
Definition of the Clinical Characteristics of Patients with Moderate and Severe Atopic Dermatitis for Whom Narrow-Band UVB (NB-UVB) and Medium-Dose UVA1 Phototherapies Are Still Valuable Treatment Options at the Age of Biologics
 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
- -
- The percentage of participants achieving an Investigator’s Global Assessment (IGA) score of 0 (clear) or 1 (almost clear) [18];
- -
- The percentage of patients achieving an IGA score of 0/1 without a relapse within 6 months from the end of treatment (EOT).
- -
- The median final EASI score;
- -
- The percentage of participants achieving EASI 75 (≥75% improvement from baseline EASI), EASI 50 (>50% to <75% improvement) and EASI 90 (>90% improvement);
- -
- The percentage of patients with an EASI improvement of <50%;
- -
- The percentage of patients with phototherapy-related adverse events;
- -
- The percentage of patients with phototherapy-related adverse events leading to treatment discontinuation.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weidinger, S.; Novak, N. Atopic Dermatitis. Lancet 2016, 387, 1109–1122. [Google Scholar] [CrossRef]
- Schneeweiss, M.C.; Perez-Chada, L.; Merola, J.F. Comparative Safety of Systemic Immunomodulatory Medications in Adults with Atopic Dermatitis. J. Am. Acad. Dermatol. 2021, 85, 321–329. [Google Scholar] [CrossRef]
- Musters, A.H.; Mashayekhi, S.; Harvey, J.; Axon, E.; Lax, S.J.; Flohr, C.; Drucker, A.M.; Gerbens, L.; Ferguson, J.; Ibbotson, S.; et al. Phototherapy for Atopic Eczema. Cochrane Database Syst. Rev. 2021, 10, CD013870. [Google Scholar] [CrossRef]
- Kemény, L.; Varga, E.; Novak, Z. Advances in Phototherapy for Psoriasis and Atopic Dermatitis. Expert Rev. Clin. Immunol. 2019, 15, 1205–1214. [Google Scholar] [CrossRef] [PubMed]
- Sidbury, R.; Davis, D.M.; Cohen, D.E.; Cordoro, K.M.; Berger, T.G.; Bergman, J.N.; Chamlin, S.L.; Cooper, K.D.; Feldman, S.R.; Hanifin, J.M.; et al. Guidelines of Care for the Management of Atopic Dermatitis: Section 3. Management and Treatment with Phototherapy And Systemic Agents. J. Am. Acad. Dermatol. 2014, 71, 327–349. [Google Scholar] [CrossRef]
- Meduri, N.B.; Vandergriff, T.; Rasmussen, H.; Jacobe, H. Phototherapy in the Management of Atopic Dermatitis: A Systematic Review. Photodermatol. Photoimmunol. Photomed. 2007, 23, 106–112. [Google Scholar] [CrossRef]
- Beck, L.A.; Thaçi, D.; Hamilton, J.D.; Graham, N.M.; Bieber, T.; Rocklin, R.; Ming, J.E.; Ren, H.; Kao, R.; Simpson, E.; et al. Dupilumab Treatment in Adults with Moderate-to-Severe Atopic Dermatitis. N. Engl. J. Med. 2014, 371, 130–139. [Google Scholar] [CrossRef] [PubMed]
- European Medical Agency. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/dupixent (accessed on 1 March 2023).
- Wollenberg, A.; Kinberger, M.; Arents, B.; Aszodi, N.; Avila Valle, G.; Barbarot, S.; Bieber, T.; Brough, H.A.; Calzavara Pinton, P.; Christen-Zäch, S.; et al. European Guideline (EuroGuiDerm) on Atopic Eczema: Part I—Systemic Therapy. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 1409–1431. [Google Scholar] [CrossRef] [PubMed]
- Eichenfield, L.F.; Tom, W.L.; Berger, T.G.; Krol, A.; Paller, A.S.; Schwarzenberger, K.; Bergman, J.N.; Chamlin, S.L.; Cohen, D.E.; Cooper, K.D.; et al. Guidelines of Care for the Management of Atopic Dermatitis: Section 2. Management and Treatment of Atopic Dermatitis with Topical Therapies. J. Am. Acad. Dermatol. 2014, 71, 116–132. [Google Scholar] [CrossRef] [PubMed]
- Simpson, E.L.; Bruin-Weller, M.; Flohr, C.; Ardern-Jones, M.R.; Barbarot, S.; Deleuran, M.; Bieber, T.; Vestergaard, C.; Brown, S.J.; Cork, M.J.; et al. When Does Atopic Dermatitis Warrant Systemic Therapy? Recommendations from an Expert Panel of the International Eczema Council. J. Am. Acad. Dermatol. 2017, 77, 623–633. [Google Scholar] [CrossRef] [PubMed]
- Chovatiya, R.; Silverberg, J.I. Evaluating the Longitudinal Course of Atopic Dermatitis: Implications for Clinical Practice. Am. J. Clin. Dermatol. 2022, 23, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Calzavara-Pinton, P.G.; Sala, R.; Arisi, M.; Rossi, M.T.; Venturini, M.; Ortel, B. Synergism between Narrowband Ultraviolet B Phototherapy and Etanercept for the Treatment of Plaque-type Psoriasis. Br. J. Dermatol. 2013, 169, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Leshem, Y.A.; Hajar, T.; Hanifin, J.M.; Simpson, E.L. What the Eczema Area and Severity Index Score Tells Us about the Severity of Atopic Dermatitis: An Interpretability Study. Br. J. Dermatol. 2015, 172, 1353–1357. [Google Scholar] [CrossRef]
- Hanifin, J.M.; Thurston, M.; Omoto, M.; Cherill, R.; Tofte, S.J.; Graeber, M.; Evaluator Group, T.E. The Eczema Area and Severity Index (EASI): Assessment of Reliability in Atopic Dermatitis. Exp. Dermatol. 2001, 10, 11–18. [Google Scholar] [CrossRef]
- Calzavara-Pinton, P.; Zanca, A.; Arisi, M.; Rossi, M.T.; Zane, C.; Venturini, M.; Ortel, B. Prevalence of Phototherapy in the Age of Biologics. Dermatology 2018, 234, 166–172. [Google Scholar] [CrossRef]
- Agenzia Italiana del Farmaco (AIFA). Available online: https://www.aifa.gov.it/-/attivazione-web-pubblicazione-registro-dupixent (accessed on 1 March 2023).
- Futamura, M.; Leshem, Y.A.; Thomas, K.S.; Nankervis, H.; Williams, H.C.; Simpson, E.L. A Systematic Review of Investigator Global Assessment (IGA) in Atopic Dermatitis (AD) Trials: Many Options, No Standards. J. Am. Acad. Dermatol. 2016, 74, 288–294. [Google Scholar] [CrossRef]
- Hong, M.R.; Lei, D.; Yousaf, M.; Chavda, R.; Gabriel, S.; Janmohamed, S.R.; Silverberg, J.I. A Real-World Study of the Longitudinal Course of Adult Atopic Dermatitis Severity in Clinical Practice. Ann. Allergy Asthma Immunol. 2020, 125, 686–692.e3. [Google Scholar] [CrossRef]
- Zuberbier, T.; Orlow, S.J.; Paller, A.S.; Taïeb, A.; Allen, R.; Hernanz-Hermosa, J.M.; Ocampo-Candiani, J.; Cox, M.; Langeraar, J.; Simon, J.C. Patient Perspectives on the Management of Atopic Dermatitis. J. Allergy Clin. Immunol. 2006, 118, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Ferriols, A.; Aranegui, B.; Pujol-Montcusí, J.A.; Martín-Gorgojo, A.; Campos-Domínguez, M.; Feltes, R.A.; Gilaberte, Y.; Echeverría-García, B.; Alvarez-Pérez, A.; García-Doval, I. Phototherapy in atopic dermatitis: A systematic review of the literature. Actas Dermo-Sifiliogr. 2015, 106, 387–401. [Google Scholar] [CrossRef]
- Sastre, J.; Baldrich, E.S.; Armario Hita, J.C.; Herráez, L.; Jáuregui, I.; Martín-Santiago, A.; Ortiz de Frutos, J.; Silvestre, J.F.; Valero, A. Consensus on the Clinical Approach to Moderate-to-Severe Atopic Dermatitis in Spain: A Delphi Survey. Dermatol. Res. Pract. 2020, 2020, 1524293. [Google Scholar] [CrossRef]
- Vermeulen, F.M.; Gerbens, L.A.A.; Schmitt, J.; Deleuran, M.; Irvine, A.D.; Logan, K.; Ouwerkerk, W.; Vestergaard, C.; Flohr, C.; Spuls, P.I. The European TREatment of ATopic Eczema (TREAT) Registry Taskforce Survey: Prescribing Practices in Europe for Phototherapy and Systemic Therapy in Adult Patients with Moderate-to-severe Atopic Eczema. Br. J. Dermatol. 2020, 183, 1073–1082. [Google Scholar] [CrossRef] [PubMed]
- Krutmann, J. Phototherapy for Atopic Dermatitis. Clin. Exp. Dermatol. 2000, 25, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Rodenbeck, D.L.; Silverberg, J.I.; Silverberg, N.B. Phototherapy for Atopic Dermatitis. Clin. Dermatol. 2016, 34, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Vieyra-Garcia, P.A.; Wolf, P. A Deep Dive into UV-Based Phototherapy: Mechanisms of Action and Emerging Molecular Targets in Inflammation and Cancer. Pharmacol. Ther. 2021, 222, 107784. [Google Scholar] [CrossRef]
- Tintle, S.; Shemer, A.; Suárez-Fariñas, M.; Fujita, H.; Gilleaudeau, P.; Sullivan-Whalen, M.; Johnson-Huang, L.; Chiricozzi, A.; Cardinale, I.; Duan, S.; et al. Reversal of Atopic Dermatitis with Narrow-Band UVB Phototherapy and Biomarkers for Therapeutic Response. J. Allergy Clin. Immunol. 2011, 128, 583–593.e4. [Google Scholar] [CrossRef]
- Legat, F.J. The Antipruritic Effect of Phototherapy. Front. Med. 2018, 5, 333. [Google Scholar] [CrossRef]
- Vieyra-Garcia, P.A.; Wolf, P. From Early Immunomodulatory Triggers to Immunosuppressive Outcome: Therapeutic Implications of the Complex Interplay Between the Wavebands of Sunlight and the Skin. Front. Med. 2018, 5, 232. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patients Treated with Medium-Dose UVA1 | Patients Treated with NB-UVB | Comparisons of Patients’ Groups Treated in 2013–2017 or 2018–2022 with the 2 Phototherapies | ||||||
|---|---|---|---|---|---|---|---|---|
| Column | (a) | (b) | (a) vs. (b) | (c) | (d) | (c) vs. (d) | (a) vs. (c) | (b) vs. (d) |
| 2013–2017 | 2018–2022 | p | 2013–2017 | 2018–2022 | p | p | p | |
| Number | 46 | 16 | 99 | 26 | ||||
| Age (years), median (range) | 26.0 (7–67) | 24.5 (10–52) | NS | 31 (13–73) | 20.5 (14–66) | NS | NS | NS |
| Gender | NS | NS | NS | NS | ||||
| Male (%) | 12 (41.3%) | 5 (31.2%) | 64 (64.6%) | 11 (42.3%) | ||||
| Female (%) | 27 (58.7%) | 11 (68.8%) | 35 (35.4%) | 15 (57.7%) | ||||
| Boston skin phototype, n (%) | NS | NS | NS | NS | ||||
| 2 (%) | 12 (26.1%) | 5 (31.2%) | 22 (22.2%) | 7 (26.9%) | ||||
| 3 (%) | 21 (67.4%) | 10 (62.5%) | 67 (67.7%) | 15 (57.7%) | ||||
| 4 (%) | 3 (6.5%) | 1 (6.3%) | 10 (10.1%) | 4 (15.4%) | ||||
| Medical history of AD | <0.001 | <0.001 | NS | NS | ||||
| continuous AD, n (%) | 27 (58.7%) | 0 (0%) | 34 (34.3%) | 0 (0%) | ||||
| intermittent AD *, n (%) | 19 (41.3%) | 16 (100%) | 65 (65.7%) | 26 (100%) | ||||
| Number of treatment sessions [median (range)] | 30 (12–66) | 18.5 (12–26) | <0.01 | 33 (16–51) | 24 (12–30) | <0.001 | NS | NS |
| Cumulative UV dose (J/cm2) [median (range)] | 1155.0 (360–3080) | 770 (230–1750) | <0.01 | 16.3 (0.6–30.8) | 11.3 (3.6–28.5) | 0.02 | ||
| Patients with an IGA 0/1 result | 21 (46%) | 12 (75%) | 0.014 | 42 (42%) | 19 (73.1%) | 0.037 | NS | NS |
| Patients with an IGA 0/1 persistent for at least 6 months | 15 (33%) | 11 (69%) | 0.012 | 28 (28%) | 18 (69.2%) | 0.016 | NS | NS |
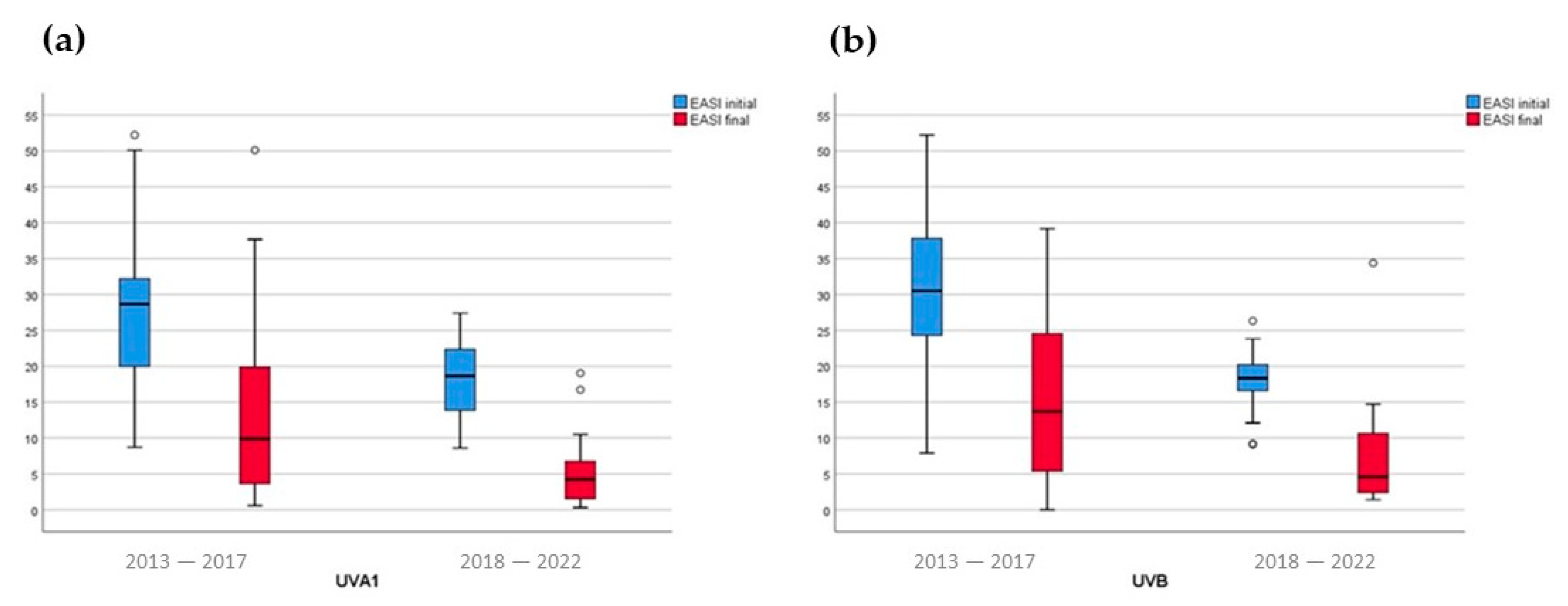
| Baseline median EASI (range) | 28.7 (8.7–52.2) | 18.7 (8.6–27.4) | <0.001 | 30.5 (7.9–52.2) | 18.4 (9.1–26.3) | <0.001 | NS | NS |
| Final median EASI (range) ** | 9.9 (0.6–50.1) | 4.3 (0.3–19.0) | 0.006 | 13.7 (0–39.2) | 4.6 (1.4–34.4) | <0.001 | NS | NS |
| Patients achieving EASI 90 | 4 (10.9%) | 5 (31.3%) | 0.027 | 11 (11%) | 9 (34.6%) | 0.041 | NS | NS |
| Patients achieving EASI 75 | 15 (32.6%) | 7 (43.8%) | 0.02 | 28 (28.3%) | 6 (30.8%) | NS | NS | NS |
| Patients with at least 1 adverse effect *** | 8 (17.4%) | 2 (12.5%) | NS | 0 | 0 | NS | NS | NS |
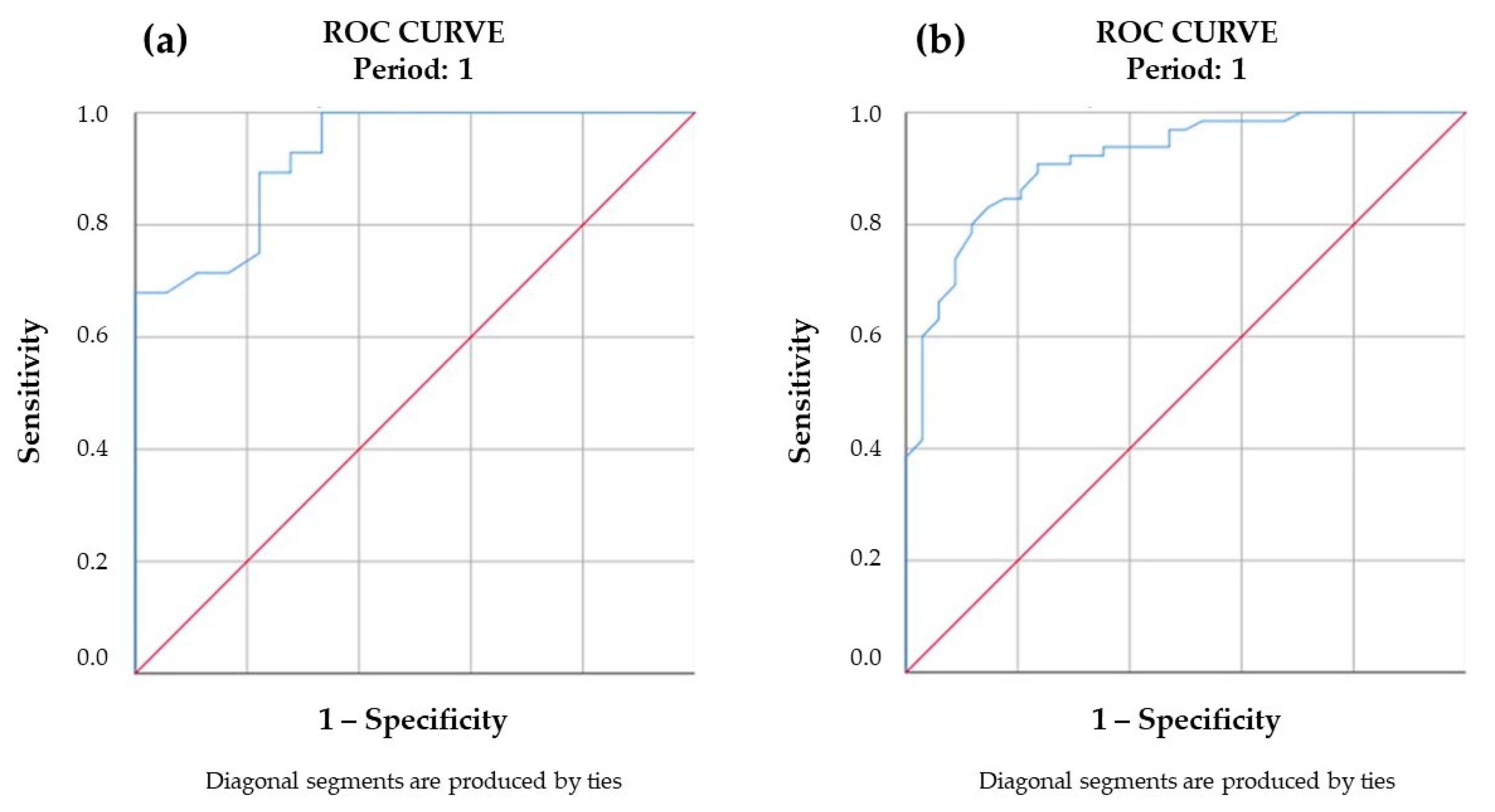
| Baseline EASI | Clinical Course | Treated Number of Patients | IGA 0/1 Persistent for at Least 6 Months | Rate (%) of Patients Achieving Persistent IGA 0/1 | p |
|---|---|---|---|---|---|
| Patients treated with medium-dose UVA1 phototherapy (n = 46) | |||||
| <24.4 | intermittent | 13 | 9 | 69.2% | <0.001 |
| <24.4 | continuous | 2 | 1 | 50% | |
| >24.5 | intermittent | 6 | 2 | 33.3% | |
| >24.5 | continuous | 25 | 3 | 12% | |
| Patients treated with NB-UVB phototherapy (n = 99) | |||||
| <24.7 | intermittent | 26 | 19 | 73.1% | <0.001 |
| <24.7 | continuous | 6 | 1 | 16.7% | |
| >24.8 | intermittent | 8 | 2 | 25.0% | |
| >24.8 | continuous | 59 | 6 | 10.2% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossi, M.; Damiani, C.; Arisi, M.; Tomasi, C.; Tonon, F.; Venturini, M.; Calzavara-Pinton, P. Definition of the Clinical Characteristics of Patients with Moderate and Severe Atopic Dermatitis for Whom Narrow-Band UVB (NB-UVB) and Medium-Dose UVA1 Phototherapies Are Still Valuable Treatment Options at the Age of Biologics. J. Clin. Med. 2023, 12, 3303. https://doi.org/10.3390/jcm12093303
Rossi M, Damiani C, Arisi M, Tomasi C, Tonon F, Venturini M, Calzavara-Pinton P. Definition of the Clinical Characteristics of Patients with Moderate and Severe Atopic Dermatitis for Whom Narrow-Band UVB (NB-UVB) and Medium-Dose UVA1 Phototherapies Are Still Valuable Treatment Options at the Age of Biologics. Journal of Clinical Medicine. 2023; 12(9):3303. https://doi.org/10.3390/jcm12093303
Chicago/Turabian StyleRossi, Mariateresa, Caterina Damiani, Mariachiara Arisi, Cesare Tomasi, Francesco Tonon, Marina Venturini, and Piergiacomo Calzavara-Pinton. 2023. "Definition of the Clinical Characteristics of Patients with Moderate and Severe Atopic Dermatitis for Whom Narrow-Band UVB (NB-UVB) and Medium-Dose UVA1 Phototherapies Are Still Valuable Treatment Options at the Age of Biologics" Journal of Clinical Medicine 12, no. 9: 3303. https://doi.org/10.3390/jcm12093303