
The Association between Autoimmune Thyroid Disease and Ocular Surface Damage: A Retrospective Population-Based Cohort Study
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Data Source
2.2. Study Population and Definition
2.3. Ocular Surface Disease
2.4. Covariates for Adjustment
2.5. Statistical Analysis
3. Results
3.1. Baseline Patient Characteristics
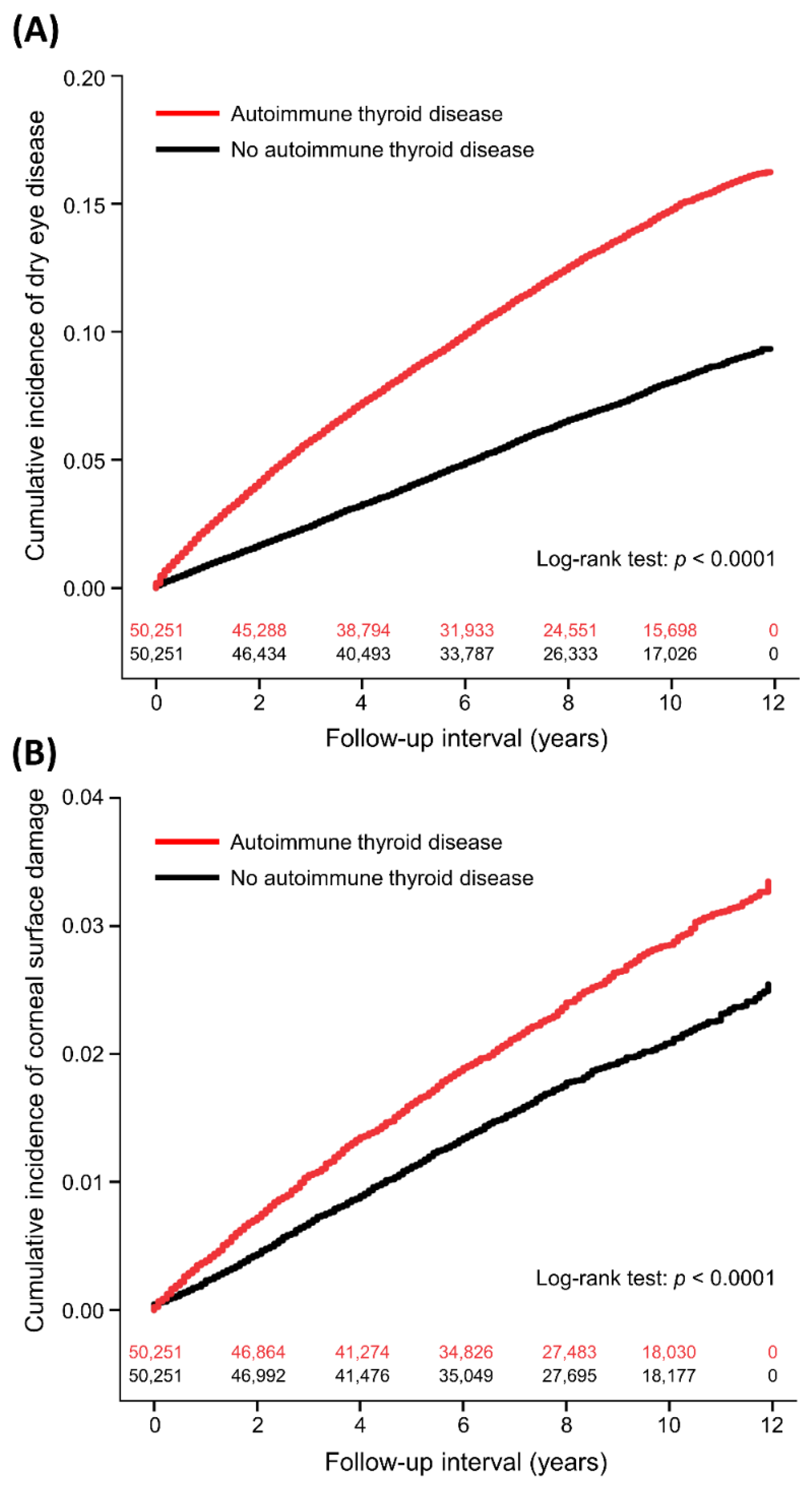
3.2. Dry Eye Disease
3.3. Corneal Surface Damage
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pflugfelder, S.C.; de Paiva, C.S. The Pathophysiology of Dry Eye Disease: What We Know and Future Directions for Research. Ophthalmology 2017, 124, S4–S13. [Google Scholar] [CrossRef]
- McCann, P.; Abraham, A.G.; Mukhopadhyay, A.; Panagiotopoulou, K.; Chen, H.; Rittiphairoj, T.; Gregory, D.G.; Hauswirth, S.G.; Ifantides, C.; Qureshi, R.; et al. Prevalence and Incidence of Dry Eye and Meibomian Gland Dysfunction in the United States: A Systematic Review and Meta-analysis. JAMA Ophthalmol. 2022, 140, 1181–1192. [Google Scholar] [CrossRef] [PubMed]
- Qian, L.; Wei, W. Identified risk factors for dry eye syndrome: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0271267. [Google Scholar] [CrossRef] [PubMed]
- Baranwal, V.K.; Satyabala, K.; Mishra, A.; Dutta, A.K. Sterile corneal perforations in a case of severe dry eyes. Med. J. Armed Forces India 2015, 71, 290–292. [Google Scholar] [CrossRef]
- Deswal, J.; Arya, S.K.; Raj, A.; Bhatti, A. A Case of Bilateral Corneal Perforation in a Patient with Severe Dry Eye. J. Clin. Diagn. Res. 2017, 11, ND01–ND02. [Google Scholar] [CrossRef]
- Hung, N.; Kang, E.Y.; Lee, T.W.; Chen, T.H.; Shyu, Y.C.; Sun, C.C. The Risks of Corneal Surface Damage in Aqueous-Deficient Dry Eye Disease: A 17-Year Population-Based Study in Taiwan. Am. J. Ophthalmol. 2021, 227, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Glover, K.; Mishra, D.; Singh, T.R.R. Epidemiology of Ocular Manifestations in Autoimmune Disease. Front. Immunol. 2021, 12, 744396. [Google Scholar] [CrossRef] [PubMed]
- Ragusa, F.; Fallahi, P.; Elia, G.; Gonnella, D.; Paparo, S.R.; Giusti, C.; Churilov, L.P.; Ferrari, S.M.; Antonelli, A. Hashimotos’ thyroiditis: Epidemiology, pathogenesis, clinic and therapy. Best Pract. Res. Clin. Endocrinol. Metab. 2019, 33, 101367. [Google Scholar] [CrossRef]
- Antonelli, A.; Ferrari, S.M.; Ragusa, F.; Elia, G.; Paparo, S.R.; Ruffilli, I.; Patrizio, A.; Giusti, C.; Gonnella, D.; Cristaudo, A.; et al. Graves’ disease: Epidemiology, genetic and environmental risk factors and viruses. Best Pract. Res. Clin. Endocrinol. Metab. 2020, 34, 101387. [Google Scholar] [CrossRef] [PubMed]
- Ajjan, R.A.; Weetman, A.P. The Pathogenesis of Hashimoto’s Thyroiditis: Further Developments in our Understanding. Horm. Metab. Res. 2015, 47, 702–710. [Google Scholar] [CrossRef]
- Caturegli, P.; De Remigis, A.; Rose, N.R. Hashimoto thyroiditis: Clinical and diagnostic criteria. Autoimmun. Rev. 2014, 13, 391–397. [Google Scholar] [CrossRef]
- Gupta, A.; Sadeghi, P.B.; Akpek, E.K. Occult thyroid eye disease in patients presenting with dry eye symptoms. Am. J. Ophthalmol. 2009, 147, 919–923. [Google Scholar] [CrossRef]
- Kan, E.; Kılıçkan, E.; Ecemiş, G.; Beyazyildiz, E.; Çolak, R. Presence of Dry Eye in Patients with Hashimoto’s Thyroiditis. J. Ophthalmol. 2014, 2014, 754923. [Google Scholar] [CrossRef]
- Abusharaha, A.; Alturki, A.A.; Alanazi, S.A.; Fagehi, R.; Al-Johani, N.; El-Hiti, G.A.; Masmali, A.M. Assessment of tear-evaporation rate in thyroid-gland patients. Clin. Ophthalmol. 2019, 13, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Alanazi, S.A.; Alomran, A.A.; Abusharha, A.; Fagehi, R.; Al-Johani, N.J.; El-Hiti, G.A.; Masmali, A.M. An assessment of the ocular tear film in patients with thyroid disorders. Clin. Ophthalmol. 2019, 13, 1019–1026. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Baek, S. Dry eye syndrome in thyroid eye disease patients: The role of increased incomplete blinking and Meibomian gland loss. Acta Ophthalmol. 2019, 97, e800–e806. [Google Scholar] [CrossRef]
- Altin Ekin, M.; Karadeniz Ugurlu, S.; Egrilmez, E.D.; Oruk, G.G. Ocular Surface Changes in Hashimoto’s Thyroiditis Without Thyroid Ophthalmopathy. Eye Contact Lens 2021, 47, 32–37. [Google Scholar] [CrossRef]
- Allam, I.Y.; Lazreg, S.; Shafik Shaheen, M.; Doheim, M.F.; Mohammed, M.A. Ocular Surface Changes in Patients with Thyroid Eye Disease: An Observational Clinical Study. Clin. Ophthalmol. 2021, 15, 2481–2488. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Chang, Q.; Li, Y.; Zhang, H.; Hou, Z.; Zhang, Z.; Li, Z.; Li, D. Correlation between extent of lacrimal gland prolapse and clinical features of thyroid-associated ophthalmopathy: A retrospective observational study. BMC Ophthalmol. 2022, 22, 66. [Google Scholar] [CrossRef] [PubMed]
- Rana, H.S.; Akella, S.S.; Clabeaux, C.E.; Skurski, Z.P.; Aakalu, V.K. Ocular surface disease in thyroid eye disease: A narrative review. Ocul. Surf. 2022, 24, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Levine, H.; Hwang, J.; Dermer, H.; Mehra, D.; Feuer, W.; Galor, A. Relationships between activated dendritic cells and dry eye symptoms and signs. Ocul. Surf. 2021, 21, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Kohriyama, K.; Katayama, Y.; Tsurusako, Y. Relationship between primary Sjögren’s syndrome and autoimmune thyroid disease. Nihon Rinsho 1999, 57, 1878–1881. [Google Scholar] [PubMed]
- Coll, J.; Anglada, J.; Tomas, S.; Reth, P.; Goday, A.; Millan, M.; Pujol-Borrell, R.; Corominas, J. High prevalence of subclinical Sjögren’s syndrome features in patients with autoimmune thyroid disease. J. Rheumatol. 1997, 24, 1719–1724. [Google Scholar]
- Pérez, B.; Kraus, A.; López, G.; Cifuentes, M.; Alarcón-Segovia, D. Autoimmune thyroid disease in primary Sjögren’s syndrome. Am. J. Med. 1995, 99, 480–484. [Google Scholar] [CrossRef] [PubMed]
- D’Arbonneau, F.; Ansart, S.; Le Berre, R.; Dueymes, M.; Youinou, P.; Pennec, Y.L. Thyroid dysfunction in primary Sjögren’s syndrome: A long-term followup study. Arthritis Rheum. 2003, 49, 804–809. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef] [PubMed]
- Ting, H.C.; Ma, S.H.; Tai, Y.H.; Dai, Y.X.; Chang, Y.T.; Chen, T.J.; Chen, M.H. Association between alopecia areata and retinal diseases: A nationwide population-based cohort study. J. Am. Acad. Dermatol. 2022, 87, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Tai, C.Y.; Liu, H.Y.; Cata, J.P.; Dai, Y.X.; Chen, M.H.; Chen, J.T.; Chen, T.J.; Wu, H.L.; Cherng, Y.G.; Li, C.C.; et al. The association between general anesthesia and new postoperative uses of sedative-hypnotics: A nationwide matched cohort study. J. Clin. Med. 2022, 11, 3360. [Google Scholar] [CrossRef]
- Lai, S.C.; Wang, C.W.; Wu, Y.M.; Dai, Y.X.; Chen, T.J.; Wu, H.L.; Cherng, Y.G.; Tai, Y.H. Rheumatoid arthritis associated with dry eye disease and corneal surface damage: A nationwide matched cohort study. Int. J. Environ. Res. Public. Health 2023, 20, 1584. [Google Scholar] [CrossRef]
- National Health Insurance Research Database. Data Subsets. Available online: https://nhird.nhri.org.tw/en/Data_Subsets.html (accessed on 7 February 2023).
- Shanti, Y.; Shehada, R.; Bakkar, M.M.; Qaddumi, J. Prevalence and associated risk factors of dry eye disease in 16 northern West bank towns in Palestine: A cross-sectional study. BMC Ophthalmol. 2020, 20, 26. [Google Scholar] [CrossRef]
- Li, B.; Evans, D.; Faris, P.; Dean, S.; Quan, H. Risk adjustment performance of Charlson and Elixhauser comorbidities in ICD-9 and ICD-10 administrative databases. BMC Health Serv. Res. 2008, 8, 12. [Google Scholar] [CrossRef]
- Austin, P.C. A comparison of 12 algorithms for matching on the propensity score. Stat. Med. 2014, 33, 1057–1069. [Google Scholar] [CrossRef]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef]
- Vehof, J.; Snieder, H.; Jansonius, N.; Hammond, C.J. Prevalence and risk factors of dry eye in 79,866 participants of the population-based Lifelines cohort study in the Netherlands. Ocul. Surf. 2021, 19, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Queiruga, J.; Pena-Verdeal, H.; Sabucedo-Villamarin, B.; Giraldez, M.J.; Garcia-Resua, C.; Yebra-Pimentel, E. A cross-sectional study of non-modifiable and modifiable risk factors of dry eye disease states. Cont. Lens Anterior Eye 2022, in press. [Google Scholar] [CrossRef] [PubMed]
- Yu, K.; Bunya, V.; Maguire, M.; Asbell, P.; Ying, G.S.; Dry Eye Assessment and Management Study Research Group. Systemic Conditions Associated with Severity of Dry Eye Signs and Symptoms in the Dry Eye Assessment and Management Study. Ophthalmology 2021, 128, 1384–1392. [Google Scholar] [CrossRef] [PubMed]
- Hasan, Z.A.I.Y. Dry eye syndrome risk factors: A systemic review. Saudi J. Ophthalmol. 2022, 35, 131–139. [Google Scholar] [CrossRef]
- Lo, C.; Yang, M.; Rootman, D. Natural history of inflammatory and non-inflammatory dry eye in thyroid eye disease. Orbit 2021, 40, 389–393. [Google Scholar] [CrossRef]
- Hsu, S.L.; Lee, P.Y.; Chang, C.H.; Chen, C.H. Immunological impression cytology of the conjunctival epithelium in patients with thyroid orbitopathy-related dry eye. Genet. Mol. Res. 2016, 15, gmr.15039011. [Google Scholar] [CrossRef]
- Park, J.; Kim, J.; Lee, H.; Park, M.; Baek, S. Functional and structural evaluation of the meibomian gland using a LipiView interferometer in thyroid eye disease. Can. J. Ophthalmol. 2018, 53, 373–379. [Google Scholar] [CrossRef]
- Wang, C.Y.; Ho, R.W.; Fang, P.C.; Yu, H.J.; Chien, C.C.; Hsiao, C.C.; Kuo, M.T. The function and morphology of Meibomian glands in patients with thyroid eye disease: A preliminary study. BMC Ophthalmol. 2018, 18, 90. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| ATD n = 50,251 | Non-ATD n = 50,251 | ASMD | |||
|---|---|---|---|---|---|
| Age (years), mean (SD) | 39.8 | 15.0 | 39.8 | 15.0 | <0.0001 |
| Sex, male, n (%) | 11,065 | 22.0 | 11,065 | 22.0 | <0.0001 |
| Insurance premium (USD/month), n (%) | <0.0001 | ||||
| 0–500 | 17,022 | 33.9 | 17,022 | 33.9 | |
| 501–800 | 16,212 | 32.3 | 16,212 | 32.3 | |
| ≥801 | 17,017 | 33.9 | 17,017 | 33.9 | |
| Coexisting diseases, n (%) | |||||
| Hypertension | 6661 | 13.3 | 4314 | 8.6 | 0.2684 |
| Diabetes mellitus | 3500 | 7.0 | 2034 | 4.1 | 0.3163 |
| Coronary artery disease | 3046 | 6.1 | 1387 | 2.8 | 0.4528 |
| Chronic obstructive pulmonary disease | 2268 | 4.5 | 1259 | 2.5 | 0.3360 |
| Chronic liver disease | 4577 | 9.1 | 2415 | 4.8 | 0.3780 |
| Chronic kidney disease | 327 | 0.7 | 177 | 0.4 | 0.3401 |
| Cerebrovascular disease | 1248 | 2.5 | 731 | 1.5 | 0.3007 |
| Major depressive disorder | 704 | 1.4 | 304 | 0.6 | 0.4674 |
| Anxiety disorder | 7681 | 15.3 | 2992 | 6.0 | 0.5774 |
| Sleeping disorder | 6231 | 12.4 | 3227 | 6.4 | 0.3992 |
| Cancer | 1314 | 2.6 | 819 | 1.6 | 0.2662 |
| Charlson Comorbidity Index | 0.0642 | ||||
| 0 | 45,572 | 90.7 | 46,587 | 92.7 | |
| 1 | 3300 | 6.6 | 2594 | 5.2 | |
| 2 | 1179 | 2.4 | 854 | 1.7 | |
| ≥3 | 200 | 0.4 | 216 | 0.4 | |
| Use of systemic corticosteroids, n (%) | 8935 | 17.8 | 6222 | 12.4 | 0.2346 |
| Number of hospitalizations, n (%) | 0.1023 | ||||
| 0 | 44,033 | 87.6 | 45,770 | 91.1 | |
| 1 | 4726 | 9.4 | 3443 | 6.9 | |
| 2 | 997 | 2.0 | 677 | 1.4 | |
| ≥3 | 495 | 1.0 | 361 | 0.7 | |
| Number of emergency room visits, n (%) | 0.2209 | ||||
| 0 | 37,162 | 74.0 | 41,577 | 82.7 | |
| 1 | 8251 | 16.4 | 6066 | 12.1 | |
| 2 | 2684 | 5.3 | 1564 | 3.1 | |
| ≥3 | 2154 | 4.3 | 1044 | 2.1 | |
| ATD n = 50,251 | Non-ATD n = 50,251 | Outcome Risk | |||||
|---|---|---|---|---|---|---|---|
| Study Outcome | Incident Case | Incidence per 1000 Person-Years | Incident Case | Incidence per 1000 Person-Years | IRR | aHR (95% CI) † | p |
| Dry eye disease | 5996 | 16.37 | 3198 | 8.36 | 1.96 | 1.81 (1.73–1.89) | <0.0001 |
| Sjögren’s syndrome-associated | 1292 | 3.30 | 519 | 1.31 | 2.52 | 2.24 (2.01–2.50) | <0.0001 |
| Non-Sjögren’s syndrome-associated | 4704 | 12.84 | 2679 | 7.00 | 1.83 | 1.72 (1.63–1.80) | <0.0001 |
| Sjögren’s syndrome | 1292 | 3.30 | 519 | 1.31 | 2.52 | 2.24 (2.01–2.50) | <0.0001 |
| Corneal surface damage | 1168 | 2.98 | 854 | 2.17 | 1.37 | 1.31 (1.19–1.44) | <0.0001 |
| Corneal ulcer | 611 | 1.56 | 520 | 1.32 | 1.18 | 1.10 (0.97–1.24) | 0.1565 |
| Recurrent corneal erosion | 377 | 0.96 | 183 | 0.46 | 2.09 | 2.00 (1.66–2.41) | <0.0001 |
| Corneal scar | 186 | 0.47 | 154 | 0.39 | 1.21 | 1.26 (1.01–1.59) | 0.0432 |
| Univariate | Multivariable | |||||
|---|---|---|---|---|---|---|
| cHR | 95% CI | p | aHR | 95% CI | p | |
| Autoimmune thyroid disease | 1.95 | 1.87–2.04 | <0.0001 | 1.81 | 1.73–1.89 | <0.0001 |
| Age (years) | 1.03 | 1.03–1.03 | <0.0001 | 1.03 | 1.03–1.03 | <0.0001 |
| Sex, male vs. female | 0.56 | 0.53–0.60 | <0.0001 | 0.52 | 0.49–0.56 | |
| Insurance premium (USD/month) | <0.0001 | <0.0001 | ||||
| 501–800 vs. 0–500 | 0.71 | 0.67–0.74 | <0.0001 | 0.86 | 0.82–0.91 | <0.0001 |
| ≥801 vs. 0–500 | 0.78 | 0.75–0.82 | <0.0001 | 1.16 | 1.10–1.22 | <0.0001 |
| Coexisting diseases | ||||||
| Hypertension | 1.85 | 1.75–1.96 | <0.0001 | 0.93 | 0.87–1.00 | 0.0388 |
| Diabetes mellitus | 1.79 | 1.67–1.93 | <0.0001 | 1.08 | 0.99–1.17 | 0.0801 |
| Coronary artery disease | 2.17 | 2.01–2.33 | <0.0001 | 1.12 | 1.03–1.21 | 0.0106 |
| COPD | 1.77 | 1.62–1.94 | <0.0001 | 1.09 | 1.00–1.20 | 0.0599 |
| Chronic liver disease | 1.69 | 1.58–1.81 | <0.0001 | 1.23 | 1.15–1.32 | <0.0001 |
| Chronic kidney disease | 1.67 | 1.30–2.15 | <0.0001 | 0.98 | 0.76–1.26 | 0.8470 |
| Cerebrovascular disease | 1.84 | 1.63–2.07 | <0.0001 | 0.93 | 0.82–1.06 | 0.2626 |
| Major depressive disorder | 1.95 | 1.66–2.28 | <0.0001 | 1.26 | 1.07–1.48 | 0.0056 |
| Anxiety disorder | 2.10 | 1.99–2.21 | <0.0001 | 1.38 | 1.30–1.47 | <0.0001 |
| Sleeping disorder | 1.91 | 1.80–2.03 | <0.0001 | 1.19 | 1.12–1.27 | <0.0001 |
| Cancer | 1.68 | 1.49–1.89 | <0.0001 | 1.09 | 0.96–1.23 | 0.1923 |
| Charlson Comorbidity Index | <0.0001 | 0.5526 | ||||
| 1 vs. 0 | 1.50 | 1.39–1.61 | <0.0001 | 0.95 | 0.88–1.03 | 0.1957 |
| 2 vs. 0 | 1.45 | 1.29–1.64 | <0.0001 | 1.00 | 0.88–1.13 | 0.9583 |
| ≥3 vs. 0 | 1.24 | 0.93–1.64 | 0.1405 | 0.90 | 0.68–1.20 | 0.4874 |
| Use of systemic corticosteroids | 1.47 | 1.40–1.55 | <0.0001 | 1.32 | 1.25–1.39 | <0.0001 |
| Number of hospitalizations | 0.0003 | 0.0014 | ||||
| 1 vs. 0 | 1.06 | 0.98–1.15 | 0.1305 | 0.90 | 0.83–0.97 | 0.0068 |
| 2 vs. 0 | 1.36 | 1.17–1.58 | <0.0001 | 0.97 | 0.83–1.13 | 0.7025 |
| ≥3 vs. 0 | 1.14 | 0.90–1.43 | 0.2780 | 0.68 | 0.53–0.87 | 0.0020 |
| Number of emergency room visits | <0.0001 | 0.4599 | ||||
| 1 vs. 0 | 1.09 | 1.02–1.15 | 0.0071 | 0.99 | 0.93–1.05 | 0.7328 |
| 2 vs. 0 | 1.20 | 1.08–1.32 | 0.0006 | 0.98 | 0.89–1.09 | 0.7527 |
| ≥3 vs. 0 | 1.20 | 1.06–1.35 | 0.0031 | 0.90 | 0.79–1.02 | 0.1094 |
| ATD n = 50,251 | Non-ATD n = 50,251 | Outcome Risk | |||||
|---|---|---|---|---|---|---|---|
| Subgroup | Incident Case | Incidence per 1000 Person-Years | Incident Case | Incidence per 1000 Person-Years | IRR | aHR (95% CI) † | p |
| All patients | 5996 | 16.37 | 3198 | 8.36 | 1.96 | 1.81 (1.73–1.89) | <0.0001 |
| Age ≥ 65 years | 631 | 28.99 | 400 | 17.28 | 1.68 | 1.56 (1.36–1.78) | <0.0001 |
| Age < 65 years | 5365 | 15.57 | 2798 | 7.78 | 2.00 | 1.84 (1.75–1.93) | <0.0001 |
| Male | 829 | 10.50 | 398 | 4.89 | 2.15 | 1.95 (1.71–2.21) | <0.0001 |
| Female | 5167 | 17.98 | 2800 | 9.30 | 1.93 | 1.78 (1.70–1.87) | <0.0001 |
| CCI score = 0 | 5242 | 15.86 | 2814 | 7.99 | 1.98 | 1.84 (1.75–1.93) | <0.0001 |
| CCI score = 1 | 550 | 21.75 | 268 | 12.51 | 1.74 | 1.66 (1.42–1.93) | <0.0001 |
| CCI score = 2 | 176 | 19.75 | 96 | 13.53 | 1.46 | 1.35 (1.03–1.75) | 0.0278 |
| CCI score ≥ 3 | 28 | 18.17 | 20 | 11.30 | 1.61 | 1.33 (0.69–2.56) | 0.3954 |
| Use of systemic corticosteroids | 1365 | 21.20 | 533 | 11.06 | 1.92 | 1.78 (1.60–1.98) | <0.0001 |
| No use of systemic corticosteroids | 4631 | 15.34 | 2665 | 7.97 | 1.92 | 1.81 (1.72–1.91) | <0.0001 |
| Univariate | Multivariable | |||||
|---|---|---|---|---|---|---|
| cHR | 95% CI | p | aHR | 95% CI | p | |
| Autoimmune thyroid disease | 1.37 | 1.26–1.50 | <0.0001 | 1.31 | 1.19–1.44 | <0.0001 |
| Age (years) | 0.998 | 0.995–1.001 | 0.2272 | 0.996 | 0.993–1.000 | 0.0354 |
| Sex, male vs. female | 0.88 | 0.79–0.98 | 0.0218 | 0.87 | 0.78–0.98 | 0.0180 |
| Insurance premium (USD/month) | 0.6098 | 0.7713 | ||||
| 501–800 vs. 0–500 | 1.05 | 0.94–1.17 | 0.3893 | 1.04 | 0.93–1.16 | 0.4958 |
| ≥801 vs. 0–500 | 1.00 | 0.90–1.11 | 1.0000 | 1.01 | 0.90–1.13 | 0.8773 |
| Coexisting diseases | ||||||
| Hypertension | 1.02 | 0.88–1.18 | 0.7675 | 0.92 | 0.77–1.09 | 0.3355 |
| Diabetes mellitus | 1.37 | 1.15–1.63 | 0.0005 | 1.31 | 1.08–1.59 | 0.0065 |
| Coronary artery disease | 1.12 | 0.91–1.38 | 0.2931 | 1.02 | 0.81–1.28 | 0.8762 |
| COPD | 1.16 | 0.93–1.46 | 0.1888 | 1.08 | 0.85–1.36 | 0.5323 |
| Chronic liver disease | 1.12 | 0.95–1.33 | 0.1836 | 1.02 | 0.86–1.21 | 0.8312 |
| Chronic kidney disease | 0.72 | 0.32–1.60 | 0.4152 | 0.63 | 0.28–1.42 | 0.2637 |
| Cerebrovascular disease | 1.11 | 0.81–1.53 | 0.5038 | 1.03 | 0.74–1.44 | 0.8606 |
| Major depressive disorder | 1.47 | 1.00–2.15 | 0.0478 | 1.25 | 0.85–1.84 | 0.2643 |
| Anxiety disorder | 1.21 | 1.06–1.39 | 0.0063 | 1.05 | 0.90–1.22 | 0.5258 |
| Sleeping disorder | 1.23 | 1.06–1.43 | 0.0063 | 1.12 | 0.95–1.32 | 0.1738 |
| Cancer | 0.99 | 0.72–1.37 | 0.9616 | 0.97 | 0.70–1.34 | 0.8321 |
| Charlson Comorbidity Index | 0.0022 | 0.0056 | ||||
| 1 vs. 0 | 1.28 | 1.09–1.51 | 0.0025 | 1.27 | 1.07–1.52 | 0.0065 |
| 2 vs. 0 | 1.13 | 0.85–1.50 | 0.4012 | 1.14 | 0.85–1.52 | 0.3750 |
| ≥3 vs. 0 | 0.11 | 0.02–0.79 | 0.0283 | 0.12 | 0.02–0.83 | 0.0318 |
| Use of systemic corticosteroids | 1.31 | 1.18–1.47 | <0.0001 | 1.26 | 1.13–1.41 | <0.0001 |
| Number of hospitalizations | 0.5917 | 0.1493 | ||||
| 1 vs. 0 | 0.91 | 0.76–1.08 | 0.2757 | 0.82 | 0.68–0.98 | 0.0313 |
| 2 vs. 0 | 0.97 | 0.67–1.41 | 0.8700 | 0.82 | 0.56–1.21 | 0.3169 |
| ≥3 vs. 0 | 1.22 | 0.76–1.96 | 0.4187 | 0.97 | 0.59–1.60 | 0.8974 |
| Number of emergency room visits | 0.0224 | 0.2657 | ||||
| 1 vs. 0 | 1.15 | 1.01–1.31 | 0.0301 | 1.11 | 0.98–1.27 | 0.1143 |
| 2 vs. 0 | 1.08 | 0.86–1.35 | 0.5367 | 1.01 | 0.80–1.28 | 0.9111 |
| ≥3 vs. 0 | 1.34 | 1.05–1.71 | 0.0186 | 1.21 | 0.93–1.57 | 0.1584 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, E.W.; Tai, Y.-H.; Wu, H.-L.; Dai, Y.-X.; Chen, T.-J.; Cherng, Y.-G.; Lai, S.-C. The Association between Autoimmune Thyroid Disease and Ocular Surface Damage: A Retrospective Population-Based Cohort Study. J. Clin. Med. 2023, 12, 3203. https://doi.org/10.3390/jcm12093203
Lai EW, Tai Y-H, Wu H-L, Dai Y-X, Chen T-J, Cherng Y-G, Lai S-C. The Association between Autoimmune Thyroid Disease and Ocular Surface Damage: A Retrospective Population-Based Cohort Study. Journal of Clinical Medicine. 2023; 12(9):3203. https://doi.org/10.3390/jcm12093203
Chicago/Turabian StyleLai, Eric W., Ying-Hsuan Tai, Hsiang-Ling Wu, Ying-Xiu Dai, Tzeng-Ji Chen, Yih-Giun Cherng, and Shih-Chung Lai. 2023. "The Association between Autoimmune Thyroid Disease and Ocular Surface Damage: A Retrospective Population-Based Cohort Study" Journal of Clinical Medicine 12, no. 9: 3203. https://doi.org/10.3390/jcm12093203