
Validation of “Neurit.Space”: Three Digital Tests for the Neuropsychological Evaluation of Unilateral Spatial Neglect
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
- (i)
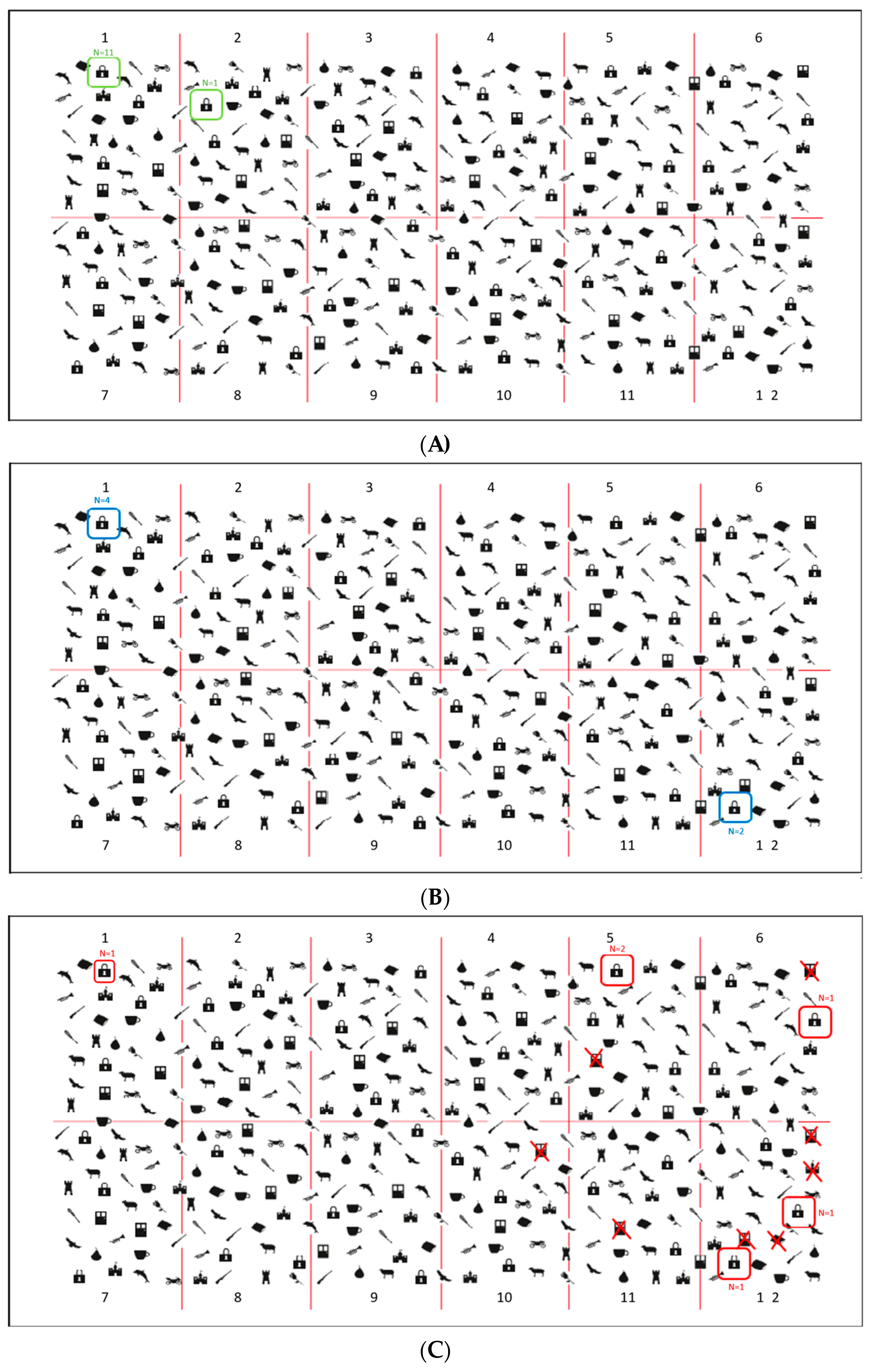
- Padlocks Cancellation Test (Figure 2A). Participants were asked to cross out all padlocks’ outlines presented on the surface of the screen among 336 distractors (i.e., outlines of doors and motorbikes). Stimuli were pseudo-randomly organized in twelve different quadrants: four on the left side, four in the middle and four on the right side of the screen. Targets and distractors were equally distributed in all of the 12 quadrants (each side of the screen contained 12 padlocks, for a total of 36 padlocks). Participants were asked to be as fast and accurate as possible and to communicate to the experimenter when they considered they had completed the task. The actual test was preceded by a practice trial with three targets and two distractors. Three different scores were assigned: (a) Total Accuracy Score (i.e., the number of targets correctly cancelled. Range: 0–36); (b) Asymmetry Score (i.e., the difference between the number of targets correctly marked in the left-hand side and the number of targets correctly marked in the right-hand side of the screen (+) and in the left one (range 0–±12); (c) Total Time to complete the test. Five other parameters were registered: (d) Time Imbalance, namely the amount of time spent on each side of the display (left vs. right); (e) Centre of Cancellation (CoC), namely: the centre of the participants’ marks in the x and y coordinates on the screen (Rorden and Karnath, 2010 [23]; Toraldo et al., 2017 [24] for a similar parameter); (f) Starting and Arrival Points, namely: the first and the last stimulus marked); (g) Errors other than omissions, such as commission errors, namely: false alarms, and perseveration, such as repeated marks and other gratuitous productions, not required by the task’s instructions (Rusconi et al. 2002 [22]). The exploration track was also available, and it could be further reviewed in a video movie action stored in the device.
- (ii)
- Digital Line Bisection Test (Figure 2B). Participants were asked to mark the mid-point of 4 red lines (25 cm in length) displaced horizontally in the centre of the screen. The test was preceded by two practice trials. The distance between the marked subjective mid-point and the objective mid-point of the line (negative values for left shifts from the mid-point and positive values for right shifts) is automatically computed and stored.
- (iii)
- Digital Five Elements Drawing Test (Figure 2C). Participants were asked to copy a complex figure at the top of the screen as accurately as possible, including five elements: two pine trees on the left-hand side, two bushes on the right-hand side and a church in the centre. The test was preceded by a practice trial in which participants were asked to make a free drawing (even a scribble) on a blank digital sheet to make them comfortable with the use of the electronic pen. The Total Time to complete the test and the Trajectory of drawings are recorded: participants’ performance can be further reviewed, sign-by-sign, in a video movie action. To provide a quantitative score of participants’ performances, a semi-automatic scoring procedure was used: omission errors were scored by the examiner as reported in [49]. For each element, 2 points were assigned for an errorless copy; 1.5 points for partial left/right-sided omissions, 1 point for complete left/right-sided omissions, 0.5 points for complete left/right-sided omissions and partial right/left-sided omissions and 0 points if no element was recognisable. The horizontal ground line was not considered for the scoring attribution.
2.3. Statistical Analyses
3. Results
3.1. Paper-and-Pencil Test vs. Neurit.Space
3.1.1. Healthy Participants
3.1.2. Patients with USN vs. Patients without USN
3.1.3. Patients vs. Healthy Participants
3.2. Further Analyses to Deepen the Padlock Cancellation Tests: New Parameters
3.2.1. Quantitative Parameters: Time Imbalance and Centre of Cancellation (CoC): Patients vs. Healthy Participants
Clinical Application of the New Quantitative Parameters: Patient #9
3.2.2. Qualitative Parameters: Starting Point and Other Errors: Patients vs. Healthy Participants
3.3. User Experience and Usability
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, P.; Ward, I.; Khan, U.; Liu, Y.; Hreha, K. Spatial neglect hinders success of inpatient rehabilitation in individuals with traumatic brain injury: A retrospective study. Neurorehabilit. Neural Repair 2016, 30, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Denes, G.; Semenza, C.; Stoppa, E.; Lis, A. Unilateral spatial neglect and recovery from hemiplegia: A follow-up study. Brain 1982, 105, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Ogden, J.A. Anterior-posterior interhemispheric differences in the loci of lesions producing visual hemineglect. Brain Cogn. 1985, 4, 59–75. [Google Scholar] [CrossRef] [PubMed]
- Vallar, G.; Perani, D. The anatomy of unilateral neglect after right-hemisphere stroke lesions. A clinical/CT-scan correlation study in man. Neuropsychologia 1986, 24, 609–622. [Google Scholar] [CrossRef]
- Bowen, A.; McKenna, K.; Tallis, R.C. Reasons for Variability in the Reported Rate of Occurrence of Unilateral Spatial Neglect After Stroke. Stroke 1999, 30, 1196–1202. [Google Scholar] [CrossRef]
- Corbetta, M.; Shulman, G.L. Spatial Neglect and Attention Networks. Annu. Rev. Neurosci. 2011, 34, 569–599. [Google Scholar] [CrossRef]
- Karnath, H.-O.; Rorden, C. The anatomy of spatial neglect. Neuropsychologia 2012, 50, 1010–1017. [Google Scholar] [CrossRef]
- Pierce, J.; Saj, A. A critical review of the role of impaired spatial remapping processes in spatial neglect. Clin. Neuropsychol. 2019, 33, 948–970. [Google Scholar] [CrossRef]
- Vallar, G. Spatial hemineglect in humans. Trends Cogn. Sci. 1998, 2, 87–97. [Google Scholar] [CrossRef]
- Vallar, G.; Calzolari, E. Unilateral spatial neglect after posterior parietal damage. Handb. Clin. Neurol. 2018, 151, 287–312. [Google Scholar] [CrossRef]
- Vuilleumier, P. Mapping the functional neuroanatomy of spatial neglect and human parietal lobe functions: Progress and challenges. Ann. N. Y. Acad. Sci. 2013, 1296, 50–74. [Google Scholar] [CrossRef] [PubMed]
- Azouvi, P. The ecological assessment of unilateral neglect. Ann. Phys. Rehabil. Med. 2017, 60, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Azouvi, P.; Samuel, C.; Louis-Dreyfus, A.; Bernati, T.; Bartolomeo, P.; Beis, J.M.; Chokron, S.; Leclercq, M.; Marchal, F.; Martin, Y. Sensitivity of clinical and behavioural tests of spatial neglect after right hemisphere stroke. J. Neurol. Neurosurg. Psychiatry 2002, 73, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Albert, M.L. A simple test of visual neglect. Neurology 1973, 23, 658–664. [Google Scholar] [CrossRef] [PubMed]
- Diller, L.; Weinberg, J. Hemi-inattention in rehabilitation: The evolution of a rational remediation program. Adv. Neurol. 1977, 18, 63–82. [Google Scholar] [PubMed]
- Gauthier, L.; Dehaut, F.; Joanette, Y. The bells test: A quantitative and qualitative test for visual neglect. Int. J. Clin. Neuropsychol. 1989, 11, 49–54. [Google Scholar]
- Bickerton, W.L.; Samson, D.; Williamson, J.; Humphreys, G.W. Separating forms of neglect using the Apples Test: Validation and functional prediction in chronic and acute stroke. Neuropsychology 2011, 25, 567–580. [Google Scholar] [CrossRef]
- Mancuso, M.; Rosadoni, S.; Capitani, D.; Bickerton, W.L.; Humphreys, G.W.; De Tanti, A.; Zampolini, M.; Galardi, G.; Caputo, M.; De Pellegrin, S.; et al. Italian standardization of the Apples Cancellation Test. Neurol. Sci. 2015, 36, 1233–1240. [Google Scholar] [CrossRef]
- Ota, H.; Fujii, T.; Suzuki, K.; Fukatsu, R.; Yamadori, A. Dissociation of body-centered and stimulus-centered representations in unilateral neglect. Neurology 2001, 57, 2064–2069. [Google Scholar] [CrossRef]
- Ota, H.; Fujii, T.; Tabuchi, M.; Sato, K.; Saito, J.; Yamadori, A. Different spatial processing for stimulus-centered and body-centered representations. Neurology 2003, 60, 1846–1848. [Google Scholar] [CrossRef]
- Ronchi, R.; Posteraro, L.; Fortis, P.; Bricolo, E.; Vallar, G. Perseveration in left spatial neglect: Drawing and cancellation tasks. Cortex 2009, 45, 300–312. [Google Scholar] [CrossRef] [PubMed]
- Rusconi, M.L.; Maravita, A.; Bottini, G.; Vallar, G. Is the intact side really intact? Perseverative responses in patients with unilateral neglect: A productive manifestation. Neuropsychologia 2002, 40, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Rorden, C.; Karnath, H.-O. A simple measure of neglect severity. Neuropsychologia 2010, 48, 2758–2763. [Google Scholar] [CrossRef] [PubMed]
- Toraldo, A.; Romaniello, C.; Sommaruga, P. Measuring and diagnosing unilateral neglect: A standardized statistical procedure. Clin. Neuropsychol. 2017, 31, 1248–1267. [Google Scholar] [CrossRef]
- Vallar, G.; Daini, R.; Antonucci, G. Processing of illusion of length in spatial hemineglect: A study of line bisection. Neuropsychologia 2000, 38, 1087–1097. [Google Scholar] [CrossRef]
- Bisiach, E.; Bulgarelli, C.; Sterzi, R.; Vallar, G. Line bisection and cognitive plasticity of unilateral neglect of space. Brain Cogn. 1983, 2, 32–38. [Google Scholar] [CrossRef]
- Schenkenberg, T.; Bradford, D.C.; Ajax, E.T. Line bisection and unilateral visual neglect in patients with neurologic impairment. Neurology 1980, 30, 509. [Google Scholar] [CrossRef]
- Gainotti, G.; Messerli, P.; Tissot, R. Qualitative analysis of unilateral spatial neglect in relation to laterality of cerebral lesions. J. Neurol. Neurosurg. Psychiatry 1972, 35, 545–550. [Google Scholar] [CrossRef]
- Bisiach, E.; Vallar, G. Unilateral neglect in humans. In Handbook of Neuropsychology; Boller, F., Grafman, J., Rizzolatti, G., Eds.; Elsevier Science Publishers: Amsterdam, The Netherlands, 2000; pp. 459–502. [Google Scholar]
- Rode, G.; Michel, C.; Rossetti, Y.; Boisson, D.; Vallar, G. Left size distortion (hyperschematia) after right brain damage. Neurology 2006, 67, 1801–1808. [Google Scholar] [CrossRef]
- Walker, R. Spatial and object-based neglect. Neurocase 1995, 1, 371–383. [Google Scholar] [CrossRef]
- Della Sala, S.; Beschin, N.; Cubelli, R. Persistent neglect in everyday life. Cortex J. Devoted Study Nerv. Syst. Behav. 2018, 103, 382–384. [Google Scholar] [CrossRef] [PubMed]
- Bonato, M.; Priftis, K.; Marenzi, R.; Umiltà, C.; Zorzi, M. Deficits of contralesional awareness: A case study on what paper-and-pencil tests neglect. Neuropsychology 2012, 26, 20–36. [Google Scholar] [CrossRef] [PubMed]
- Bonato, M.; Priftis, K.; Marenzi, R.; Umiltà, C.; Zorzi, M. Increased attentional demands impair contralesional space awareness following stroke. Neuropsychologia 2010, 48, 3934–3940. [Google Scholar] [CrossRef]
- Terruzzi, S.; Albini, F.; Massetti, G.; Etzi, R.; Gallace, A.; Vallar, G. The Neuropsychological Assessment of Unilateral Spatial Neglect through Computerized and Virtual Reality Tools: A Scoping Review. Neuropsychol. Rev. 2023, 1–39. [Google Scholar] [CrossRef]
- Deouell, L.Y.; Sacher, Y.; Soroker, N. Assessment of spatial tients with and without unilateral spatial neglect. Arch. Phys. 2005, 11, 697–707. [Google Scholar]
- Rabuffetti, M.; Ferrarin, M.; Spadone, R.; Pellegatta, D.; Gentileschi, V.; Vallar, G.; Pedotti, A. Touch-screen system for assessing visuo-motor exploratory skills in neuropsychological disorders of spatial cognition. Med. Biol. Eng. Comput. 2002, 40, 675–686. [Google Scholar] [CrossRef]
- Van der Stigchel, S.; Nijboer, T.C.W. The imbalance of oculomotor capture in unilateral visual neglect. Conscious. Cogn. 2010, 19, 186–197. [Google Scholar] [CrossRef]
- Esposito, E.; Shekhtman, G.; Chen, P. Prevalence of spatial neglect post-stroke: A systematic review. Ann. Phys. Rehabil. Med. 2021, 64, 101459. [Google Scholar] [CrossRef]
- Dozio, N.; Maggioni, E.; Pittera, D.; Gallace, A.; Obrist, M. May I smell your attention: Exploration of smell and sound for visuospatial attention in virtual reality. Front. Psychol. 2021, 12, 671470. [Google Scholar] [CrossRef]
- Frigione, I.; Massetti, G.; Girondini, M.; Etzi, R.; Scurati, G.W.; Ferrise, F.; Chirico, A.; Gaggioli, A.; Gallace, A. An Exploratory Study on the Effect of Virtual Environments on Cognitive Performances and Psychophysiological Responses. Cyberpsychology Behav. Soc. Netw. 2022, 25, 666–671. [Google Scholar] [CrossRef]
- Gallace, A. Haptic Interaction in Virtual Reality: Are We Ready for the Metaverse? Neuroscientific and Behavioral Considerations. In Handbook of Research on Implementing Digital Reality and Interactive Technologies to Achieve Society 5.0; IGI Global: Hershey, PA, USA, 2022; pp. 1–14. [Google Scholar]
- Johnson, E.; Anderson-Hanley, C.; Puleio, A.; Wall, K. A-82 Neuropsychological Assessment in the Age of Technology: Comparing Traditional Paper versus Electronic Administration. Arch. Clin. Neuropsychol. 2019, 34, 942. [Google Scholar] [CrossRef]
- Marin, J.O. Neuropsychological diagnostic accuracy: Factors that might lead to a wrong diagnosis and how to avoid them. Rev. Iberoam. Psicol. Cienc. Y Tecnol. 2019, 12, 29–38. [Google Scholar]
- Oldfield, R.C. The assessment and analysis of handedness: The Edinburgh inventory. Neuropsychologia 1971, 9, 97–113. [Google Scholar] [CrossRef] [PubMed]
- Magni, E.; Binetti, G.; Bianchetti, A.; Rozzini, R.; Trabucchi, M. Mini-Mental State Examination: A normative study in Italian elderly population. Eur. J. Neurol. 1996, 3, 198–202. [Google Scholar] [CrossRef]
- Basagni, B.; De Tanti, A.; Damora, A.; Abbruzzese, L.; Varalta, V.; Antonucci, G.; Bickerton, W.L.; Smania, N.; Mancuso, M. The assessment of hemineglect syndrome with cancellation tasks: A comparison between the Bells test and the Apples test. Neurol. Sci. 2017, 38, 2171–2176. [Google Scholar] [CrossRef]
- Gottesman, R.F.; Kleinman, J.T.; Davis, C.; Heidler-Gary, J.; Newhart, M.; Kannan, V.; Hillis, A.E. Unilateral neglect is more severe and common in older patients with right hemispheric stroke. Neurology 2008, 71, 1439–1444. [Google Scholar] [CrossRef]
- Mancini, F.; Bricolo, E.; Mattioli, F.C.; Vallar, G. Visuo-Haptic Interactions in Unilateral Spatial Neglect: The Cross Modal Judd Illusion. Front. Psychol. 2011, 2, 341. [Google Scholar] [CrossRef]
- Crawford, J.; Howell, D.C. Comparing an Individual’s Test Score against Norms Derived from Small Samples. Clin. Neuropsychol. 1998, 12, 482–486. [Google Scholar] [CrossRef]
- Brooke, J. SUS: A ‘Quick and Dirty’ Usability Scale. Usability Eval. Ind. 1996, 189, 4–7. [Google Scholar]
- Eccles, D.W.; Arsal, G. The think aloud method: What is it and how do I use it? Qual. Res. Sport Exerc. Health 2017, 9, 514–531. [Google Scholar] [CrossRef]
- Fonteyn, M.E.; Kuipers, B.; Grobe, S.J. A Description of Think Aloud Method and Protocol Analysis. Qual. Health Res. 1993, 3, 430–441. [Google Scholar] [CrossRef]
- Jaspers, M.W.M.; Steen, T.; Van Den Bos, C.; Geenen, M. The think aloud method: A guide to user interface design. Int. J. Med. Inform. 2004, 73, 781–795. [Google Scholar] [CrossRef]
- Tesio, L.; Scarano, S.; Hassan, S.; Kumbhare, D.; Caronni, A. Why Questionnaire Scores are not Measures: A question-raising article. Am. J. Phys. Med. Rehabil. 2023, 102, 75–82. [Google Scholar] [CrossRef]
- Liang, Y.; Fairhurst, M.C.; Guest, R.M.; Potter, J.M. A Learning Model for the Automated Assessment of Hand-Drawn Images for Visuo-Spatial Neglect Rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2010, 18, 560–570. [Google Scholar] [CrossRef] [PubMed]
- Ulm, L.; Wohlrapp, D.; Meinzer, M.; Steinicke, R.; Schatz, A.; Denzler, P.; Klehmet, J.; Dohle, C.; Niedeggen, M.; Meisel, A. A circle-monitor for computerized assessment of visual neglect in peripersonal space. PLoS ONE 2013, 8, e82892. [Google Scholar] [CrossRef] [PubMed]
- Bonato, M.; Priftis, K.; Umiltà, C.; Zorzi, M. Computer-based attention-demanding testing unveils severe neglect in apparently intact patients. Behav. Neurol. 2013, 26, 179–181. [Google Scholar] [CrossRef]
- Villarreal, S.; Linnavuo, M.; Sepponen, R.; Vuori, O.; Bonato, M.; Jokinen, H.; Hietanen, M. Unilateral Stroke: Computer-based Assessment Uncovers Non-Lateralized and Contralesional Visuoattentive Deficits. J. Int. Neuropsychol. Soc. 2021, 27, 959–969. [Google Scholar] [CrossRef]
- Villarreal, S.; Linnavuo, M.; Sepponen, R.; Vuori, O.; Jokinen, H.; Hietanen, M. Dual-Task in Large Perceptual Space Reveals Subclinical Hemispatial Neglect. J. Int. Neuropsychol. Soc. 2020, 26, 993–1005. [Google Scholar] [CrossRef]
- Ferber, S.; Karnath, H.-O. How to assess spatial neglect-line bisection or cancellation tasks? J. Clin. Exp. Neuropsychol. 2001, 23, 599–607. [Google Scholar] [CrossRef]
- Bailey, M.J.; Riddoch, M.J.; Crome, P. Test–retest stability of three tests for unilateral visual neglect in patients with stroke: Star Cancellation, Line Bisection, and the Baking Tray Task. Neuropsychol. Rehabil. 2004, 14, 403–419. [Google Scholar] [CrossRef]
- Azouvi, P.; Bartolomeo, P.; Beis, J.-M.; Perennou, D.; Pradat-Diehl, P.; Rousseaux, M. A battery of tests for the quantitative assessment of unilateral neglect. Restor. Neurol. Neurosci. 2006, 24, 273–285. [Google Scholar] [PubMed]
- Osaki, S.; Amimoto, K.; Miyazaki, Y.; Tanabe, J.; Yoshihiro, N. Investigating the Characteristics of Covert Unilateral Spatial Neglect Using the Modified Posner Task: A Single-subject Design Study. Prog. Rehabil. Med. 2021, 6, 20210014. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Fyffe, D.C.; Hreha, K. Informal caregivers’ burden and stress in caring for stroke survivors with spatial neglect: An exploratory mixed-method study. Top. Stroke Rehabil. 2017, 24, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Gillen, R.; Tennen, H.; McKee, T. Unilateral spatial neglect: Relation to rehabilitation outcomes in patients with right hemisphere stroke. Arch. Phys. Med. Rehabil. 2005, 86, 763–767. [Google Scholar] [CrossRef] [PubMed]
- Wee, J.Y.M.; Hopman, W.M. Comparing Consequences of Right and Left Unilateral Neglect in a Stroke Rehabilitation Population. Am. J. Phys. Med. Rehabil. 2008, 87, 910–920. [Google Scholar] [CrossRef] [PubMed]
- Gainotti, G.; Trojano, L. Constructional apraxia. Handb. Clin. Neurol. 2018, 151, 331–348. [Google Scholar] [PubMed]
- De Vet, H.C.; Terwee, C.B.; Ostelo, R.W.; Beckerman, H.; Knol, D.L.; Bouter, L.M. Minimal changes in health status questionnaires: Distinction between minimally detectable change and minimally important change. Health Qual Life Outcomes 2006, 4, 54–59. [Google Scholar] [CrossRef]
- Nobre, A.C.; Nobre, K.; Kastner, S. (Eds.) The Oxford Handbook of Attention; Oxford University Press: Oxford, UK, 2014. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | Sex/Age (Years)/Educational Level (Years) | Duration of the Disease (Days) | Lesion Site/Aetiology | Apples Cancellation Test | USN | ||
|---|---|---|---|---|---|---|---|
| Total Score | Egocentric Score | Allocentric Score | |||||
| 1 | F/53/13 | 48 | R Cn/CVA-H | + | + | − | + |
| 2 | F/83/5 | 19 | R P-T-In/CVA-I | + | + | + | + |
| 3 | F/80/13 | 12 | R F-In/CVA-I | + | + | − | + |
| 4 | F/72/18 | 171 | R Th/CVA-H | + | + | − | + |
| 5 | M/80/13 | 166 | R F-In-T/CVA-I | + | − | + | + |
| 6 | F/83/18 | 67 | R T-P/CVA-I | + | + | − | + |
| 7 | F/65/8 | 31 | Ic-Cn/CVA-I | + | − | − | − |
| 8 | M/48/13 | 2235 | R T-O/CVA-H | − | − | − | − |
| 9 | F/59/16 | 133 | R F-T-P/CVA-H | − | − | − | − |
| 10 | M/39/11 | 45 | R Ic/CVA-H | − | − | − | − |
| 11 | F/70/17 | 23 | R F/CVA-H | − | − | − | − |
| 12 | M/72/18 | 39 | R M/CVA-I | − | − | − | − |
| Healthy Participants | N+ | N− | |
|---|---|---|---|
| Paper-and-Pencil | |||
| 10 ± 0.00 | 7 ± 4.28 | 10 ± 0.00 |
| 93.08 ± 7.35 | 56.76 ± 29.97 | 96.57 ± 2.39 |
| 11.85 ± 1.45 | 15.22 ± 3.40 | 12.84 ± 0.60 |
| Neurit.Space | |||
| 9.87 ± 0.25 | 5.41 ± 3.74 | 9.66 ± 0.25 |
| 96.99 ± 2.2 | 56.63 ± 33.96 | 94.9 ± 5.39 |
| 12.39 ± 0.32 | 15.05 ± 2.71 | 12.65 ± 0.49 |
| Healthy Participants | N+ | N− | |
|---|---|---|---|
| Neurit.Space | |||
| 8.57 ± 11.53 | −56.46 ± 43.2 | 9.23 ± 20.85 |
| 49.51 ± 1.09 | 67.91 ± 19.02 | 50.81 ± 2.25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Massetti, G.; Albini, F.; Casati, C.; Toneatto, C.; Terruzzi, S.; Etzi, R.; Tesio, L.; Gallace, A.; Vallar, G. Validation of “Neurit.Space”: Three Digital Tests for the Neuropsychological Evaluation of Unilateral Spatial Neglect. J. Clin. Med. 2023, 12, 3042. https://doi.org/10.3390/jcm12083042
Massetti G, Albini F, Casati C, Toneatto C, Terruzzi S, Etzi R, Tesio L, Gallace A, Vallar G. Validation of “Neurit.Space”: Three Digital Tests for the Neuropsychological Evaluation of Unilateral Spatial Neglect. Journal of Clinical Medicine. 2023; 12(8):3042. https://doi.org/10.3390/jcm12083042
Chicago/Turabian StyleMassetti, Gemma, Federica Albini, Carlotta Casati, Carlo Toneatto, Stefano Terruzzi, Roberta Etzi, Luigi Tesio, Alberto Gallace, and Giuseppe Vallar. 2023. "Validation of “Neurit.Space”: Three Digital Tests for the Neuropsychological Evaluation of Unilateral Spatial Neglect" Journal of Clinical Medicine 12, no. 8: 3042. https://doi.org/10.3390/jcm12083042