pain. Acad. Emerg. Med. 2001, 8, 1153–1157. [Google Scholar] [CrossRef]
- Emshoff, R.; Bertram, S.; Emshoff, I. Clinically important difference thresholds of the visual analog scale: A conceptual model for identifying meaningful intraindividual changes for pain intensity. Pain 2011, 152, 2277–2282. [Google Scholar] [CrossRef] [PubMed]
- Robinson, H.S.; Mengshoel, A.M. Assessments of lumbar flexion range of motion: Intertester reliability and concurrent validity of 2 commonly used clinical tests. Spine 2014, 39, E270. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.; Jenkinson, C.; Kennedy, S. Evaluating the responsiveness of the Endometriosis Health Profile Questionnaire: The EHP-30. Qual. Life Res. 2004, 13, 705–713. [Google Scholar] [CrossRef] [PubMed]
- Marí-Alexandre, J.; García-Oms, J.; Agababyan, C.; Belda-Montesinos, R.; Royo-Bolea, S.; Varo-Gómez, B.; Díaz-Sierra, C.; González-Cantó, E.; Gilabert-Estellés, J. Toward an improved assessment of quality of life in endometriosis: Evaluation of the Spanish version of the Endometriosis Health Profile 30. J. Psychosom. Obstet. Gynaecol. 2020, 43, 251–257. [Google Scholar] [CrossRef]
- Ware, J.; Sherbourne, C. The MOS 36-item short form health survey (SF-36). Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Vilagut, G.; Ferrer, M.; Rajmil, L.; Rebollo, P.; Permanyer-Miralda, G.; Quintana, J.M.; Santed, R.; Valderas, J.M.; Ribera, A.; Domingo-Salvany, A.; et al. The Spanish version of the Short Form 36 Health Survey: A decade of experience and new developments. Gac. Sanit. 2005, 19, 135–150. [Google Scholar] [CrossRef]
- Perrot, S.; Lantéri-Minet, M. Patients’ global impression of change in the management of peripheral neuropathic pain: Clinical relevance and correlations in daily practice. Eur. J. Pain 2019, 23, 1117–1128. [Google Scholar] [CrossRef]
- Beck, A.; Ward, C.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiat. 1961, 4, 561–571. [Google Scholar] [CrossRef]
- Beck, A.; Steer, R.; Brown, G. Manual for the Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Wang, Y.-P.; Gorenstein, C. Psychometric properties of the Beck Depression Inventory-II: A comprehensive review. Braz. J. Psychiatry 2013, 35, 416–431. [Google Scholar] [CrossRef]
- Dworkin, R.H.; Turk, D.C.; Wyrwich, K.W.; Beaton, D.; Cleeland, C.S.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Kerns, R.D.; Ader, D.N.; et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J. Pain 2008, 9, 105–121. [Google Scholar] [CrossRef]
- Spielberger, C.; Gorsuch, R.; Lushene, R.; Vagg, P.; Jacobs, G. Manual for State-Trait Anxiety Inventory; Consulting Psychologist Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Guillén-Riquelme, A.; Buela-Casal, G. Meta-analysis of group comparison and meta-analysis of reliability generalization of the State-Trait Anxiety Inventory Questionnaire (STAI). Rev. Esp. Salud Publica 2014, 88, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Taghizadeh, N.; Tremblay, A.; Cressman, S.; Peacock, S.; McWilliams, A.M.; MacEachern, P.; Johnston, M.R.; Goffin, J.; Goss, G.; Nicholas, G.; et al. Health-related quality of life and anxiety in the PAN-CAN lung cancer screening cohort. BMJ Open 2019, 9, e024719. [Google Scholar] [CrossRef] [PubMed]
- Kamper, S.J.; Maher, C.G.; Mackay, G. Global rating of change scales: A review of strengths and weaknesses and considerations for design. J. Man. Manip. Ther. 2009, 17, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, L.; Scheman, J. Patient global impression of change scores within the context of a chronic pain rehabilitation program. J. Pain 2009, 10, S73. [Google Scholar] [CrossRef]
- Thalheimer, W.; Cook, S. How to calculate effect sizes from published research: A simplified methodology. Work. Learn. Res. 2002, 1, 1–9. [Google Scholar]
- Barral, J.; Mercier, P. Visceral Manipulation; Eastland Press: Seattle, WA, USA, 1988; pp. 1–20. [Google Scholar]
- Wójcik, M.; Szczepaniak, R.; Placek, K. Physiotherapy management in endometriosis. Int. J. Environ. Res. Public Health 2022, 19, 16148. [Google Scholar] [CrossRef]
- Bender, T.; Nagy, G.; Barna, I.; Tefner, I.; Kádas, E.; Géher, P. The effect of physical therapy on beta-endorphin levels. Eur. J. Appl. Physiol. 2007, 100, 371–382. [Google Scholar] [CrossRef]
- Vigotsky, A.D.; Bruhns, R.P. The role of descending modulation in manual therapy and its analgesic implications: A narrative review. Pain Res. Treat. 2015, 2015, 292805. [Google Scholar] [CrossRef]
- Coronado, R.A.; Gay, C.W.; Bialosky, J.E.; Carnaby, G.D.; Bishop, M.D.; George, S.Z. Changes in pain sensitivity following spinal manipulation: A systematic review and meta-analysis. J. Electromyogr. Kinesiol. 2012, 22, 752–767. [Google Scholar] [CrossRef]
- Schmid, A.; Brunner, F.; Wright, A.; Bachmann, L.M. Paradigm shift in manual therapy? Evidence for a central nervous system component in the response to passive cervical joint mobilisation. Man. Ther. 2008, 13, 387–396. [Google Scholar] [CrossRef]
- Chu, J.; Allen, D.D.; Pawlowsky, S.; Smoot, B. Peripheral response to cervical or thoracic spinal manual therapy: An evidence-based review with meta analysis. J. Man. Manip. Ther. 2014, 22, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Voogt, L.; de Vries, J.; Meeus, M.; Struyf, F.; Meuffels, D.; Nijs, J. Analgesic effects of manual therapy in patients with musculoskeletal pain: A systematic review. Man. Ther. 2015, 20, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Abril-Coello, R.; Correyero-León, M.; Ceballos-Laita, L.; Jiménez-Barrio, S. Benefits of physical therapy in improving quality of life and pain associated with endometriosis: A systematic review and meta-analysis. Int. J. Gynecol. Obstet. 2022. [Google Scholar] [CrossRef]
- Lozano-Lozano, M.; Mundo-López, A.; San-Sebastian, A.P.; Galiano-Castillo, N.; Fernandez-Lao, C.; Cantarero-Villanueva, I.; Arroyo-Morales, M.; Ocón-Hernández, O.; Artacho-Cordón, F. Limitations in activities of daily living among spanish women diagnosed with endometriosis. Am. J. Occup. Ther. 2021, 75, 7506205050. [Google Scholar] [CrossRef] [PubMed]
- Castro-Sánchez, A.M.; Gil-Martínez, E.; Fernández-Sánchez, M.; Lara-Palomo, I.C.; Nastasia, I.; de Los Ángeles Querol-Zaldívar, M.; Aguilar-Ferrándiz, M.E. Manipulative therapy of sacral torsion versus myofascial release in patients clinically diagnosed posterior pelvic pain: A consort compliant randomized controlled trial. Spine J. 2021, 21, 1890–1899. [Google Scholar] [CrossRef]
- Bialosky, J.E.; Bishop, M.D.; Penza, C.W. Placebo mechanisms of manual therapy: A sheep in wolf ’s clothing? J. Orthop. Sport. Phys. Ther. 2017, 47, 301–304. [Google Scholar] [CrossRef] [PubMed]
- Daraï, C.; Bendifallah, S.; Foulot, H.; Ballester, M.; Chabbert-Buffet, N.; Daraï, E. Impact of osteopathic manipulative therapy in patient with deep with colorectal endometriosis: A classification based on symptoms and quality of life. Gynécologie Obs. Fertil. Sénologie 2017, 45, 472–477. [Google Scholar] [CrossRef]
- Benz, L.N.; Flynn, T.W. Placebo, nocebo, and expectations: Leveraging positive outcomes. J. Orthop. Sports Phys. Ther. 2013, 43, 439–441. [Google Scholar] [CrossRef]
- van Barneveld, E.; Manders, J.; van Osch, F.H.M.; van Poll, M.; Visser, L.; van Hanegem, N.; Lim, A.C.; Bongers, M.Y.; Leue, C. Depression, anxiety, and correlating factors in endometriosis: A systematic review and meta-analysis. J. Women’s Health 2022, 31, 219–230. [Google Scholar] [CrossRef]
- Vandyken, C.; Hilton, S. Physical therapy in the treatment of central pain mechanisms for female sexual pain. Sex. Med. Rev. 2017, 5, 20–30. [Google Scholar] [CrossRef]
- Geri, T.; Viceconti, A.; Minacci, M.; Testa, M.; Rossettini, G. Manual therapy: Exploiting the role of human touch. Musculoskelet. Sci. Pract. 2019, 44, 102044. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| MTG (n = 21) | PG (n = 20) | Total (n = 41) | p-Value | |
|---|---|---|---|---|
| Age a | 34.85 (7.23) | 37.40 (6.62) | 36.10 (6.97) | 0.25 |
| Time of evolution (months) a | 38.86 (43.53) | 74.18 (88.02) | 56.09 (70.34) | 0.11 |
| Pregnancy history b | ||||
| No pregnancy | 10 (47.62%) | 10 (50.00%) | 20 (48.78%) | 0.88 |
| One pregnancy | 7 (33.33%) | 6 (30.00%) | 13 (31.71%) | 0.82 |
| More than one pregnancy | 2 (9.52%) | 2 (10.00%) | 4 (9.76%) | 0.96 |
| Miscarriage | 2 (9.52%) | 3 (15.00%) | 5 (12.20%) | 0.59 |
| Delayed fertility | 6 (28.57%) | 4 (20.00%) | 10 (24.39%) | 0.52 |
| Hysterectomy history b | 0.07 | |||
| No | 21 (100.00%) | 17 (85.00%) | 38 (92.68%) | |
| Yes | 0 (0.00%) | 3 (15.00%) | 3 (7.32%) | |
| Symptoms associated with endometriosis b | ||||
| Abdominal swelling | 17 (80.95%) | 16 (80.00%) | 33 (33.00%) | 0.94 |
| Menstrual pain | 15 (71.43%) | 11 (55.00%) | 26 (26.00%) | 0.28 |
| Non-menstrual pelvic pain | 15 (71.43%) | 15 (75.00%) | 30 (30.00%) | 0.80 |
| Fatigue | 14 (66.67%) | 11 (55.00%) | 25 (25.00%) | 0.44 |
| Low back pain | 13 (61.90%) | 13 (65.00%) | 26 (26.00%) | 0.84 |
| Ovulation pain | 11 (52.38%) | 5 (25.00%) | 16 (16.00%) | 0.07 |
| Dyspareunia | 8 (38.10%) | 10 (50.00%) | 18 (18.00%) | 0.44 |
| Abundant bleeding | 8 (38.10%) | 7 (35.00%) | 15 (15.00%) | 0.84 |
| Diarrhea | 8 (38.10%) | 7 (35.00%) | 15 (15.00%) | 0.84 |
| Constipation | 8 (38.10%) | 13 (65.00%) | 21 (21.00%) | 0.09 |
| Urinary incontinence | 4 (19.05%) | 6 (30.00%) | 10 (10.00%) | 0.414 |
| Full bladder sensation | 4 (19.05%) | 8 (40.00%) | 12 (12.00%) | 0.141 |
| Delayed fertility | 2 (9.52%) | 3 (15.00%) | 5 (5.00%) | 0.592 |
| Infertility | 1 (4.76%) | 2 (10.00%) | 3 (3.00%) | 0.520 |
| Medication intake b | ||||
| Hormonal | 9 (42.86%) | 13 (65.00%) | 22 (53.66%) | 0.16 |
| Analgesics | 15 (71.43%) | 13 (65.00%) | 28 (68.29%) | 0.66 |
| Anti-inflammatory | 3 (14.29%) | 2 (10.00%) | 5 (12.20%) | 0.68 |
| Dietary supplements | 3 (14.29%) | 3 (15.00%) | 6 (14.63%) | 0.95 |
| Anxiolytic/Antidepressant | 2 (9.52%) | 0 (0.00%) | 2 (4.88%) | 0.16 |
| None | 4 (19.05%) | 2 (10.00%) | 6 (14.63%) | 0.41 |
| Variable | Group | T0 | T1 | T2 | T3 |
|---|---|---|---|---|---|
| Pain (VAS) | MTG | 5.43 (1.78) | 3.76 (1.55) * # | 3.95 (1.86) * | 1.62 (1.56) * # |
| PG | 5.10 (1.92) | 5.05 (2.09) | 4.70 (2.08) | 4.55 (1.67) * | |
| Lumbar mobility (Schober test; cm) | MTG | 19.62 (1.06) | 20.05 (0.99) # | 20.08 (0.94) # | 19.94 (1.38) # |
| PG | 19.00 (1.48) | 19.04 (0.73) | 19.13 (0.71) | 18.08 (2.39) |
| Variable | Group | T0 | T1 | T2 | T3 |
|---|---|---|---|---|---|
| Endometriosis Health Profile (EHP-30) | |||||
| Pain | MTG | 52.38 (16.17) | 25.87 (17.96) * # | 30.12 (23.65) * | 30.95 (24.49) * |
| PG | 47.27 (16.43) | 42.05 (15.10) | 38.18 (20.76) | 36.14 (23.93) | |
| Control and powerlessness | MTG | 48.81 (22.09) | 33.44 (22.90) * | 41.83 (28.04) | 38.29 (25.87) |
| PG | 48.54 (19.97) | 42.84 (14.11) | 41.04 (25.26) | 42.50 (27.92) | |
| Emotional wellbeing | MTG | 55.75 (17.70) | 44.44 (26.63) * | 48.21 (24.32) | 41.47 (22.11) * |
| PG | 47.50 (13.75) | 37.50 (17.15) * | 38.75 (14.44) | 37.92 (17.46) * | |
| Social support | MTG | 53.87 (20.39) | 47.92 (33.68) | 47.62 (26.55) | 47.02 (30.47) |
| PG | 45.31 (27.72) | 39.06 (16.95) | 42.38 (22.31) | 39.06 (22.39) | |
| Self-image | MTG | 47.62 (21.11) | 44.44 (30.43) | 46.03 (28.58) | 42.06 (29.87) |
| PG | 45.42 (22.70) | 40.00 (25.01) | 40.00 (24.42) | 45.42 (27.24) | |
| Total score | MTG | 51.69 (16.01) | 39.22 (23.56) * | 42.76 (22.50) * | 39.96 (23.66) * |
| PG | 46.81 (14.76) | 40.29 (14.22) | 40.07 (17.39) | 40.21 (20.13) | |
| Quality of life (SF-36) | |||||
| Physical functioning | MTG | 83.57 (21.28) | 84.52 (21.21) | 80.95 (22.28) | 90.24 (10.78) |
| PG | 72.75 (26.28) | 78.00 (21.30) | 76.25 (26.40) | 78.50 (29.43) | |
| Physical role | MTG | 30.95 (42.50) | 60.71 (40.75) * | 50.00 (41.08) | 52.38 (41.01) |
| PG | 42.50 (45.23) | 48.75 (40.13) | 50.00 (45.16) | 50.00 (45.88) | |
| Corporal pain | MTG | 48.57 (24.68) | 64.00 (23.82) * # | 62.67 (20.54) | 55.81 (25.46) |
| PG | 42.30 (22.74) | 46.40 (25.60) | 49.00 (26.43) | 51.30 (30.53) | |
| General health | MTG | 39.81 (19.85) | 51.62 (22.39) * | 44.52 (18.72) | 46.05 (20.48) |
| PG | 39.50 (15.70) | 43.25 (17.54) | 47.50 (20.84) | 44.25 (19.67) | |
| Vitality | MTG | 40.00 (20.86) | 48.57 (20.13) | 47.14 (18.55) | 46.19 (19.93) |
| PG | 46.25 (20.89) | 46.75 (21.78) | 48.00 (19.76) | 48.75 (19.79) | |
| Social functioning | MTG | 67.26 (22.87) | 67.26 (29.97) | 74.40 (37.18) | 61.90 (28.63) |
| PG | 62.50 (25.33) | 69.38 (26.74) | 70.00 (26.72) | 71.88 (30.31) | |
| Emotional role | MTG | 44.44 (45.13) | 65.08 (37.23) | 60.32 (37.45) | 63.49 (42.04) |
| PG | 68.33 (43.90) | 71.67 (34.67) | 66.67 (40.47) | 66.67 (34.20) | |
| Mental health | MTG | 55.62 (15.28) | 61.52 (14.06) | 56.57 (11.19) | 59.62 (17.34) |
| PG | 58.20 (17.96) | 67.20 (17.15) | 66.00 (18.87) * | 66.60 (18.32) | |
| Physical subscale | MTG | 50.73 (20.63) | 65.21 (21.29) * | 59.54 (19.30) | 61.12 (20.25) |
| PG | 49.26 (22.91) | 54.10 (20.97) | 55.69 (26.33) | 56.01 (27.7) | |
| Mental subscale | MTG | 51.83 (22.01) | 60.61 (22.14) | 58.27 (17.62) | 57.80 (23.51) |
| PG | 58.82 (20.48) | 63.75 (20.58) | 62.67 (21.24) | 63.47 (18.65) | |
| Overall quality of life | MTG | 51.28 (20.12) | 61.00 (22.53) | 60.03 (19.66) | 59.46 (20.53) |
| PG | 54.04 (20.23) | 59.71 (19.68) | 59.33 (22.98) | 59.74 (21.59) | |
| Variable | Group | T0 | T1 | T2 | T3 |
|---|---|---|---|---|---|
| Depression levels (BDI-II) | MTG | 15.86 (8.45) | 13.71 (9.32) | 13.29 (8.85) | 11.14 (10.07) |
| PG | 14.90 (10.20) | 13.20 (8.73) | 12.10 (7.58) | 9.60 (6.98) | |
| Anxiety levels (STAI) | |||||
| State-anxiety | MTG | 36.14 (5.52) | 45.00 (13.94) | 43.57 (12.50) | 46.71 (14.84) |
| PG | 37.70 (3.37) | 41.70 (10.15) | 39.90 (8.03) | 39.40 (7.79) | |
| Trait-anxiety | MTG | 40.57 (10.03) | 38.57 (12.42) | 37.57 (13.46) | 41.29 (11.76) |
| PG | 41.30 (7.44) | 35.40 (9.17) | 36.80 (7.64) | 37.70 (8.38) | |
| Overall anxiety levels | MTG | 38.36 (6.54) | 41.79 (12.93) | 42.79 (10.82) | 44.00 (13.22) |
| PG | 39.50 (4.43) | 38.55 (9.26) | 38.40 (7.55) | 38.55 (7.92) |
| MTG (n = 21) | PG (n = 20) | |
|---|---|---|
| Normal physiotherapy | 21 (100%) | 20 (100%) |
| Control group | 0 (0%) | 0 (0%) |
| Others | 0 (0%) | 0 (0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz-Gómez, E.; Alcaraz-Martínez, A.M.; Mollà-Casanova, S.; Sempere-Rubio, N.; Aguilar-Rodríguez, M.; Serra-Añó, P.; Inglés, M. Effectiveness of a Manual Therapy Protocol in Women with Pelvic Pain Due to Endometriosis: A Randomized Clinical Trial. J. Clin. Med. 2023, 12, 3310. https://doi.org/10.3390/jcm12093310
Muñoz-Gómez E, Alcaraz-Martínez AM, Mollà-Casanova S, Sempere-Rubio N, Aguilar-Rodríguez M, Serra-Añó P, Inglés M. Effectiveness of a Manual Therapy Protocol in Women with Pelvic Pain Due to Endometriosis: A Randomized Clinical Trial. Journal of Clinical Medicine. 2023; 12(9):3310. https://doi.org/10.3390/jcm12093310
Chicago/Turabian StyleMuñoz-Gómez, Elena, Ana María Alcaraz-Martínez, Sara Mollà-Casanova, Núria Sempere-Rubio, Marta Aguilar-Rodríguez, Pilar Serra-Añó, and Marta Inglés. 2023. "Effectiveness of a Manual Therapy Protocol in Women with Pelvic Pain Due to Endometriosis: A Randomized Clinical Trial" Journal of Clinical Medicine 12, no. 9: 3310. https://doi.org/10.3390/jcm12093310