
Metabolic Support in Acute Respiratory Distress Syndrome: A Narrative Review

Abstract
:1. Introduction
2. Artificial Nutrition Pitfalls in Critical Illness Patients
2.1. The Determinants of Energy Consumption
2.2. Diet-Induced Thermogenesis (DIT)
2.3. Resting Energy Expenditure (REE)
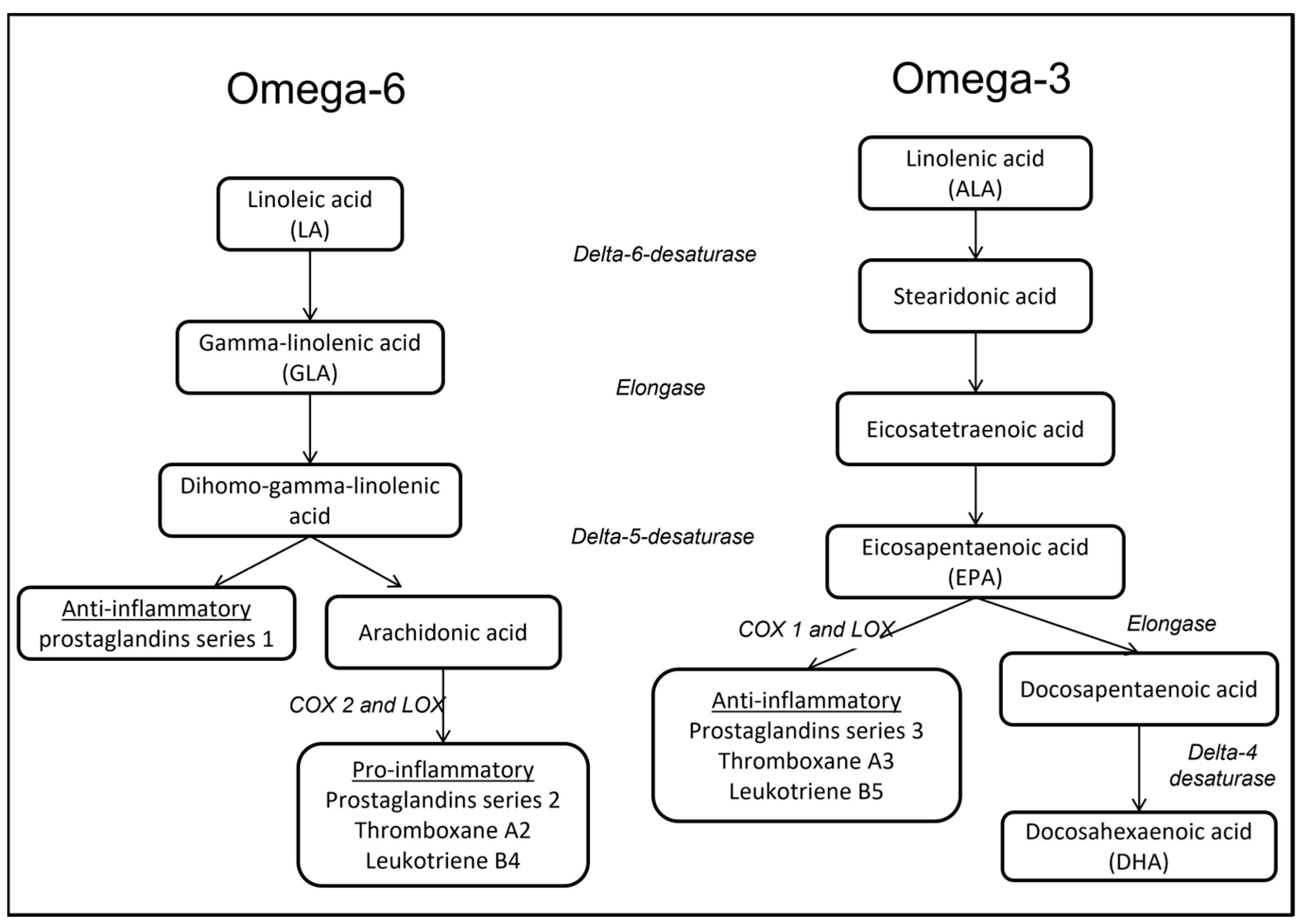
2.4. Polyunsaturated Fatty Acids
3. Peculiarity of Artificial Nutrition in Acute Respiratory Failure
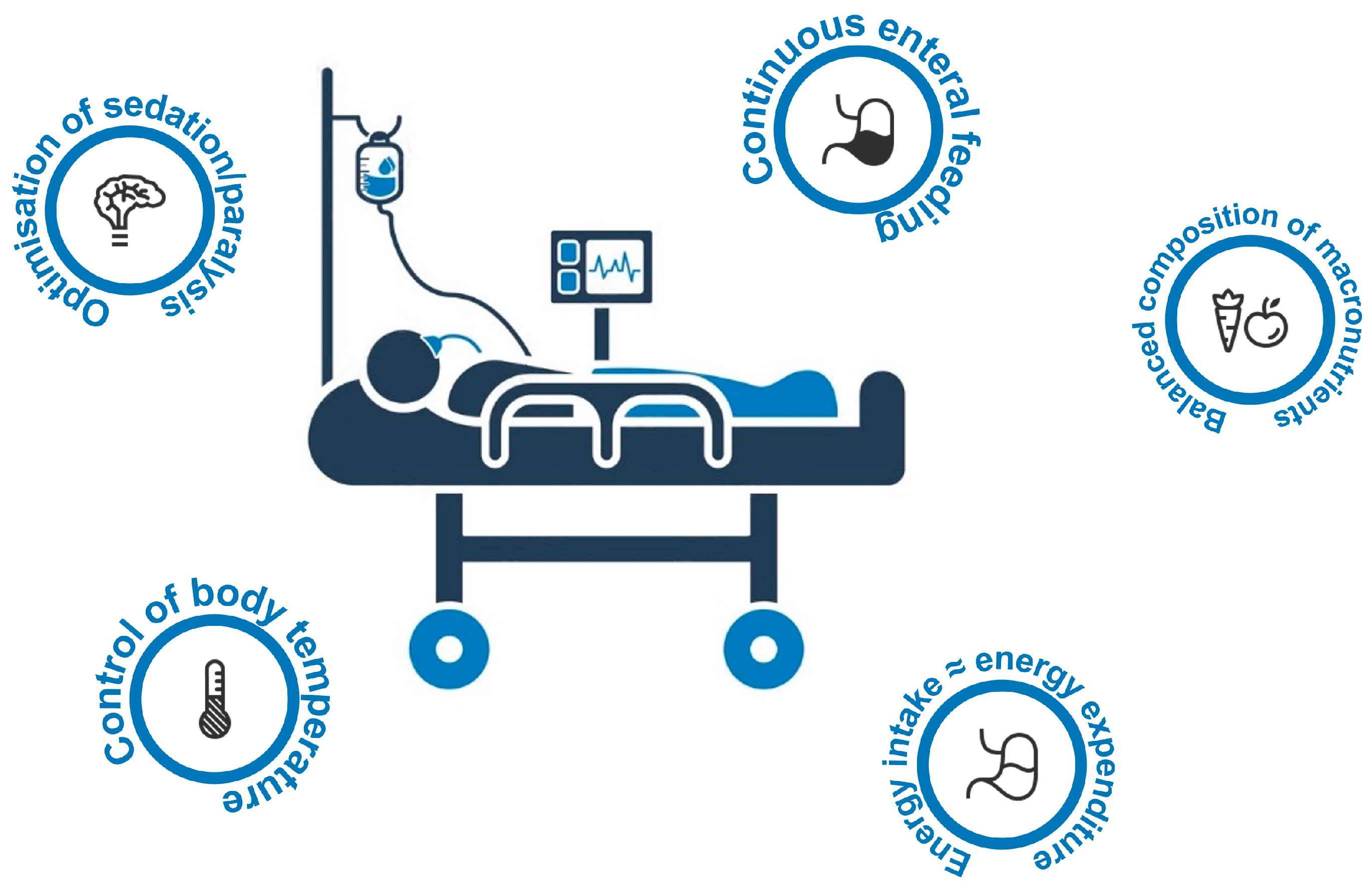
4. Metabolic Control in ARDS Patients
5. Special Issues Related to SARS-CoV-2 Infection
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kreymann, K.G.; Berger, M.M.; Deutz, N.E.; Hiesmayr, M.; Jolliet, P.; Kazandjiev, G.; Nitenberg, G.; van den Berghe, G.; Wernerman, J.; Ebner, C.; et al. ESPEN Guidelines on Enteral Nutrition: Intensive Care. Clin. Nutr. 2006, 25, 210–223. [Google Scholar] [CrossRef] [PubMed]
- Reignier, J.; Plantefeve, G.; Mira, J.-P.; Argaud, L.; Asfar, P.; Aissaoui, N.; Badie, J.; Botoc, N.-V.; Brisard, L.; Bui, H.-N.; et al. Low versus Standard Calorie and Protein Feeding in Ventilated Adults with Shock: A Randomised, Controlled, Multicentre, Open-Label, Parallel-Group Trial (NUTRIREA-3). Lancet Respir. Med. 2023. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, L.; Millar, A.B. Relative Production of Tumour Necrosis Factor Alpha and Interleukin 10 in Adult Respiratory Distress Syndrome. Thorax 1997, 52, 442–446. [Google Scholar] [CrossRef]
- Nandi, J.; Meguid, M.M.; Inui, A.; Xu, Y.; Makarenko, I.G.; Tada, T.; Chen, C. Central Mechanisms Involved with Catabolism. Curr. Opin. Clin. Nutr. Metab. Care 2002, 5, 407–418. [Google Scholar] [CrossRef]
- Dungan, K.M.; Braithwaite, S.S.; Preiser, J.C. Stress Hyperglycaemia. Lancet 2009, 373, 1798–1807. [Google Scholar] [CrossRef] [PubMed]
- Casaer, M.P.; Mesotten, D.; Hermans, G.; Wouters, P.J.; Schetz, M.; Meyfroidt, G.; Van Cromphaut, S.; Ingels, C.; Meersseman, P.; Muller, J.; et al. Early versus Late Parenteral Nutrition in Critically Ill Adults. N. Engl. J. Med. 2011, 365, 506–517. [Google Scholar] [CrossRef]
- Fivez, T.; Kerklaan, D.; Mesotten, D.; Verbruggen, S.; Wouters, P.J.; Vanhorebeek, I.; Debaveye, Y.; Vlasselaers, D.; Desmet, L.; Casaer, M.P.; et al. Early versus Late Parenteral Nutrition in Critically Ill Children. N. Engl. J. Med. 2016, 374, 1111–1122. [Google Scholar] [CrossRef]
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network; Rice, T.W.; Wheeler, A.P.; Thompson, B.T.; Steingrub, J.; Hite, R.D.; Moss, M.; Morris, A.; Dong, N.; Rock, P. Initial Trophic vs Full Enteral Feeding in Patients with Acute Lung Injury: The EDEN Randomized Trial. JAMA 2012, 307, 795–803. [Google Scholar] [CrossRef]
- Arabi, Y.M.; Aldawood, A.S.; Al-Dorzi, H.M.; Tamim, H.M.; Haddad, S.H.; Jones, G.; McIntyre, L.; Solaiman, O.; Sakkijha, M.H.; Sadat, M.; et al. Permissive Underfeeding or Standard Enteral Feeding in High- and Low-Nutritional-Risk Critically Ill Adults. Post Hoc Analysis of the PermiT Trial. Am. J. Respir. Crit. Care Med. 2017, 195, 652–662. [Google Scholar] [CrossRef]
- TARGET Investigators, for the ANZICS Clinical Trials Group; Chapman, M.; Peake, S.L.; Bellomo, R.; Davies, A.; Deane, A.; Horowitz, M.; Hurford, S.; Lange, K.; Little, L.; et al. Energy-Dense versus Routine Enteral Nutrition in the Critically Ill. N. Engl. J. Med. 2018, 379, 1823–1834. [Google Scholar] [CrossRef]
- Arabi, Y.M.; Haddad, S.H.; Aldawood, A.S.; Al-Dorzi, H.M.; Tamim, H.M.; Sakkijha, M.; Jones, G.; McIntyre, L.; Mehta, S.; Solaiman, O.; et al. Permissive Underfeeding versus Target Enteral Feeding in Adult Critically Ill Patients (PermiT Trial): A Study Protocol of a Multicenter Randomized Controlled Trial. Trials 2012, 13, 191. [Google Scholar] [CrossRef] [PubMed]
- Rice, T.W.; Mogan, S.; Hays, M.A.; Bernard, G.R.; Jensen, G.L.; Wheeler, A.P. Randomized Trial of Initial Trophic versus Full-Energy Enteral Nutrition in Mechanically Ventilated Patients with Acute Respiratory Failure. Crit. Care Med. 2011, 39, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Braunschweig, C.A.; Sheean, P.M.; Peterson, S.J.; Perez, S.G.; Freels, S.; Lateef, O.; Gurka, D.; Fantuzzi, G. Intensive Nutrition in Acue Lung Injury: A Clinical Trial (INTACT). JPEN J. Parenter. Enter. Nutr. 2015, 39, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Gunst, J.; Casaer, M.P.; Preiser, J.-C.; Reignier, J.; Van den Berghe, G. Toward Nutrition Improving Outcome of Critically Ill Patients: How to Interpret Recent Feeding RCTs? Crit. Care 2023, 27, 43. [Google Scholar] [CrossRef] [PubMed]
- Compher, C.; Nicolo, M.; Chittams, J.; Kang, Y.; Day, A.G.; Heyland, D.K. Clinical Outcomes in Critically Ill Patients Associated With the Use of Complex vs Weight-Only Predictive Energy Equations. JPEN J. Parenter. Enter. Nutr. 2015, 39, 864–869. [Google Scholar] [CrossRef]
- Reignier, J.; Boisramé-Helms, J.; Brisard, L.; Lascarrou, J.-B.; Ait Hssain, A.; Anguel, N.; Argaud, L.; Asehnoune, K.; Asfar, P.; Bellec, F.; et al. Enteral versus Parenteral Early Nutrition in Ventilated Adults with Shock: A Randomised, Controlled, Multicentre, Open-Label, Parallel-Group Study (NUTRIREA-2). Lancet 2018, 391, 133–143. [Google Scholar] [CrossRef]
- Fong, K.M.; Au, S.Y.; Ng, G.W.Y. Glycemic Control in Critically Ill Patients with or without Diabetes. BMC Anesth. 2022, 22, 227. [Google Scholar] [CrossRef]
- Moisey, L.L.; Merriweather, J.L.; Drover, J.W. The Role of Nutrition Rehabilitation in the Recovery of Survivors of Critical Illness: Underrecognized and Underappreciated. Crit. Care 2022, 26, 270. [Google Scholar] [CrossRef]
- Slingerland-Boot, R.; van der Heijden, I.; Schouten, N.; Driessen, L.; Meijer, S.; Mensink, M.; van Zanten, A. Prospective Observational Cohort Study of Reached Protein and Energy Targets in General Wards during the Post-Intensive Care Period: The PROSPECT-I Study. Clin. Nutr. 2022, 41, 2124–2134. [Google Scholar] [CrossRef]
- Berger, M.M.; Shenkin, A.; Schweinlin, A.; Amrein, K.; Augsburger, M.; Biesalski, H.-K.; Bischoff, S.C.; Casaer, M.P.; Gundogan, K.; Lepp, H.-L.; et al. ESPEN Micronutrient Guideline. Clin. Nutr. 2022, 41, 1357–1424. [Google Scholar] [CrossRef]
- Bertolini, G.; Iapichino, G.; Radrizzani, D.; Facchini, R.; Simini, B.; Bruzzone, P.; Zanforlin, G.; Tognoni, G. Early Enteral Immunonutrition in Patients with Severe Sepsis: Results of an Interim Analysis of a Randomized Multicentre Clinical Trial. Intensive Care Med. 2003, 29, 834–840. [Google Scholar] [CrossRef] [PubMed]
- Iapichino, G.; Radrizzani, D.; Armani, S.; Noto, A.; Spanu, P.; Mistraletti, G. Metabolic Treatment of Critically Ill Patients: Energy Balance and Substrate Disposal. Minerva Anestesiol. 2006, 72, 533–541. [Google Scholar]
- Iapichino, G.; Radrizzani, D.; Giacomini, M.; Pezzi, A.; Zaniboni, M.; Mistraletti, G. Metabolic Treatment of Critically Ill Patients: Energy Expenditure and Energy Supply. Minerva Anestesiol. 2006, 72, 559–565. [Google Scholar] [PubMed]
- Westerterp, K.R. Control of Energy Expenditure in Humans. Eur. J. Clin. Nutr. 2017, 71, 340–344. [Google Scholar] [CrossRef]
- Cahill, G.F., Jr. Fuel Metabolism in Starvation. Annu. Rev. Nutr. 2006, 26, 1–22. [Google Scholar] [CrossRef]
- Westerterp, K.R. Diet Induced Thermogenesis. Nutr. Metab. (Lond.) 2004, 1, 5. [Google Scholar] [CrossRef]
- Jequier, E. The Influence of Nutrient Administration on Energy Expenditure in Man. Clin. Nutr. 1986, 5, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Fraipont, V.; Preiser, J.C. Energy Estimation and Measurement in Critically Ill Patients. JPEN J. Parenter. Enter. Nutr. 2013, 37, 705–713. [Google Scholar] [CrossRef]
- Wei, X.; Day, A.G.; Ouellette-Kuntz, H.; Heyland, D.K. The Association Between Nutritional Adequacy and Long-Term Outcomes in Critically Ill Patients Requiring Prolonged Mechanical Ventilation: A Multicenter Cohort Study. Crit. Care Med. 2015, 43, 1569–1579. [Google Scholar] [CrossRef]
- Heyland, D.K.; Cahill, N.; Day, A.G. Optimal Amount of Calories for Critically Ill Patients: Depends on How You Slice the Cake! Crit. Care Med. 2011, 39, 2619–2626. [Google Scholar] [CrossRef]
- Villet, S.; Chiolero, R.L.; Bollmann, M.D.; Revelly, J.P.; Cayeux, R.N.M.; Delarue, J.; Berger, M.M. Negative Impact of Hypocaloric Feeding and Energy Balance on Clinical Outcome in ICU Patients. Clin. Nutr. 2005, 24, 502–509. [Google Scholar] [CrossRef] [PubMed]
- De Waele, E.; Opsomer, T.; Honore, P.M.; Diltoer, M.; Mattens, S.; Huyghens, L.; Spapen, H. Measured versus Calculated Resting Energy Expenditure in Critically Ill Adult Patients. Do Mathematics Match the Gold Standard? Minerva Anestesiol. 2015, 81, 272–282. [Google Scholar] [PubMed]
- Weir, J.B. New Methods for Calculating Metabolic Rate with Special Reference to Protein Metabolism. J. Physiol. 1949, 109, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Alberda, C.; Gramlich, L.; Jones, N.; Jeejeebhoy, K.; Day, A.G.; Dhaliwal, R.; Heyland, D.K. The Relationship between Nutritional Intake and Clinical Outcomes in Critically Ill Patients: Results of an International Multicenter Observational Study. Intensive Care Med. 2009, 35, 1728–1737. [Google Scholar] [CrossRef]
- Dvir, D.; Cohen, J.; Singer, P. Computerized Energy Balance and Complications in Critically Ill Patients: An Observational Study. Clin. Nutr. 2006, 25, 37–44. [Google Scholar] [CrossRef]
- Stapleton, R.D.; Martin, T.R.; Weiss, N.S.; Crowley, J.J.; Gundel, S.J.; Nathens, A.B.; Akhtar, S.R.; Ruzinski, J.T.; Caldwell, E.; Curtis, J.R.; et al. A Phase II Randomized Placebo-Controlled Trial of Omega-3 Fatty Acids for the Treatment of Acute Lung Injury. Crit. Care Med. 2011, 39, 1655–1662. [Google Scholar] [CrossRef]
- Weijs, P.J.; Stapel, S.N.; de Groot, S.D.; Driessen, R.H.; de Jong, E.; Girbes, A.R.; Strack van Schijndel, R.J.; Beishuizen, A. Optimal Protein and Energy Nutrition Decreases Mortality in Mechanically Ventilated, Critically Ill Patients: A Prospective Observational Cohort Study. JPEN J. Parenter. Enter. Nutr. 2012, 36, 60–68. [Google Scholar] [CrossRef]
- Allingstrup, M.J.; Esmailzadeh, N.; Wilkens Knudsen, A.; Espersen, K.; Hartvig Jensen, T.; Wiis, J.; Perner, A.; Kondrup, J. Provision of Protein and Energy in Relation to Measured Requirements in Intensive Care Patients. Clin. Nutr. 2012, 31, 462–468. [Google Scholar] [CrossRef]
- Zusman, O.; Theilla, M.; Cohen, J.; Kagan, I.; Bendavid, I.; Singer, P. Resting Energy Expenditure, Calorie and Protein Consumption in Critically Ill Patients: A Retrospective Cohort Study. Crit. Care 2016, 20, 367. [Google Scholar] [CrossRef]
- Compher, C.; Chittams, J.; Sammarco, T.; Nicolo, M.; Heyland, D.K. Greater Protein and Energy Intake May Be Associated With Improved Mortality in Higher Risk Critically Ill Patients: A Multicenter, Multinational Observational Study. Crit. Care Med. 2017, 45, 156–163. [Google Scholar] [CrossRef]
- Koekkoek, W.A.C.K.; van Setten, C.H.C.; Olthof, L.E.; Kars, J.C.N.H.; van Zanten, A.R.H. Timing of PROTein INtake and Clinical Outcomes of Adult Critically Ill Patients on Prolonged Mechanical VENTilation: The PROTINVENT Retrospective Study. Clin. Nutr. 2019, 38, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Hartl, W.H.; Kopper, P.; Bender, A.; Scheipl, F.; Day, A.G.; Elke, G.; Küchenhoff, H. Protein Intake and Outcome of Critically Ill Patients: Analysis of a Large International Database Using Piece-Wise Exponential Additive Mixed Models. Crit. Care 2022, 26, 7. [Google Scholar] [CrossRef] [PubMed]
- Brandi, L.S.; Bertolini, R.; Calafa, M. Indirect Calorimetry in Critically Ill Patients: Clinical Applications and Practical Advice. Nutrition 1997, 13, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Delsoglio, M.; Achamrah, N.; Berger, M.M.; Pichard, C. Indirect Calorimetry in Clinical Practice. J. Clin. Med. 2019, 8, 1387. [Google Scholar] [CrossRef]
- Simonson, D.C.; DeFronzo, R.A. Indirect Calorimetry: Methodological and Interpretative Problems. Am. J. Physiol. 1990, 258, E399–E412. [Google Scholar] [CrossRef]
- Wischmeyer, P.E.; Molinger, J.; Haines, K. Point-Counterpoint: Indirect Calorimetry Is Essential for Optimal Nutrition Therapy in the Intensive Care Unit. Nutr. Clin. Pr. 2021, 36, 275–281. [Google Scholar] [CrossRef]
- Singer, P.; Anbar, R.; Cohen, J.; Shapiro, H.; Shalita-Chesner, M.; Lev, S.; Grozovski, E.; Theilla, M.; Frishman, S.; Madar, Z. The Tight Calorie Control Study (TICACOS): A Prospective, Randomized, Controlled Pilot Study of Nutritional Support in Critically Ill Patients. Intensive Care Med. 2011, 37, 601–609. [Google Scholar] [CrossRef]
- Lindner, M.; Geisler, C.; Rembarz, K.; Hummitzsch, L.; Radke, D.I.; Schulte, D.M.; Müller, M.J.; Bosy-Westphal, A.; Elke, G. Resting Energy Expenditure in the Critically Ill and Healthy Elderly-A Retrospective Matched Cohort Study. Nutrients 2023, 15, 303. [Google Scholar] [CrossRef]
- Achamrah, N.; Delsoglio, M.; De Waele, E.; Berger, M.M.; Pichard, C. Indirect Calorimetry: The 6 Main Issues. Clin. Nutr. 2021, 40, 4–14. [Google Scholar] [CrossRef]
- Pielmeier, U.; Andreassen, S. VCO2 Calorimetry Is a Convenient Method for Improved Assessment of Energy Expenditure in the Intensive Care Unit. Crit. Care 2016, 20, 224. [Google Scholar] [CrossRef]
- Singer, P.; Berger, M.M.; Van den Berghe, G.; Biolo, G.; Calder, P.; Forbes, A.; Griffiths, R.; Kreyman, G.; Leverve, X.; Pichard, C.; et al. ESPEN Guidelines on Parenteral Nutrition: Intensive Care. Clin. Nutr. 2009, 28, 387–400. [Google Scholar] [CrossRef] [PubMed]
- Radrizzani, D.; Iapichino, G. Every Need Is Perfectly Met If You Do Not Measure It. Minerva Anestesiol. 2015, 81, 253–254. [Google Scholar]
- Calder, P.C. N-3 Fatty Acids, Inflammation, and Immunity--Relevance to Postsurgical and Critically Ill Patients. Lipids 2004, 39, 1147–1161. [Google Scholar] [CrossRef] [PubMed]
- Venus, B.; Smith, R.A.; Patel, C.; Sandoval, E. Hemodynamic and Gas Exchange Alterations during Intralipid Infusion in Patients with Adult Respiratory Distress Syndrome. Chest 1989, 95, 1278–1281. [Google Scholar] [CrossRef]
- Gadek, J.E.; DeMichele, S.J.; Karlstad, M.D.; Pacht, E.R.; Donahoe, M.; Albertson, T.E.; Van Hoozen, C.; Wennberg, A.K.; Nelson, J.L.; Noursalehi, M. Effect of Enteral Feeding with Eicosapentaenoic Acid, Gamma-Linolenic Acid, and Antioxidants in Patients with Acute Respiratory Distress Syndrome. Enteral Nutrition in ARDS Study Group. Crit. Care Med. 1999, 27, 1409–1420. [Google Scholar] [CrossRef]
- Mathru, M.; Dries, D.J.; Zecca, A.; Fareed, J.; Rooney, M.W.; Rao, T.L. Effect of Fast vs Slow Intralipid Infusion on Gas Exchange, Pulmonary Hemodynamics, and Prostaglandin Metabolism. Chest 1991, 99, 426–429. [Google Scholar] [CrossRef]
- Djuricic, I.; Calder, P.C. Beneficial Outcomes of Omega-6 and Omega-3 Polyunsaturated Fatty Acids on Human Health: An Update for 2021. Nutrients 2021, 13, 2421. [Google Scholar] [CrossRef] [PubMed]
- Rosa Neto, J.C.; Calder, P.C.; Curi, R.; Newsholme, P.; Sethi, J.K.; Silveira, L.S. The Immunometabolic Roles of Various Fatty Acids in Macrophages and Lymphocytes. Int. J. Mol. Sci. 2021, 22, 8460. [Google Scholar] [CrossRef] [PubMed]
- Takala, J.; Askanazi, J.; Weissman, C.; Lasala, P.A.; Milic-Emili, J.; Elwyn, D.H.; Kinney, J.M. Changes in Respiratory Control Induced by Amino Acid Infusions. Crit. Care Med. 1988, 16, 465–469. [Google Scholar] [CrossRef]
- Luiking, Y.C.; Poeze, M.; Ramsay, G.; Deutz, N.E.P. The Role of Arginine in Infection and Sepsis. JPEN J. Parenter. Enter. Nutr. 2005, 29, S70–S74. [Google Scholar] [CrossRef]
- Gorman, E.A.; O’Kane, C.M.; McAuley, D.F. Acute Respiratory Distress Syndrome in Adults: Diagnosis, Outcomes, Long-Term Sequelae, and Management. Lancet 2022, 400, 1157–1170. [Google Scholar] [CrossRef] [PubMed]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute Respiratory Distress Syndrome: The Berlin Definition. Jama 2012, 307, 2526–2533. [Google Scholar] [CrossRef] [PubMed]
- Krzak, A.; Pleva, M.; Napolitano, L.M. Nutrition Therapy for ALI and ARDS. Crit. Care Clin. 2011, 27, 647–659. [Google Scholar] [CrossRef] [PubMed]
- Aubier, M.; Murciano, D.; Lecocguic, Y.; Viires, N.; Jacquens, Y.; Squara, P.; Pariente, R. Effect of Hypophosphatemia on Diaphragmatic Contractility in Patients with Acute Respiratory Failure. N. Engl. J. Med. 1985, 313, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Pingleton, S.K.; Harmon, G.S. Nutritional Management in Acute Respiratory Failure. Jama 1987, 257, 3094–3099. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.O.; Rogers, R.M.; Sanders, M.H.; Pennock, B.E.; Reilly, J.J. Nutritional Intervention in Malnourished Patients with Emphysema. Am. Rev. Respir. Dis. 1986, 134, 672–677. [Google Scholar] [CrossRef]
- Askanazi, J.; Elwyn, D.H.; Silverberg, P.A.; Rosenbaum, S.H.; Kinney, J.M. Respiratory Distress Secondary to a High Carbohydrate Load: A Case Report. Surgery 1980, 87, 596–598. [Google Scholar]
- Askanazi, J.; Nordenstrom, J.; Rosenbaum, S.H.; Elwyn, D.H.; Hyman, A.I.; Carpentier, Y.A.; Kinney, J.M. Nutrition for the Patient with Respiratory Failure: Glucose vs. Fat. Anesthesiology 1981, 54, 373–377. [Google Scholar] [CrossRef]
- al-Saady, N.M.; Blackmore, C.M.; Bennett, E.D. High Fat, Low Carbohydrate, Enteral Feeding Lowers PaCO2 and Reduces the Period of Ventilation in Artificially Ventilated Patients. Intensive Care Med. 1989, 15, 290–295. [Google Scholar] [CrossRef]
- Garrel, D.R.; Razi, M.; Lariviere, F.; Jobin, N.; Naman, N.; Emptoz-Bonneton, A.; Pugeat, M.M. Improved Clinical Status and Length of Care with Low-Fat Nutrition Support in Burn Patients. JPEN J. Parenter. Enter. Nutr. 1995, 19, 482–491. [Google Scholar] [CrossRef]
- Hart, D.W.; Wolf, S.E.; Zhang, X.J.; Chinkes, D.L.; Buffalo, M.C.; Matin, S.I.; DebRoy, M.A.; Wolfe, R.R.; Herndon, D.N. Efficacy of a High-Carbohydrate Diet in Catabolic Illness. Crit. Care Med. 2001, 29, 1318–1324. [Google Scholar] [CrossRef] [PubMed]
- Wolf, S.E.; Shields, B.A.; Wade, C.E. Substrate Utilization in the Critically Ill. JPEN J. Parenter. Enter. Nutr. 2009, 33, 111. [Google Scholar] [CrossRef] [PubMed]
- Pendyala, G.; Want, E.J.; Webb, W.; Siuzdak, G.; Fox, H.S. Biomarkers for NeuroAIDS: The Widening Scope of Metabolomics. J. Neuroimmune Pharmacol. Off. J. Soc. NeuroImmune Pharmacol. 2007, 2, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Cox, R., Jr.; Phillips, O.; Fukumoto, J.; Fukumoto, I.; Parthasarathy, P.T.; Arias, S.; Cho, Y.; Lockey, R.F.; Kolliputi, N. Enhanced Resolution of Hyperoxic Acute Lung Injury as a Result of Aspirin Triggered Resolvin D1 Treatment. Am. J. Respir. Cell. Mol. Biol. 2015, 53, 422–435. [Google Scholar] [CrossRef] [PubMed]
- Heidegger, C.P.; Berger, M.M.; Graf, S.; Zingg, W.; Darmon, P.; Costanza, M.C.; Thibault, R.; Pichard, C. Optimisation of Energy Provision with Supplemental Parenteral Nutrition in Critically Ill Patients: A Randomised Controlled Clinical Trial. Lancet 2013, 381, 385–393. [Google Scholar] [CrossRef]
- Petros, S.; Horbach, M.; Seidel, F.; Weidhase, L. Hypocaloric vs Normocaloric Nutrition in Critically Ill Patients: A Prospective Randomized Pilot Trial. JPEN J. Parenter. Enter. Nutr. 2016, 40, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, R.R.; O’Donnell, T.F., Jr.; Stone, M.D.; Richmand, D.A.; Burke, J.F. Investigation of Factors Determining the Optimal Glucose Infusion Rate in Total Parenteral Nutrition. Metab. Clin. Exp. 1980, 29, 892–900. [Google Scholar] [CrossRef] [PubMed]
- Radrizzani, D.; Iapichino, G. Nutrition and Lung Function in the Critically Ill Patient. Clin. Nutr. 1998, 17, 7–10. [Google Scholar] [CrossRef]
- Askanazi, J.; Rosenbaum, S.H.; Michelsen, C.B.; Elwyn, D.H.; Hyman, A.I.; Kinney, J.M. Increased Body Temperature Secondary to Total Parenteral Nutrition. Crit. Care Med. 1980, 8, 736–737. [Google Scholar] [CrossRef]
- Talpers, S.S.; Romberger, D.J.; Bunce, S.B.; Pingleton, S.K. Nutritionally Associated Increased Carbon Dioxide Production. Excess Total Calories vs High Proportion of Carbohydrate Calories. Chest 1992, 102, 551–555. [Google Scholar] [CrossRef]
- Heymsfield, S.B.; Head, C.A.; McManus, C.B., 3rd; Seitz, S.; Staton, G.W.; Grossman, G.D. Respiratory, Cardiovascular, and Metabolic Effects of Enteral Hyperalimentation: Influence of Formula Dose and Composition. Am. J. Clin. Nutr. 1984, 40, 116–130. [Google Scholar] [CrossRef] [PubMed]
- Heymsfield, S.B.; Hill, J.O.; Evert, M.; Casper, K.; DiGirolamo, M. Energy Expenditure during Continuous Intragastric Infusion of Fuel. Am. J. Clin. Nutr. 1987, 45, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Krajmalnik-Brown, R.; Ilhan, Z.-E.; Kang, D.-W.; DiBaise, J.K. Effects of Gut Microbes on Nutrient Absorption and Energy Regulation. Nutr. Clin. Pr. 2012, 27, 201–214. [Google Scholar] [CrossRef] [PubMed]
- Radrizzani, D.; Iapichino, G.; Colombo, A.; Codazzi, D.; Pasetti, G.; Ronzoni, G.; Savioli, M. Effect of Infusion and Withdrawl of Glucose and Insulin on Gas Exchange in Injured Ventilated Patients. J. Crit. Care 1995, 10, 15–20. [Google Scholar] [CrossRef]
- Taylor, B.E.; McClave, S.A.; Martindale, R.G.; Warren, M.M.; Johnson, D.R.; Braunschweig, C.; McCarthy, M.S.; Davanos, E.; Rice, T.W.; Cresci, G.A.; et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). Crit. Care Med. 2016, 44, 390–438. [Google Scholar] [CrossRef]
- Suchner, U.; Katz, D.P.; Furst, P.; Beck, K.; Felbinger, T.W.; Senftleben, U.; Thiel, M.; Goetz, A.E.; Peter, K. Effects of Intravenous Fat Emulsions on Lung Function in Patients with Acute Respiratory Distress Syndrome or Sepsis. Crit. Care Med. 2001, 29, 1569–1574. [Google Scholar] [CrossRef]
- Pacht, E.R.; DeMichele, S.J.; Nelson, J.L.; Hart, J.; Wennberg, A.K.; Gadek, J.E. Enteral Nutrition with Eicosapentaenoic Acid, Gamma-Linolenic Acid, and Antioxidants Reduces Alveolar Inflammatory Mediators and Protein Influx in Patients with Acute Respiratory Distress Syndrome. Crit. Care Med. 2003, 31, 491–500. [Google Scholar] [CrossRef]
- Singer, P.; Theilla, M.; Fisher, H.; Gibstein, L.; Grozovski, E.; Cohen, J. Benefit of an Enteral Diet Enriched with Eicosapentaenoic Acid and Gamma-Linolenic Acid in Ventilated Patients with Acute Lung Injury. Crit. Care Med. 2006, 34, 1033–1038. [Google Scholar] [CrossRef]
- Grau-Carmona, T.; Moran-Garcia, V.; Garcia-de-Lorenzo, A.; Heras-de-la-Calle, G.; Quesada-Bellver, B.; Lopez-Martinez, J.; Gonzalez-Fernandez, C.; Montejo-Gonzalez, J.C.; Blesa-Malpica, A.; Albert-Bonamusa, I.; et al. Effect of an Enteral Diet Enriched with Eicosapentaenoic Acid, Gamma-Linolenic Acid and Anti-Oxidants on the Outcome of Mechanically Ventilated, Critically Ill, Septic Patients. Clin. Nutr. 2011, 30, 578–584. [Google Scholar] [CrossRef]
- Rice, T.W.; Wheeler, A.P.; Thompson, B.T.; deBoisblanc, B.P.; Steingrub, J.; Rock, P. Enteral Omega-3 Fatty Acid, Gamma-Linolenic Acid, and Antioxidant Supplementation in Acute Lung Injury. Jama 2011, 306, 1574–1581. [Google Scholar] [CrossRef]
- Li, C.; Bo, L.; Liu, W.; Lu, X.; Jin, F. Enteral Immunomodulatory Diet (Omega-3 Fatty Acid, Gamma-Linolenic Acid and Antioxidant Supplementation) for Acute Lung Injury and Acute Respiratory Distress Syndrome: An Updated Systematic Review and Meta-Analysis. Nutrients 2015, 7, 5572–5585. [Google Scholar] [CrossRef] [PubMed]
- Compher, C.; Bingham, A.L.; McCall, M.; Patel, J.; Rice, T.W.; Braunschweig, C.; McKeever, L. Guidelines for the Provision of Nutrition Support Therapy in the Adult Critically Ill Patient: The American Society for Parenteral and Enteral Nutrition. JPEN J. Parenter. Enter. Nutr. 2022, 46, 12–41. [Google Scholar] [CrossRef] [PubMed]
- Preiser, J.-C.; Arabi, Y.M.; Berger, M.M.; Casaer, M.; McClave, S.; Montejo-González, J.C.; Peake, S.; Reintam Blaser, A.; Van den Berghe, G.; van Zanten, A.; et al. A Guide to Enteral Nutrition in Intensive Care Units: 10 Expert Tips for the Daily Practice. Crit. Care 2021, 25, 424. [Google Scholar] [CrossRef] [PubMed]
- van Zanten, A.R.H.; Sztark, F.; Kaisers, U.X.; Zielmann, S.; Felbinger, T.W.; Sablotzki, A.R.; De Waele, J.J.; Timsit, J.-F.; Honing, M.L.H.; Keh, D.; et al. High-Protein Enteral Nutrition Enriched with Immune-Modulating Nutrients vs Standard High-Protein Enteral Nutrition and Nosocomial Infections in the ICU: A Randomized Clinical Trial. JAMA 2014, 312, 514–524. [Google Scholar] [CrossRef]
- Heyland, D.; Muscedere, J.; Wischmeyer, P.E.; Cook, D.; Jones, G.; Albert, M.; Elke, G.; Berger, M.M.; Day, A.G. A Randomized Trial of Glutamine and Antioxidants in Critically Ill Patients. N. Engl. J. Med. 2013, 368, 1489–1497. [Google Scholar] [CrossRef]
- Ziegler, T.R.; May, A.K.; Hebbar, G.; Easley, K.A.; Griffith, D.P.; Dave, N.; Collier, B.R.; Cotsonis, G.A.; Hao, L.; Leong, T.; et al. Efficacy and Safety of Glutamine-Supplemented Parenteral Nutrition in Surgical ICU Patients: An American Multicenter Randomized Controlled Trial. Ann. Surg. 2016, 263, 646–655. [Google Scholar] [CrossRef]
- Andrews, P.J.D.; Avenell, A.; Noble, D.W.; Campbell, M.K.; Croal, B.L.; Simpson, W.G.; Vale, L.D.; Battison, C.G.; Jenkinson, D.J.; Cook, J.A.; et al. Randomised Trial of Glutamine, Selenium, or Both, to Supplement Parenteral Nutrition for Critically Ill Patients. BMJ 2011, 342, d1542. [Google Scholar] [CrossRef]
- Wernerman, J.; Kirketeig, T.; Andersson, B.; Berthelson, H.; Ersson, A.; Friberg, H.; Guttormsen, A.B.; Hendrikx, S.; Pettilä, V.; Rossi, P.; et al. Scandinavian Glutamine Trial: A Pragmatic Multi-Centre Randomised Clinical Trial of Intensive Care Unit Patients. Acta Anaesthesiol. Scand. 2011, 55, 812–818. [Google Scholar] [CrossRef]
- Vardavas, C.I.; Mathioudakis, A.G.; Nikitara, K.; Stamatelopoulos, K.; Georgiopoulos, G.; Phalkey, R.; Leonardi-Bee, J.; Fernandez, E.; Carnicer-Pont, D.; Vestbo, J.; et al. Prognostic Factors for Mortality, Intensive Care Unit and Hospital Admission Due to SARS-CoV-2: A Systematic Review and Meta-Analysis of Cohort Studies in Europe. Eur. Respir. Rev. 2022, 31, 220098. [Google Scholar] [CrossRef]
- Reyna-Villasmil, E.; Caponcello, M.G.; Maldonado, N.; Olivares, P.; Caroccia, N.; Bonazzetti, C.; Tazza, B.; Carrara, E.; Giannella, M.; Tacconelli, E.; et al. Association of Patients’ Epidemiological Characteristics and Comorbidities with Severity and Related Mortality Risk of SARS-CoV-2 Infection: Results of an Umbrella Systematic Review and Meta-Analysis. Biomedicines 2022, 10, 2437. [Google Scholar] [CrossRef]
- Soares, M.N.; Eggelbusch, M.; Naddaf, E.; Gerrits, K.H.L.; van der Schaaf, M.; van den Borst, B.; Wiersinga, W.J.; van Vugt, M.; Weijs, P.J.M.; Murray, A.J.; et al. Skeletal Muscle Alterations in Patients with Acute Covid-19 and Post-Acute Sequelae of Covid-19. J. Cachexia Sarcopenia Muscle 2022, 13, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Grund, S.; Bauer, J.M. Malnutrition and Sarcopenia in COVID-19 Survivors. Clin. Geriatr. Med. 2022, 38, 559–564. [Google Scholar] [CrossRef] [PubMed]
- King, C.S.; Sahjwani, D.; Brown, A.W.; Feroz, S.; Cameron, P.; Osborn, E.; Desai, M.; Djurkovic, S.; Kasarabada, A.; Hinerman, R.; et al. Outcomes of Mechanically Ventilated Patients with COVID-19 Associated Respiratory Failure. PLoS ONE 2020, 15, e0242651. [Google Scholar] [CrossRef] [PubMed]
- Nolley, E.P.; Sahetya, S.K.; Hochberg, C.H.; Hossen, S.; Hager, D.N.; Brower, R.G.; Stuart, E.A.; Checkley, W. Outcomes Among Mechanically Ventilated Patients With Severe Pneumonia and Acute Hypoxemic Respiratory Failure From SARS-CoV-2 and Other Etiologies. JAMA Netw. Open 2023, 6, e2250401. [Google Scholar] [CrossRef] [PubMed]
- Ojo, O.; Ojo, O.O.; Feng, Q.; Boateng, J.; Wang, X.; Brooke, J.; Adegboye, A.R.A. The Effects of Enteral Nutrition in Critically Ill Patients with COVID-19: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 1120. [Google Scholar] [CrossRef] [PubMed]
- Aguila, E.J.T.; Cua, I.H.Y.; Fontanilla, J.A.C.; Yabut, V.L.M.; Causing, M.F.P. Gastrointestinal Manifestations of COVID-19: Impact on Nutrition Practices. Nutr. Clin. Pr. 2020, 35, 800–805. [Google Scholar] [CrossRef]
- Bodolea, C.; Nemes, A.; Avram, L.; Craciun, R.; Coman, M.; Ene-Cocis, M.; Ciobanu, C.; Crisan, D. Nutritional Risk Assessment Scores Effectively Predict Mortality in Critically Ill Patients with Severe COVID-19. Nutrients 2022, 14, 2105. [Google Scholar] [CrossRef]
- Thibault, R.; Seguin, P.; Tamion, F.; Pichard, C.; Singer, P. Nutrition of the COVID-19 Patient in the Intensive Care Unit (ICU): A Practical Guidance. Crit. Care 2020, 24, 447. [Google Scholar] [CrossRef]
- Otten, J.J.; Averill, M.M.; Spiker, M.L. Food Security and Food Access during the COVID-19 Pandemic: Impacts, Adaptations, and Looking Ahead. JPEN J. Parenter. Enter. Nutr. 2022. [Google Scholar] [CrossRef]
- Sbaih, N.; Hawthorne, K.; Lutes, J.; Cavallazzi, R. Nutrition Therapy in Non-Intubated Patients with Acute Respiratory Failure. Curr. Nutr. Rep. 2021, 10, 307–316. [Google Scholar] [CrossRef]
- Formenti, P.; Bichi, F.; Castagna, V.; Pozzi, T.; Chiumello, D. Nutrition Support in Patients With Acute Respiratory Distress Syndrome COVID-19. Nutr. Clin. Pr. 2021, 36, 500–501. [Google Scholar] [CrossRef] [PubMed]
- Jin, S.; Lu, X.; Xu, C. COVID-19 Induces Gastrointestinal Symptoms and Affects Patients’ Prognosis. J. Int. Med. Res. 2022, 50, 3000605221129543. [Google Scholar] [CrossRef] [PubMed]
- Osuna-Padilla, I.; Rodríguez-Moguel, N.C.; Aguilar-Vargas, A.; Rodríguez-Llamazares, S. Safety and Tolerance of Enteral Nutrition in COVID-19 Critically Ill Patients, a Retrospective Study. Clin. Nutr. ESPEN 2021, 43, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Saseedharan, S.; Chada, R.R.; Kadam, V.; Chiluka, A.; Nagalla, B. Energy Expenditure in COVID-19 Mechanically Ventilated Patients: A Comparison of Three Methods of Energy Estimation. JPEN J. Parenter. Enter. Nutr. 2022, 46, 1875–1882. [Google Scholar] [CrossRef]
- Burslem, R.; Gottesman, K.; Newkirk, M.; Ziegler, J. Energy Requirements for Critically Ill Patients with COVID-19. Nutr. Clin. Pr. 2022, 37, 594–604. [Google Scholar] [CrossRef]
- Grecco, B.H.; Araújo-Rossi, P.A.O.; Nicoletti, C.F. Nutritional Therapy for Hospitalized Patients with COVID-19: A Narrative and Integrative Review. J. Intensive Med. 2022, 2, 249–256. [Google Scholar] [CrossRef]
- Brahmi, F.; Vejux, A.; Ghzaiel, I.; Ksila, M.; Zarrouk, A.; Ghrairi, T.; Essadek, S.; Mandard, S.; Leoni, V.; Poli, G.; et al. Role of Diet and Nutrients in SARS-CoV-2 Infection: Incidence on Oxidative Stress, Inflammatory Status and Viral Production. Nutrients 2022, 14, 2194. [Google Scholar] [CrossRef]
- Feiner Solís, Á.; Avedillo Salas, A.; Luesma Bartolomé, M.J.; Santander Ballestín, S. The Effects of Vitamin D Supplementation in COVID-19 Patients: A Systematic Review. Int. J. Mol. Sci. 2022, 23, 12424. [Google Scholar] [CrossRef]
- Alves de Paula, J.; Rabito, E.I.; Justino, S.R.; Leite, L.S.; Dantas, D.; Makiyama da Silva, J.S.; Maffini, L.F.; Júnior, O.R. Administration of Enteral Nutrition and Gastrointestinal Complications in Covid-19 Critical Patients in Prone Position. Clin. Nutr. Open. Sci. 2022, 45, 80–90. [Google Scholar] [CrossRef]
- López-Gómez, J.J.; Lastra-González, P.; Gómez-Hoyos, E.; Ortolá-Buigues, A.; Jiménez-Sahagún, R.; Cuadrado-Clemente, L.; Benito-Sendín-Plaar, K.; Cuenca-Becerril, S.; Portugal-Rodríguez, E.; De Luis Román, D.A. Evolution of Nutrition Support in Patients with COVID-19 Disease Admitted in the Intensive Care Unit. Endocrinol. Diabetes Nutr. (Engl. Ed.) 2022, S2530-0180(22)00216-5. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Substrate | O2 Consumed (L) | CO2 Produced (L) | RQ | Energy Yield (kcal) | ATP Yield (mol) |
|---|---|---|---|---|---|
| Glucose | 134 | 134 | 1 | 670 | 36 |
| Palmitate | 515 | 358 | 0.7 | 2400 | 132 |
| Amino acids | 114 | 92 | 0.8 | 479 | 23 |
| Study | Study Design | Comparator | Main Finding |
|---|---|---|---|
| Alberda 1999 [34] | Observational cohort study; 2772 mechanically ventilated patients | Calories prescribed | Provision of higher calories was associated with reduced 60-day mortality (OR 0.76 for every 1000 kcal/day provided) Sub-analysis for BMI classes suggested significant effects for patients with a BMI <25 or ≥35 kg/m2 |
| Villet 2005 [31] | Prospective observational study; 48 patients | Energy balance | The cumulative negative energy balance was significantly correlated with the length of ICU stay and the number of infectious complications |
| Dvir 2006 [35] | Prospective observational study; 50 patients | Energy balance | The cumulative negative energy balance during ICU stays was significantly correlated with a higher rate of occurrence of ARDS, renal failure requiring surgery, and the total complication rate |
| Heyland 2011 [36] | Prospective, multi-institutional audit; 7872 mechanically ventilated patients | Calories prescribed | Patients who received >2/3 of their caloric prescription had lower mortality than those receiving <1/3 of their prescription (OR 0.67) |
| Weijs 2012 [37] | Prospective observational cohort study; 886 patients | Provision of both the protein and energy target | Provision of a protein target (defined as 1.2 g/kg) was associated with a reduced 28-day mortality (The hazard ratios for the energy target and protein + energy target were 0.83 (0.67–1.01) and 0.47 (0.31–0.73)) |
| Allingstrup 2012 [38] | Prospective observational cohort study; 113 patients | Proteins prescribed | A significantly decreased hazard ratio of ICU mortality was associated with increased protein provision (HR 0.98 for every g/day of protein prescribed) |
| Wei 2015 [29] | Retrospective analysis of prospectively collected data from a multicenter RCT; 475 patients | Proportion of received/prescribed calories during the first 8 days | Greater amounts of nutritional intake were associated with longer survival times and faster physical recovery to 3 months |
| Zusman 2016 [39] | Retrospective; 1171 patients | Outcome vs. the percentage of administered calories | The % AdCal/REE had a significant non-linear association with mortality after adjusting for other variables. Increasing the percentage from 0 to 70% resulted in a hazard ratio of 0.98, pointing to reduced mortality, while increases above 70% suggested an increase in mortality |
| Compher 2017 [40] | Prospective; 202 patients | Nutritional risk and nutritional intake | In high-risk but not low-risk patients, mortality was lower with greater protein and energy intake |
| Koekkoek 2019 [41] | Retrospective; 455 patients | Low vs. high protein intake | Time-dependent association of protein intake and mortality; low protein intake (<0.8 g/kg/day) before day 3 and high protein intake (>0.8 g/kg/day) after day 3 were associated with lower 6-month mortality compared to patients with overall high protein intake |
| Hartl 2022 [42] | Retrospective; 16,489 patients | Protein intake | In comparison with an exclusively low-protein diet, a late standard protein diet was associated with a lower hazard of in-hospital death: minimum 0.75 (95% CI 0.64, 0.87), and a higher hazard of live hospital discharge: maximum HR 1.98 (95% CI 1.72, 2.28) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Umbrello, M.; Marini, J.J.; Formenti, P. Metabolic Support in Acute Respiratory Distress Syndrome: A Narrative Review. J. Clin. Med. 2023, 12, 3216. https://doi.org/10.3390/jcm12093216
Umbrello M, Marini JJ, Formenti P. Metabolic Support in Acute Respiratory Distress Syndrome: A Narrative Review. Journal of Clinical Medicine. 2023; 12(9):3216. https://doi.org/10.3390/jcm12093216
Chicago/Turabian StyleUmbrello, Michele, John J. Marini, and Paolo Formenti. 2023. "Metabolic Support in Acute Respiratory Distress Syndrome: A Narrative Review" Journal of Clinical Medicine 12, no. 9: 3216. https://doi.org/10.3390/jcm12093216