
Diagnosis and Treatment of Japanese Children with Neurogenic Bladder: Analysis of Data from a National Health Insurance Database


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
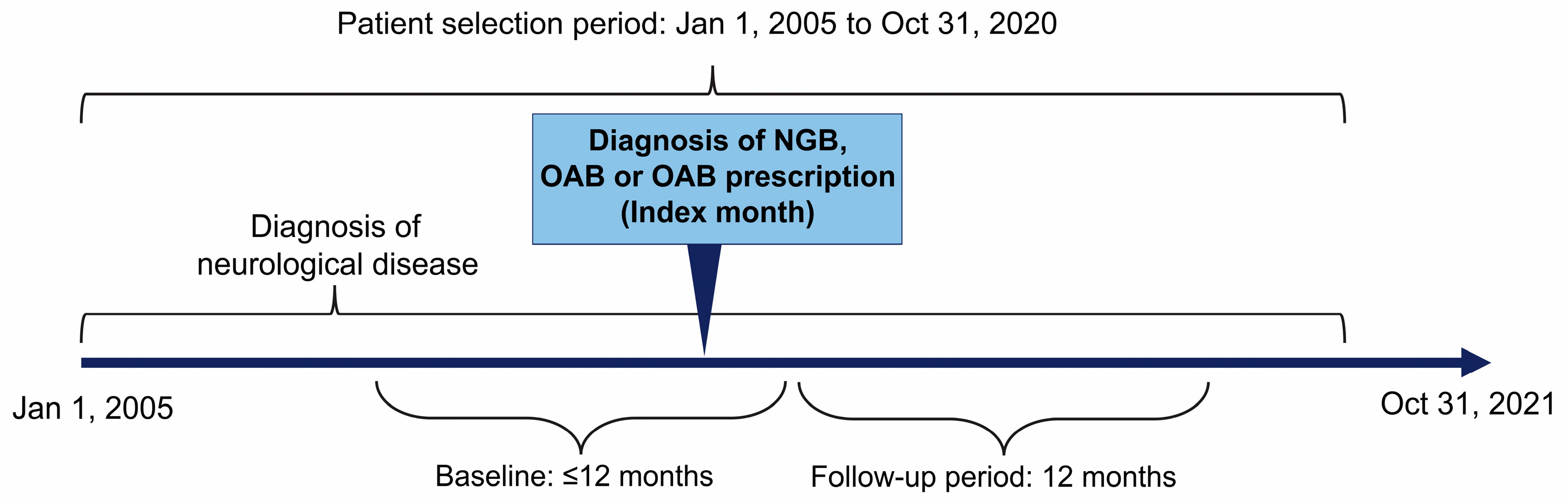
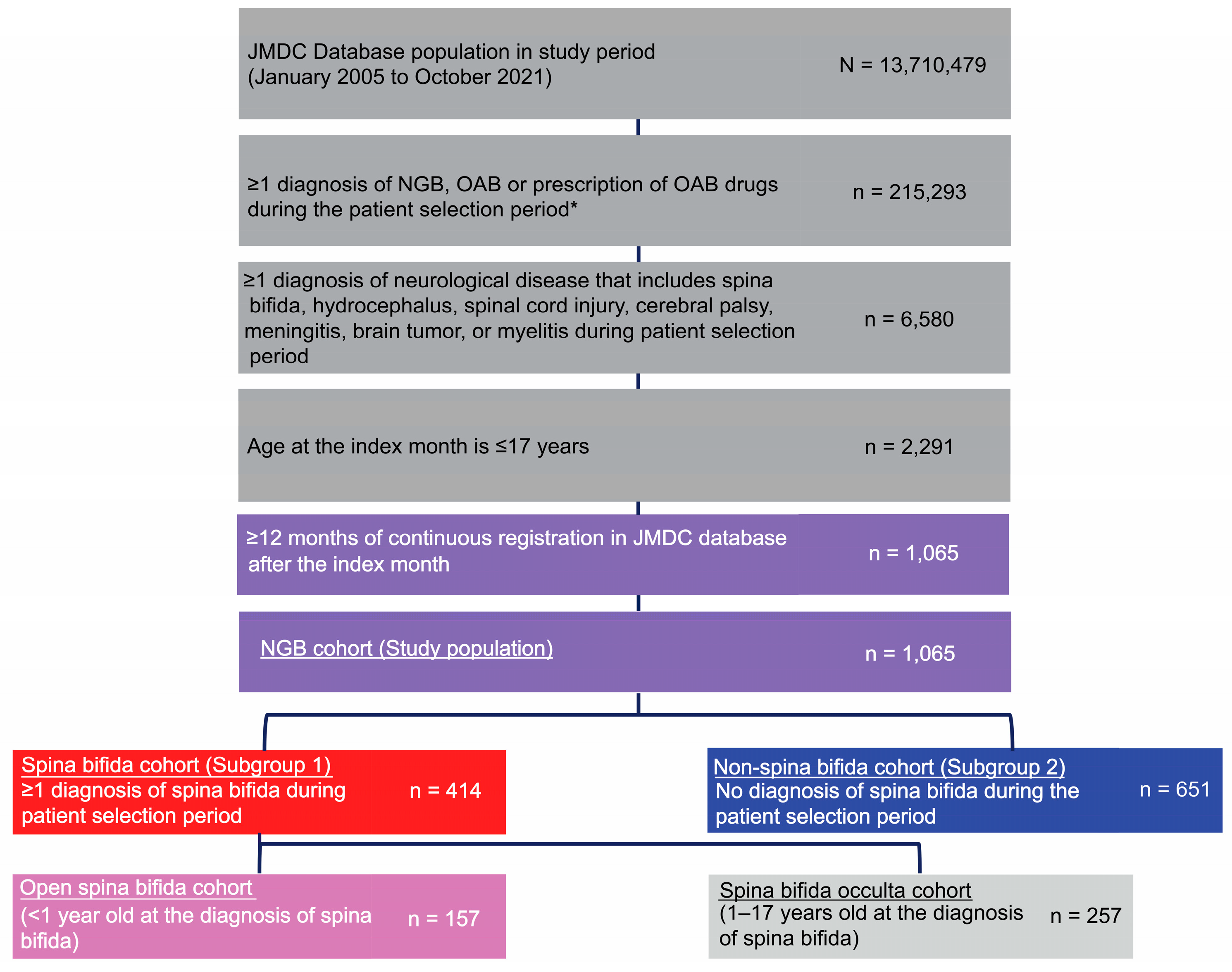
2.2. Study Design and Population
- One or more diagnosis of neurological disease (Table S3) that includes spina bifida, hydrocephalus, spinal cord injury, cerebral palsy, meningitis, brain tumor, or myelitis during the patient selection period (excluding suspected disease);
- Continuous registration in the JMDC database for ≥12 months before the index month including the index month for patients aged 1–17 years and from birth to the index month for patients aged <1 year; and
- Continuous registration in the JMDC database for ≥12 months after the index month.
2.3. Statistical Analysis
2.4. Ethical Considerations
3. Results
4. Discussion
4.1. Clinical Characteristics
4.2. Diagnosis
4.3. Treatment
4.4. Complications
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jaggi, A.; Nazir, J.; Fatoye, F.; Siddiqui, E.; Choudhury, N.; Argoubi, R.; Ali, M.; de Ridder, D.; Drake, M.J. Drug utilization patterns and healthcare resource use and costs in patients with neurogenic bladder in the United Kingdom: A retrospective primary care database study. Neurourol. Urodyn. 2019, 38, 1278–1289. [Google Scholar] [CrossRef] [PubMed]
- Guys, J.M.; Hery, G.; Haddad, M.; Borrionne, C. Neurogenic bladder in children: Basic principles, new therapeutic trends. Scand. J. Surg. 2011, 100, 256–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drake, M.; Apostolidis, A.; Emmanuel, A.; Gajewski, J.; Harrison, S.C.W.; Heesakkers, J.; Lemack, G.; Madersbacher, H.; Panicker, J.; Radziszewski, P.; et al. Neurologic urinary and fecal incontinence. In Incontinence, 5th ed.; Abrams, P., Cardozo, L., Khoury, S., Wein, A., Eds.; ICUD-EAU: Bristol, UK, 2013; pp. 827–1000. [Google Scholar]
- Kondo, A.; Matsuo, T.; Morota, N.; Kondo, A.S.; Okai, I.; Fukuda, H. Neural tube defects: Risk factors and preventive measures. Congenit. Anom 2017, 57, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Boussetta, A.; Jellouli, M.; Baati, R.; Gargah, T. Neurogenic non-neurogenic bladder in childhood: Complications and prognostic factors. Tunis Med. 2021, 99, 898–902. [Google Scholar] [PubMed]
- Bauer, S.B. Neuropathology of the lower urinary tract. In Clinical Pediatric Urology, 3rd ed.; Kelalis, P.P., King, L.R., Belman, A.B., Eds.; W. B. Saunders: Philadelphia, PA, USA, 1992; Volume 1, pp. 399–440. [Google Scholar]
- Sripathi, V.; Mitra, A. Management of neurogenic bladder. Indian J. Pediatr. 2017, 84, 545–554. [Google Scholar] [CrossRef] [PubMed]
- Stein, R.; Bogaert, G.; Dogan, H.S.; Hoen, L.; Kocvara, R.; Nijman, R.J.M.; Quadackers, J.S.L.T.; Rawashdeh, Y.F.; Silay, M.S.; Tekgul, S.; et al. EAU/ESPU guidelines on the management of neurogenic bladder in children and adolescent part I diagnostics and conservative treatment. Neurourol. Urodyn. 2020, 39, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Dorsher, P.T.; McIntosh, P.M. Neurogenic bladder. Adv. Urol. 2012, 2012, 816274. [Google Scholar] [CrossRef] [PubMed]
- Hobbs, K.T.; Krischak, M.; Tejwani, R.; Purves, J.T.; Wiener, J.S.; Routh, J.C. The importance of early diagnosis and management of pediatric neurogenic bladder dysfunction. Res. Rep. Urol. 2021, 13, 647–657. [Google Scholar] [CrossRef] [PubMed]
- The Japanese Continence Society. Clinical Guidelines for Lower Urinary Tract Dysfunction in Patients with Spina Bifida. Available online: https://www.urol.or.jp/lib/files/other/guideline/31_lower-urinary_dysfunction_2017.pdf (accessed on 13 September 2022).
- JMDC Claims Database. Available online: https://www.jmdc.co.jp/en/jmdc-claims-database/ (accessed on 8 September 2022).
- Statistics Bureau of Japan. Available online: https://www.stat.go.jp/english/info/news/20220228.html (accessed on 8 September 2022).
- Ministry of Health, Labour and Welfare. Ethical Guidelines for Medical and Health Research Involving Human Subjects (English Translation, March 2015). Available online: https://www.mhlw.go.jp/file/06-Seisakujouhou-10600000-Daijinkanboukouseikagakuka/0000080278.pdf (accessed on 13 September 2022).
- Bax, M.; Tydeman, C.; Flodmark, O. Clinical and MRI correlates of cerebral palsy: The European Cerebral Palsy Study. JAMA 2006, 296, 1602–1608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, G.; Mjøen, T.R.; Vik, T. Prevalence of speech problems and the use of augmentative and alternative communication in children with cerebral palsy: A registry-based study in Norway. Perspect. Augment. Altern. Commun. 2010, 19, 12–20. [Google Scholar] [CrossRef]
- Kane, G.; Doyle, M.; Kelly, G.; Subramaniam, R.; Cascio, S. A multinational survey on the management of the urinary tract in newborns with spina bifida: Are we following current EAU/ESPU guidelines? Neurourol. Urodyn. 2022, 41, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Jaggi, A.; Fatoye, F. Sub-optimal diagnosis of neurogenic bladder among general practitioners in the United Kingdom-evidence from the Clinical Practice Research Datalink. AME Med. J. 2019, 4, 16. [Google Scholar] [CrossRef]
- Sager, C.; Barroso, U., Jr.; Bastos, J.M.N.; Retamal, G.; Ormaechea, E. Management of neurogenic bladder dysfunction in children update and recommendations on medical treatment. Int. Braz. J. Urol. 2022, 48, 31–51. [Google Scholar] [CrossRef] [PubMed]
- Jiang, M.; Deng, J.; Zhou, G.; Li, S.; Liu, G. Risk factors for recurrent urinary tract infection in children with neurogenic bladder following clean intermittent catheterization. Urology 2022, 164, 224–229. [Google Scholar] [CrossRef] [PubMed]
- McKibben, M.J.; Seed, P.; Ross, S.S.; Borawski, K.M. Urinary tract infection and neurogenic bladder. Urol. Clin. N. Am. 2015, 42, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, N.; Hoberman, A.; Keren, R.; Gotman, N.; Docimo, S.G.; Mathews, R.; Bhatnagar, S.; Ivanova, A.; Mattoo, T.K.; Moxey-Mims, M.; et al. Recurrent urinary tract infections in children with bladder and bowel dysfunction. Pediatrics 2016, 137, e20152982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaudhry, R.; Balsara, Z.R.; Madden-Fuentes, R.J.; Wiener, J.S.; Routh, J.C.; Seed, P.; Ross, S.S. Risk factors associated with recurrent urinary tract infection in neurogenic bladders managed by clean intermittent catheterization. Urology 2017, 102, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Manack, A.; Motsko, S.P.; Haag-Molkenteller, C.; Dmochowski, R.R.; Goehring, E.L., Jr.; Nguyen-Khoa, B.A.; Jones, J.K. Epidemiology and healthcare utilization of neurogenic bladder patients in a US claims database. Neurourol. Urodyn. 2011, 30, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Kanematsu, A.; Johnin, K.; Yoshimura, K.; Imamura, M.; Ogawa, O. Comparison of the effects by obybutynin and tolterodine on spina bifida patients: A pilot crossover study. Low. Urin. Tract Symptoms 2011, 3, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Kennelly, M.J.; Devoe, W.B. Overactive bladder: Pharmacologic treatments in the neurogenic population. Rev. Urol. 2008, 10, 182–191. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| NGB Cohort (n = 1065) | Spina Bifida | Non-Spina Bifida Cohort (n = 651) | |||
|---|---|---|---|---|---|
| Total Cohort (n = 414) | (a) Open (n = 157) | (b) Occulta (n = 257) | |||
| Age at the index month, mean [SD] | 6.7 [4.8] | 4.8 [4.5] ** | 0.7 [1.5] †† | 7.4 [3.9] | 7.8 [4.5] |
| Age at the index month, median (Q1–Q3) | 6.0 (3.0–10.0) | 4.5 (0.0–8.0) | 0.0 (0.0–1.0) | 7.0 (5.0–10.0) | 7.0 (4.0–11.0) |
| Sex, male, n (%) | 633 (59.4) | 229 (55.3) * | 75 (47.8) † | 154 (59.9) | 404 (62.1) |
| Comorbidities, n (%) | |||||
| Dermatitis, unspecified | 459 (43.1) | 167 (40.3) | 67 (42.7) | 100 (38.9) | 292 (44.9) |
| Constipation | 427 (40.1) | 107 (25.8) ** | 36 (22.9) | 71 (27.6) | 320 (49.2) |
| Xerosis cutis | 391 (36.7) | 133 (32.1) * | 54 (34.4) | 79 (30.7) | 258 (39.6) |
| Gastroenteritis and colitis of unspecified origin | 378 (35.5) | 141 (34.1) | 39 (24.8) †† | 102 (39.7) | 237 (36.4) |
| Cramp and spasm | 257 (24.1) | 2 (0.5) ** | 1 (0.6) | 1 (0.4) | 255 (39.2) |
| Epilepsy, unspecified | 240 (22.5) | 17 (4.1) ** | 6 (3.8) | 11 (4.3) | 223 (34.3) |
| Scoliosis, unspecified | 188 (17.7) | 11 (2.7) ** | 3 (1.9) | 8 (3.1) | 177 (27.2) |
| Dislocation of hip | 165 (15.5) | 6 (1.4) ** | 3 (1.9) | 3 (1.2) | 159 (24.4) |
| Developmental disorder of speech and language, unspecified | 106 (10.0) | 11 (2.7) ** | 2 (1.3) | 9 (3.5) | 95 (14.6) |
| Other and unspecified gastroenteritis and colitis of infectious origin | 99 (9.3) | 34 (8.2) | 8 (5.1) | 26 (10.1) | 65 (10.0) |
| Hospitalization, n (%) | 503 (47.2) | 169 (40.8) ** | 119 (75.8) †† | 50 (19.5) | 334 (51.3) |
| NGB Cohort (n = 1065) | Spina Bifida | Non-Spina Bifida Cohort (n = 651) | |||
|---|---|---|---|---|---|
| Total Cohort (n = 414) | (a) Open (n = 157) | (b) Occulta (n = 257) | |||
| Specific tests | |||||
| Urodynamics | 32 (3.0) | 26 (6.3) ** | 14 (8.9) | 12 (4.7) | 6 (0.9) |
| Cystourethrography during urination | 12 (1.1) | 4 (1.0) | 4 (2.5) | 0 (0.0) | 8 (1.2) |
| Static renal scintigraphy | 5 (0.5) | 4 (1.0) | 4 (2.5) † | 0 (0.0) | 1 (0.2) |
| Commonly performed tests | |||||
| Urinalysis § | 354 (33.2) | 181 (43.7) ** | 44 (28.0) †† | 137 (53.3) | 173 (26.6) |
| Urine culture | 89 (8.4) | 35 (8.5) | 15 (9.6) | 20 (7.8) | 54 (8.3) |
| Renal/bladder ultrasound | 408 (38.3) | 255 (61.6) ** | 107 (68.2) † | 148 (57.6) | 153 (23.5) |
| Residual urine measurement | 83 (7.8) | 47 (11.4) ** | 6 (3.8) †† | 41 (16.0) | 36 (5.5) |
| Urine flow measurement | 57 (5.4) | 41 (9.9) ** | 2 (1.3) †† | 39 (15.2) | 16 (2.5) |
| Magnetic resonance imaging | 165 (15.5) | 119 (28.7) ** | 67 (42.7) †† | 52 (20.2) | 46 (7.1) |
| NGB Cohort (n = 1065) | Spina Bifida | Non-Spina Bifida Cohort (n = 651) | |||
|---|---|---|---|---|---|
| Total Cohort (n = 414) | (a) Open (n = 157) | (b) Occulta (n = 257) | |||
| Pharmacological prescription, n (%) | 195 (18.3) | 123 (29.7) ** | 33 (21.0) †† | 90 (35.0) | 72 (11.1) |
| Anticholinergic drugs | 191 (17.9) | 121 (29.2) ** | 33 (21.0) †† | 88 (34.2) | 70 (10.8) |
| Oxybutynin hydrochloride | 77 (7.2) | 57 (13.8) ** | 28 (17.8) | 29 (11.3) | 20 (3.1) |
| Propiverine hydrochloride | 67 (6.3) | 45 (10.9) ** | 6 (3.8) †† | 39 (15.2) | 22 (3.4) |
| Solifenacin succinate | 62 (5.8) | 31 (7.5) | 2 (1.3) †† | 29 (11.3) | 31 (4.8) |
| Imidafenacin | 13 (1.2) | 8 (1.9) | 0 (0.0) † | 8 (3.1) | 5 (0.8) |
| Fesoterodine fumarate | 7 (0.7) | 4 (1.0) | 0 (0.0) | 4 (1.6) | 3 (0.5) |
| Tolterodine tartrate | 2 (0.2) | 2 (0.5) | 0 (0.0) | 2 (0.8) | 0 (0.0) |
| Beta 3-agonists | 5 (0.5) | 3 (0.7) | 0 (0.0) | 3 (1.2) | 2 (0.3) |
| Mirabegron | 3 (0.3) | 1 (0.2) ** | 0 (0.0) | 1 (0.4) | 2 (0.3) |
| Vibegron | 2 (0.2) | 2 (0.5) | 0 (0.0) | 2 (0.8) | 0 (0.0) |
| Other (oral agents) | 3 (0.3) | 1 (0.2) | 0 (0.0) | 1 (0.4) | 2 (0.3) |
| Flavoxate hydrochloride | 3 (0.3) | 1 (0.2) | 0 (0.0) | 1 (0.4) | 2 (0.3) |
| CIC, n (%) | 99 (9.3) | 62 (15.0) ** | 44 (28.0) †† | 18 (7.0) | 37 (5.7) |
| Medicines and CIC, n (%) | 42 (3.9) | 31 (7.5) ** | 24 (15.3) †† | 7 (2.7) | 11 (1.7) |
| Number of medicines, n (%) | |||||
| 0 | 870 (81.7) | 291 (70.3) ‡‡ | 124 (79.0) §§ | 167 (65.0) | 579 (88.9) |
| 1 | 161 (15.1) | 98 (23.7) | 30 (19.1) | 68 (26.5) | 63 (9.7) |
| 2 | 27 (2.5) | 22 (5.3) | 3 (1.9) | 19 (7.4) | 5 (0.8) |
| 3 | 7 (0.7) | 3 (0.7) | 0 (0.0) | 3 (1.2) | 4 (0.6) |
| ≥4 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Mean [SD] | 0.2 [0.5] | 0.4 [0.6] ** | 0.2 [0.5] | 0.4 [0.7] | 0.1 [0.4] |
| Medicine categories, n (%) | |||||
| Anticholinergic drugs only | 187 (17.6) | 119 (28.7) ** | 33 (21.0) †† | 86 (33.5) | 68 (10.4) |
| Beta 3-agonists only | 1 (0.1) | 1 (0.2) | 0 (0.0) | 1 (0.4) | 0 (0.0) |
| Other (oral agents) only | 3 (0.3) | 1 (0.2) | 0 (0.0) | 1 (0.4) | 2 (0.3) |
| Anticholinergic drugs/beta 3-agonists | 4 (0.4) | 2 (0.5) | 0 (0.0) | 2 (0.8) | 2 (0.3) |
| Anticholinergic drugs/other (oral agents) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Beta 3-agonists/other (oral agents) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Anticholinergic drugs/beta 3-agonists/Other (oral agents) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Incidence, n (%) | NGB Cohort (n = 1065) | Spina Bifida | Non-Spina Bifida Cohort (n = 651) | ||
|---|---|---|---|---|---|
| Total Cohort (n = 414) | (a) Open (n = 157) | (b) Occulta (n = 257) | |||
| Lower urinary tract infection | 193 (18.1) | 121 (29.2) ** | 85 (54.1) †† | 36 (14.0) | 72 (11.1) |
| Urinary incontinence | 85 (8.0) | 66 (15.9) ** | 2 (1.3) †† | 64 (24.9) | 19 (2.9) |
| Hydronephrosis | 60 (5.6) | 38 (9.2) ** | 18 (11.5) | 20 (7.8) | 22 (3.4) |
| Obstructive uropathy | 35 (3.3) | 21 (5.1) * | 10 (6.4) | 11 (4.3) | 14 (2.2) |
| Upper urinary tract infection | 35 (3.3) | 16 (3.9) | 12 (7.6) †† | 4 (1.6) | 19 (2.9) |
| Vesicoureteral reflux | 33 (3.1) | 21 (5.1) ** | 10 (6.4) | 11 (4.3) | 12 (1.8) |
| Frequent urination/frequent urination at night | 26 (2.4) | 11 (2.7) | 1 (0.6) | 10 (3.9) | 15 (2.3) |
| Urinary retention | 24 (2.3) | 6 (1.4) | 2 (1.3) | 4 (1.6) | 18 (2.8) |
| Renal failure | 19 (1.8) | 9 (2.2) | 4 (2.5) | 5 (1.9) | 10 (1.5) |
| Sepsis/septicemia | 10 (0.9) | 2 (0.5) | 2 (1.3) | 0 (0.0) | 8 (1.2) |
| Extra-renal urinary overflow | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kitta, T.; Mitsui, T.; Izumi, N. Diagnosis and Treatment of Japanese Children with Neurogenic Bladder: Analysis of Data from a National Health Insurance Database. J. Clin. Med. 2023, 12, 3191. https://doi.org/10.3390/jcm12093191
Kitta T, Mitsui T, Izumi N. Diagnosis and Treatment of Japanese Children with Neurogenic Bladder: Analysis of Data from a National Health Insurance Database. Journal of Clinical Medicine. 2023; 12(9):3191. https://doi.org/10.3390/jcm12093191
Chicago/Turabian StyleKitta, Takeya, Takahiko Mitsui, and Naoko Izumi. 2023. "Diagnosis and Treatment of Japanese Children with Neurogenic Bladder: Analysis of Data from a National Health Insurance Database" Journal of Clinical Medicine 12, no. 9: 3191. https://doi.org/10.3390/jcm12093191