


3-Tesla T2 Mapping Magnetic Resonance Imaging for Evaluation of SLAP Lesions in Patients with Shoulder Pain: An Arthroscopy-Controlled Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design and Reporting
2.3. MRI Protocol and T2 Mapping
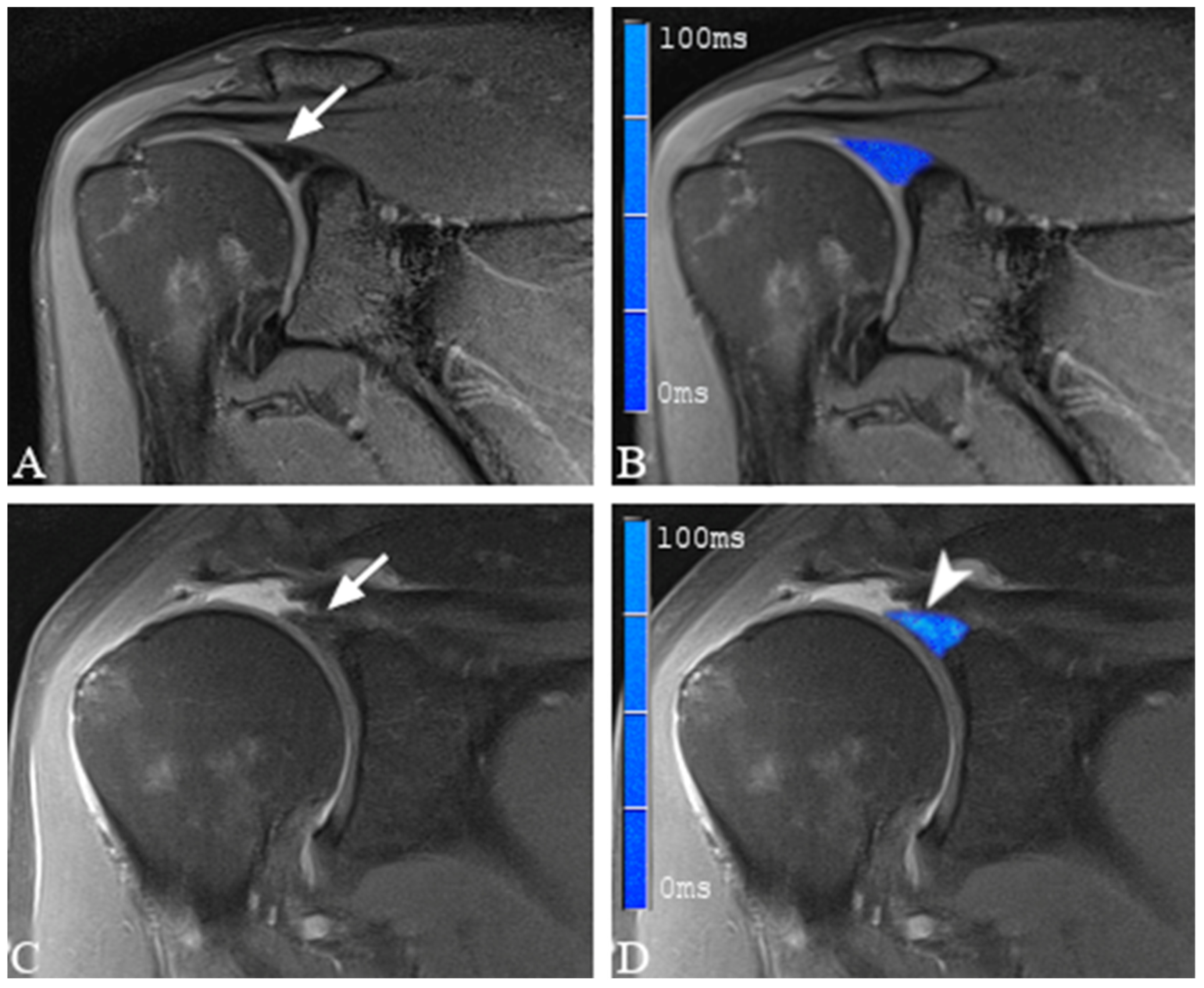
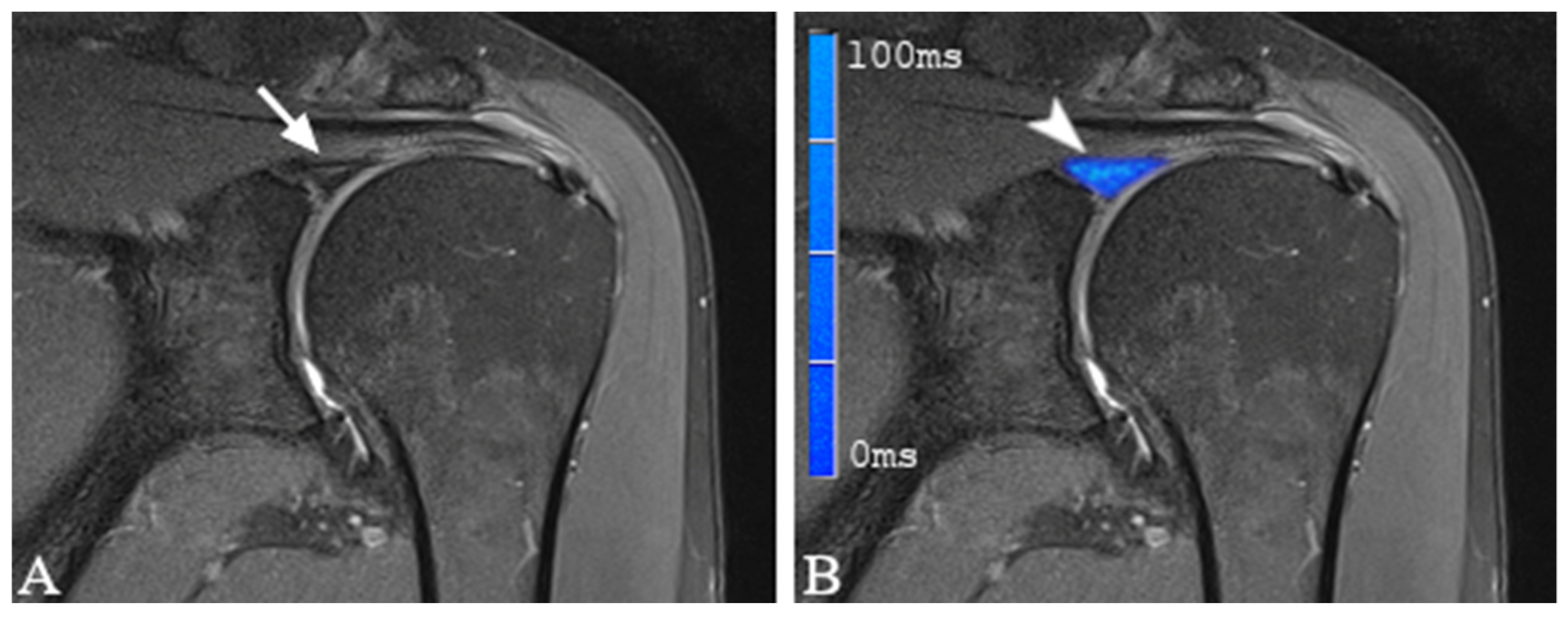
2.4. Image Analysis and Definition of SLAP Lesions
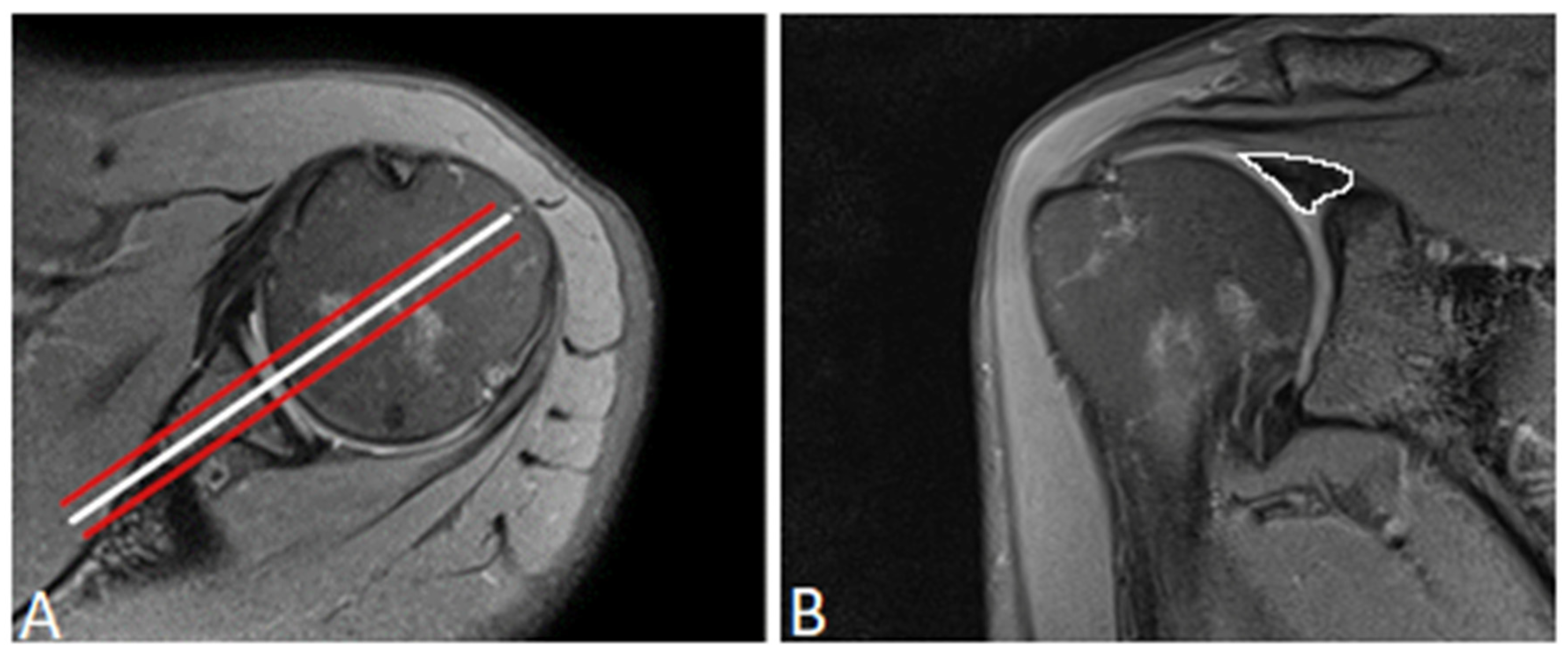
2.5. Placement of Regions of Interest
2.6. Arthroscopy
2.7. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Arthroscopic Evaluation of the Glenoid Labrum
3.3. T2 Mapping of the Glenoid Labrum
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Luime, J.; Koes, B.; Hendriksen, I.; Burdorf, A.; Verhagen, A.; Miedema, H.; Verhaar, J. Prevalence and Incidence of Shoulder Pain in the General Population; a Systematic Review. Scand. J. Rheumatol. 2004, 33, 73–81. [Google Scholar] [CrossRef]
- Rodosky, M.W.; Harner, C.D.; Fu, F.H. The Role of the Long Head of the Biceps Muscle and Superior Glenoid Labrum in Anterior Stability of the Shoulder. Am. J. Sport. Med. 1994, 22, 121–130. [Google Scholar] [CrossRef]
- Pagnani, M.J.; Deng, X.H.; Warren, R.F.; Torzilli, P.A.; Altchek, D.W. Effect of Lesions of the Superior Portion of the Glenoid Labrum on Glenohumeral Translation. J. Bone Jt. Surg. 1995, 77, 1003–1010. [Google Scholar] [CrossRef] [PubMed]
- Kessler, M.A.; Burkart, A.; Weiss, M.; Imhoff, A.B. SLAP-Läsionen Als Ursache Einer Posterioren Instabilität. Orthopade 2003, 32, 642–646. [Google Scholar] [CrossRef]
- Patzer, T.; Lichtenberg, S.; Kircher, J.; Magosch, P.; Habermeyer, P. Influence of SLAP Lesions on Chondral Lesions of the Glenohumeral Joint. Knee Surg. Sport. Traumatol. Arthrosc. 2010, 18, 982–987. [Google Scholar] [CrossRef]
- Reinold, M.M.; Curtis, A.S. Microinstability of the Shoulder in the Overhead Athlete. Int. J. Sport. Phys. Ther. 2013, 8, 601–616. [Google Scholar]
- Onyekwelu, I.; Khatib, O.; Zuckerman, J.D.; Rokito, A.S.; Kwon, Y.W. The Rising Incidence of Arthroscopic Superior Labrum Anterior and Posterior (SLAP) Repairs. J. Shoulder Elb. Surg. 2012, 21, 728–731. [Google Scholar] [CrossRef]
- Weber, S.C.; Martin, D.F.; Seiler, J.G.; Harrast, J.J. Superior Labrum Anterior and Posterior Lesions of the Shoulder. Am. J. Sport. Med. 2012, 40, 1538–1543. [Google Scholar] [CrossRef]
- Dougherty, M.C.; Kulenkamp, J.E.; Boyajian, H.; Koh, J.L.; Lee, M.J.; Shi, L.L. National Trends in the Diagnosis and Repair of SLAP Lesions in the United States. J. Orthop. Surg. 2020, 28, 230949901988855. [Google Scholar] [CrossRef] [PubMed]
- LeVasseur, M.R.; Mancini, M.R.; Hawthorne, B.C.; Romeo, A.A.; Calvo, E.; Mazzocca, A.D. SLAP Tears and Return to Sport and Work: Current Concepts. J. ISAKOS 2021, 6, 204–211. [Google Scholar] [CrossRef]
- Burkhart, S.; Morgan, C. SLAP Lesions in the Overhead Athlete. Orthop. Clin. N. Am. 2001, 32, 431–441. [Google Scholar] [CrossRef]
- Schwartzberg, R.; Reuss, B.L.; Burkhart, B.G.; Butterfield, M.; Wu, J.Y.; McLean, K.W. High Prevalence of Superior Labral Tears Diagnosed by MRI in Middle-Aged Patients with Asymptomatic Shoulders. Orthop. J. Sport. Med. 2016, 4, 232596711562321. [Google Scholar] [CrossRef]
- Chandnani, V.; Ho, C.; Gerharter, J.; Neumann, C.; Kursunoglu-Brahme, S.; Sartoris, D.J.; Resnick, D. MR Findings in Asymptomatic Shoulders: A Blind Analysis Using Symptomatic Shoulders as Controls. Clin. Imaging 1992, 16, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Pfahler, M.; Haraida, S.; Schulz, C.; Anetzberger, H.; Refior, H.J.; Bauer, G.S.; Bigliani, L.U. Age-Related Changes of the Glenoid Labrum in Normal Shoulders. J. Shoulder Elb. Surg. 2003, 12, 40–52. [Google Scholar] [CrossRef]
- Prodromos, C.C.; Ferry, J.A.; Schiller, A.L.; Zarins, B. Histological Studies of the Glenoid Labrum from Fetal Life to Old Age. J. Bone Jt. Surg. Am. 1990, 72, 1344–1348. [Google Scholar] [CrossRef]
- Vogel, L.A.; Moen, T.C.; Macaulay, A.A.; Arons, R.R.; Cadet, E.R.; Ahmad, C.S.; Levine, W.N. Superior Labrum Anterior-to-Posterior Repair Incidence: A Longitudinal Investigation of Community and Academic Databases. J. Shoulder Elb. Surg. 2014, 23, e119–e126. [Google Scholar] [CrossRef] [PubMed]
- Enad, J.G.; Gaines, R.J.; White, S.M.; Kurtz, C.A. Arthroscopic Superior Labrum Anterior-Posterior Repair in Military Patients. J. Shoulder Elb. Surg. 2007, 16, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Friel, N.A.; Karas, V.; Slabaugh, M.A.; Cole, B.J. Outcomes of Type II Superior Labrum, Anterior to Posterior (SLAP) Repair: Prospective Evaluation at a Minimum Two-Year Follow-Up. J. Shoulder Elb. Surg. 2010, 19, 859–867. [Google Scholar] [CrossRef] [PubMed]
- Stetson, W.B.; Snyder, S.J. Clinical Presentation and Follow-up of Isolated SLAP Lesions of the Shoulder (SS-04). Arthrosc. J. Arthrosc. Relat. Surg. 2011, 27, e30–e31. [Google Scholar] [CrossRef]
- Neri, B.R.; ElAttrache, N.S.; Owsley, K.C.; Mohr, K.; Yocum, L.A. Outcome of Type II Superior Labral Anterior Posterior Repairs in Elite Overhead Athletes. Am. J. Sport. Med. 2011, 39, 114–120. [Google Scholar] [CrossRef]
- DeFazio, M.W.; Özkan, S.; Wagner, E.R.; Warner, J.J.P.; Chen, N.C. Isolated Type II SLAP Tears Undergo Reoperation More Frequently. Knee Surg. Sport. Traumatol. Arthrosc. 2021, 29, 2570–2578. [Google Scholar] [CrossRef]
- Chloros, G.D.; Haar, P.J.; Loughran, T.P.; Hayes, C.W. Imaging of Glenoid Labrum Lesions. Clin. Sport. Med. 2013, 32, 361–390. [Google Scholar] [CrossRef] [PubMed]
- de Coninck, T.; Ngai, S.S.; Tafur, M.; Chung, C.B. Imaging the Glenoid Labrum and Labral Tears. RadioGraphics 2016, 36, 1628–1647. [Google Scholar] [CrossRef] [PubMed]
- Connolly, K.P.; Schwartzberg, R.S.; Reuss, B.; Crumbie, D.; Homan, B.M. Sensitivity and Specificity of Noncontrast Magnetic Resonance Imaging Reports in the Diagnosis of Type-II Superior Labral Anterior-Posterior Lesions in the Community Setting. J. Bone Jt. Surg.-Am. Vol. 2013, 95, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Connell, D.A.; Potter, H.G.; Wickiewicz, T.L.; Altchek, D.W.; Warren, R.F. Noncontrast Magnetic Resonance Imaging of Superior Labral Lesions. Am. J. Sport. Med. 1999, 27, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.F.; Youssef, A.O. The Diagnostic Value of Magnetic Resonance Arthrography of the Shoulder in Detection and Grading of SLAP Lesions: Comparison with Arthroscopic Findings. Eur. J. Radiol. 2012, 81, 2343–2347. [Google Scholar] [CrossRef] [PubMed]
- Arnold, H. Non-Contrast Magnetic Resonance Imaging for Diagnosing Shoulder Injuries. J. Orthop. Surg. 2012, 20, 361–364. [Google Scholar] [CrossRef]
- Houtz, C.G.; Schwartzberg, R.S.; Barry, J.A.; Reuss, B.L.; Papa, L. Shoulder MRI Accuracy in the Community Setting. J. Shoulder Elb. Surg. 2011, 20, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Rehnitz, C.; Klaan, B.; Burkholder, I.; von Stillfried, F.; Kauczor, H.-U.; Weber, M.-A. Delayed Gadolinium-Enhanced MRI of Cartilage (DGEMRIC) and T 2 Mapping at 3T MRI of the Wrist: Feasibility and Clinical Application. J. Magn. Reson. Imaging 2017, 45, 381–389. [Google Scholar] [CrossRef]
- Hesper, T.; Neugroda, C.; Schleich, C.; Antoch, G.; Hosalkar, H.; Krauspe, R.; Zilkens, C.; Bittersohl, B. T2*-Mapping of Acetabular Cartilage in Patients with Femoroacetabular Impingement at 3 Tesla: Comparative Analysis with Arthroscopic Findings. Cartilage 2018, 9, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Bittersohl, B.; Miese, F.R.; Dekkers, C.; Senyurt, H.; Kircher, J.; Wittsack, H.-J.; Antoch, G.; Krauspe, R.; Zilkens, C. T2* Mapping and Delayed Gadolinium-Enhanced Magnetic Resonance Imaging in Cartilage (DGEMRIC) of Glenohumeral Cartilage in Asymptomatic Volunteers at 3 T. Eur. Radiol. 2013, 23, 1367–1374. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-Y.; Park, H.-J.; Kwon, H.-J.; Kim, M.S.; Choi, S.H.; Choi, Y.J.; Kim, E. T2 Relaxation Times of the Glenohumeral Joint at 3.0 T MRI in Patients with and without Primary and Secondary Osteoarthritis. Acta Radiol. 2015, 56, 1388–1395. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, J.C.; Liu, F.; Blankenbaker, D.G.; Woo, K.M.; Kijowski, R. Juvenile Osteochondritis Dissecans: Cartilage T2 Mapping of Stable Medial Femoral Condyle Lesions. Radiology 2018, 288, 536–543. [Google Scholar] [CrossRef]
- Renner, N.; Kleyer, A.; Krönke, G.; Simon, D.; Söllner, S.; Rech, J.; Uder, M.; Janka, R.; Schett, G.; Welsch, G.H.; et al. T2 Mapping as a New Method for Quantitative Assessment of Cartilage Damage in Rheumatoid Arthritis. J. Rheumatol. 2020, 47, 820–825. [Google Scholar] [CrossRef] [PubMed]
- Eijgenraam, S.M.; Bovendeert, F.A.T.; Verschueren, J.; van Tiel, J.; Bastiaansen-Jenniskens, Y.M.; Wesdorp, M.A.; Nasserinejad, K.; Meuffels, D.E.; Guenoun, J.; Klein, S.; et al. T2 Mapping of the Meniscus Is a Biomarker for Early Osteoarthritis. Eur. Radiol. 2019, 29, 5664–5672. [Google Scholar] [CrossRef]
- Bossuyt, P.M.; Reitsma, J.B.; Bruns, D.E.; Gatsonis, C.A.; Glasziou, P.P.; Irwig, L.; Lijmer, J.G.; Moher, D.; Rennie, D.; de Vet, H.C.W.; et al. STARD 2015: An Updated List of Essential Items for Reporting Diagnostic Accuracy Studies. Radiology 2015, 277, 826–832. [Google Scholar] [CrossRef]
- Snyder, S.J.; Karzel, R.P.; del Pizzo, W.; Ferkel, R.D.; Friedman, M.J. SLAP Lesions of the Shoulder. Arthrosc. J. Arthrosc. Relat. Surg. 1990, 6, 274–279. [Google Scholar] [CrossRef]
- Shrout, P.E.; Fleiss, J.L. Intraclass Correlations: Uses in Assessing Rater Reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Alashkham, A.; Alraddadi, A.; Felts, P.; Soames, R. Histology, Vascularity and Innervation of the Glenoid Labrum. J. Orthop. Surg. 2018, 26, 230949901877090. [Google Scholar] [CrossRef]
- Cooper, D.E.; Arnoczky, S.P.; O’Brien, S.J.; Warren, R.F.; DiCarlo, E.; Allen, A.A. Anatomy, Histology, and Vascularity of the Glenoid Labrum. An Anatomical Study. J. Bone Jt. Surg. Am. 1992, 74, 46–52. [Google Scholar] [CrossRef]
- Bain, G.I.; Galley, I.J.; Singh, C.; Carter, C.; Eng, K. Anatomic Study of the Superior Glenoid Labrum. Clin. Anat. 2013, 26, 367–376. [Google Scholar] [CrossRef] [PubMed]
- Cook, J.L.; Purdam, C.R. Is Tendon Pathology a Continuum? A Pathology Model to Explain the Clinical Presentation of Load-Induced Tendinopathy. Br. J. Sport. Med. 2009, 43, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Khan, K.M.; Cook, J.L.; Bonar, F.; Harcourt, P.; Astrom, M. Histopathology of Common Tendinopathies. Sport. Med. 1999, 27, 393–408. [Google Scholar] [CrossRef] [PubMed]
- Pollard, T.C.B.; Gwilym, S.E.; Carr, A.J. The Assessment of Early Osteoarthritis. J. Bone Jt. Surg. Br. 2008, 90-B, 411–421. [Google Scholar] [CrossRef] [PubMed]
- Liess, C.; Lüsse, S.; Karger, N.; Heller, M.; Glüer, C.-C. Detection of Changes in Cartilage Water Content Using MRI T2-Mapping in Vivo. Osteoarthr. Cartil. 2002, 10, 907–913. [Google Scholar] [CrossRef]
- Xie, Y.; Liu, S.; qiao, Y.; Hu, Y.; Zhang, Y.; Qu, J.; Shen, Y.; Tao, H.; Chen, S. Quantitative T2 Mapping-Based Tendon Healing Is Related to the Clinical Outcomes during the First Year after Arthroscopic Rotator Cuff Repair. Knee Surg. Sport. Traumatol. Arthrosc. 2021, 29, 127–135. [Google Scholar] [CrossRef]
- Soellner, S.T.; Goldmann, A.; Muelheims, D.; Welsch, G.H.; Pachowsky, M.L. Intraoperative Validation of Quantitative T2 Mapping in Patients with Articular Cartilage Lesions of the Knee. Osteoarthr. Cartil. 2017, 25, 1841–1849. [Google Scholar] [CrossRef]
- Golditz, T.; Steib, S.; Pfeifer, K.; Uder, M.; Gelse, K.; Janka, R.; Hennig, F.F.; Welsch, G.H. Functional Ankle Instability as a Risk Factor for Osteoarthritis: Using T2-Mapping to Analyze Early Cartilage Degeneration in the Ankle Joint of Young Athletes. Osteoarthr. Cartil. 2014, 22, 1377–1385. [Google Scholar] [CrossRef]
- Monu, J.U.; Pope, T.L.; Chabon, S.J.; Vanarthos, W.J. MR Diagnosis of Superior Labral Anterior Posterior (SLAP) Injuries of the Glenoid Labrum: Value of Routine Imaging without Intraarticular Injection of Contrast Material. Am. J. Roentgenol. 1994, 163, 1425–1429. [Google Scholar] [CrossRef]
- Major, N.M.; Browne, J.; Domzalski, T.; Cothran, R.L.; Helms, C.A. Evaluation of the Glenoid Labrum With 3-T MRI: Is Intraarticular Contrast Necessary? Am. J. Roentgenol. 2011, 196, 1139–1144. [Google Scholar] [CrossRef]
- Wuennemann, F.; Kintzelé, L.; Braun, A.; Zeifang, F.; Maier, M.W.; Burkholder, I.; Weber, M.-A.; Kauczor, H.-U.; Rehnitz, C. 3-T T2 Mapping Magnetic Resonance Imaging for Biochemical Assessment of Normal and Damaged Glenoid Cartilage: A Prospective Arthroscopy-Controlled Study. Sci. Rep. 2020, 10, 14396. [Google Scholar] [CrossRef] [PubMed]
- Le, J.; Peng, Q.; Sperling, K. Biochemical Magnetic Resonance Imaging of Knee Articular Cartilage: T1rho and T2 Mapping as Cartilage Degeneration Biomarkers. Ann. N. Y. Acad. Sci. 2016, 1383, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Rehnitz, C.; Kuni, B.; Wuennemann, F.; Chloridis, D.; Kirwadi, A.; Burkholder, I.; Kauczor, H.-U.; Weber, M.-A. Delayed Gadolinium-Enhanced MRI of Cartilage (DGEMRIC) and T 2 Mapping of Talar Osteochondral Lesions: Indicators of Clinical Outcomes. J. Magn. Reson. Imaging 2017, 46, 1601–1610. [Google Scholar] [CrossRef] [PubMed]
- Rehnitz, C.; Kupfer, J.; Streich, N.A.; Burkholder, I.; Schmitt, B.; Lauer, L.; Kauczor, H.-U.; Weber, M.-A. Comparison of Biochemical Cartilage Imaging Techniques at 3 T MRI. Osteoarthr. Cartil. 2014, 22, 1732–1742. [Google Scholar] [CrossRef]
- Mosher, T.J.; Smith, H.; Dardzinski, B.J.; Schmithorst, V.J.; Smith, M.B. MR Imaging and T2 Mapping of Femoral Cartilage. Am. J. Roentgenol. 2001, 177, 665–669. [Google Scholar] [CrossRef]
- Kaneko, Y.; Nozaki, T.; Yu, H.; Chang, A.; Kaneshiro, K.; Schwarzkopf, R.; Hara, T.; Yoshioka, H. Normal T2 Map Profile of the Entire Femoral Cartilage Using an Angle/Layer-Dependent Approach. J. Magn. Reson. Imaging 2015, 42, 1507–1516. [Google Scholar] [CrossRef]
- Watanabe, A.; Boesch, C.; Siebenrock, K.; Obata, T.; Anderson, S.E. T2 Mapping of Hip Articular Cartilage in Healthy Volunteers at 3T: A Study of Topographic Variation. J. Magn. Reson. Imaging 2007, 26, 165–171. [Google Scholar] [CrossRef]
- Sasaki, T.; Yodono, H.; Prado, G.L.M.; Saito, Y.; Miura, H.; Itabashi, Y.; Ootsuka, H.; Ishibashi, Y. Increased Signal Intensity in the Normal Glenoid Labrum in MR Imaging: Diagnostic Pitfalls Caused by the Magic-Angle Effect. Magn. Reson. Med. Sci. 2002, 1, 149–156. [Google Scholar] [CrossRef]
- Kang, Y.; Choi, J.-A. T2 Mapping of Articular Cartilage of the Glenohumeral Joint at 3.0 T in Healthy Volunteers: A Feasibility Study. Skelet. Radiol. 2016, 45, 915–920. [Google Scholar] [CrossRef]
- Lockard, C.A.; Wilson, K.J.; Ho, C.P.; Shin, R.C.; Katthagen, J.C.; Millett, P.J. Quantitative Mapping of Glenohumeral Cartilage in Asymptomatic Subjects Using 3 T Magnetic Resonance Imaging. Skelet. Radiol 2018, 47, 671–682. [Google Scholar] [CrossRef]
- Lansdown, D.A.; Wang, K.; Cotter, E.; Davey, A.; Cole, B.J. Relationship Between Quantitative MRI Biomarkers and Patient-Reported Outcome Measures After Cartilage Repair Surgery: A Systematic Review. Orthop. J. Sport. Med. 2018, 6, 232596711876544. [Google Scholar] [CrossRef] [PubMed]
- Jungmann, P.M.; Baum, T.; Bauer, J.S.; Karampinos, D.C.; Erdle, B.; Link, T.M.; Li, X.; Trattnig, S.; Rummeny, E.J.; Woertler, K.; et al. Cartilage Repair Surgery: Outcome Evaluation by Using Noninvasive Cartilage Biomarkers Based on Quantitative MRI Techniques? BioMed. Res. Int. 2014, 2014, 1–17. [Google Scholar] [CrossRef]
- Stathellis, A.; Brilakis, E.; Georgoulis, J.-D.; Antonogiannakis, E.; Georgoulis, A. Treatment of SLAP Lesions. Open Orthop. J. 2018, 12, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Brockmeyer, M.; Tompkins, M.; Kohn, D.M.; Lorbach, O. SLAP Lesions: A Treatment Algorithm. Knee Surg. Sport. Traumatol. Arthrosc. 2016, 24, 447–455. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Sequence | Orientation | Repetition Time (TR; ms) | Echo Time (TE; ms) | Acquisition Matrix | Flip Angle | Echo Train Length | No. of Slices | TA (Min) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | PD fs TSE | axial | 3660 | 24 | 384 × 346 | 176 | 7 | 27 | 04:32 |
| 2 | PD fs TSE | oblique coronal | 2490 | 24 | 384 × 307 | 160 | 7 | 19 | 03:37 |
| 3 | PD fs TSE | oblique sagittal | 3950 | 23 | 320 × 256 | 140 | 7 | 29 | 04:49 |
| 4 | PD TSE | oblique coronal | 1670 | 23 | 384 × 307 | 160 | 5 | 19 | 03:24 |
| 5 | T1 SE | oblique coronal | 787 | 10 | 384 × 346 | 90 | 1 | 19 | 04:51 |
| 6 | T2 TSE | oblique sagittal | 5640 | 88 | 384 × 307 | 150 | 15 | 29 | 02:33 |
| 7 | T2 MapIt | oblique coronal | 2140 | 13.8, 27.6, 41.4, 55.2, 69 | 320 × 320 | 180 | 1 | 16 | 06:50 |
| SLAP Lesion | ||||
|---|---|---|---|---|
| No (N = 6) | Yes (N = 12) | p-Value Wilcoxon | ||
| Gender | male | 3 (50.0%) | 9 (75.0%) | |
| female | 3 (50.0%) | 3 (25.0%) | ||
| Age (years) | n | 6 | 12 | 0.2216 |
| Mean | 46.2 | 55.5 | ||
| SD | 18.82 | 11.93 | ||
| Median | 53.5 | 58.5 | ||
| Min | 22.0 | 29.0 | ||
| Max | 64.0 | 67.0 | ||
| Total (N = 18) | ||
|---|---|---|
| SLAP lesion | no | 6 (33.3%) |
| yes | 12 (66.7%) | |
| SLAP Classification | SLAP 1 | 9 (75.0%) |
| SLAP 2 | 1 (8.3%) | |
| SLAP 3 | 2 (16.7%) | |
| SLAP 4 | -- | |
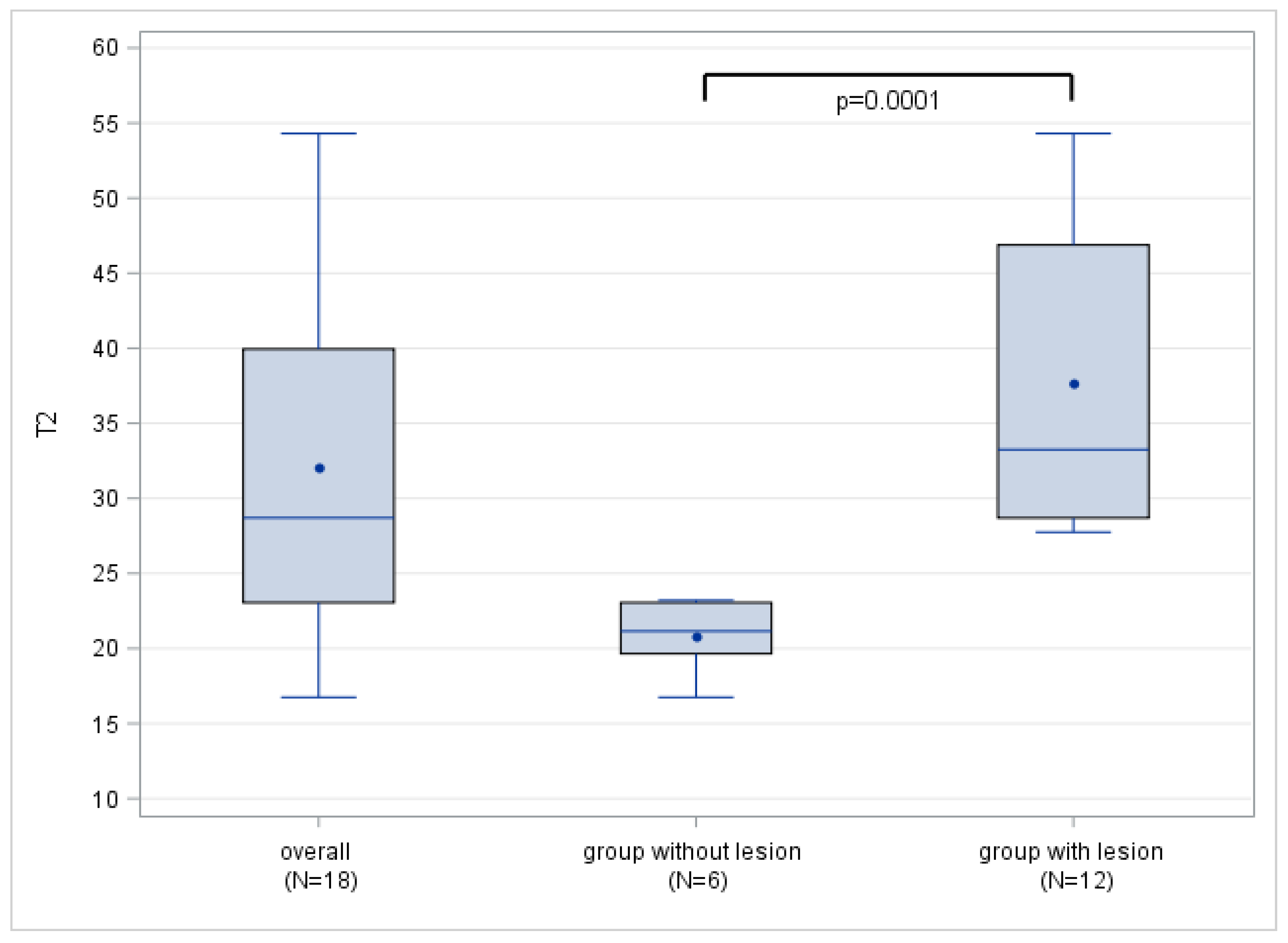
| Overall | Population without Lesion | Population with Lesion | ||
|---|---|---|---|---|
| T2 | n | 18 | 6 | 12 |
| Mean | 32.1 | 20.8 | 37.7 | |
| SD | 11.90 | 2.40 | 10.63 | |
| Median | 28.7 | 21.2 | 33.3 | |
| Min | 16.8 | 16.8 | 27.8 | |
| Max | 54.3 | 21.2 | 54.3 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stein, P.; Wuennemann, F.; Schneider, T.; Zeifang, F.; Burkholder, I.; Weber, M.-A.; Kauczor, H.-U.; Rehnitz, C. 3-Tesla T2 Mapping Magnetic Resonance Imaging for Evaluation of SLAP Lesions in Patients with Shoulder Pain: An Arthroscopy-Controlled Study. J. Clin. Med. 2023, 12, 3109. https://doi.org/10.3390/jcm12093109
Stein P, Wuennemann F, Schneider T, Zeifang F, Burkholder I, Weber M-A, Kauczor H-U, Rehnitz C. 3-Tesla T2 Mapping Magnetic Resonance Imaging for Evaluation of SLAP Lesions in Patients with Shoulder Pain: An Arthroscopy-Controlled Study. Journal of Clinical Medicine. 2023; 12(9):3109. https://doi.org/10.3390/jcm12093109
Chicago/Turabian StyleStein, Patrick, Felix Wuennemann, Thomas Schneider, Felix Zeifang, Iris Burkholder, Marc-André Weber, Hans-Ulrich Kauczor, and Christoph Rehnitz. 2023. "3-Tesla T2 Mapping Magnetic Resonance Imaging for Evaluation of SLAP Lesions in Patients with Shoulder Pain: An Arthroscopy-Controlled Study" Journal of Clinical Medicine 12, no. 9: 3109. https://doi.org/10.3390/jcm12093109