
Marinobufagenin, Left Ventricular Hypertrophy and Residual Renal Function in Kidney Transplant Recipients
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients’ Selection
2.2. Clinical Assessment
2.3. Exploratory Follow-Up
2.4. Statistical Analysis
3. Results
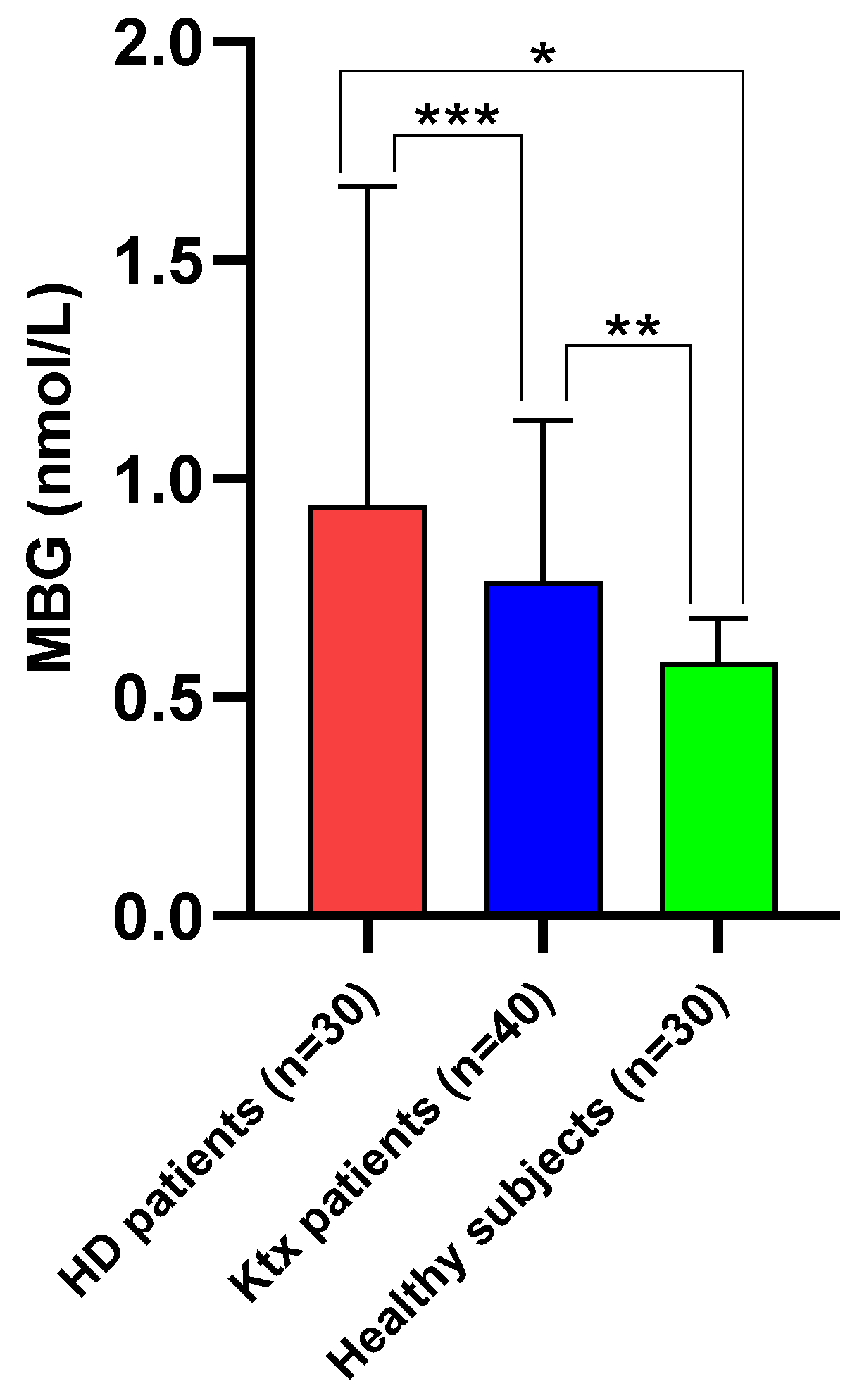
3.1. Main Characteristics of the Study Population
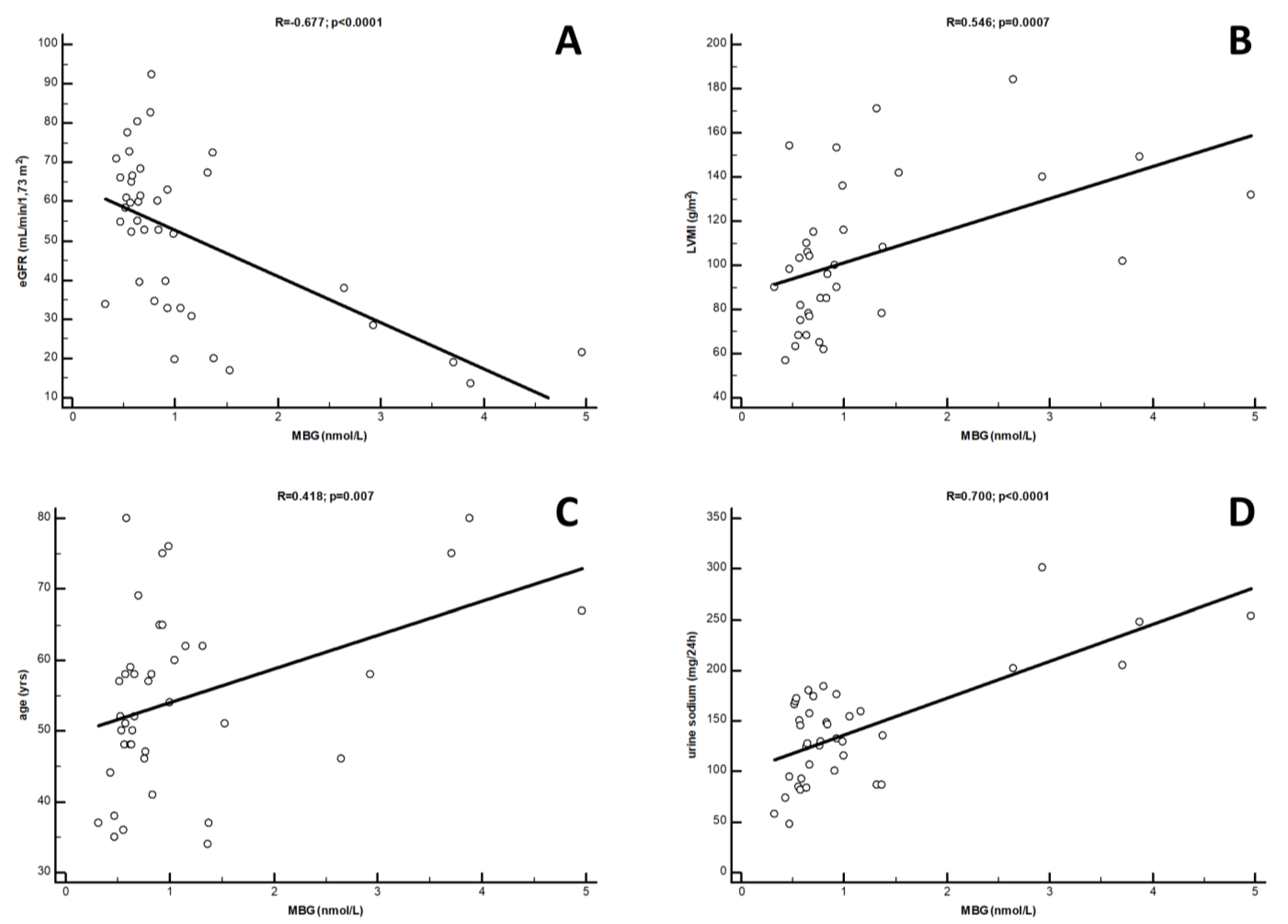
3.2. Clinical Correlates of MBG
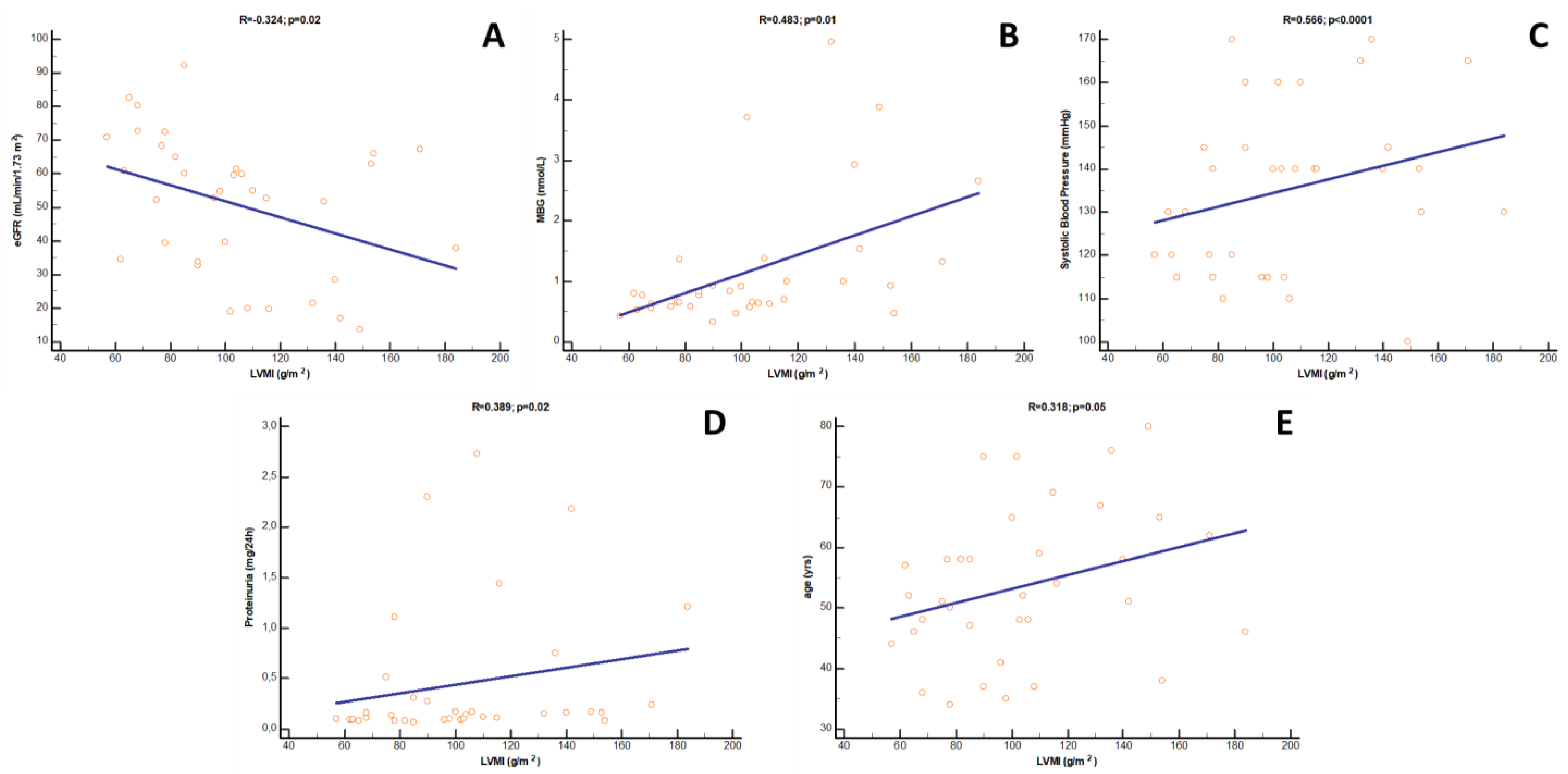
3.3. Clinical Correlates of LVMi
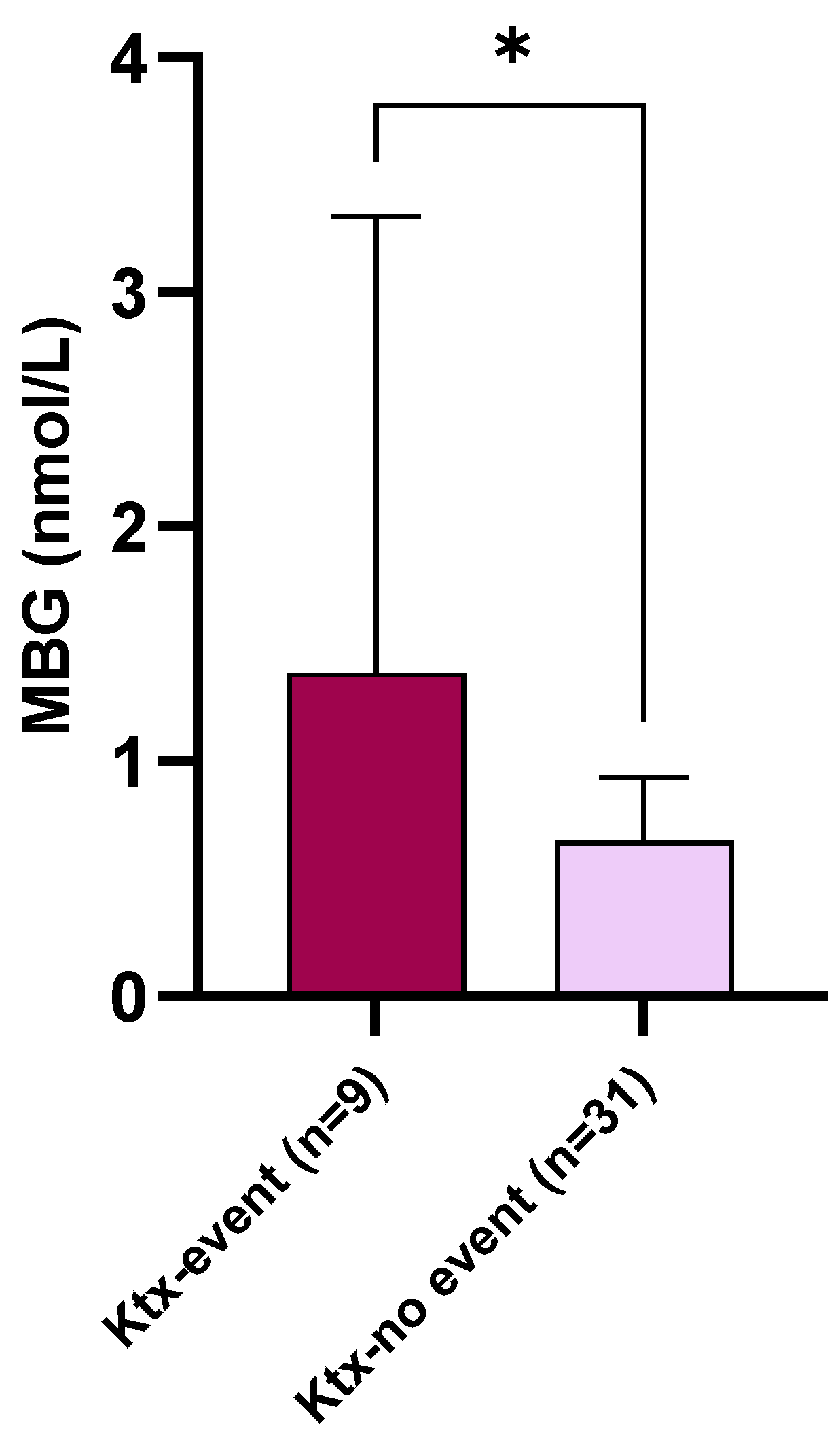
3.4. Exploratory Cardio-Renal Endpoint in Ktx Recipients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hariharan, S.; Israni, A.K.; Danovitch, G. Long-Term Survival after Kidney Transplantation. N. Engl. J. Med. 2021, 385, 729–743. [Google Scholar] [CrossRef] [PubMed]
- Ojo, A.O.; Hanson, J.A.; Wolfe, R.A.; Leichtman, A.B.; Agodoa, L.Y.; Port, F.K. Long-term survival in renal transplant recipients with graft function. Kidney Int. 2000, 57, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, D. Left ventricular hypertrophy after renal transplantation: New approach to a deadly disorder. Nephrol. Dial. Transplant. 2004, 19, 1682–1686. [Google Scholar] [CrossRef] [PubMed]
- Schoner, W. Endogenous cardiac glycosides, a new class of steroid hormones. Eur. J. Biochem. 2002, 269, 2440–2448. [Google Scholar] [CrossRef] [PubMed]
- Fedorova, O.V.; Fadeev, A.V.; Grigorova, Y.N.; Marshall, C.A.; Zernetkina, V.; Kolodkin, N.I.; Agalakova, N.I.; Konradi, A.O.; Lakatta, E.G.; Bagrov, A.Y. Cardiotonic Steroids Induce Vascular Fibrosis Via Pressure-Independent Mechanism in NaCl-Loaded Diabetic Rats. J. Cardiovasc. Pharmacol. 2019, 74, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Elkareh, J.; Kennedy, D.J.; Yashaswi, B.; Vetteth, S.; Shidyak, A.; Kim, E.G.R.; Smaili, S.; Periyasamy, S.M.; Hariri, I.M.; Fedorova, L.; et al. Marinobufagenin stimulates fibroblast collagen production and causes fibrosis in experimental uremic cardiomyopathy. Hypertension 2007, 49, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Keppel, M.H.; Piecha, G.; März, W.; Cadamuro, J.; Auer, S.; Felder, T.K.; Mrazek, C.; Oberkofler, H.; Trummer, C.; Grübler, M.R.; et al. The endogenous cardiotonic steroid Marinobufagenin and decline in estimated glomerular filtration rate at follow-up in patients with arterial hypertension. PLoS ONE 2019, 14, e0212973. [Google Scholar] [CrossRef] [PubMed]
- Bolignano, D.; De Rosa, S.; Greco, M.; Presta, P.; Patella, G.; Crugliano, G.; Sabatino, J.; Strangio, A.; Romano, L.R.; Comi, A.; et al. Marinobufagenin, left ventricular geometry and cardiac dysfunction in end-stage kidney disease patients. Int. Urol. Nephrol. 2022, 54, 2581–2589. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef] [PubMed]
- Puschett, J.B.; Agunanne, E.; Uddin, M.N. Emerging role of the bufadienolides in cardiovascular and kidney diseases. Am. J. Kidney Dis. 2010, 56, 359–370. [Google Scholar] [CrossRef] [PubMed]
- Pavlovic, D. The role of cardiotonic steroids in the pathogenesis of cardiomyopathy in chronic kidney disease. Nephron Clin. Pract. 2014, 128, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Hamlyn, J.M.; Manunta, P. Endogenous cardiotonic steroids in kidney failure: A review and an hypothesis. Adv. Chronic Kidney Dis. 2015, 22, 232–244. [Google Scholar] [CrossRef] [PubMed]
- Bagrov, A.Y.; Shapiro, J.I.; Fedorova, O.V. Endogenous cardiotonic steroids: Physiology, pharmacology, and novel therapeutic targets. Pharmacol. Rev. 2009, 61, 9–38. [Google Scholar] [CrossRef] [PubMed]
- Bolignano, D.; Greco, M.; Presta, P.; Crugliano, G.; Sabatino, J.; Carullo, N.; Arena, R.; Leo, I.; Comi, A.; Andreucci, M.; et al. Altered circulating marinobufagenin levels and recurrent intradialytic hypotensive episodes in chronic hemodialysis patients: A pilot, prospective study. Rev. Cardiovasc. Med. 2021, 22, 1577–1587. [Google Scholar] [CrossRef] [PubMed]
- Gansevoort, R.T.; Correa-Rotter, R.; Hemmelgarn, B.R.; Jafar, T.H.; Heerspink, H.J.L.; Mann, J.F.; Matsushita, K.; Wen, C.P. Chronic kidney disease and cardiovascular risk: Epidemiology, mechanisms, and prevention. Lancet 2013, 382, 339–352. [Google Scholar] [CrossRef] [PubMed]
- Piecha, G.; Kujawa-Szewieczek, A.; Kuczera, P.; Skiba, K.; Sikora-Grabka, E.; Wiecek, A. Plasma marinobufagenin immunoreactivity in patients with chronic kidney disease: A case control study. Am. J. Physiol.-Renal Physiol. 2018, 315, F637–F643. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, D.J.; Shrestha, K.; Sheehey, B.; Li, X.S.; Guggilam, A.; Wu, Y.; Finucan, M.; Gabi, A.; Medert, C.M.; Westfall, K.M.; et al. Elevated Plasma Marinobufagenin, An Endogenous Cardiotonic Steroid, Is Associated With Right Ventricular Dysfunction and Nitrative Stress in Heart Failure. Circ. Heart Fail. 2015, 8, 1068–1076. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n = 40 | |
|---|---|
| Age (yrs) | 56.6 ± 12.5 |
| Gender (%Male) | 65 |
| Dialysis vintage (mo.) | 33.5 [13–65] |
| Ktx vintage (yrs) | 9 [3–18] |
| DD Ktx (%) | 85 |
| BMI (kg/m2) | 26.1 ± 4.9 |
| WHR (cm/cm) | 0.92 ± 0.08 |
| Current smokers (%) | 15 |
| Immunosuppressive Therapy (%): | |
| 82.5 |
| 92.5 |
| 72.5 |
| -m-TORi | 10 |
| Any RAAS blocker (%) | 30 |
| Diabetes (%) | 25 |
| Coronary disease (%) | 2.5 |
| Heart failure (%) | 5 |
| Hypertension (%) | 65 |
| SBP (mmHg) | 135 ± 18 |
| DBP (mmHg) | 85 ± 6.6 |
| LAVi (mL/m2) | 35.1 ± 13 |
| LVMi (g/m2) | 104 ± 33 |
| Ejection Fraction (%) | 59.3 ± 3.6 |
| Vmax (m/s) | 2.06 ± 0.54 |
| TAPSE (mm) | 21.8 ± 2.2 |
| E/e’ | 9.4 ± 3.9 |
| RAVi (mL/m2) | 18.3 ± 7.3 |
| Glycemia (mg/dL) | 96.5 ± 22.9 |
| eGFR (CKD-EpimL/min/1.73 m2) | 54.8 [32.7–66.1] |
| Proteinuria (g/24 h) | 0.15 [0.10–0.40] |
| Urine sodium (mg/24 h) | 142.2 ± 52.2 |
| Urine potassium (mg/24 h) | 48 [41.2–60] |
| Urea (mg/dL) | 55 [43.5–89.5] |
| Serum Phosphate (mg/dL) | 3.34 ± 0.97 |
| Serum Calcium (mg/dL) | 9.6 ± 0.82 |
| Parathormone (pg/mL) | 122.7 [68.6–167.2] |
| Alkaline Phosphatase (U/L) | 80.4 ± 20.5 |
| Total Cholesterol (mg/dL) | 184.6 ± 36.7 |
| LDL Cholesterol (mg/dL) | 109.5 ± 34.2 |
| Triglycerides (mg/dL) | 140.5 ± 55.8 |
| Fibrinogen (mg/dL) | 352.3 ± 99.1 |
| ESR (mm/h) | 15 [9–27] |
| Albumin (g/dL) | 4.38 ± 0.35 |
| RBC (n × 106) | 4.68 ± 0.82 |
| Hb (g/dL) | 12.6 ± 1.9 |
| C-reactive protein (mg/L) | 3.23 [2.13–4.10] |
| Ferritin (mg/dL) | 38 [16.5–97] |
| TSAT (%) | 31.7 ± 5.7 |
| Serumiron (mg/dL) | 66.1 ± 28.9 |
| MBG (nmol/L) | 0.765 [0.580–1.105] |
| Univariate Correlation Coefficient | p | |
|---|---|---|
| (log)eGFR | −0.677 | <0.0001 |
| Urinary Sodium | 0.700 | <0.0001 |
| LVMi | 0.546 | 0.0007 |
| Age | 0.418 | 0.007 |
| Gender | 0.319 | 0.04 |
| Multivariate Standardized Correlation Coefficient (β) | p | |
| Urinary Sodium | 0.423 | 0.01 |
| (log)eGFR | −0.324 | 0.02 |
| LVMi | 0.244 | 0.11 |
| Age | 0.756 | 0.45 |
| Gender | 0.594 | 0.55 |
| Univariate Correlation Coefficient | p | |
|---|---|---|
| Systolic Blood Pressure | 0.566 | <0.0001 |
| (log)MBG | 0.483 | 0.01 |
| (log)eGFR | −0.374 | 0.02 |
| (log)Proteinuria | 0.389 | 0.02 |
| Age | 0.318 | 0.05 |
| Multivariate Standardized Correlation Coefficient (β) | p | |
| Systolic Blood Pressure | 0.319 | 0.01 |
| (log)eGFR | −0.201 | 0.01 |
| (log)MBG | 0.257 | 0.08 |
| (log)Proteinuria | 0.231 | 0.25 |
| Age | 0.181 | 0.32 |
| Unit of Increase | OR | 95% CI | p | |
|---|---|---|---|---|
| eGFR | 1 mL/min/1.73 m2 | 0.90 | 0.84–0.96 | <0.0001 |
| Serum Phosphate | 1 mg/dL | 3.23 | 1.46–5.76 | 0.0001 |
| LVMi | 1 g/m2 | 1.04 | 1.01–1.06 | 0.0003 |
| Proteinuria | 100 mg/24 h | 3.37 | 1.51–6.04 | 0.002 |
| MBG | 1 nmoL/L | 2.38 | 1.10–5.12 | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bolignano, D.; Greco, M.; Presta, P.; Caglioti, A.; Carullo, N.; Zicarelli, M.; Foti, D.P.; Dragone, F.; Andreucci, M.; Coppolino, G. Marinobufagenin, Left Ventricular Hypertrophy and Residual Renal Function in Kidney Transplant Recipients. J. Clin. Med. 2023, 12, 3072. https://doi.org/10.3390/jcm12093072
Bolignano D, Greco M, Presta P, Caglioti A, Carullo N, Zicarelli M, Foti DP, Dragone F, Andreucci M, Coppolino G. Marinobufagenin, Left Ventricular Hypertrophy and Residual Renal Function in Kidney Transplant Recipients. Journal of Clinical Medicine. 2023; 12(9):3072. https://doi.org/10.3390/jcm12093072
Chicago/Turabian StyleBolignano, Davide, Marta Greco, Pierangela Presta, Alfredo Caglioti, Nazareno Carullo, Mariateresa Zicarelli, Daniela Patrizia Foti, Francesco Dragone, Michele Andreucci, and Giuseppe Coppolino. 2023. "Marinobufagenin, Left Ventricular Hypertrophy and Residual Renal Function in Kidney Transplant Recipients" Journal of Clinical Medicine 12, no. 9: 3072. https://doi.org/10.3390/jcm12093072