
The Role of Angiogenesis Targeted Therapies in Metastatic Advanced Gastric Cancer: A Narrative Review


Abstract
:1. Introduction
2. History of Anti-Angiogenic Therapy
Signal Transduction via VEGF-Related Pathways
3. Clinical Trials for the Treatment of Patients with AGC
3.1. Application of Bev in the Treatment of Patients with AGC
3.2. Ram Was the First Approved Anti-Angiogenic Agent for AGC Treatment
3.3. Rechallenge of Anti-VEGF Therapy in First-Line Treatment
3.4. Combination Therapy with Ram and Nanoparticle Albumin-Bound (nab)-PTX
3.5. Combination Therapy with IRI
3.6. Combination Therapy with Trifluridine/Tipiracil (FTD/TPI)
3.7. Multikinase Inhibitors
4. Anti-Angiogenic Therapy with Immunotherapy
4.1. Ramucirumab Plus Anti-PD1/PD-L1 Therapy without Cytotoxic Agents
4.2. Multikinase Inhibitor with Anti-PD-1 Therapy without Cytotoxic Agents
4.3. Ram Plus Chemotherapy with Immunotherapy
4.4. Therapeutic Development of Multikinase Inhibitors and Immunotherapy in the Frontline
5. Conclusions and Future Perspectives

Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Glimelius, B.; Ekström, K.; Hoffman, K.; Graf, W.; Sjödén, P.O.; Haglund, U.; Svensson, C.; Enander, L.K.; Linné, T.; Sellsröm, H.; et al. Randomized comparison between chemotherapy plus best supportive care with best supportive care in advanced gastric cancer. Ann. Oncol. 1997, 8, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, W.; Narahara, H.; Hara, T.; Takagane, A.; Akiya, T.; Takagi, M.; Miyashita, K.; Nishizaki, T.; Kobayashi, O.; Takiyama, W.; et al. S-1 plus cisplatin versus S-1 alone for first-line treatment of advanced gastric cancer (SPIRITS trial): A phase III trial. Lancet Oncol. 2008, 9, 215–221. [Google Scholar] [CrossRef]
- Bang, Y.-J.; Van Cutsem, E.; Feyereislova, A.; Chung, H.C.; Shen, L.; Sawaki, A.; Lordick, F.; Ohtsu, A.; Omuro, Y.; Satoh, T.; et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): A phase 3, open-label, randomised controlled trial. Lancet 2010, 376, 687–697. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Higuchi, K.; Nishikawa, K.; Gotoh, M.; Fuse, N.; Sugimoto, N.; Nishina, T.; Amagai, K.; Chin, K.; Niwa, Y.; et al. Phase III study comparing oxaliplatin plus S-1 with cisplatin plus S-1 in chemotherapy-naïve patients with advanced gastric cancer. Ann. Oncol. 2014, 26, 141–148. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Shitara, K.; Moehler, M.; Garrido, M.; Salman, P.; Shen, L.; Wyrwicz, L.; Yamaguchi, K.; Skoczylas, T.; Bragagnoli, A.C.; et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): A randomised, open-label, phase 3 trial. Lancet 2021, 398, 27–40. [Google Scholar] [CrossRef]
- Kang, Y.-K.; Chen, L.-T.; Ryu, M.-H.; Oh, D.-Y.; Oh, S.C.; Chung, H.C.; Lee, K.-W.; Omori, T.; Shitara, K.; Sakuramoto, S.; et al. Nivolumab plus chemotherapy versus placebo plus chemotherapy in patients with HER2-negative, untreated, unresectable advanced or recurrent gastric or gastro-oesophageal junction cancer (ATTRACTION-4): A randomised, multicentre, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2022, 23, 234–247. [Google Scholar] [CrossRef] [PubMed]
- Ohtsu, A.; Shah, M.A.; Van Cutsem, E.; Rha, S.Y.; Sawaki, A.; Park, S.R.; Lim, H.Y.; Yamada, Y.; Wu, J.; Langer, B.; et al. Bevacizumab in Combination With Chemotherapy As First-Line Therapy in Advanced Gastric Cancer: A Randomized, Double-Blind, Placebo-Controlled Phase III Study. J. Clin. Oncol. 2011, 29, 3968–3976. [Google Scholar] [CrossRef] [PubMed]
- Wilke, H.; Muro, K.; Van Cutsem, E.; Oh, S.-C.; Bodoky, G.; Shimada, Y.; Hironaka, S.; Sugimoto, N.; Lipatov, O.; Kim, T.-Y.; et al. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): A double-blind, randomised phase 3 trial. Lancet Oncol. 2014, 15, 1224–1235. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, C.S.; Tomasek, J.; Yong, C.J.; Dumitru, F.; Passalacqua, R.; Goswami, C.; Safran, H.; dos Santos, L.V.; Aprile, G.; Ferry, D.R.; et al. Ramucirumab monotherapy for previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (REGARD): An international, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet 2013, 383, 31–39. [Google Scholar] [CrossRef]
- Li, J.; Qin, S.; Xu, J.; Xiong, J.; Wu, C.; Bai, Y.; Liu, W.; Tong, J.; Liu, Y.; Xu, R.; et al. Randomized, Double-Blind, Placebo-Controlled Phase III Trial of Apatinib in Patients With Chemotherapy-Refractory Advanced or Metastatic Adenocarcinoma of the Stomach or Gastroesophageal Junction. J. Clin. Oncol. 2016, 34, 1448–1454. [Google Scholar] [CrossRef] [PubMed]
- Pavlakis, N.; Sjoquist, K.; Martin, A.J.; Tsobanis, E.; Yip, S.; Kang, Y.-K.; Bang, Y.-J.; Alcindor, T.; O’callaghan, C.J.; Burnell, M.J.; et al. Regorafenib for the Treatment of Advanced Gastric Cancer (INTEGRATE): A Multinational Placebo-Controlled Phase II Trial. J. Clin. Oncol. 2016, 34, 2728–2735. [Google Scholar] [CrossRef] [PubMed]
- Pavlakis, N.; Shitara, K.; Sjoquist, K.M.; Martin, A.J.; Jaworski, A.; Yip, S.; Bang, Y.-J.; Alcindor, T.; O’callaghan, C.J.; Burnell, M.J.; et al. INTEGRATE IIa: A randomised, double-blind, phase III study of regorafenib versus placebo in refractory advanced gastro-oesophageal cancer (AGOC)—A study led by the Australasian Gastro-intestinal Trials Group (AGITG). J. Clin. Oncol. 2023, 41 (Suppl. S4), LBA294. [Google Scholar] [CrossRef]
- Patel, S.A.; Nilsson, M.B.; Le, X.; Cascone, T.; Jain, R.K.; Heymach, J.V. Molecular Mechanisms and Future Implications of VEGF/VEGFR in Cancer Therapy. Clin. Cancer Res. 2022, 29, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Folkman, J. Tumor angiogenesis: Therapeutic implications. N. Engl. J. Med. 1971, 285, 1182–1186. [Google Scholar] [CrossRef] [PubMed]
- Hurwitz, H.; Fehrenbacher, L.; Novotny, W.; Cartwright, T.; Hainsworth, J.; Heim, W.; Berlin, J.; Baron, A.; Griffing, S.; Holmgren, E.; et al. Bevacizumab plus Irinotecan, Fluorouracil, and Leucovorin for Metastatic Colorectal Cancer. N. Engl. J. Med. 2004, 350, 2335–2342. [Google Scholar] [CrossRef]
- Senger, D.R.; Galli, S.J.; Dvorak, A.M.; Perruzzi, C.A.; Harvey, V.S.; Dvorak, H.F. Tumor Cells Secrete a Vascular Permeability Factor That Promotes Accumulation of Ascites Fluid. Science 1983, 219, 983–985. [Google Scholar] [CrossRef]
- Keck, P.J.; Hauser, S.D.; Krivi, G.; Sanzo, K.; Warren, T.; Feder, J.; Connolly, D.T. Vascular Permeability Factor, an Endothelial Cell Mitogen Related to PDGF. Science 1989, 246, 1309–1312. [Google Scholar] [CrossRef]
- Maglione, D.; Guerriero, V.; Viglietto, G.; Delli-Bovi, P.; Persico, M.G. Isolation of a human placenta cDNA coding for a protein related to the vascular permeability factor. Proc. Natl. Acad. Sci. USA 1991, 88, 9267–9271. [Google Scholar] [CrossRef] [PubMed]
- Leung, D.W.; Cachianes, G.; Kuang, W.-J.; Goeddel, D.V.; Ferrara, N. Vascular Endothelial Growth Factor Is a Secreted Angiogenic Mitogen. Science 1989, 246, 1306–1309. [Google Scholar] [CrossRef] [PubMed]
- Javle, M.; Smyth, E.C.; Chau, I. Ramucirumab: Successfully Targeting Angiogenesis in Gastric Cancer. Clin. Cancer Res. 2014, 20, 5875–5881. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.J.; Li, B.; Winer, J.; Armanini, M.; Gillett, N.; Phillips, H.S.; Ferrara, N. Inhibition of vascular endothelial growth factor-induced angiogenesis suppresses tumour growth in vivo. Nature 1993, 362, 841–844. [Google Scholar] [CrossRef] [PubMed]
- Park, D.J.; Thomas, N.; Yoon, C.; Yoon, S.S. Vascular Endothelial Growth Factor A Inhibition in Gastric Cancer. Gastric Cancer 2015, 18, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.; Wang, M.; Gralow, J.; Dickler, M.; Cobleigh, M.; Perez, E.A.; Shenkier, T.; Cella, D.; Davidson, N.E. Paclitaxel plus Bevacizumab versus Paclitaxel Alone for Metastatic Breast Cancer. N. Engl. J. Med. 2007, 357, 2666–2676. [Google Scholar] [CrossRef]
- Friedman, H.S.; Prados, M.D.; Wen, P.Y.; Mikkelsen, T.; Schiff, D.; Abrey, L.E.; Yung, W.A.; Paleologos, N.; Nicholas, M.K.; Jensen, R.; et al. Bevacizumab Alone and in Combination With Irinotecan in Recurrent Glioblastoma. J. Clin. Oncol. 2009, 27, 4733–4740. [Google Scholar] [CrossRef]
- Reck, M.; Von Pawel, J.; Zatloukal, P.; Ramlau, R.; Gorbounova, V.; Hirsh, V.; Leighl, N.; Mezger, J.; Archer, V.; Moore, N.; et al. Phase III Trial of Cisplatin Plus Gemcitabine With Either Placebo or Bevacizumab As First-Line Therapy for Nonsquamous Non–Small-Cell Lung Cancer: AVAiL. J. Clin. Oncol. 2009, 27, 1227–1234. [Google Scholar] [CrossRef]
- Shah, M.A.; Ramanathan, R.K.; Ilson, D.H.; Levnor, A.; D’Adamo, D.; O’Reilly, E.; Tse, A.; Trocola, R.; Schwartz, L.; Capanu, M.; et al. Multicenter Phase II Study of Irinotecan, Cisplatin, and Bevacizumab in Patients With Metastatic Gastric or Gastroesophageal Junction Adenocarcinoma. J. Clin. Oncol. 2006, 24, 5201–5206. [Google Scholar] [CrossRef] [PubMed]
- Boku, N.; Ohtsu, A.; Shimada, Y.; Shirao, K.; Seki, S.; Saito, H.; Sakata, Y.; Hyodo, I. Phase II Study of a Combination of Irinotecan and Cisplatin Against Metastatic Gastric Cancer. J. Clin. Oncol. 1999, 17, 319. [Google Scholar] [CrossRef] [PubMed]
- Ajani, J.A.; Baker, J.; Pisters, P.W.T.; Ho, L.; Mansfield, P.F.; Feig, B.W.; Charnsangavej, C. CPT-11 plus cisplatin in patients with advanced, untreated gastric or gastroesophageal junction carcinoma: Results of a phase II study. Cancer 2002, 94, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Ilson, D.H.; Saltz, L.; Enzinger, P.; Huang, Y.; Kornblith, A.; Gollub, M.; O’Reilly, E.M.; Schwartz, G.; DeGroff, J.; Gonzalez, G.; et al. Phase II Trial of Weekly Irinotecan Plus Cisplatin in Advanced Esophageal Cancer. J. Clin. Oncol. 1999, 17, 3270–3275. [Google Scholar] [CrossRef] [PubMed]
- El-Rayes, B.F.; Zalupski, M.; Bekai-Saab, T.; Heilbrun, L.K.; Hammad, N.; Patel, B.; Urba, S.; Shields, A.F.; Vaishampayan, U.; Dawson, S.; et al. A phase II study of bevacizumab, oxaliplatin, and docetaxel in locally advanced and metastatic gastric and gastroesophageal junction cancers. Ann. Oncol. 2010, 21, 1999–2004. [Google Scholar] [CrossRef]
- Shen, L.; Li, J.; Xu, J.; Pan, H.; Dai, G.; Qin, S.; Wang, L.; Wang, J.; Yang, Z.; Shu, Y.; et al. Bevacizumab plus capecitabine and cisplatin in Chinese patients with inoperable locally advanced or metastatic gastric or gastroesophageal junction cancer: Randomized, double-blind, phase III study (AVATAR study). Gastric Cancer 2015, 18, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Moiseyenko, V.M.; Tjulandin, S.; Majlis, A.; Constenla, M.; Boni, C.; Rodrigues, A.; Fodor, M.; Chao, Y.; Voznyi, E.; et al. Phase III study of docetaxel and cisplatin plus fluorouracil compared with cisplatin and fluorouracil as first-line therapy for advanced gastric cancer: A report of the V25 study group. J. Clin. Oncol. 2006, 24, 4991–4997. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.A.; Jhawer, M.; Ilson, D.H.; Lefkowitz, R.A.; Robinson, E.; Capanu, M.; Kelsen, D.P. Phase II Study of Modified Docetaxel, Cisplatin, and Fluorouracil With Bevacizumab in Patients With Metastatic Gastroesophageal Adenocarcinoma. J. Clin. Oncol. 2011, 29, 868–874. [Google Scholar] [CrossRef]
- Shah, M.A.; Shibata, S.; Stoller, R.G.; Kemeny, M.; Ritch, P.S.; Krishnamurthi, S.S.; Su, Y.B.; Janjigian, Y.Y.; Capanu, M.; Kelsen, D.P.; et al. Random assignment multicenter phase II study of modified docetaxel, cisplatin, fluorouracil (mDCF) versus DCF with growth factor support (GCSF) in metastatic gastroesophageal adenocarcinoma (GE). J. Clin. Oncol. 2010, 28, 4014. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ®) Gastric Cancer. Available online: https://www.nccn.org/professionals/physician_gls/pdf/gastric.pdf (accessed on 24 March 2023).
- Muro, K.; Van Cutsem, E.; Narita, Y.; Pentheroudakis, G.; Baba, E.; Li, J.; Ryu, M.-H.; Wan Zamaniah, W.I.; Yong, W.-P.; Yeh, K.-H.; et al. Pan-Asian adapted ESMO Clinical Practice Guidelines for the management of patients with metastatic gastric cancer: A JSMO–ESMO initiative endorsed by CSCO, KSMO, MOS, SSO and TOS. Ann. Oncol. 2019, 30, 19–33. [Google Scholar] [CrossRef] [PubMed]
- Lordick, F.; Carneiro, F.; Cascinu, S.; Fleitas, T.; Haustermans, K.; Piessen, G.; Vogel, A.; Smyth, E. Gastric cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2022, 33, 1005–1020. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.; Kim, I.; Kang, S.J.; Choi, M.; Kim, B.; Eom, B.W.; Kim, B.J.; Min, B.H.; Choi, C.I.; Shin, C.M.; et al. Korean Practice Guidelines for Gastric Cancer 2022: An Evidence-based, Multidisciplinary Approach. J. Gastric Cancer 2023, 23, 3–106. [Google Scholar] [CrossRef] [PubMed]
- Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer 2020, 24, 1–21. [Google Scholar]
- Eom, S.S.; Choi, W.; Eom, B.W.; Park, S.H.; Kim, S.J.; Kim, Y.I.; Yoon, H.M.; Lee, J.Y.; Kim, C.G.; Kim, H.K.; et al. A Comprehensive and Comparative Review of Global Gastric Cancer Treatment Guidelines. J. Gastric Cancer 2022, 22, 3–23. [Google Scholar] [CrossRef]
- Xu, R.-H.; Zhang, Y.; Pan, H.; Feng, J.; Zhang, T.; Liu, T.; Qin, Y.; Qin, S.; Yin, X.; Liu, B.; et al. Efficacy and safety of weekly paclitaxel with or without ramucirumab as second-line therapy for the treatment of advanced gastric or gastroesophageal junction adenocarcinoma (RAINBOW-Asia): A randomised, multicentre, double-blind, phase 3 trial. Lancet Gastroenterol. Hepatol. 2021, 6, 1015–1024. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, C.S.; Shitara, K.; Di Bartolomeo, M.; Lonardi, S.; Al-Batran, S.-E.; Van Cutsem, E.; Ilson, D.H.; Alsina, M.; Chau, I.; Lacy, J.; et al. Ramucirumab with cisplatin and fluoropyrimidine as first-line therapy in patients with metastatic gastric or junctional adenocarcinoma (RAINFALL): A double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 420–435. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.; Bendell, J.; Braiteh, F.; Firdaus, I.; Philip, P.; Cohn, A.; Lewis, N.; Anderson, D.; Arrowsmith, E.; Schwartz, J.; et al. Ramucirumab combined with FOLFOX as front-line therapy for advanced esophageal, gastroesophageal junction, or gastric adenocarcinoma: A randomized, double-blind, multicenter Phase II trial. Ann. Oncol. 2016, 27, 2196–2203. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, T.; Muro, K.; Shitara, K.; Oh, D.Y.; Kang, Y.K.; Chung, H.C.; Kudo, T.; Chin, K.; Kadowaki, S.; Hamamoto, Y.; et al. Effect of First-line S-1 Plus Oxaliplatin With or Without Ramucirumab Followed by Paclitaxel Plus Ramucirumab on Advanced Gastric Cancer in East Asia: The Phase 2 RAINSTORM Randomized Clinical Trial. JAMA Netw. Open 2019, 2, e198243. [Google Scholar] [CrossRef] [PubMed]
- Shitara, K.; Kadowaki, S.; Nishina, T.; Sakai, D.; Yoshikawa, R.; Piao, Y.; Ozeki, A.; Inoue, K.; Gritli, I.; Muro, K. Safety, pharmacokinetic, and clinical activity profiles of ramucirumab in combination with three platinum/fluoropyrimidine doublets in Japanese patients with chemotherapy-naïve metastatic gastric/gastroesophageal junction cancer. Gastric Cancer 2018, 21, 106–113. [Google Scholar] [CrossRef]
- Ohtsu, A.; Shah, M.A.; Van Cutsem, E.; Rha, S.Y.; Sawaki, A.; Park, S.R.; Lim, H.Y.; Yamada, Y.; Wu, J.; Langer, B.; et al. Bevacizumab in combination with chemotherapy as first-line therapy in advanced gastric cancer: A biomarker evaluation from the AVAGAST randomized phase III trial. J. Clin. Oncol. 2012, 30, 2119–2127. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Tabernero, J.; Lakomy, R.; Prenen, H.; Prausová, J.; Macarulla, T.; Ruff, P.; Van Hazel, G.A.; Moiseyenko, V.; Ferry, D.; et al. Addition of aflibercept to fluorouracil, leucovorin, and irinotecan improves survival in a phase III randomized trial in patients with metastatic colorectal cancer previously treated with an oxaliplatin-based regimen. J. Clin. Oncol. 2012, 30, 3499–3506. [Google Scholar] [CrossRef]
- Cleary, J.M.; Horick, N.K.; McCleary, N.J.; Abrams, T.A.; Yurgelun, M.B.; Azzoli, C.G.; Rubinson, D.A.; Brooks, G.A.; Chan, J.A.; Blaszkowsky, L.S.; et al. FOLFOX plus ziv-aflibercept or placebo in first-line metastatic esophagogastric adenocarcinoma: A double-blind, randomized, multicenter phase 2 trial. Cancer 2019, 125, 2213–2221. [Google Scholar] [CrossRef] [PubMed]
- Di Bartolomeo, M.; Niger, M.; Morano, F.; Corallo, S.; Antista, M.; Tamberi, S.; Lonardi, S.; Di Donato, S.; Berardi, R.; Scartozzi, M.; et al. Assessment of Ramucirumab plus paclitaxel as switch maintenance versus continuation of first-line chemotherapy in patients with advanced HER-2 negative gastric or gastroesophageal junction cancers: The ARMANI phase III trial. BMC Cancer 2019, 19, 283. [Google Scholar] [CrossRef] [PubMed]
- Shitara, K.; Takashima, A.; Fujitani, K.; Koeda, K.; Hara, H.; Nakayama, N.; Hironaka, S.; Nishikawa, K.; Makari, Y.; Amagai, K.; et al. Nab-paclitaxel versus solvent-based paclitaxel in patients with previously treated advanced gastric cancer (ABSOLUTE): An open-label, randomised, non-inferiority, phase 3 trial. Lancet Gastroenterol. Hepatol. 2017, 2, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Bando, H.; Shimodaira, H.; Fujitani, K.; Takashima, A.; Yamaguchi, K.; Nakayama, N.; Takahashi, T.; Oki, E.; Azuma, M.; Nishina, T.; et al. A phase II study of nab-paclitaxel in combination with ramucirumab in patients with previously treated advanced gastric cancer. Eur. J. Cancer 2018, 91, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Bendell, J.C.; Percent, I.J.; Weaver, R.W.; Chua, C.C.; Xiong, H.Q.; Cohn, A.L.; Zakari, A.; Singh, J.; Kozloff, M.; Lietman, C.; et al. A phase II study of nab-paclitaxel plus ramucirumab for the second-line treatment of patients with metastatic gastroesophageal cancer. J. Clin. Oncol. 2020, 38, 365. [Google Scholar] [CrossRef]
- Takashima, A.; Shitara, K.; Fujitani, K.; Koeda, K.; Hara, H.; Nakayama, N.; Hironaka, S.; Nishikawa, K.; Kimura, Y.; Amagai, K.; et al. Peritoneal metastasis as a predictive factor for nab-paclitaxel in patients with pretreated advanced gastric cancer: An exploratory analysis of the phase III ABSOLUTE trial. Gastric Cancer 2019, 22, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Hirata, K.; Hamamoto, Y.; Ando, M.; Imamura, C.K.; Yoshimura, K.; Yamazaki, K.; Hironaka, S.; Muro, K. Weekly paclitaxel plus ramucirumab versus weekly nab-paclitaxel plus ramucirumab for unresectable advanced or recurrent gastric cancer with peritoneal dissemination refractory to first-line therapy—The P-SELECT trial (WJOG10617G)—A randomised phase II. BMC Cancer 2020, 20, 584. [Google Scholar] [CrossRef]
- Hirata, K.; Hamamoto, Y.; Shoji, H.; Hara, H.; Kondoh, C.; Yasui, H.; Kajiwara, T.; Baba, E.; Ando, T.; Sugimoto, N.; et al. A randomized phase II trial of paclitaxel plus ramucirumab versus nab-paclitaxel plus ramucirumab for gastric cancer with peritoneal dissemination refractory to first-line therapy (WJOG10617G/P-SELECT). J. Clin. Oncol. 2022, 40, 280. [Google Scholar] [CrossRef]
- Hironaka, S.; Ueda, S.; Yasui, H.; Nishina, T.; Tsuda, M.; Tsumura, T.; Sugimoto, N.; Shimodaira, H.; Tokunaga, S.; Moriwaki, T.; et al. Randomized, open-label, phase III study comparing irinotecan with paclitaxel in patients with advanced gastric cancer without severe peritoneal metastasis after failure of prior combination chemotherapy using fluoropyrimidine plus platinum: WJOG 4007 tria. J. Clin. Oncol. 2013, 31, 4438–4444. [Google Scholar] [CrossRef] [PubMed]
- Makiyama, A.; Arimizu, K.; Hirano, G.; Makiyama, C.; Matsushita, Y.; Shirakawa, T.; Ohmura, H.; Komoda, M.; Uchino, K.; Inadomi, K.; et al. Irinotecan monotherapy as third-line or later treatment in advanced gastric cancer. Gastric Cancer 2018, 21, 464–472. [Google Scholar] [CrossRef]
- Kang, J.H.; Lee, S.I.; Lim, D.H.; Park, K.-W.; Oh, S.Y.; Kwon, H.-C.; Hwang, I.G.; Lee, S.-C.; Nam, E.; Shin, D.B.; et al. Salvage Chemotherapy for Pretreated Gastric Cancer: A Randomized Phase III Trial Comparing Chemotherapy Plus Best Supportive Care With Best Supportive Care Alone. J. Clin. Oncol. 2012, 30, 1513–1518. [Google Scholar] [CrossRef] [PubMed]
- Takahari, D. Second-line chemotherapy for patients with advanced gastric cancer. Gastric Cancer 2017, 20, 395–406. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, T.; Machida, N.; Yasui, H.; Kawahira, M.; Kawai, S.; Kito, Y.; Yoshida, Y.; Hamauchi, S.; Tsushima, T.; Todaka, A.; et al. Efficacy and safety of irinotecan monotherapy as third-line treatment for advanced gastric cancer. Cancer Chemother. Pharmacol. 2016, 78, 809–814. [Google Scholar] [CrossRef]
- Nishimura, T.; Iwasa, S.; Nagashima, K.; Okita, N.; Takashima, A.; Honma, Y.; Kato, K.; Hamaguchi, T.; Yamada, Y.; Shimada, Y.; et al. Irinotecan monotherapy as third-line treatment for advanced gastric cancer refractory to fluoropyrimidines, platinum, and taxanes. Gastric Cancer 2017, 20, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Tabernero, J.; Yoshino, T.; Cohn, A.L.; Obermannova, R.; Bodoky, G.; Garcia-Carbonero, R.; Ciuleanu, T.-E.; Portnoy, D.C.; Van Cutsem, E.; Grothey, A.; et al. Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab, oxaliplatin, and a fluoropyrimidine (RAISE): A randomised, double-blind, multicentre, phase 3 study. Lancet Oncol. 2015, 16, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Lorenzen, S.; Thuss-Patience, P.; Pauligk, C.; Gökkurt, E.; Ettrich, T.; Lordick, F.; Stahl, M.; Reichardt, P.; Sökler, M.; Pink, D.; et al. FOLFIRI plus ramucirumab versus paclitaxel plus ramucirumab as second-line therapy for patients with advanced or metastatic gastroesophageal adenocarcinoma with or without prior docetaxel—Results from the phase II RAMIRIS Study of the German Gastric Cancer Study Group at AIO. Eur. J. Cancer 2022, 165, 48–57. [Google Scholar] [PubMed]
- Satake, H.; Sagawa, T.; Fujikawa, K.; Hatachi, Y.; Yasui, H.; Kotaka, M.; Kato, T.; Tsuji, A. Phase Ib study of irinotecan and ramucirumab for advanced gastric cancer previously treated with fluoropyrimidine with/without platinum and taxane. Cancer Chemother. Pharmacol. 2018, 82, 839–845. [Google Scholar] [CrossRef]
- Kawamoto, Y.; Yuki, S.; Sawada, K.; Nakamura, M.; Muto, O.; Sogabe, S.; Shindo, Y.; Ishiguro, A.; Sato, A.; Tsuji, Y.; et al. Phase II Study of Ramucirumab Plus Irinotecan Combination Therapy as Second-Line Treatment in Patients with Advanced Gastric Cancer: HGCSG1603. Oncologist 2022, 27, e642–e649. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, T.; Kawakami, H.; Sakai, D.; Kurokawa, Y.; Shimokawa, T.; Goto, M.; Satoh, T. Protocol of OGSG 1901: A phase II trial of ramucirumab plus irinotecan for patients with early relapsed gastric cancer during or after adjuvant docetaxel plus S—1 therapy. BMC Cancer 2022, 22, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Bennouna, J.; Sastre, J.; Arnold, D.; Österlund, P.; Greil, R.; Van Cutsem, E.; von Moos, R.; Viéitez, J.M.; Bouché, O.; Borg, C.; et al. Continuation of bevacizumab after first progression in metastatic colorectal cancer (ML18147): A randomised phase 3 trial. Lancet Oncol. 2013, 14, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Shitara, K.; Doi, T.; Dvorkin, M.; Mansoor, W.; Arkenau, H.-T.; Prokharau, A.; Alsina, M.; Ghidini, M.; Faustino, C.; Gorbunova, V.; et al. Trifluridine/tipiracil versus placebo in patients with heavily pretreated metastatic gastric cancer (TAGS): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2018, 19, 1437–1448. [Google Scholar] [CrossRef]
- Kuboki, Y.; Nishina, T.; Shinozaki, E.; Yamazaki, K.; Shitara, K.; Okamoto, W.; Kajiwara, T.; Matsumoto, T.; Tsushima, T.; Mochizuki, N.; et al. TAS-102 plus bevacizumab for patients with metastatic colorectal cancer refractory to standard therapies (C-TASK FORCE): An investigator-initiated, open-label, single-arm, multicentre, phase 1/2 study. Lancet Oncol. 2017, 18, 1172–1181. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, P.; Yilmaz, M.; Möller, S.; Zitnjak, D.; Krogh, M.; Petersen, L.N.; Poulsen, L.; Winther, S.B.; Thomsen, K.G.; Qvortrup, C. TAS-102 with or without bevacizumab in patients with chemorefractory metastatic colorectal cancer: An investigator-initiated, open-label, randomised, phase 2 trial. Lancet Oncol. 2020, 21, 412–420. [Google Scholar] [CrossRef]
- Tabernero, J.; Taieb, J.; Prager, G.W.; Ciardiello, F.; Fakih, M.; Leger, C.; Fougeray, R.; Amellal, N.; van Cutsem, E. Trifluridine/tipiracil plus bevacizumab for third-line management of metastatic colorectal cancer: SUNLIGHT study design. Future Oncol. 2021, 17, 1977–1985. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, P.; Yilmaz, M.; Nordsmark, M.; Möller, S.; Elle, I.; Ladekarl, M.; Winther, S.; Qvortrup, C.; Baeksgaard, L. O-4 Trifluridine/tipiracil (TAS-102) with or without bevacizumab in patients with pretreated metastatic esophago-gastric adenocarcinoma (mEGA): A Danish randomized trial (LonGas). Ann. Oncol. 2022, 33, S380. [Google Scholar] [CrossRef]
- Kawazoe, A.; Ando, T.; Hosaka, H.; Fujita, J.; Koeda, K.; Nishikawa, K.; Amagai, K.; Fujitani, K.; Ogata, K.; Watanabe, K.; et al. Safety and activity of trifluridine/tipiracil and ramucirumab in previously treated advanced gastric cancer: An open-label, single-arm, phase 2 trial. Lancet Gastroenterol. Hepatol. 2021, 6, 209–217. [Google Scholar] [CrossRef]
- Escudier, B.; Eisen, T.; Stadler, W.M.; Szczylik, C.; Oudard, S.; Siebels, M.; Negrier, S.; Chevreau, C.; Solska, E.; Desai, A.A.; et al. Sorafenib in Advanced Clear-Cell Renal-Cell Carcinoma. N. Engl. J. Med. 2007, 356, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Lovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.-F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.-L.; Forner, A.; et al. Sorafenib in Advanced Hepatocellular Carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Hutson, T.E.; Tomczak, P.; Michaelson, M.D.; Bukowski, R.M.; Rixe, O.; Oudard, S.; Negrier, S.; Szczylik, C.; Kim, S.T. Sunitinib versus Interferon Alfa in Metastatic Renal-Cell Carcinoma. N. Engl. J. Med. 2007, 356, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Kawazoe, A.; Lordick, F.; Janjigian, Y.Y.; Shitara, K. Biomarker-targeted therapies for advanced-stage gastric and gastro-oesophageal junction cancers: An emerging paradigm. Nat. Rev. Clin. Oncol. 2021, 18, 473–487. [Google Scholar] [CrossRef] [PubMed]
- Drescher, D.; Moeheler, M.; Gockel, I.; Frerichs, K.; Müller, A.; Dünschede, F.; Borschitz, T.; Biesterfeld, S.; Holtmann, M.; Wehler, T.; et al. Coexpression of receptor-tyrosine-kinases in gastric adenocarcinoma-a rationale for a molecular targeting strategy? World J. Gastroenterol. 2007, 13, 3605–3609. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Kiyota, N.; Fuse, N.; Kato, K.; Minami, H.; Hashizume, K.; Kuroki, Y.; Ito, Y.; Ohtsu, A. A phase I study of sorafenib in combination with S-1 plus cisplatin in patients with advanced gastric cancer. Gastric Cancer 2014, 17, 161–172. [Google Scholar] [CrossRef]
- Ryu, M.; Lee, K.H.; Shen, L.; Yeh, K.; Yoo, C.; Hong, Y.S.; Park, Y.I.; Yang, S.H.; Shin, D.B.; Zang, D.Y.; et al. Randomized phase II study of capecitabine plus cisplatin with or without sorafenib in patients with metastatic gastric cancer (STARGATE). Cancer Med. 2023, 12, 7784–7794. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Powell, M.; O’Dwyer, P.J.; Catalano, P.; Ansari, R.H.; Benson, A.B. Phase II Study of Sorafenib in Combination With Docetaxel and Cisplatin in the Treatment of Metastatic or Advanced Gastric and Gastroesophageal Junction Adenocarcinoma: ECOG 5203. J. Clin. Oncol. 2010, 28, 2947–2951. [Google Scholar] [CrossRef] [PubMed]
- Boku, N.; Muro, K.; Machida, N.; Hashigaki, S.; Kimura, N.; Suzuki, M.; Lechuga, M.; Miyata, Y. Phase I study of sunitinib plus S-1 and cisplatin in Japanese patients with advanced or metastatic gastric cancer. Investig. New Drugs 2014, 32, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Yi, J.H.; Lee, J.; Park, S.H.; Park, J.O.; Yim, D.-S.; Park, Y.S.; Lim, H.Y.; Kang, W.K. Randomised phase II trial of docetaxel and sunitinib in patients with metastatic gastric cancer who were previously treated with fluoropyrimidine and platinum. Br. J. Cancer 2012, 106, 1469–1474. [Google Scholar] [CrossRef] [PubMed]
- Moehler, M.; Gepfner-Tuma, I.; Maderer, A.; Thuss-Patience, P.C.; Ruessel, J.; Hegewisch-Becker, S.; Wilke, H.; Al-Batran, S.-E.; Rafiyan, M.-R.; Weißinger, F.; et al. Sunitinib added to FOLFIRI versus FOLFIRI in patients with chemorefractory advanced adenocarcinoma of the stomach or lower esophagus: A randomized, placebo-controlled phase II AIO trial with serum biomarker program. BMC Cancer 2016, 16, 699. [Google Scholar] [CrossRef] [PubMed]
- Bang, Y.-J.; Kang, Y.-K.; Kang, W.K.; Boku, N.; Chung, H.; Chen, J.-S.; Doi, T.; Sun, Y.; Shen, L.; Qin, S.; et al. Phase II study of sunitinib as second-line treatment for advanced gastric cancer. Investig. New Drugs 2011, 29, 1449–1458. [Google Scholar] [CrossRef] [PubMed]
- Högner, A.; Al-Batran, S.E.; Siveke, J.T.; Lorenz, M.; Bartels, P.; Breithaupt, K.; Malfertheiner, P.; Homann, N.; Stein, A.; Gläser, D.; et al. Pazopanib with 5-FU and oxaliplatin as first line therapy in advanced gastric cancer: A randomized phase-II study—The PaFLO trial. A study of the Arbeitsgemeinschaft Internistische Onkologie AIO-STO-0510. Int. J. Cancer 2022, 150, 1007–1017. [Google Scholar] [CrossRef]
- Kim, S.T.; Lee, J.; Lee, S.J.; Park, S.H.; Jung, S.-H.; Park, Y.S.; Lim, H.Y.; Kang, W.K.; Park, J.O. Prospective phase II trial of pazopanib plus CapeOX (capecitabine and oxaliplatin) in previously untreated patients with advanced gastric cancer. Oncotarget 2016, 7, 24088–24096. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xu, J.; Wang, Q.; Ling, G.; Mao, Y.; Cai, M.; Yang, Y.; Mei, J.; Han, Z.; Feng, J.; et al. Efficacy and safety of second-line therapy with apatinib combined with chemotherapy as second-line therapy in advanced gastric cancer: A single-arm, open-label, prospective, multicenter study. Ann. Transl. Med. 2022, 10, 641. [Google Scholar] [CrossRef]
- Ruan, H.; Dong, J.; Zhou, X.; Xiong, J.; Wang, H.; Zhong, X.; Cao, X. Multicenter phase II study of apatinib treatment for metastatic gastric cancer after failure of second-line chemotherapy. Oncotarget 2017, 8, 104552–104559. [Google Scholar] [CrossRef]
- Li, J.; Qin, S.; Xu, J.; Guo, W.; Xiong, J.; Bai, Y.; Sun, G.; Yang, Y.; Wang, L.; Xu, N.; et al. Apatinib for Chemotherapy-Refractory Advanced Metastatic Gastric Cancer: Results From a Randomized, Placebo-Controlled, Parallel-Arm, Phase II Trial. J. Clin. Oncol. 2013, 31, 3219–3225. [Google Scholar] [CrossRef]
- Kang, Y.-K.; Kang, W.K.; Di Bartolomeo, M.; Chau, I.; Yoon, H.H.; Cascinu, S.; Ryu, M.-H.; Kim, J.G.; Lee, K.W.; Oh, S.C.; et al. Randomized phase III ANGEL study of rivoceranib (apatinib) + best supportive care (BSC) vs. placebo + BSC in patients with advanced/metastatic gastric cancer who failed ≥2 prior chemotherapy regimens. Ann. Oncol. 2019, 30, v877–v878. [Google Scholar] [CrossRef]
- Wilhelm, S.M.; Dumas, J.; Adnane, L.; Lynch, M.; Carter, C.A.; Schütz, G.; Thierauch, K.-H.; Zopf, D. Regorafenib (BAY 73-4506): A new oral multikinase inhibitor of angiogenic, stromal and oncogenic receptor tyrosine kinases with potent preclinical antitumor activity. Int. J. Cancer 2011, 129, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Grothey, A.; Van Cutsem, E.; Sobrero, A.; Siena, S.; Falcone, A.; Ychou, M.; Humblet, Y.; Bouché, O.; Mineur, L.; Barone, C.; et al. Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): An international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet 2013, 381, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Pavlakis, N.; Shitara, K.; Sjoquist, K.M.; Martin, A.J.; Jaworski, A.; Yip, S.; Oh, D.-Y.; Moehler, M.H.; Bekaii-Saab, T.S.; Simes, J.; et al. INTEGRATE IIb: A randomized phase III open label study of regorafenib + nivolumab versus standard chemotherapy in refractory advanced gastroesophageal cancer (AGOC). J. Clin. Oncol. 2022, 40, TPS366. [Google Scholar] [CrossRef]
- Fukumura, D.; Kloepper, J.; Amoozgar, Z.; Duda, D.G.; Jain, R.K. Enhancing cancer immunotherapy using antiangiogenics: Opportunities and challenges. Nat. Rev. Clin. Oncol. 2018, 15, 325–340. [Google Scholar] [CrossRef] [PubMed]
- McDermott, D.F.; Huseni, M.A.; Atkins, M.B.; Motzer, R.J.; Rini, B.I.; Escudier, B.; Fong, L.; Joseph, R.W.; Pal, S.K.; Reeves, J.A.; et al. Clinical activity and molecular correlates of response to atezolizumab alone or in combination with bevacizumab versus sunitinib in renal cell carcinoma. Nat. Med. 2018, 24, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Penkov, K.; Haanen, J.; Rini, B.; Albiges, L.; Campbell, M.T.; Venugopal, B.; Kollmannsberger, C.; Negrier, S.; Uemura, M.; et al. Avelumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2019, 380, 1103–1115. [Google Scholar] [CrossRef]
- Rini, B.I.; Plimack, E.R.; Stus, V.; Gafanov, R.; Hawkins, R.; Nosov, D.; Pouliot, F.; Alekseev, B.; Soulières, D.; Melichar, B.; et al. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2019, 380, 1116–1127. [Google Scholar] [CrossRef] [PubMed]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.S.; Arkenau, H.-T.; Santana-Davila, R.; Calvo, E.; Paz-Ares, L.; Cassier, P.A.; Bendell, J.; Penel, N.; Krebs, M.G.; Martin-Liberal, J.; et al. Ramucirumab plus pembrolizumab in patients with previously treated advanced non-small-cell lung cancer, gastro-oesophageal cancer, or urothelial carcinomas (JVDF): A multicohort, non-randomised, open-label, phase 1a/b trial. Lancet Oncol. 2019, 20, 1109–1123. [Google Scholar] [CrossRef]
- Chau, I.; Penel, N.; Soriano, A.O.; Arkenau, H.-T.; Cultrera, J.; Santana-Davila, R.; Calvo, E.; Le Tourneau, C.; Zender, L.; Bendell, J.C.; et al. Ramucirumab in Combination with Pembrolizumab in Treatment-Naïve Advanced Gastric or GEJ Adenocarcinoma: Safety and Antitumor Activity from the Phase 1a/b JVDF Trial. Cancers 2020, 12, 2985. [Google Scholar] [CrossRef] [PubMed]
- Bang, Y.-J.; Golan, T.; Dahan, L.; Fu, S.; Moreno, V.; Park, K.; Geva, R.; De Braud, F.; Wainberg, Z.A.; Reck, M.; et al. Ramucirumab and durvalumab for previously treated, advanced non–small-cell lung cancer, gastric/gastro-oesophageal junction adenocarcinoma, or hepatocellular carcinoma: An open-label, phase Ia/b study (JVDJ). Eur. J. Cancer 2020, 137, 272–284. [Google Scholar] [CrossRef] [PubMed]
- Hara, H.; Shoji, H.; Takahari, D.; Esaki, T.; Machida, N.; Nagashima, K.; Aoki, K.; Honda, K.; Miyamoto, T.; Boku, N.; et al. Phase I/II study of ramucirumab plus nivolumab in patients in second-line treatment for advanced gastric adenocarcinoma (NivoRam study). J. Clin. Oncol. 2019, 37, 129. [Google Scholar] [CrossRef]
- Kang, Y.-K.; Boku, N.; Satoh, T.; Ryu, M.-H.; Chao, Y.; Kato, K.; Chung, H.C.; Chen, J.-S.; Muro, K.; Kang, W.K.; et al. Nivolumab in patients with advanced gastric or gastro-oesophageal junction cancer refractory to, or intolerant of, at least two previous chemotherapy regimens (ONO-4538-12, ATTRACTION-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 390, 2461–2471. [Google Scholar] [CrossRef]
- Xu, J.; Zhang, Y.; Jia, R.; Yue, C.; Chang, L.; Liu, R.; Zhang, G.; Zhao, C.; Zhang, Y.; Chen, C.; et al. Anti-PD-1 antibody SHR-1210 combined with apatinib for advanced hepatocellular carcinoma, gastric, or esophagogastric junction cancer: An Open-label, Dose Escalation and Expansion Study. Clin. Cancer Res. 2019, 25, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Hoff, S.; Grünewald, S.; Röse, L.; Zopf, D. Immunomodulation by regorafenib alone and in combination with anti PD1 antibody on murine models of colorectal cancer. Ann. Oncol. 2017, 28, v423. [Google Scholar] [CrossRef]
- Ou, D.-L.; Chen, W.; Lee, S. Regorafenib enhances antitumor immunity via inhibition of p38 kinase/Creb1/Klf4 axis in tumor- associated macrophages. J. Immunother. Cancer 2021, 9, e001657. [Google Scholar] [CrossRef] [PubMed]
- Fukuoka, S.; Hara, H.; Takahashi, N.; Kojima, T.; Kawazoe, A.; Asayama, M.; Yoshii, T.; Kotani, D.; Tamura, H.; Mikamoto, Y.; et al. Regorafenib Plus Nivolumab in Patients With Advanced Gastric or Colorectal Cancer: An Open-Label, Dose-Escalation, and Dose-Expansion Phase Ib Trial (REGONIVO, EPOC1603). J. Clin. Oncol. 2020, 38, 2053–2061. [Google Scholar] [CrossRef]
- Cousin, S.; Metges, J.P.; Bellera, C.A.; Guégan, J.P.; Adenis, A.; Gomez-Roca, C.A.; Cassier, P.A.; Hollebecque, A.; Cantarel, C.; Palmieri, L.J.; et al. REGOMUNE: A phase II study of regorafenib plus avelumab in solid tumors—Results of the oesophageal or gastric carcinoma (OGC) cohort. J. Clin. Oncol. 2022, 40, 4060. [Google Scholar] [CrossRef]
- Shitara, K.; Muro, K.; Shimada, Y.; Hironaka, S.; Sugimoto, N.; Komatsu, Y.; Nishina, T.; Yamaguchi, K.; Segawa, Y.; Omuro, Y.; et al. Subgroup analyses of the safety and efficacy of ramucirumab in Japanese and Western patients in RAINBOW: A randomized clinical trial in second-line treatment of gastric cancer. Gastric Cancer 2016, 19, 927–938. [Google Scholar] [CrossRef] [PubMed]
- Kawazoe, A.; Fukuoka, S.; Nakamura, Y.; Kuboki, Y.; Wakabayashi, M.; Nomura, S.; Mikamoto, Y.; Shima, H.; Fujishiro, N.; Higuchi, T.; et al. Lenvatinib plus pembrolizumab in patients with advanced gastric cancer in the first-line or second-line setting (EPOC1706): An open-label, single-arm, phase 2 trial. Lancet Oncol. 2020, 21, 1057–1065. [Google Scholar] [CrossRef] [PubMed]
- Taylor, M.; Dutcus, C.; Schmidt, E.; Bagulho, T.; Li, D.; Shumaker, R.; Rasco, D. A phase 1b trial of lenvatinib (LEN) plus pembrolizumab (PEM) in patients with selected solid tumors. Ann. Oncol. 2016, 27, vi267. [Google Scholar] [CrossRef]
- Shitara, K.; Van Cutsem, E.; Bang, Y.-J.; Fuchs, C.; Wyrwicz, L.; Lee, K.-W.; Kudaba, I.; Garrido, M.; Chung, H.C.; Lee, J.; et al. Efficacy and Safety of Pembrolizumab or Pembrolizumab Plus Chemotherapy vs Chemotherapy Alone for Patients With First-line, Advanced Gastric Cancer: The KEYNOTE-062 Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1571–1580. [Google Scholar] [CrossRef] [PubMed]
- Shitara, K.; Özgüroğlu, M.; Bang, Y.-J.; Di Bartolomeo, M.; Mandalà, M.; Ryu, M.-H.; Fornaro, L.; Olesiński, T.; Caglevic, C.; Chung, H.C.; et al. Pembrolizumab versus paclitaxel for previously treated, advanced gastric or gastro-oesophageal junction cancer (KEYNOTE-061): A randomised, open-label, controlled, phase 3 trial. Lancet 2018, 392, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Donnini, S.; Filippelli, A.; Ciccone, V.; Spini, A.; Ristori, E.; Ziche, M.; Morbidelli, L. Cancer Sensitizing Agents for Chemotherapy; Academic Press: Cambridge, MA, USA, 2022; Volume 18, pp. 29–66. [Google Scholar]
- Yoshino, T.; Arnold, D.; Taniguchi, H.; Pentheroudakis, G.; Yamazaki, K.; Xu, R.-H.; Kim, T.; Ismail, F.; Tan, I.; Yeh, K.-H.; et al. Pan-Asian adapted ESMO consensus guidelines for the management of patients with metastatic colorectal cancer: A JSMO–ESMO initiative endorsed by CSCO, KACO, MOS, SSO and TOS. Ann. Oncol. 2018, 29, 44–70. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Muro, K.; Cunningham, D.; Bodoky, G.; Sobrero, A.; Cascinu, S.; Jaffer, A.; Oh, S.C.; Al-Batran, S.E.; Wainberg, Z.A.; et al. Biomarker analyses of second-line ramucirumab in patients with advanced gastric cancer from RAINBOW, a global, randomized, double-blind, phase 3 study. Eur. J. Cancer 2020, 127, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, T.E.; Kadowaki, S.; Minashi, K.; Nishina, T.; Yamanaka, T.; Hayashi, Y.; Izawa, N.; Muro, K.; Hironaka, S.; Kajiwara, T.; et al. Multicenter Phase I/II Study of Nivolumab Combined with Paclitaxel Plus Ramucirumab as Second-line Treatment in Patients with Advanced Gastric CancerNivolumab/Paclitaxel/Ramucirumab for Advanced Gastric Cancer. Clin. Cancer Res. 2021, 27, 1029–1036. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Trial Name/Authors | Ph | Regimen | Line | No. of Patients | Primary Endpoint | MST (95% CI) (Months) | HR (95% CI) p-Value | mPFS (95% CI) (Months) | HR (95% CI) p-Value | ORR (95% CI) (%) | OR (95% CI) p-Value | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bevacizumab (Bev) | ||||||||||||
| Shah MA, et al. | II | Bev (15mg/kg) +IRI + CDDP | 1L | 47 | TTP | 12.3 (11.3–17.2) | 8.3 (5.5–9.9) *TTP | 65 (46–80) | ||||
| El-Rayes BF, et al. | II | Bev (7.5mg/kg) +DTX + L-OHP | 1L | 38 | PFS | 11.1 (8.2–15.3) | 6.6 (4.4–10.5) | 42 (28–58) | ||||
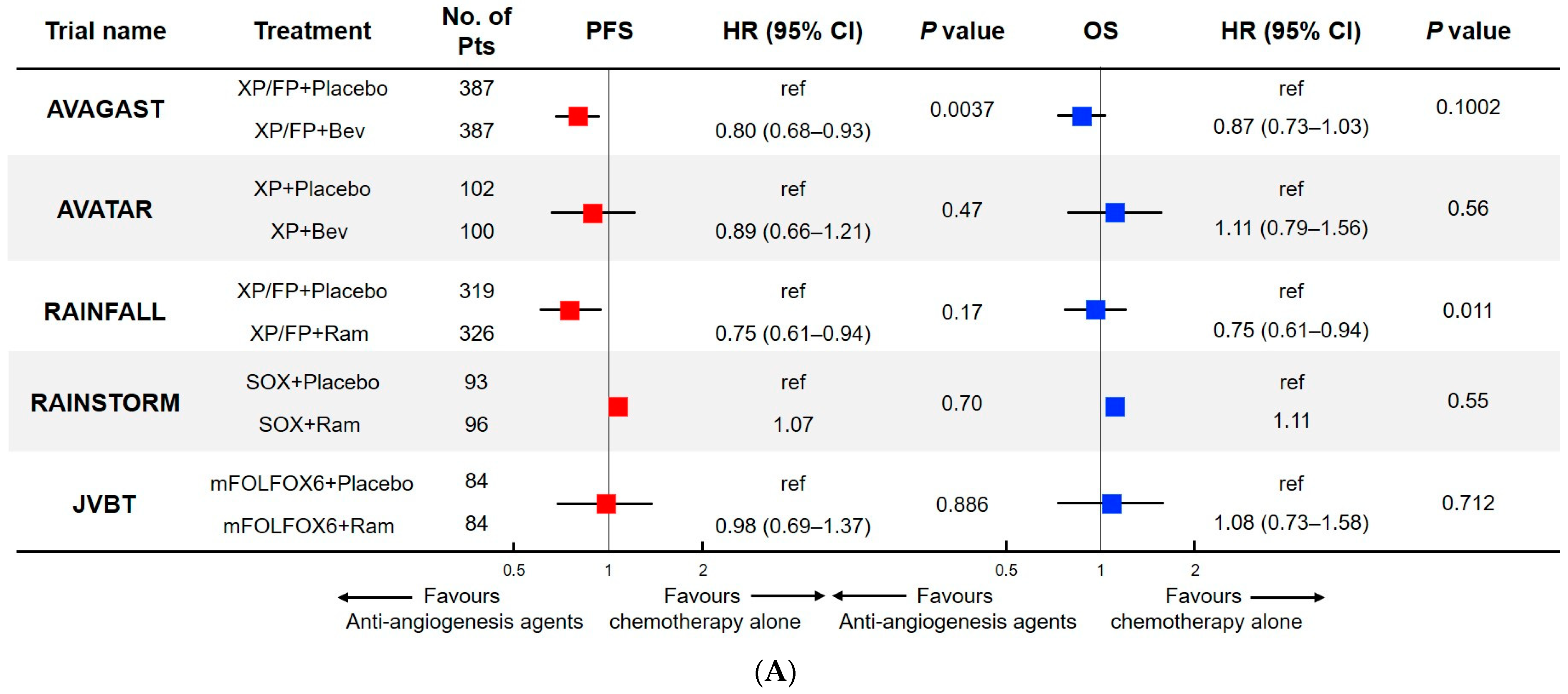
| AVAGAST | III | Bev (7.5mg/kg) +XP or FP vs. Placebo + XP or FP | 1L | 387 (Bev) vs. 387 (PBO) | OS | 12.1 (11.1–13.8) vs. 10.1 (9.0–11.3) | 0.87 (0.73–1.03) p = 0.1002 | 6.7 (5.9–7.1) vs. 5.3 (4.4–5.6) | 0.80 (0.68–0.93) p = 0.0037 | 46.0 vs. 37.4 | p = 0.315 | negative |
| AVATAR | III | Bev (7.5 mg/kg) +XP vs. Placebo + XP | 1L | 100 (Bev) vs. 102 (PBO) | OS | 11.4 (8.6–16.0) vs. 10.5 (8.9–14.1) | 1.11 (0.79–1.56) p = 0.56 | 6.0 (4.9–7.4) vs. 6.3 (5.7–7.4) | 0.89 (0.66–1.21) p = 0.47 | 41 vs. 34 | 1.19 (0.65–2.20) p = 0.35 | negative |
| Shah MA, et al. | II | Bev (10 mg/kg) + mDCF | 1L | 44 | PFS at 6 m | 12.0 (8.8–18.2) | 16.8 (12.1–26.0) | 67 (50–81) | positive | |||
| Ramucirumab (Ram) | ||||||||||||
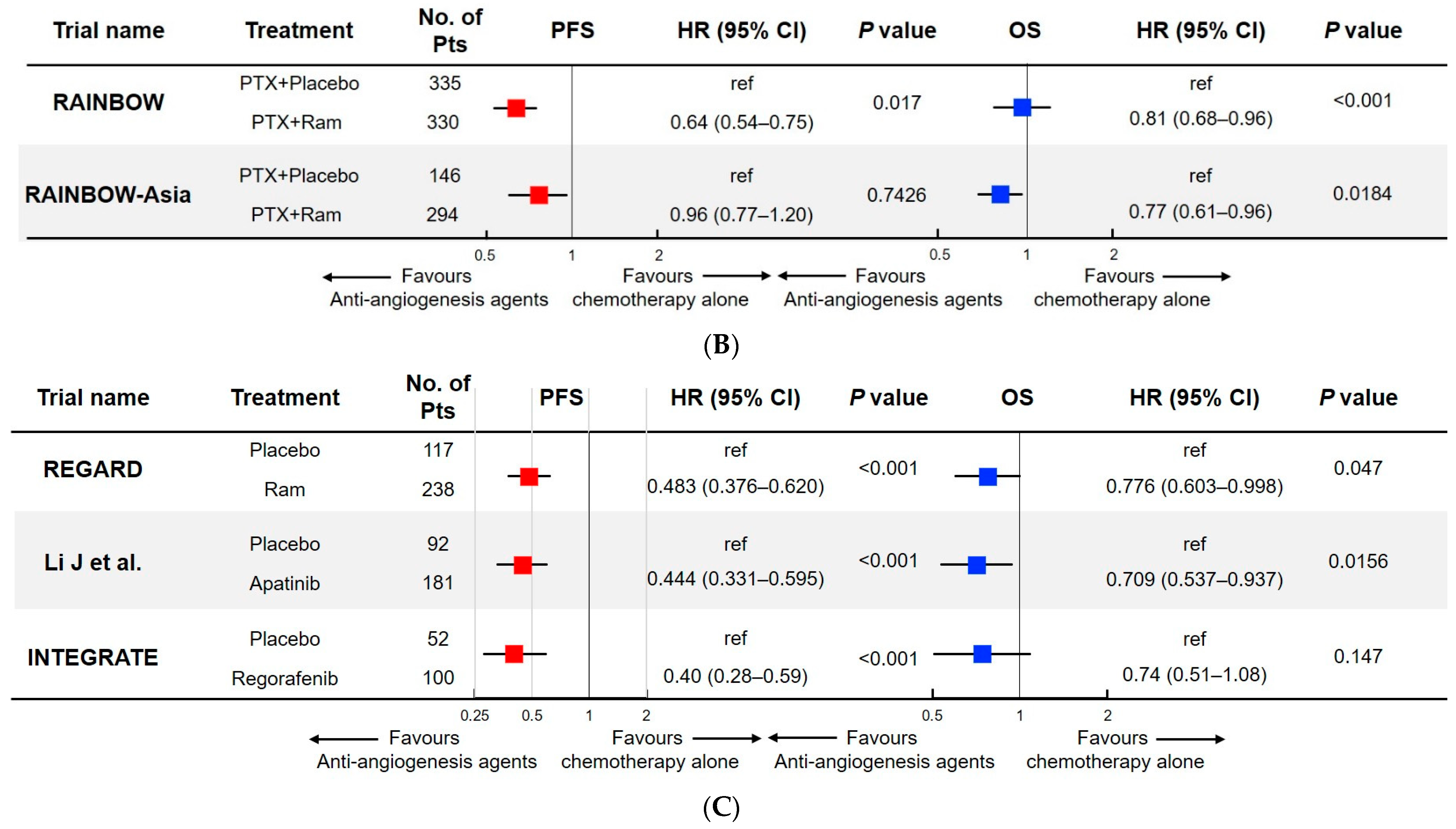
| RAGERD | III | Ram vs. Placebo | 2L | 238 (Ram) vs. 117 (PBO) | OS | 5.2 (IQR 2.3–9.9) vs. 3.8 (IQR 1.7–7.1) | 0.78 (0.60–0.99) p = 0.047 | 2.1 (IQR 5.9–7.1) vs. 1.3 (IQR 1.3–4.2) | positive | |||
| RAINBOW | III | Ram + PTX vs. Placebo + PTX | 2L | 330 (Ram) vs. 335 (PBO) | OS | 9.6 (8.5–10.8) vs. 7.4 (6.3–8.4) | 0.81 (0.68–0.96) p = 0.017 | 4.4 (4.2–5.3) vs. 2.9 (2.8–3.0) | 0.64 (0.54–0.75) p < 0.001 | 28 (23–33) vs. 16 (13–20) | p = 0.315 | positive |
| RAINBOW-Asia | III | Ram + PTX vs. Placebo + PTX | 2L | 294 (Ram) vs. 146 (PBO) | OS/PFS | 8.7 (8.0–9.5) vs. 7.9 (6.3–9.1) | 0.96 (0.77–1.20) p = 0.7426 | 4.1 (3.7–4.3) vs. 3.2 (2.8–4.1) | 0.77 (0.61–0.96) p = 0.0184 | 27 (21–32) vs. 22 (16–30) | negative | |
| RAINFALL | III | Ram + XP or FP vs. Placebo + XP or FP | 1L | 326 (Ram) vs. 319 (PBO) | PFS | 11.2 (9.9–11.9) vs. 10.7 (9.5–11.9) | 0.96 (0.80–1.16) p = 0.68 | 5.7 (5.5–6.5) vs. 5.4 (4.5–5.7) | 0.75 (0.61–0.94) p = 0.011 | 41 (36–46) vs. 36 (31–42) | p = 0.17 | positive |
| RAINSTORM | rII | Ram + SOX vs. Placebo + SOX | 1L | 96 (Ram) vs. 93 (PBO) | PFS | 14.7 vs. 14.3 | 1.11 (80% CI 0.89–1.40) p = 0.55 | 6.3 vs. 6.7 | 1.07 (80% CI 0.86–1.33) p = 0.70 | 58 vs. 50 | 1.37 (80% CI; 0.84–2.24) p = 0.40 | negative |
| JVBT | rII | Ram + mFOLFOX6 vs. Placebo + mFOLFOX6 | 1L | 84 (Ram) vs. 84 (PBO) | PFS | 11.7 vs. 11.5 | 1.08 (95% CI 0.73–1.58) p = 0.712 | 6.4 vs. 6.7 | 0.98 (95% CI 0.69–1.37) p = 0.886 | 45.2 (34.3–56.5) vs. 46.4 (35.5–57.6) | p = 0.830 | negative |
| Bando H, et al. | II | Ram + nab-PTX | 2L | 45 | ORR | NR | 7.6 (5.4–8.1) | 54.8 (41.0–68.0) | positive | |||
| RAMIRIS | II | Ram +FOLFIRI vs. Ram +PTX | 2L | 72 (FOLFIRI) vs. 38 (PTX) | OS at 6 m | 6.8 (5.1–11.1) vs. 7.6 (6.1–11.5) | 0.97 (95% CI 0.62–1.52) | 3.9 (2.8–6.8) vs. 3.7 (2.1–5.5) | 0.73 (95% CI 0.48–1.11) | 22 vs. 11 | negative | |
| HGCSG1603 | II | Ram + IRI | 2L | 35 | PFS at 6 m | 9.6 (6.4–16.6) | 4.2 (2.5–5.4) | 25.9 (11.1–36.3) | negative | |||
| Kawazoe A, et al. | II | Ram + FTD/TPI (Cohort A/B) | 2L/≥3L | 33 (A)/31 (B) | DCR | A; 5.9 (4.2–7.9) B; 5.3 (2.8–6.0) | DCR 85 (68–95)/77 (59–90) | positive | ||||
| Apatinib/Regorafenib | ||||||||||||
| Li J, et al. | rII | Placebo (Group A) Apatinib 850mg (Group B) Apatinib 425mg (Group C) | ≥3L | 46 (A) 47 (B) 48 (C) | PFS | A; 2.50 (1.87–3.70) B; 4.83 (4.03–5.97) C; 4.27 (3.83–4.77) | B vs. A 0.37 (0.22–0.62) p = 0.0017 C vs. A 0.41 (0.24–0.72) p = 0.119 | A; 1.40 (1.20–1.83) B; 3.67 (2.17–6.80) C; 3.20 (2.37–4.53) | B vs. A 0.18 (0.10–0.34) p < 0.001 C vs. A 0.21 (0.11–0.38) p < 0.001 | A; 0.00 (0.0–7.4) B; 6.38 (1.3–17.5) C; 13.04 (4.9–26.3) | positive | |
| Li J, et al. | III | Apatinib vs. BSC | ≥3L | 181 (RAM) vs. 92 (PBO) | OS/PFS | 6.5 (4.8–7.6) vs. 4.7 (3.6–5.4) | 0.709 (0.537–0.937), p = 0.0156 | 2.6 (2.0–2.9) vs. 1.8 (1.4–1.9) | 0.444 (0.331–0.595) p < 0.001 | 2.84 (investigator) vs. 0.00 (investigator) | p = 0.1695 | positive |
| INTEGRATE | rII | Regorafenib vs. BSC | ≥2L | 100 (Rego) vs. 52 (PBO) | PFS | 5.8 (4.4–6.8) vs. 4.5 (3.4–5.2) | 0.74 (0.51–1.08), p = 0.147 | 2.6 (1.8–3.1) vs. 0.9 (0.9–0.9) | 0.40 (0.28–0.59) p < 0.001 | positive | ||
| Trial Name/Authors | Ph | Antiangiogenesis Agent | Immunotherapy | Chemotherapy | Line | No. of Patients | MST (95% CI) (Months) | mPFS (95% CI) (Months) | ORR (95% CI) (%) |
|---|---|---|---|---|---|---|---|---|---|
| JVDF | I | Ramucirumab | Pembrolizumab | none | 1L | 28 | 14.6 (5.4–27.7) | 5.6 (3.9–12.3) | 25 (10.7–44.9) |
| EPOC1706 | II | Lenvatinib | Pembrolizumab | none | 1L/2L | 29 | NR (11.8–NR) | 7.1 (5.4–13.7) | 69 (49–85) |
| NivoRam | I/II | Ramucirumab | Nivolumab | none | 2L | 46 | 9 | 2.9 | 26.7 |
| Xu J et al. | I | Apatinib | SHR1210 | none | 2L | 23 | 11.4 (8.6–NR) | 2.9 (2.5–4.2) | 17.4 (5.0–38.9) |
| Nakajima T, et al. | I/II | Ramucirumab | Nivolumab | Paclitaxel | 2L | 43 | 13.1 (8.0–16.6) | 5.1 (4.5–6.5) | 37.2 (23.0–53.5) |
| JVDJ | I | Ramucirumab | Duruvalumab | none | ≥2L | 29 | 12.4 (5.5–16.9) | 2.6 (1.5–7.1) | 21 |
| REGOMUNE | II | Regorafenib | Avelumab | none | ≥2L | 49 | 7.5 (4.5–15.7) | 1.9 (1.8–3.5) | 16.7 |
| JVDF | I | Ramucirumab | Pembrolizumab | none | ≥2L | 41 | 5.9 (4.4–10.6) | 2.5 (1.5–4.2) | 7 (1.5–19.9) |
| REGONIVO | I | Regorafenib | Nivolumab | none | ≥3L | 25 | 12.3 (5.3–NR) | 5.6 (2.7–10.4) | 44 (24.4–65.1) |
| Trial Name | Ph | Anti-Angiogenic Agent | Immunotherapy | Chemotherapy | Line | No. of Patients | Primary Endpoint | ClinicalTrials.gov Identifier |
|---|---|---|---|---|---|---|---|---|
| IMMUNOGAST | II | Bevacizumab | Atezolizumab | none | ≥2L | 60 | ORR | NCT04739202 |
| 2020-03-115 | II | Ramucirumab | Pembrolizumab | none | 2L/3L | 35 | ORR | NCT04632459 |
| SEQUEL | rII | Ramucirumab | Pembrolizumab | Paclitaxel | 2L | 58 | ORR | NCT04069273 |
| AIO-STO-0218 | I | Ramucirumab | Avelumab | Paclitaxel | 2L | 59 | OS at 6 months | NCT03966118 |
| AHQU-2022001 | II | Apatinib | Sintilimab | SOX | 1L | 31 | ORR | NCT05216237 |
| FDZL-CAP | rII | Apatinib | Camrelizumab | none | 3L | 102 | PFS | NCT05095636 |
| MA-GC-II-011 | II | Apatinib | Camrelizumab | none | ≥2L | 20 | ORR | NCT04948125 |
| PD-1-APTN-II-AFPGC | II | Apatinib | Camrelizumab | none | ≥2L | 30 | ORR | NCT04006821 |
| NFEC-2020-024 | II | Apatinib | Camrelizumab | Irinotecan | 2L | 85 | OS | NCT04934618 |
| HCCSC G05 | Apatinib | Camrelizumab | S1 + Docetaxel | 1L | 35 | PFS | NCT04781686 | |
| INTEGRATEIIb | rIII | Regorafenib | Nivolumab | none | ≥3L | 450 | OS | NCT04879368 |
| 17-00626 | II | Lenvatinib | Pembrolizumab | none | ≥2L | 24 | ORR | NCT03321630 |
| NCI-2021-09188 | Lenvatinib | Pembrolizumab | none | ≥2L | 15 | ORR | NCT05041153 | |
| LEAP-015 | Lenvatinib | Pembrolizumab | CAPOX/FOLFOX | 1 | 890 | OS (Part 2) | NCT04662710 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakayama, I.; Takahari, D. The Role of Angiogenesis Targeted Therapies in Metastatic Advanced Gastric Cancer: A Narrative Review. J. Clin. Med. 2023, 12, 3226. https://doi.org/10.3390/jcm12093226
Nakayama I, Takahari D. The Role of Angiogenesis Targeted Therapies in Metastatic Advanced Gastric Cancer: A Narrative Review. Journal of Clinical Medicine. 2023; 12(9):3226. https://doi.org/10.3390/jcm12093226
Chicago/Turabian StyleNakayama, Izuma, and Daisuke Takahari. 2023. "The Role of Angiogenesis Targeted Therapies in Metastatic Advanced Gastric Cancer: A Narrative Review" Journal of Clinical Medicine 12, no. 9: 3226. https://doi.org/10.3390/jcm12093226