

Use of Daridorexant among Patients with Chronic Insomnia: A Retrospective Observational Analysis

Abstract
:1. Introduction
2. Materials and Methods
- Severity of sleep onset;
- Sleep maintenance;
- Early morning awakening problems;
- Sleep dissatisfaction;
- Interference of sleep difficulties with daytime functioning;
- Noticeability of sleep problems by others;
- Distress caused by difficulty sleeping.
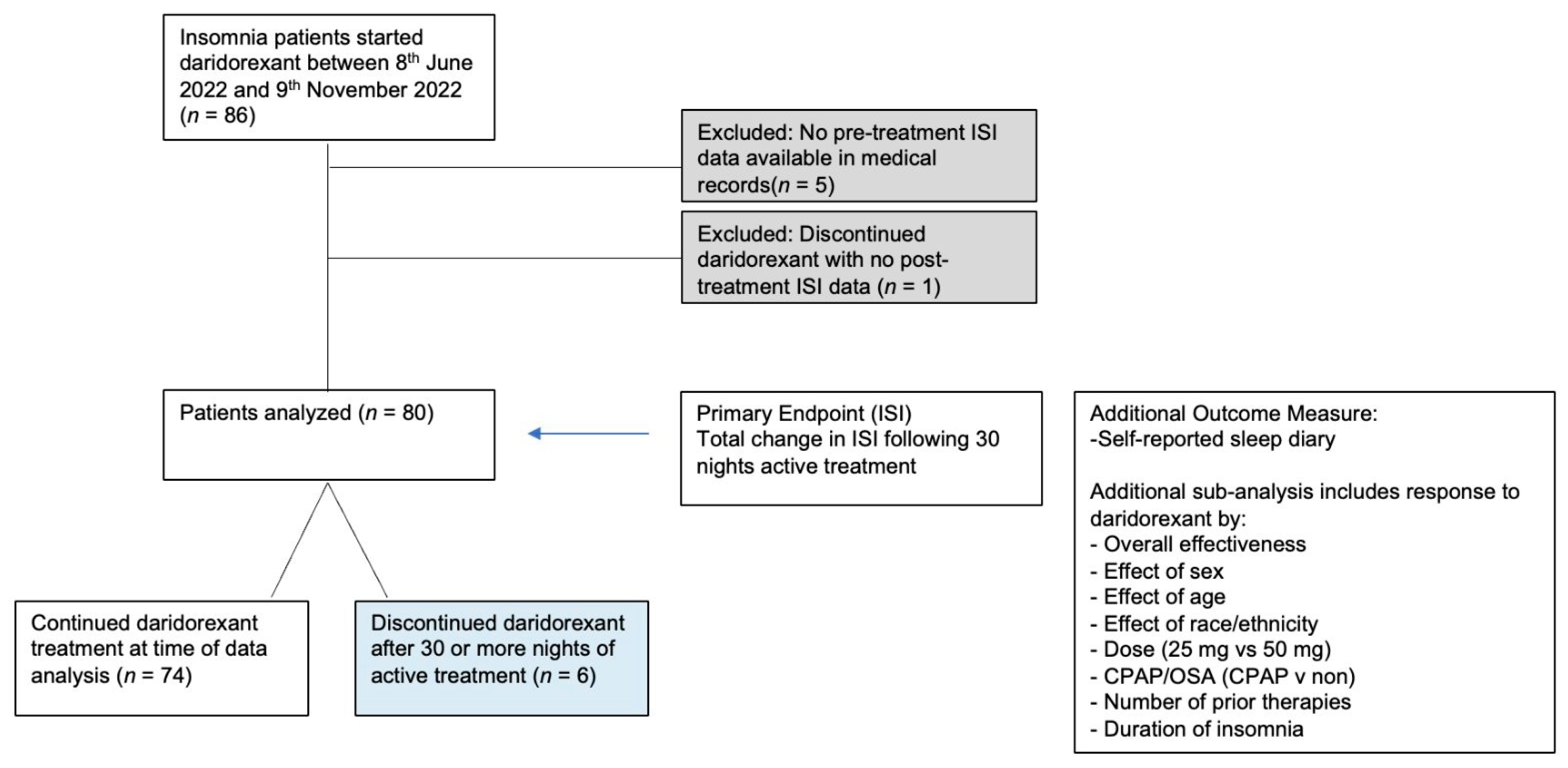
2.1. Patient Population
2.2. Sample Characteristics
- Subjective measures of daytime function, including fatigue, sleepiness, concentration, mood, and anxiety.
- Subjective measures of sleep, including total sleep time (TST), sleep onset latency (SOL), wake after sleep onset (WASO) and sleep efficiency (SE).
2.3. Statistical Analysis
3. Results
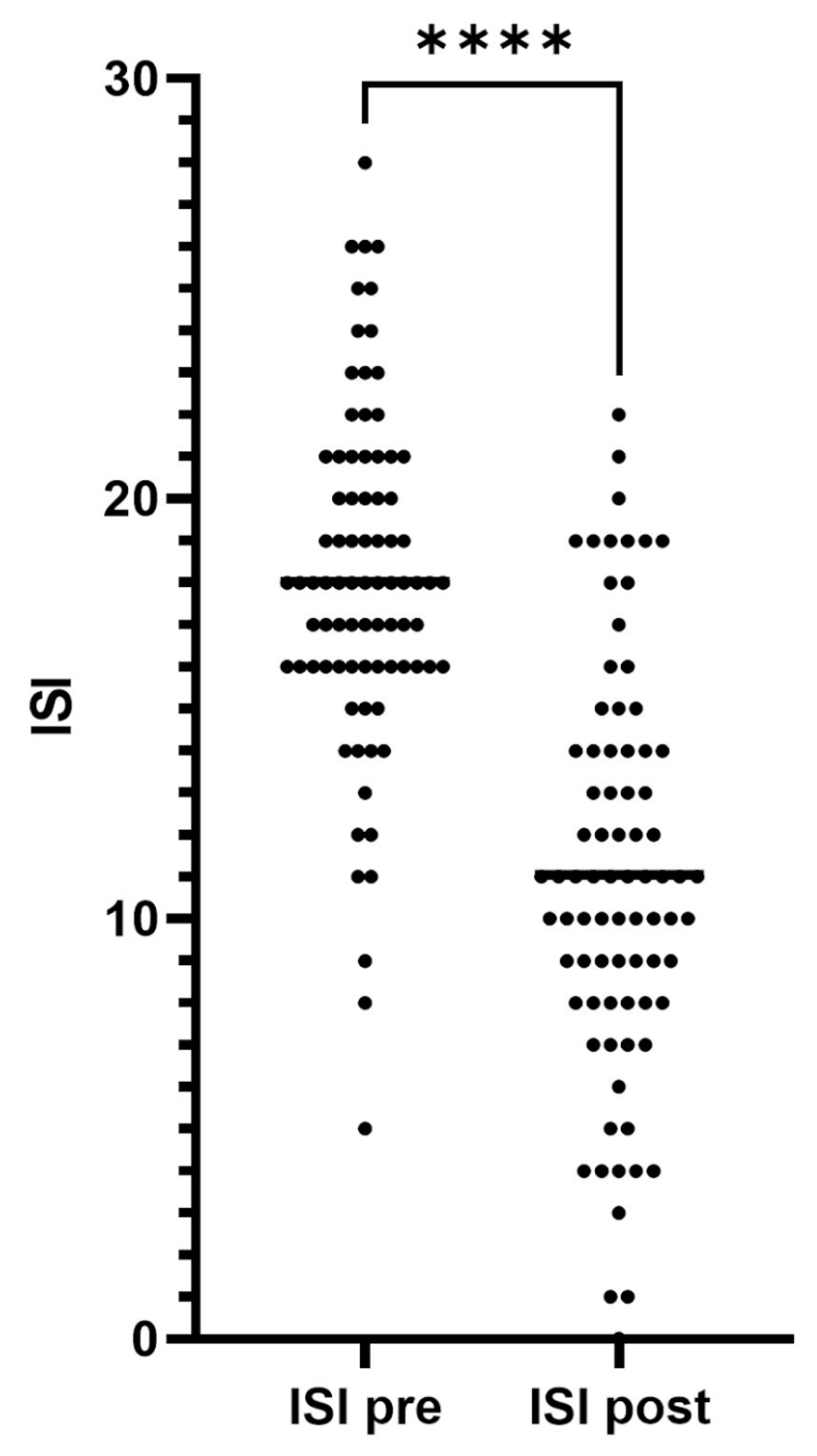
3.1. Insomnia Severity Index (ISI) Data
3.1.1. ISI Scores before and after 30 Days or More of Daridorexant Treatment
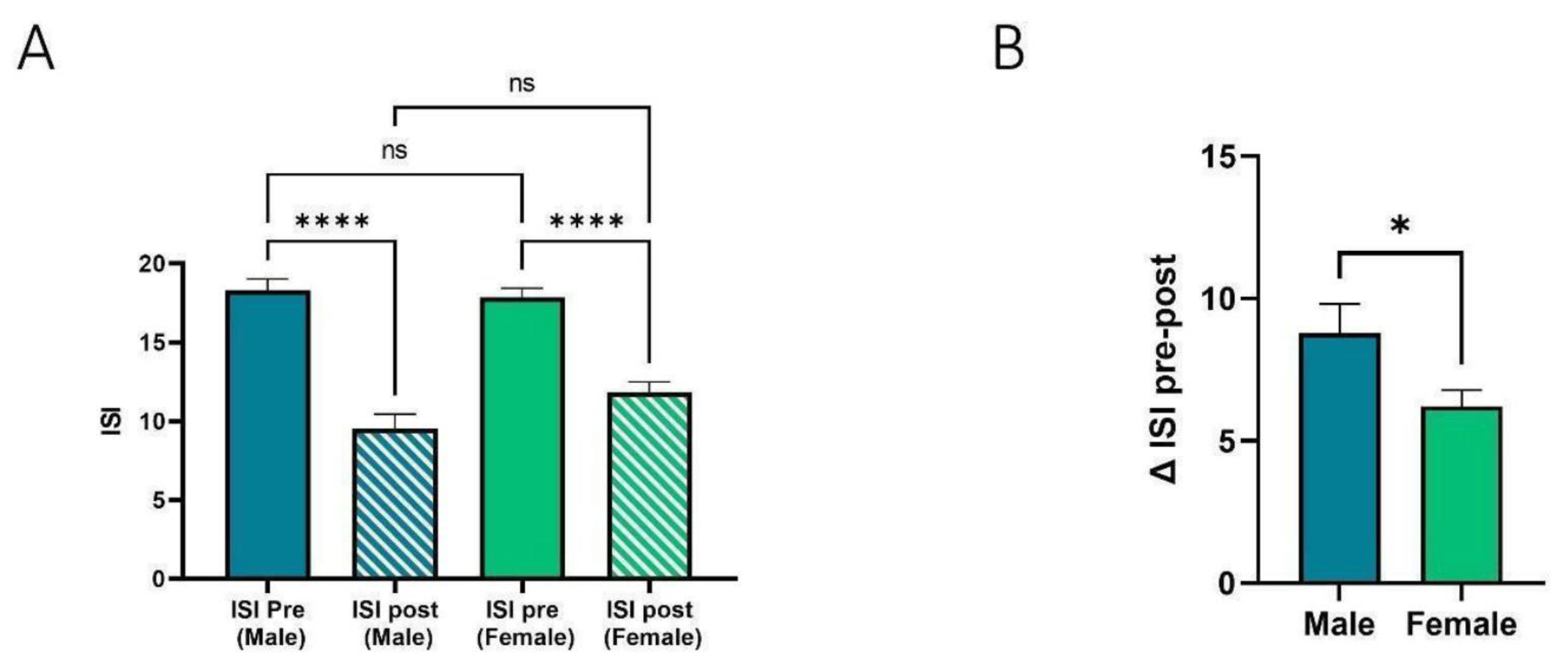
3.1.2. Effect of Sex on ISI
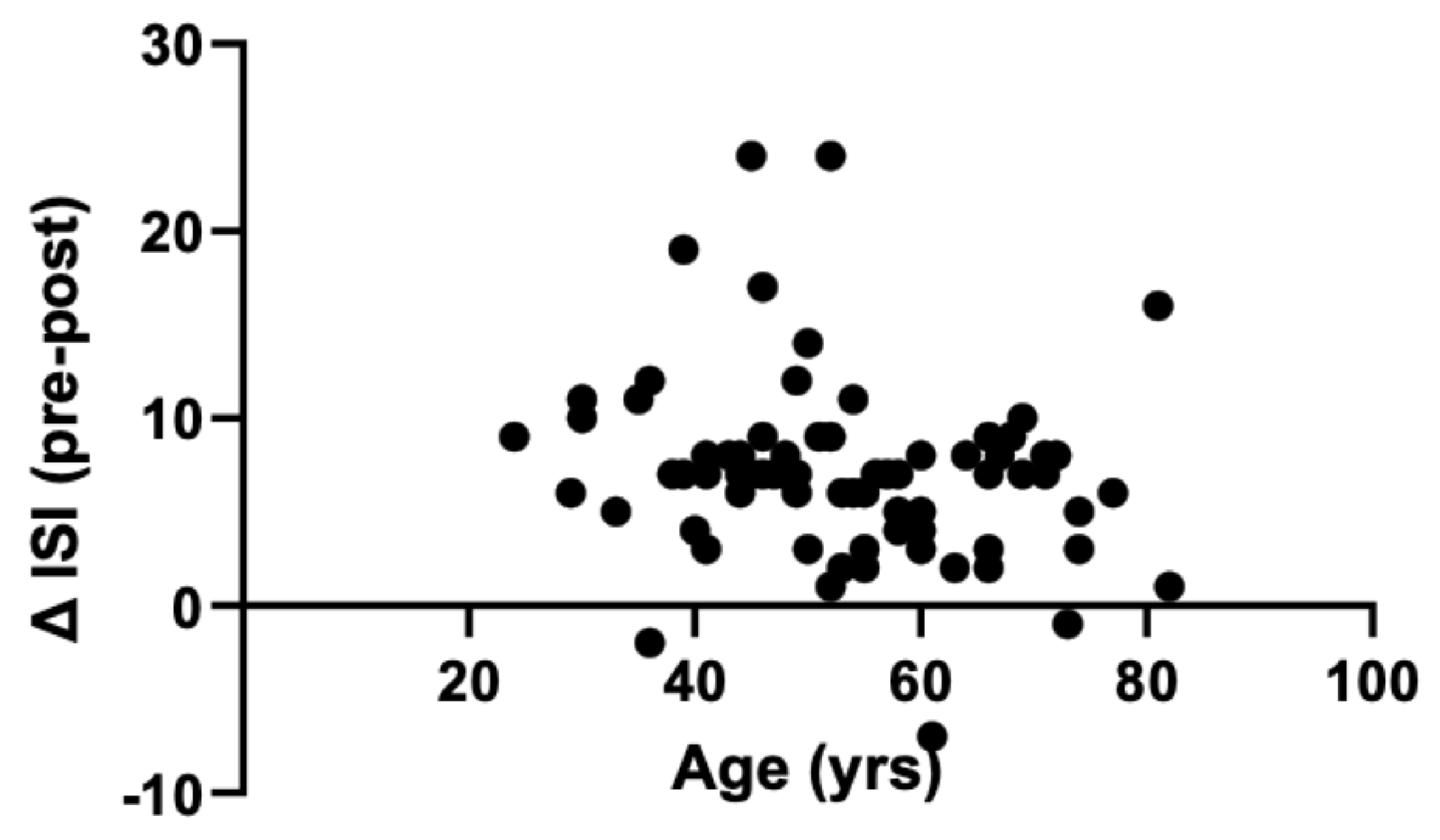
3.1.3. Effect of Age on ISI
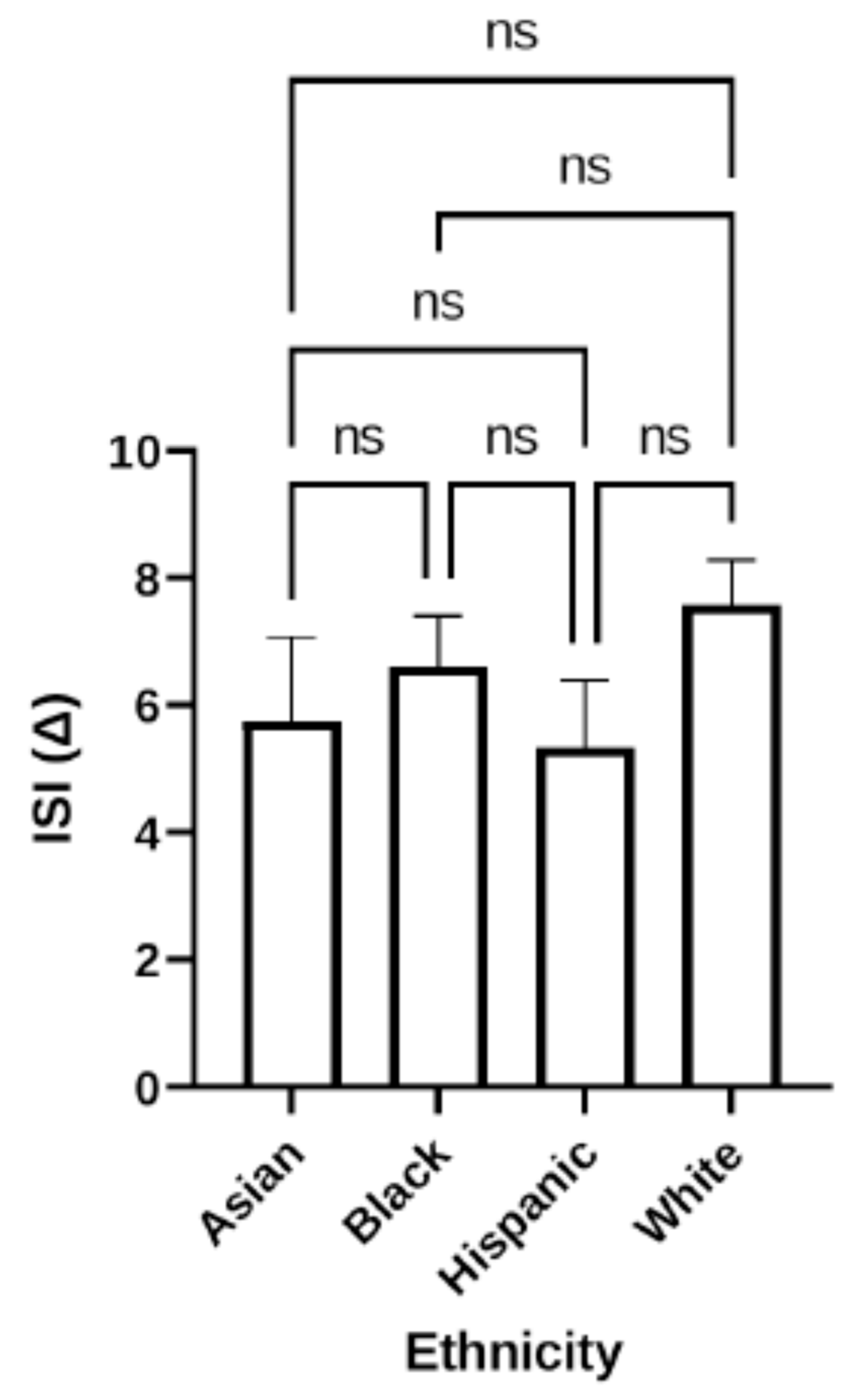
3.1.4. Effect of Race/Ethnicity on ISI
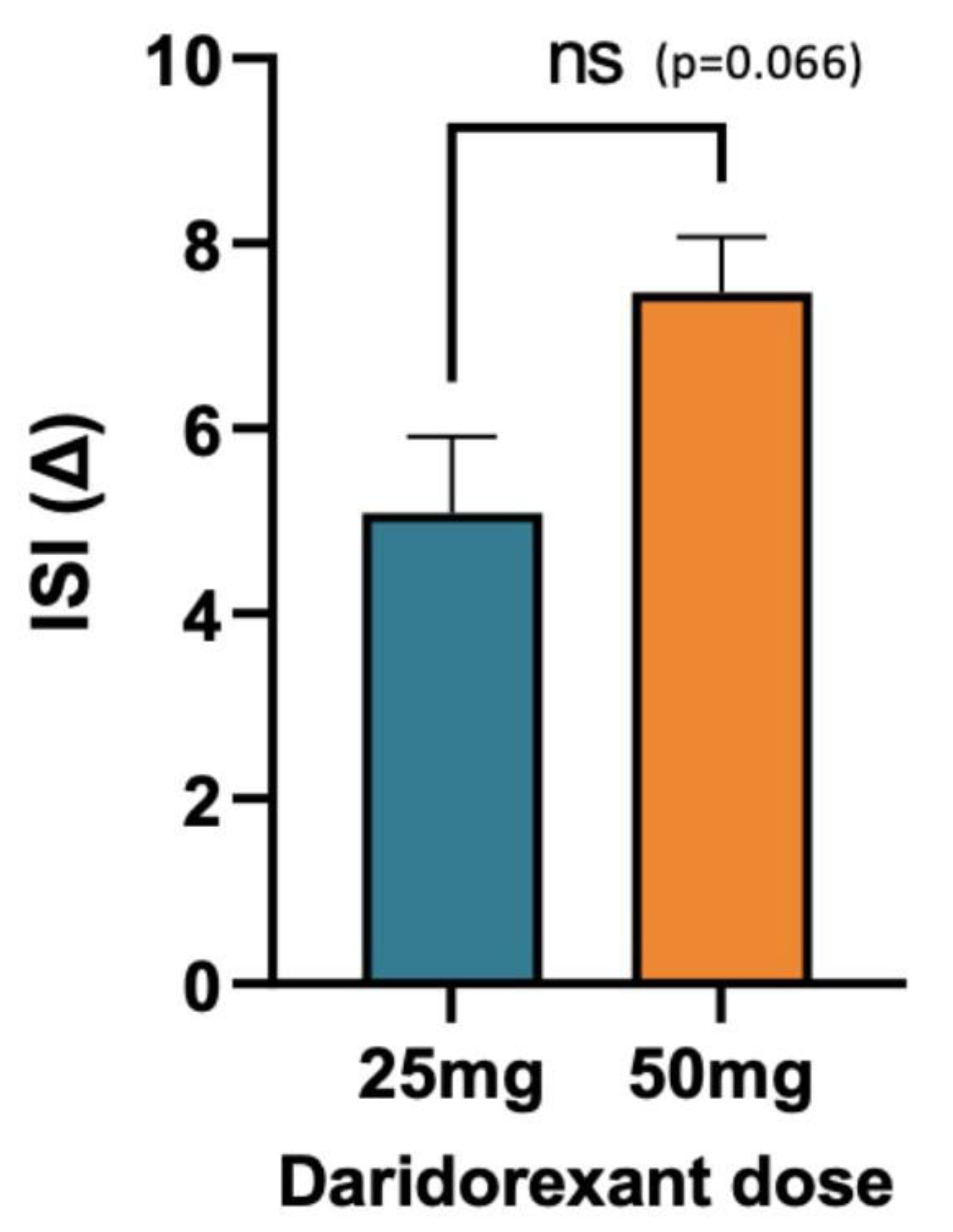
3.1.5. Impact of Dose on ISI
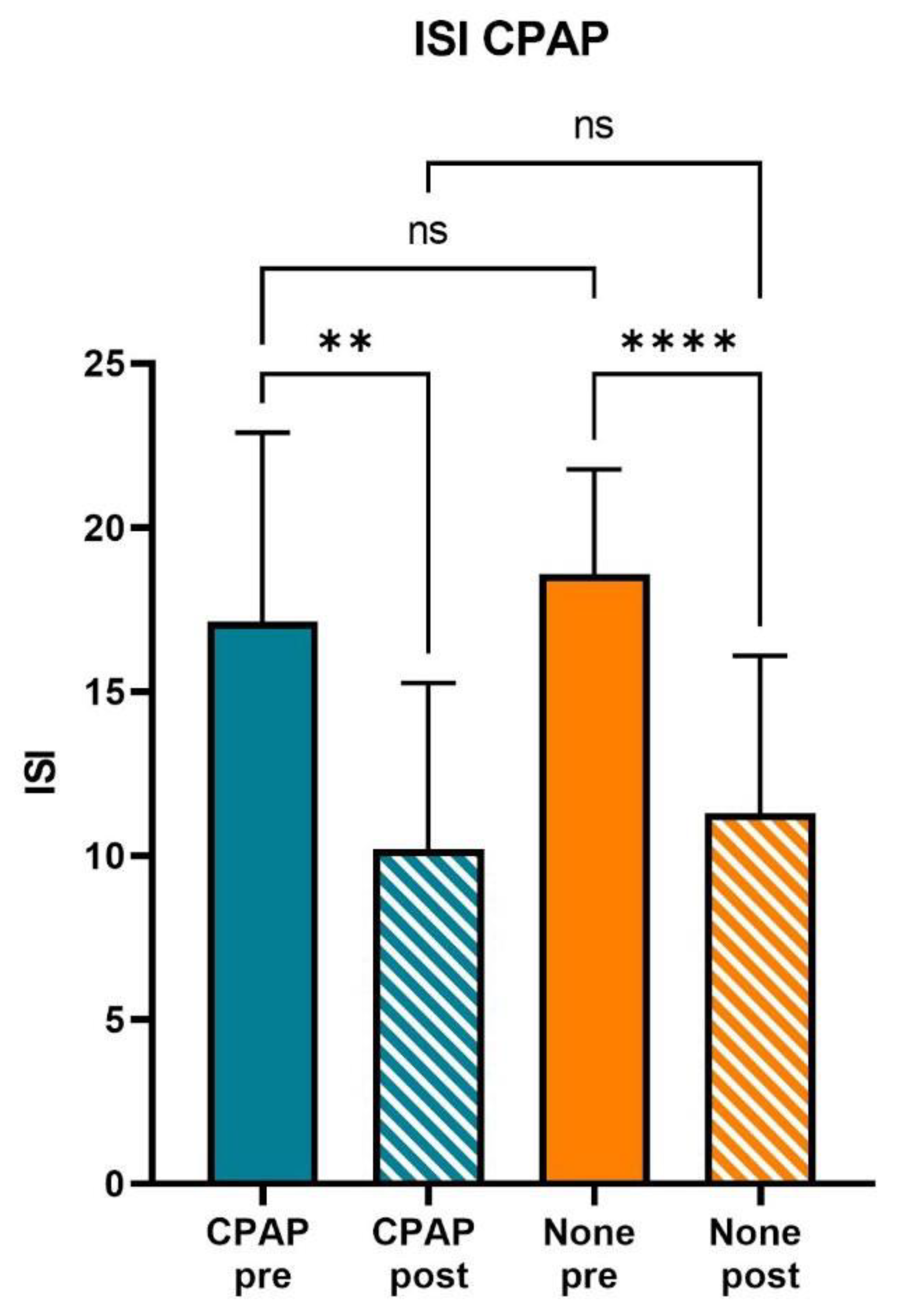
3.1.6. Effect of CPAP Therapy
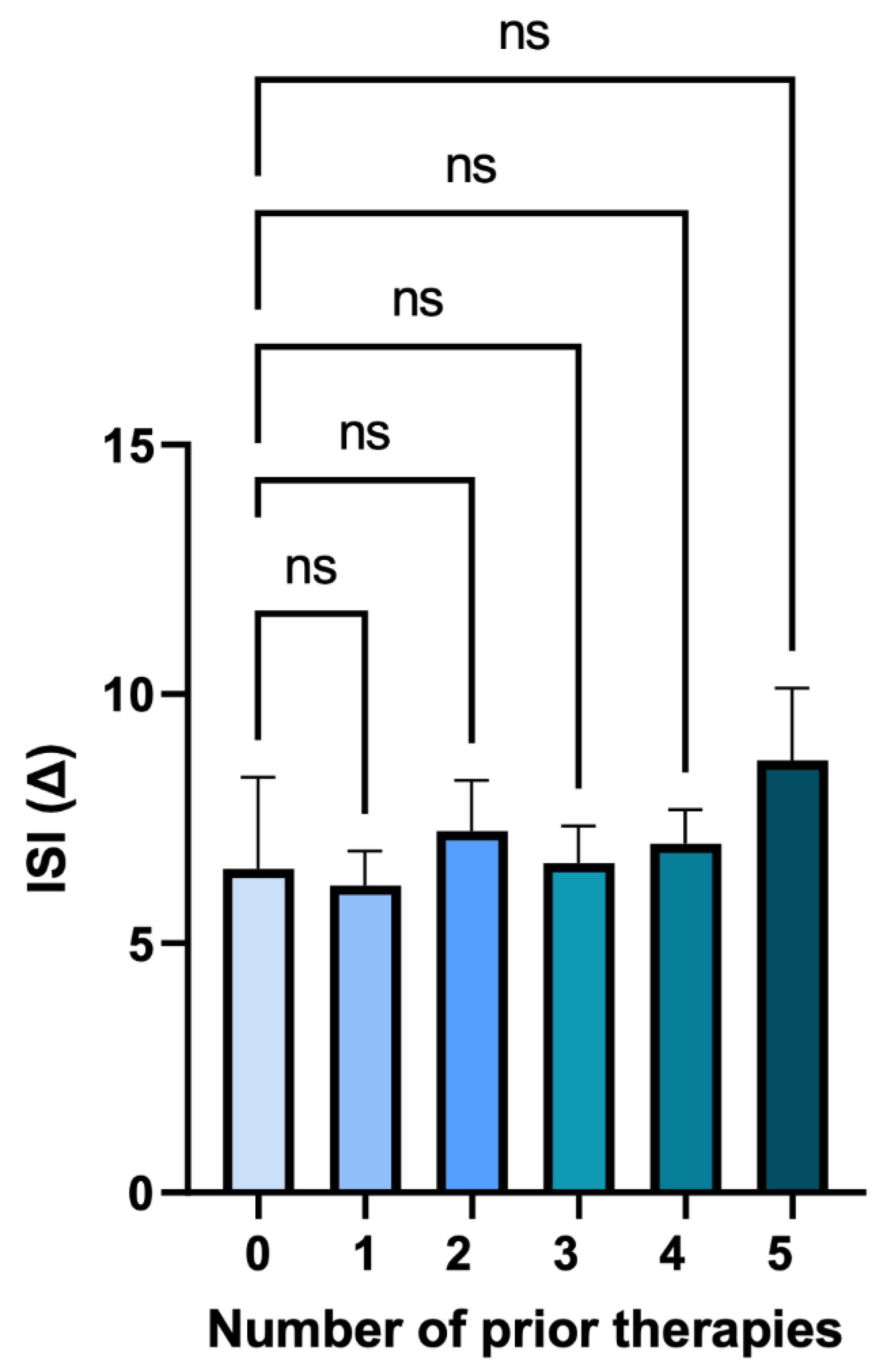
3.1.7. Number of Prior Therapies
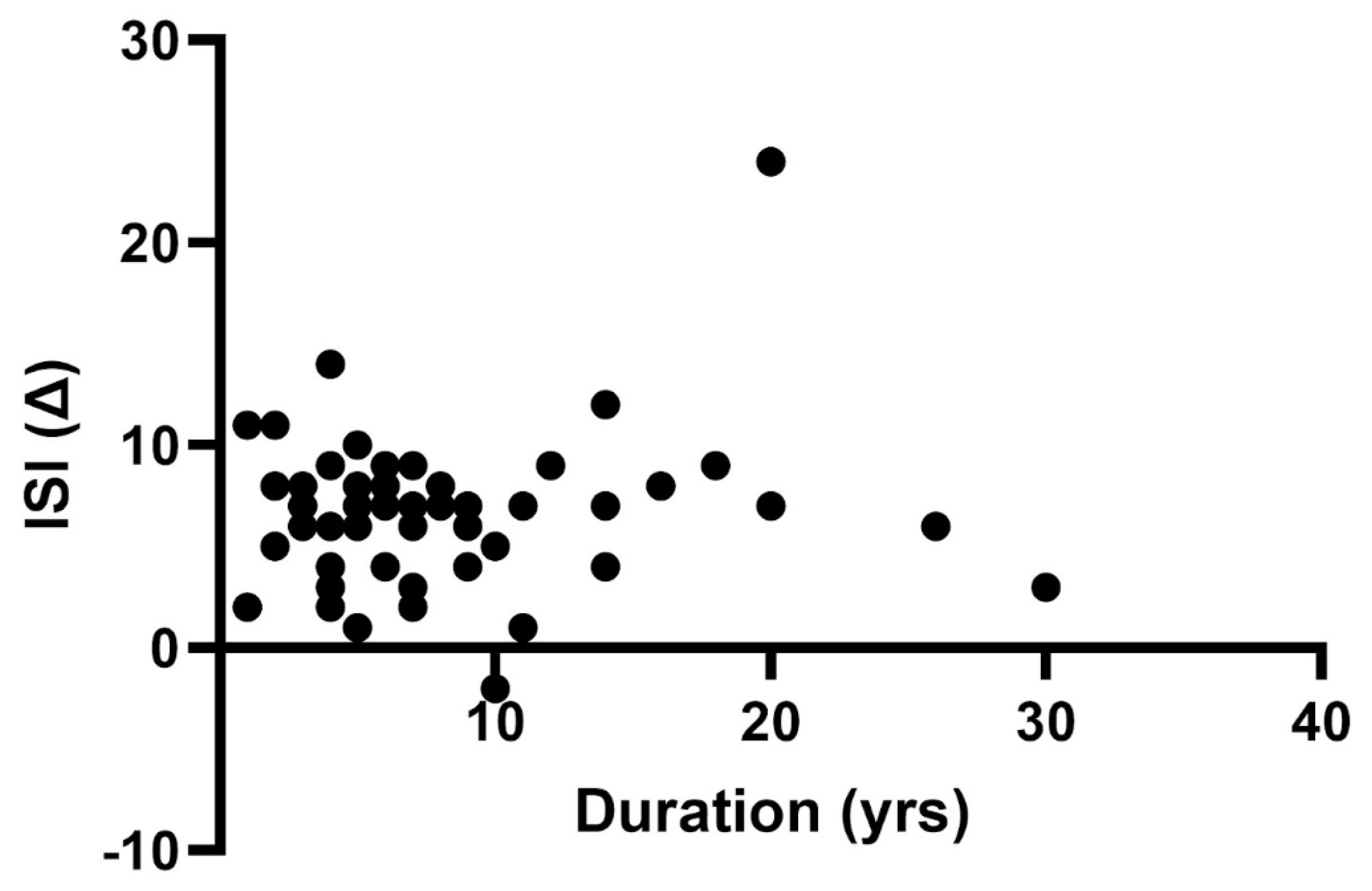
3.1.8. Prior Duration of Insomnia Treatment
3.2. Subjective Measures
3.2.1. Subjective Measures of Daytime Function
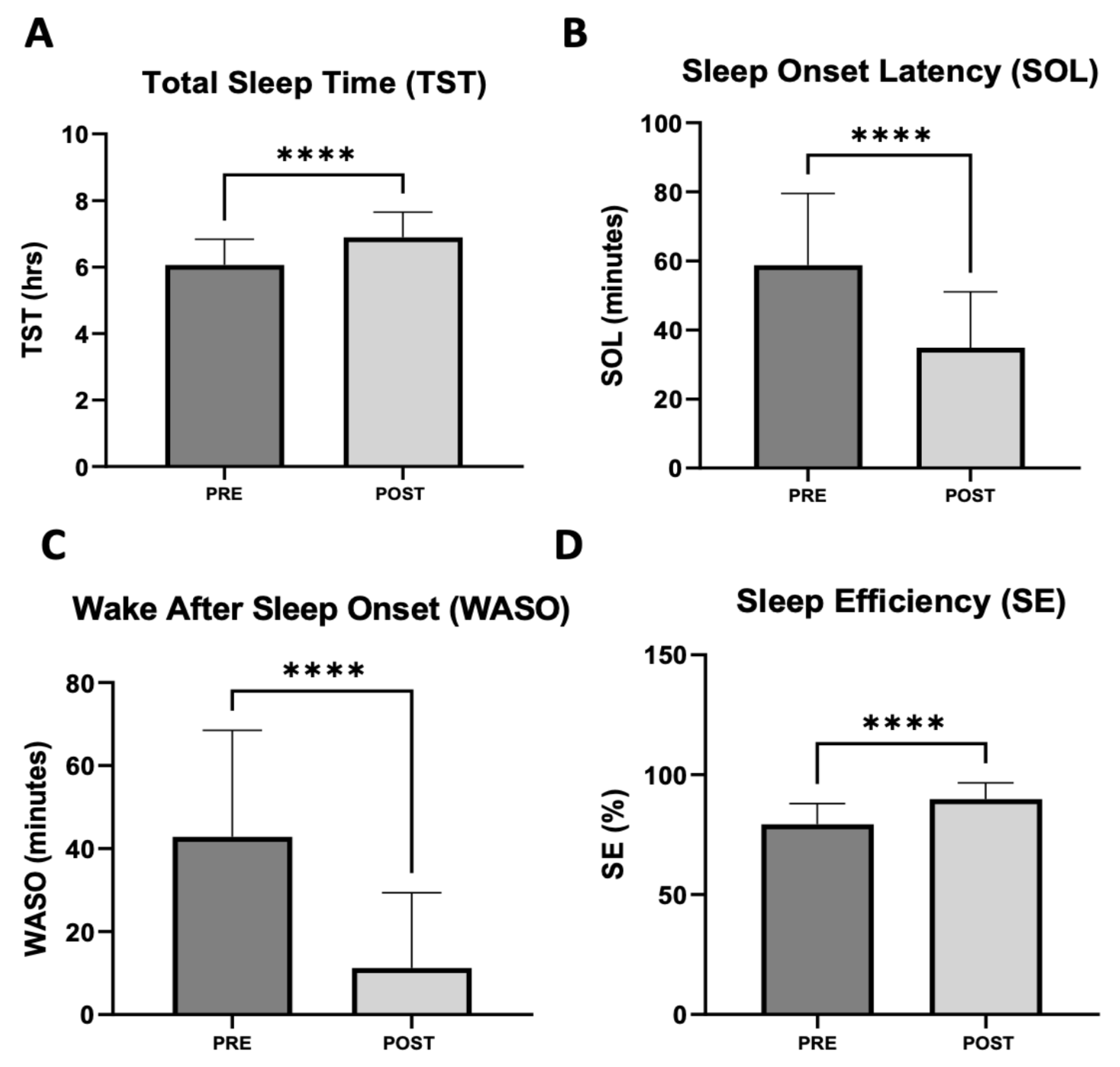
3.2.2. Subjective Sleep Assessment
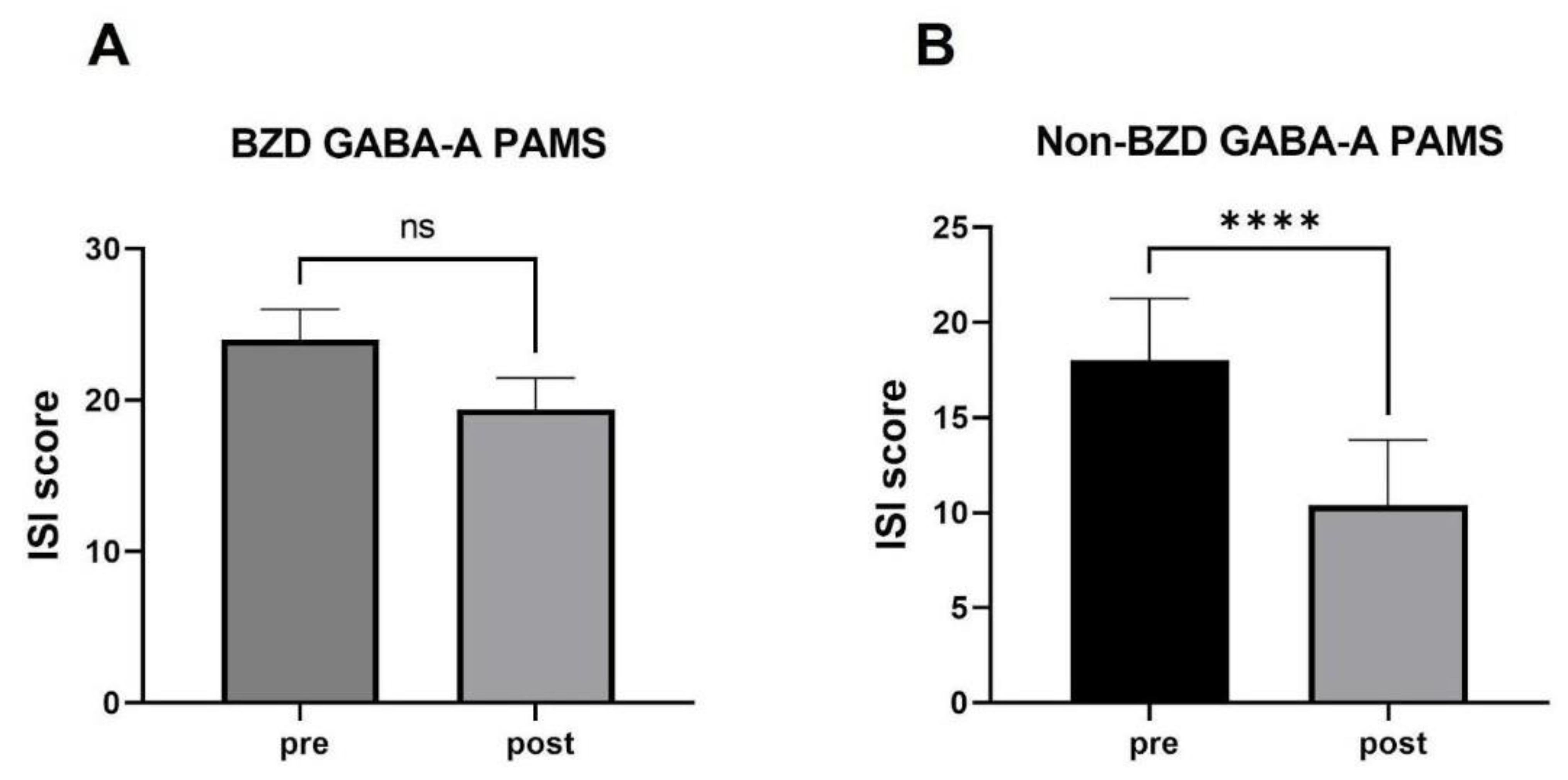
3.2.3. Sleep Assessment in Patients Treated with BZD GABA-A PAMs versus non-BZD GABA-A PAMs Prior to Switching to Daridorexant
3.3. Changes in ISI and Subjective Sleep Measures for Patients Who Discontinued Medication
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer Statement
References
- American Academy of Sleep Medicine. The International Classification of Sleep Disorders, 3rd ed.; (ICSD-3); American Academy of Sleep Medicine: Darien, IL, USA, 2014. [Google Scholar]
- Sateia, M.J.; Buysse, D.J.; Krystal, A.D.; Neubauer, D.N.; Heald, J.L. Clinical Practice Guideline for the Pharmacologic Treatment of Chronic Insomnia in Adults: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 307–349. [Google Scholar] [CrossRef] [PubMed]
- Reuben, C.; Elgaddal, N.; Black, L.I. Sleep Medication Use in Adults Aged 18 and Over: United States, 2020. NCHS Data Brief, no 462. Hyattsville, MD: National Center for Health Statistics. 2023. Available online: https://www.cdc.gov/nchs/data/databriefs/db462.pdf (accessed on 2 February 2023).
- Sallard, E.; Letourneur, D.; Legendre, P. Electrophysiology of ionotropic GABA receptors. Cell Mol. Life Sci. 2021, 78, 5341–5370. [Google Scholar] [CrossRef] [PubMed]
- Möhler, H.; Fritschy, J.M.; Rudolph, U. A new benzodiazepine pharmacology. J. Pharmacol. Exp. Ther. 2002, 300, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Rush, C.R.; Frey, J.M.; Griffiths, R.R. Zaleplon and triazolam in humans: Acute behavioral effects and abuse potential. Psychopharmacology 1999, 145, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, R.R.; Johnson, M.W. Relative abuse liability of hypnotic drugs: A conceptual framework and algorithm for differentiating among compounds. J. Clin. Psychiatry 2005, 66 (Suppl. S9), 31–41. [Google Scholar]
- Lader, M. Benzodiazepines revisited—Will we ever learn? Addiction 2011, 106, 2086–2109. [Google Scholar] [CrossRef]
- Schepis, T.S. Age cohort differences in the nonmedical use of prescription zolpidem: Findings from a nationally representative sample. Addict. Behav. 2014, 39, 1311–1317. [Google Scholar] [CrossRef]
- Schepis, T.S.; Teter, C.J.; Simoni-Wastila, L.; McCabe, S.E. Prescription tranquilizer/sedative misuse prevalence and correlates across age cohorts in the US. Addict. Behav. 2018, 87, 24–32. [Google Scholar] [CrossRef]
- Modesto-Lowe, V.; Harabasz, A.K.; Walker, S.A. Quetiapine for primary insomnia: Consider the risks. Cleve Clin. J. Med. 2021, 88, 286–294. [Google Scholar] [CrossRef]
- Holbrook, A.M.; Crowther, R.; Lotter, A.; Cheng, C.; King, D. Meta-analysis of benzodiazepine use in the treatment of insomnia. CMAJ 2000, 162, 225–233. [Google Scholar]
- American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J. Am. Geriatr. Soc. 2012, 60, 616–631. [Google Scholar] [CrossRef]
- Wilt, T.J.; MacDonald, R.; Brasure, M.; Olson, C.M.; Carlyle, M.; Fuchs, E.; Khawaja, I.S.; Diem, S.; Koffel, E.; Ouellette, J.; et al. Pharmacologic Treatment of Insomnia Disorder: An Evidence Report for a Clinical Practice Guideline by the American College of Physicians. Ann. Intern. Med. 2016, 165, 103–112. [Google Scholar] [CrossRef]
- Amari, D.T.; Juday, T.; Frech, F.H.; Wang, W.; Wu, Z.; Atkins, N., Jr.; Wickwire, E.M. Falls, healthcare resources and costs in older adults with insomnia treated with zolpidem, trazodone, or benzodiazepines. BMC Geriatr. 2022, 22, 484. [Google Scholar] [CrossRef]
- FDA Drug Safety Communication: FDA Adds Boxed Warning for Risk of Serious Injuries Caused by Sleepwalking with Certain Prescription Insomnia Medicines. 2019. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-adds-boxed-warning-risk-serious-injuries-caused-sleepwalking-certain-prescription-insomnia (accessed on 2 February 2023).
- Lavigne, J.E.; Hur, K.; Kane, C.; Au, A.; Bishop, T.M.; Pigeon, W.R. Prescription Medications for the Treatment of Insomnia and Risk of Suicide Attempt: A Comparative Safety Study. J. Gen. Intern. Med. 2019, 34, 1554–1563. [Google Scholar] [CrossRef]
- Roach, M.; Juday, T.; Tuly, R.; Chou, J.W.; Jena, A.B.; Doghramji, P.P. Challenges and opportunities in insomnia disorder. Int. J. Neurosci. 2021, 131, 1058–1065. [Google Scholar] [CrossRef]
- Herring, W.J.; Snyder, E.; Budd, K.; Hutzelmann, J.; Snavely, D.; Liu, K.; Lines, C.; Roth, T.; Michelson, D. Orexin receptor antagonism for treatment of insomnia: A randomized clinical trial of suvorexant. Neurology 2012, 79, 2265–2274. [Google Scholar] [CrossRef]
- Freeman, L.R.; Aston-Jones, G. Activation of medial hypothalamic orexin neurons during a Go/No-Go task. Brain Res. 2020, 1731, 145928. [Google Scholar] [CrossRef]
- Alger, S.E.; Stekl, E.; Allotey-Addo, S.; Klosterman, G.; Balkin, T.J. The Role of Pharmacological Interventions for Sleep Deprivation and Restriction, Reference Module in Neuroscience and Biobehavioral Psychology; Elsevier: Amsterdam, The Netherlands, 2021; ISBN 9780128093245. [Google Scholar] [CrossRef]
- Merck Sharp & Dohme. United States Prescribing Information: BELSOMRA® (Suvorexant). 2014. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/204569s000lbledt.pdf (accessed on 2 February 2023).
- Sun, H.; Kennedy, W.P.; Wilbraham, D.; Lewis, N.; Calder, N.; Li, X.; Ma, J.; Yee, K.L.; Ermlich, S.; Mangin, E.; et al. Effects of suvorexant, an orexin receptor antagonist, on sleep parameters as measured by polysomnography in healthy men. Sleep 2013, 36, 259–267. [Google Scholar] [CrossRef]
- Roth, T.; Rosenberg, R.; Morin, C.M.; Yardley, J.; Pinner, K.; Perdomo, C.; Atkins, N., Jr.; Pappadopulos, E.; Malhotra, M.; Moline, M. Impact of lemborexant treatment on insomnia severity: Analyses from a 12-month study of adults with insomnia disorder. Sleep Med. 2022, 90, 249–257. [Google Scholar] [CrossRef]
- Dauvilliers, Y.; Zammit, G.; Fietze, I.; Mayleben, D.; Seboek Kinter, D.; Pain, S.; Hedner, J. Daridorexant, a New Dual Orexin Receptor Antagonist to Treat Insomnia Disorder. Ann. Neurol. 2020, 87, 347–356. [Google Scholar] [CrossRef]
- Mignot, E.; Mayleben, D.; Fietze, I.; Leger, D.; Zammit, G.; Bassetti, C.L.A.; Pain, S.; Kinter, D.S.; Roth, T.; investigators. Safety and efficacy of daridorexant in patients with insomnia disorder: Results from two multicentre, randomised, double-blind, placebo-controlled, phase 3 trials. Lancet Neurol. 2022, 21, 125–139, Erratum in Lancet Neurol. 2022, 21, e6. [Google Scholar] [CrossRef] [PubMed]
- Leger, D.; Fietze, I.; Pain, S.; Seboek Kinter, D.; Flamion, B.; Mignot, E. 348 Absence of Withdrawal Symptoms and Rebound Insomnia Upon Discontinuation of Daridorexant in Patients with Insomnia. Sleep 2021, 44, A139. [Google Scholar] [CrossRef]
- Roth, T.; Zammit, G.; Mignot, E.; Leger, D.; Bassetti, C.; Pain, S.; Seboek Kinter, D. Daridorexant, a novel dual orexin receptor antagonist, delivers significant improvement in sleep parameters and daytime function for patients with insomnia disorder. J. SleepRes. 2020, 29 (Suppl. S1), 152. [Google Scholar] [CrossRef]
- Kunz, D.; Dauvilliers, Y.; Benes, H.; García-Borreguero, D.; Plazzi, G.; Seboek Kinter, D.; Coloma, P.; Rausch, M.; Sassi-Sayadi, M.; Thein, S. Long-Term Safety and Tolerability of Daridorexant in Patients with Insomnia Disorder. CNS Drugs, 2022; Epub ahead of print. [Google Scholar] [CrossRef]
- Morin, C.M. Insomnia: Psychological Assessment and Management; Guilford Press: New York, NY, USA, 1993. [Google Scholar]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Morin, C.M.; Belleville, G.; Bélanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef]
- Yang, M.; Morin, C.M.; Schaefer, K.; Wallenstein, G.V. Interpreting score differences in the Insomnia Severity Index: Using health-related outcomes to define the minimally important difference. Curr. Med. Res. Opin. 2009, 25, 2487–2494. [Google Scholar] [CrossRef]
- Suzuki, H.; Hibino, H. Characteristics of patients who were able to switch from benzodiazepine hypnotics to lemborexant. SAGE Open Med. 2021, 9, 20503121211037903. [Google Scholar] [CrossRef]
- De Crescenzo, F.; D’Alò, G.L.; Ostinelli, E.G.; Ciabattini, M.; Di Franco, V.; Watanabe, N.; Kurtulmus, A.; Tomlinson, A.; Mitrova, Z.; Foti, F.; et al. Comparative effects of pharmacological interventions for the acute and long-term management of insomnia disorder in adults: A systematic review and network meta-analysis. Lancet 2022, 400, 170–184. [Google Scholar] [CrossRef]
- Sateia, M.J. International classification of sleep disorders-third edition: Highlights and modifications. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef]
- Fava, M.; Asnis, G.M.; Shrivastava, R.K.; Lydiard, B.; Bastani, B.; Sheehan, D.V.; Roth, T. Improved insomnia symptoms and sleep-related next-day functioning in patients with comorbid major depressive disorder and insomnia following concomitant zolpidem extended-release 12.5 mg and escitalopram treatment: A randomized controlled trial. J. Clin. Psychiatry 2011, 72, 914–928. [Google Scholar] [CrossRef]
- Kärppä, M.; Yardley, J.; Pinner, K.; Filippov, G.; Zammit, G.; Moline, M.; Perdomo, C.; Inoue, Y.; Ishikawa, K.; Kubota, N. Long-term efficacy and tolerability of lemborexant compared with placebo in adults with insomnia disorder: Results from the phase 3 randomized clinical trial SUNRISE 2. Sleep 2020, 43, zsaa123. [Google Scholar] [CrossRef]
- Benz, F.; Knoop, T.; Ballesio, A.; Bacaro, V.; Johann, A.F.; Rücker, G.; Feige, B.; Riemann, D.; Baglioni, C. The efficacy of cognitive and behavior therapies for insomnia on daytime symptoms: A systematic review and network meta-analysis. Clin. Psychol. Rev. 2020, 80, 101873. [Google Scholar] [CrossRef]
- Hintze, J.P.; Edinger, J.D. Hypnotic Discontinuation in Chronic Insomnia. Sleep Med. Clin. 2022, 17, 523–530. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Descriptor | Patient | Patient | Total Sample |
|---|---|---|---|
| Cohort 1 | Cohort 2 | Population | |
| Number of Subjects Analyzed | 59 | 21 | 80 |
| Male | 20 | 8 | 28 |
| Female | 39 | 13 | 52 |
| Age range (years) | 24–82 | 30–74 | 24–82 |
| Mean age (SD) | 53.1 (12.6) | 53.9 (14.3) | 53.5 (13.0) |
| Age 64 and under | 46 | 15 | 61 (76.3%) |
| Age 65 and older | 13 | 6 | 19 (23.8%) |
| Race/Ethnicity | |||
| Asian | 4 | 0 | 4 |
| Black | 8 | 2 | 10 |
| Hispanic | 8 | 1 | 9 |
| White | 39 | 18 | 57 |
| Insomnia Severity Index (ISI) score | |||
| Mean pre-daridorexant | 18.1 | 18.0 | 18.0 |
| Range (SD) | 9–26 (2.8) | 5–28 (5.3) | 5–28 (4.1) |
| Mean post-30-night daridorexant | 11.3 | 10.7 | 11.0 |
| Range (SD) | 4–22 (3.8) | 0–20 (6.4) | 0–22 (4.9) |
| Mean within-patient change in ISI | −6.8 | −7.3 | −7.0 |
| Range (SD) | 1–14 (2.7) | −7–24 (8.1) | −7–24 (4.7) |
| Number of Subjects Reporting | % Total Subjects (of 80) | Subjective Measures of Daytime Function Pre-Treatment | Number of Subjects Reporting | % Total Subjects (of 80) | Subjective Measures of Daytime Function Post-Treatment |
|---|---|---|---|---|---|
| 36 | 45.0 | hypersomnolence/severe to moderate sleepiness | 37 | 46.2 | fatigue/sleepiness improved |
| 27 | 33.7 | daytime fatigue | 26 | 32.5 | fatigue/sleepiness resolved/nearly resolved |
| 26 | 32.5 | poor concentration | 10 | 12.5 | increased alertness |
| 9 | 11.3 | depression | 5 | 6.3 | anxiety/depression improved |
| 4 | 5.0 | anxiety | 5 | 6.3 | no change in symptoms |
| 4 | 5.0 | none | 4 | 5.0 | no change/no symptoms |
| Insomnia Severity Index | Subjective Measures of Sleep | ||||||
|---|---|---|---|---|---|---|---|
| Patient | Pre- Treatment ISI | Post- Treatment ISI | Improvement in ISI | Improvement in TST (min) | Improvement in SOL (min) | Improvement in WASO (min) | Improvement in SE (%) |
| 1 | 26 | 21 | 5 | 24 | 30 | 20 | 12 |
| 2 | 22 | 19 | 3 | 30 | 30 | 0 | 11 |
| 3 | 21 | 19 | 2 | 60 | 30 | 30 | 12 |
| 4 | 26 | 22 | 4 | 30 | 0 | 30 | 7 |
| 5 | 21 | 19 | 2 | - | - | - | - |
| 6 | 22 | 18 | 4 | - | - | - | - |
| MEAN | 23.0 | 19.7 | 3.3 | 36 | 23 | 20 | 10.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Williams, S.G.; Rodriguez-Cué, D. Use of Daridorexant among Patients with Chronic Insomnia: A Retrospective Observational Analysis. J. Clin. Med. 2023, 12, 3240. https://doi.org/10.3390/jcm12093240
Williams SG, Rodriguez-Cué D. Use of Daridorexant among Patients with Chronic Insomnia: A Retrospective Observational Analysis. Journal of Clinical Medicine. 2023; 12(9):3240. https://doi.org/10.3390/jcm12093240
Chicago/Turabian StyleWilliams, Scott G., and Domingo Rodriguez-Cué. 2023. "Use of Daridorexant among Patients with Chronic Insomnia: A Retrospective Observational Analysis" Journal of Clinical Medicine 12, no. 9: 3240. https://doi.org/10.3390/jcm12093240