
The Interaction Effect of Anti-RgpA and Anti-PPAD Antibody Titers: An Indicator for Rheumatoid Arthritis Diagnosis
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
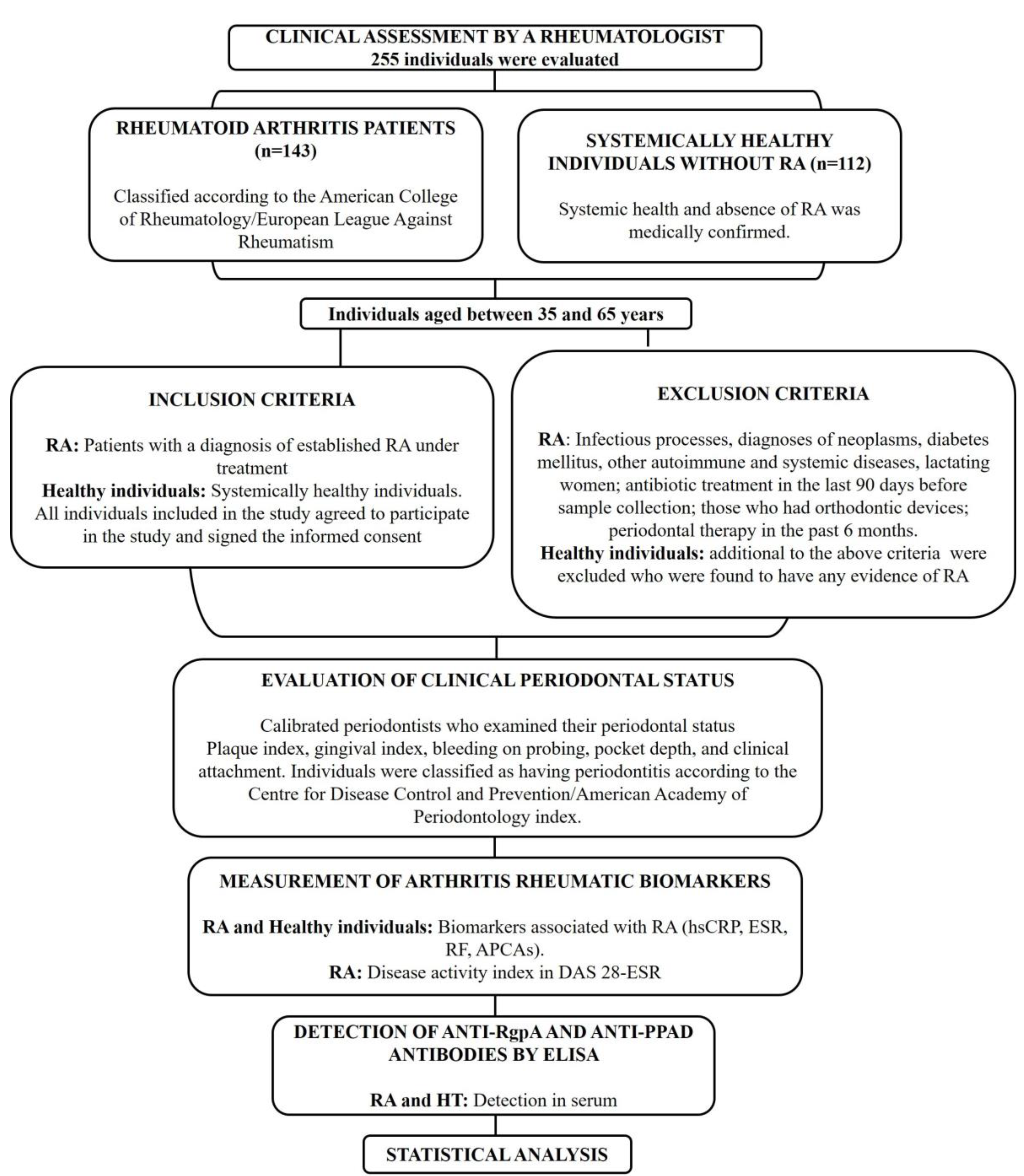
2.1. Type of Study
2.2. Population and Sample
2.3. Inclusion Criteria for RA Individuals and Controls
2.4. Exclusion Criteria
2.5. Evaluation of Clinical Periodontal Status
2.6. Identification and Quantification of P. gingivalis in Subgingival Plaque
2.7. Measurement of Arthritis Rheumatic Biomarkers
2.8. Detection of Anti-RgpA and Anti-PPAD Antibodies by ELISA
2.8.1. Purification of Native RgpA
2.8.2. Recombinant PPAD Production
2.8.3. Indirect ELISA
2.9. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cush, J.J. Rheumatoid Arthritis: Early Diagnosis and Treatment. Med. Clin. N. Am. 2021, 105, 355–365. [Google Scholar] [CrossRef]
- Darrah, E.; Andrade, F. Rheumatoid arthritis and citrullination. Curr. Opin. Rheumatol. 2018, 30, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Ciesielski, O.; Biesiekierska, M.; Panthu, B.; Soszyński, M.; Pirola, L.; Balcerczyk, A. Citrullination in the pathology of inflammatory and autoimmune disorders: Recent advances and future perspectives. Cell. Mol. Life Sci. 2022, 79, 94. [Google Scholar] [CrossRef] [PubMed]
- Yuzhalin, A.E. Citrullination in Cancer. Cancer Res. 2019, 79, 1274–1284. [Google Scholar] [CrossRef]
- Witalison, E.E.; Thompson, P.R.; Hofseth, L.J. Protein Arginine Deiminases and Associated Citrullination: Physiological Functions and Diseases Associated with Dysregulation. Curr. Drug Targets 2015, 16, 700–710. [Google Scholar] [CrossRef]
- Vossenaar, E.R.; Radstake, T.R.; van der Heijden, A.; van Mansum, M.A.; Dieteren, C.; de Rooij, D.J.; Barrera, P.; Zendman, A.J.; van Venrooij, W.J. Expression and activity of citrullinating peptidylarginine deiminase enzymes in monocytes and macrophages. Ann. Rheum. Dis. 2004, 63, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Derksen, V.; Huizinga, T.; van der Woude, D. The role of autoantibodies in the pathophysiology of rheumatoid arthritis. Semin. Immunopathol. 2017, 39, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Potempa, J.; Sroka, A.; Imamura, T.; Travis, J. Gingipains, the major cysteine proteinases and virulence factors of Porphyromonas gingivalis: Structure, function and assembly of multidomain protein complexes. Curr. Protein Pept. Sci. 2003, 4, 397–407. [Google Scholar] [CrossRef]
- Smalley, J.W.; Olczak, T. Heme acquisition mechanisms of Porphyromonas gingivalis—Strategies used in a polymicrobial community in a heme-limited host environment. Mol. Oral Microbiol. 2017, 32, 1–23. [Google Scholar] [CrossRef]
- Laugisch, O.; Wong, A.; Sroka, A.; Kantyka, T.; Koziel, J.; Neuhaus, K.; Sculean, A.; Venables, P.J.; Potempa, J.; Möller, B.; et al. Citrullination in the periodontium—A possible link between periodontitis and rheumatoid arthritis. Clin. Oral Investig. 2016, 20, 675–683. [Google Scholar] [CrossRef]
- Olsen, I.; Singhrao, S.K.; Potempa, J. Citrullination as a plausible link to periodontitis, rheumatoid arthritis, atherosclerosis and Alzheimer′s disease. J. Oral Microbiol. 2018, 10, 1487742. [Google Scholar] [CrossRef] [PubMed]
- Wegner, N.; Wait, R.; Sroka, A.; Eick, S.; Nguyen, K.A.; Lundberg, K.; Kinloch, A.; Culshaw, S.; Potempa, J.; Venables, P.J. Peptidylarginine deiminase from Porphyromonas gingivalis citrullinates human fibrinogen and α-enolase: Implications for autoimmunity in rheumatoid arthritis. Arthritis Rheum. 2010, 62, 2662–2672. [Google Scholar] [CrossRef] [PubMed]
- Qiao, Y.; Wang, Z.; Li, Y.; Han, Y.; Zhou, Y.; Cao, X. Rheumatoid arthritis risk in periodontitis patients: A systematic review and meta-analysis. Jt. Bone Spine 2020, 87, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Bender, P.; Bürgin, W.B.; Sculean, A.; Eick, S. Serum antibody levels against Porphyromonas gingivalis in patients with and without rheumatoid arthritis—A systematic review and meta-analysis. Clin. Oral Investig. 2017, 2, 33–42. [Google Scholar] [CrossRef]
- Unriza-Puin, S.; Bautista-Molano, W.; Lafaurie, G.I.; Valle-Oñate, R.; Chalem, P.; Chila-Moreno, L.; Bello-Gualtero, J.M.; Romero-Sánchez, C. Are obesity, ACPAs and periodontitis conditions that influence the risk of developing rheumatoid arthritis in first-degree relatives? Clin. Rheumatol. 2017, 36, 799–806. [Google Scholar] [CrossRef]
- Johansson, L.; Sherina, N.; Kharlamova, N.; Potempa, B.; Larsson, B.; Israelsson, L.; Potempa, J.; Rantapää-Dahlqvist, S.; Lundberg, K. Concentration of antibodies against Porphyromonas gingivalis is increased before the onset of symptoms of rheumatoid arthritis. Arthritis Res. Ther. 2016, 18, 201. [Google Scholar] [CrossRef]
- Bello-Gualtero, J.M.; Lafaurie, G.I.; Hoyos, L.X.; Castillo, D.M.; De-Avila, J.; Munevar, J.C.; Unriza, S.; Londoño, J.; Valle-Oñate, R.; Romero-Sánchez, C. Periodontal Disease in Individuals with a Genetic Risk of Developing Arthritis and Early Rheumatoid Arthritis: A Cross-Sectional Study. J. Periodontol. 2016, 87, 346–356. [Google Scholar] [CrossRef]
- Quirke, A.M.; Lugli, E.B.; Wegner, N.; Hamilton, B.C.; Charles, P.; Chowdhury, M.; Ytterberg, A.J.; Zubarev, R.A.; Potempa, J.; Culshaw, S.; et al. Heightened immune response to autocitrullinated Porphyromonas gingivalis peptidylarginine deiminase: A potential mechanism for breaching immunologic tolerance in rheumatoid arthritis. Ann. Rheum. Dis. 2014, 73, 263–269. [Google Scholar] [CrossRef]
- Montgomery, A.B.; Kopec, J.; Shrestha, L.; Thezenas, M.L.; Burgess-Brown, N.A.; Fischer, R.; Yue, W.W.; Venables, P.J. Crystal structure of Porphyromonas gingivalis peptidylarginine deiminase: Implications for autoimmunity in rheumatoid arthritis. Ann. Rheum. Dis. 2016, 75, 1255–1261. [Google Scholar] [CrossRef]
- Konig, M.F.; Paracha, A.S.; Moni, M.; Bingham, C.O., 3rd; Andrade, F. Defining the role of Porphyromonas gingivalis peptidylarginine deiminase (PPAD) in rheumatoid arthritis through the study of PPAD biology. Ann. Rheum. Dis. 2015, 74, 2054–2061. [Google Scholar] [CrossRef]
- Fisher, B.A.; Cartwright, A.J.; Quirke, A.M.; de Pablo, P.; Romaguera, D.; Panico, S.; Mattiello, A.; Gavrila, D.; Navarro, C.; Sacerdote, C.; et al. Smoking, Porphyromonas gingivalis and the immune response to citrullinated autoantigens before the clinical onset of rheumatoid arthritis in a Southern European nested case-control study. MC Musculoskelet. Disord. 2015, 16, 331. [Google Scholar] [CrossRef]
- Wilensky, A.; Polak, D.; Houri-Haddad, Y.; Shapira, L. The role of RgpA in the pathogenicity of Porphyromonas gingivalis in the murine periodontitis model. J. Clin. Periodontol. 2013, 40, 924–932. [Google Scholar] [CrossRef] [PubMed]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef] [PubMed]
- Page, R.C.; Eke, P.I. Case Definitions for Use in Population-Based Surveillance of Periodontitis. J. Periodontol. 2007, 78 (Suppl. 7S), 1387–1399. [Google Scholar] [CrossRef] [PubMed]
- Eke, P.I.; Page, R.C.; Wei, L.; Thornton-Evans, G.; Genco, R.J. Update of the case definitions for population-based surveillance of periodontitis. J. Periodontol. 2012, 83, 1449–1454. [Google Scholar] [CrossRef]
- Boutaga, K.; van Winkelhoff, A.J.; Vandenbroucke-Grauls, C.M.; Savelkoul, P.H. Comparison of real-time PCR and culture for detection of Porphyromonas gingivalis in subgingival plaque samples. J. Clin. Microbiol. 2003, 41, 4950–4954. [Google Scholar] [CrossRef] [PubMed]
- Fransen, J.; Stucki, G.; van Riel, P.L.C.M. Rheumatoid arthritis measures: Disease Activity Score (DAS), Disease Activity Score-28 (DAS28), Rapid Assessment of Disease Activity in Rheumatology (RADAR), and Rheumatoid Arthritis Disease Activity Index (RADAI). Arthritis Rheum. 2003, 49, S214–S224. [Google Scholar] [CrossRef]
- Furuta, N.; Takeuchi, H.; Amano, A. Entry of Porphyromonas gingivalis outer membrane vesicles into epithelial cells causes cellular functional impairment. Infect. Immun. 2009, 77, 4761–4770. [Google Scholar] [CrossRef]
- Castillo, Y.; Castellanos, J.E.; Lafaurie, G.I.; Castillo, D.M. Porphyromonas gingivalis outer membrane vesicles modulate cytokine and chemokine production by gingipain-dependent mechanisms in human macrophages. Arch. Oral Biol. 2022, 140, 105453. [Google Scholar] [CrossRef]
- Castillo, D.M.; Castillo, Y.; Delgadillo, N.A.; Neuta, Y.; Lafaurie, G.I.; Romero-Sánchez, C.; Castellanos, J.E. Purification of RgpA from external outer membrane vesicles of Porphyromonas gingivalis. Anaerobe 2022, 77, 102647. [Google Scholar] [CrossRef]
- Moses, T.; Holland, P.W. A comparison of statistical selection strategies for univariate and bivariate log-linear models. Br. J. Math. Stat. Psychol. 2010, 63, 557–574. [Google Scholar] [CrossRef] [PubMed]
- Rovas, A.; Puriene, A.; Punceviciene, E.; Butrimiene, I.; Stuopelyte, K.; Jarmalaite, S. Associations of periodontal status in periodontitis and rheumatoid arthritis patients. J. Periodontal. Implant. Sci. 2021, 51, 124–134. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, K.; Fei, G.; Lundmark, A.; Benchimol, D.; Lee, L.; Hu, Y.O.O.; Kats, A.; Saevarsdottir, S.; Catrina, A.I.; Klinge, B.; et al. Periodontal Health and Oral Microbiota in Patients with Rheumatoid Arthritis. J. Clin. Med. 2019, 8, 630. [Google Scholar] [CrossRef] [PubMed]
- Loutan, L.; Alpizar-Rodriguez, D.; Courvoisier, D.S.; Finckh, A.; Mombelli, A.; Giannopoulou, C. Periodontal status correlates with anti-citrullinated protein antibodies in first-degree relatives of individuals with rheumatoid arthritis. J. Clin. Periodontol. Schmickler. 2019, 46, 690–698. [Google Scholar] [CrossRef] [PubMed]
- Schmickler, J.; Rupprecht, A.; Patschan, S.; Patschan, D.; Müller, G.A.; Haak, R.; Mausberg, R.F.; Schmalz, G.; Kottmann, T.; Ziebolz, D. Cross-Sectional Evaluation of Periodontal Status and Microbiologic and Rheumatoid Parameters in a Large Cohort of Patients with Rheumatoid Arthritis. J. Periodontol. 2017, 88, 368–379. [Google Scholar] [CrossRef]
- Mikuls, T.R.; Payne, J.B.; Yu, F.; Thiele, G.M.; Reynolds, R.J.; Cannon, G.W.; Markt, J.; McGowan, D.; Kerr, G.S.; Redman, R.S.; et al. Periodontitis and Porphyromonas gingivalis in patients with rheumatoid arthritis. Arthritis Rheumatol. 2014, 66, 1090–1100. [Google Scholar] [CrossRef]
- Posada-López, A.; Botero, J.E.; Pineda-Tamayo, R.A.; Agudelo-Suárez, A.A. The Effect of Periodontal Treatment on Clinical and Biological Indicators, Quality of Life, and Oral Health in Rheumatoid Arthritis Patients: A Quasi-Experimental Study. Int. J. Environ. Res. Public Health 2022, 19, 1789. [Google Scholar] [CrossRef]
- Sun, J.; Zheng, Y.; Bian, X.; Ge, H.; Wang, J.; Zhang, Z. Non-surgical periodontal treatment improves rheumatoid arthritis disease activity: A meta-analysis. Clin. Oral Investig. 2021, 25, 4975–4985. [Google Scholar] [CrossRef]
- Shimada, A.; Kobayashi, T.; Ito, S.; Okada, M.; Murasawa, A.; Nakazono, K.; Yoshie, H. Expression of anti-Porphyromonas gingivalis peptidylarginine deiminase immunoglobulin G and peptidylarginine deiminase-4 in patients with rheumatoid arthritis and periodontitis. J. Periodontal. Res. 2016, 51, 103–111. [Google Scholar] [CrossRef]
- Maresz, K.J.; Hellvard, A.; Sroka, A.; Adamowicz, K.; Bielecka, E.; Koziel, J.; Gawron, K.; Mizgalska, D.; Marcinska, K.A.; Benedyk, M.; et al. Porphyromonas gingivalis facilitates the development and progression of destructive arthritis through its unique bacterial peptidylarginine deiminase (PAD). PLoS Pathog. 2013, 9, e1003627. [Google Scholar] [CrossRef]
- Gabarrini, G.; Chlebowicz, M.A.; Vega-Quiroz, M.E.; Veloo, A.C.M.; Rossen, J.W.A.; Harmsen, H.J.M.; Laine, M.L.; van Dijl, J.M.; van Winkelhoff, A.J. Conserved Citrullinating Exoenzymes in Porphyromonas Species. J. Dent. Res. 2018, 97, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Hedström, A.K.; Stawiarz, L.; Klareskog, L.; Alfredsson, L. Smoking and susceptibility to rheumatoid arthritis in a Swedish population-based case-control study. Eur. J. Epidemiol. 2018, 33, 415–423. [Google Scholar] [CrossRef]
- Rahajoe, P.S.; de Smit, M.; Schuurmans, G.; Raveling-Eelsing, E.; Kertia, N.; Vissink, A.; Westra, J. Increased IgA anti-citrullinated protein antibodies in the periodontal inflammatory exudate of healthy individuals compared to rheumatoid arthritis patients. J. Clin. Periodontol. 2020, 47, 552–560. [Google Scholar] [CrossRef]
- Rodríguez, J.; Lafaurie, G.I.; Bautista-Molano, W.; Chila-Moreno, L.; Bello-Gualtero, J.M.; Romero-Sánchez, C. Adipokines and periodontal markers as risk indicators of early rheumatoid arthritis: A cross-sectional study. Clin. Oral Investig. 2021, 25, 1685–1695. [Google Scholar] [CrossRef] [PubMed]
- Chaparro-Sanabria, J.A.; Bautista-Molano, W.; Bello-Gualtero, J.M.; Chila-Moreno, L.; Castillo, D.M.; Valle-Oñate, R.; Chalem, P.; Romero-Sánchez, C. Association of adipokines with rheumatic disease activity indexes and periodontal disease in patients with early rheumatoid arthritis and their first-degree relatives. Int. J. Rheum. Dis. 2019, 22, 1990–2000. [Google Scholar] [CrossRef] [PubMed]
- Qin, B.; Yang, M.; Fu, H.; Ma, N.; Wei, T.; Tang, Q.; Hu, Z.; Liang, Y.; Yang, Z.; Zhong, R. Body mass index and the risk of rheumatoid arthritis: A systematic review and dose-response meta-analysis. Arthritis Res. Ther. 2015, 17, 86. [Google Scholar] [CrossRef]
- Schmalz, G.; Noack, S.; Patschan, S.; Patschan, D.; Müller, G.A.; Rupprecht, A.; Schmickler, J.; Haak, R.; Ziebolz, D. Disease activity, morning stiffness and missing teeth are associated with oral health-related quality of life in individuals with rheumatoid arthritis. Clin. Oral Investig. 2020, 24, 3559–3566. [Google Scholar] [CrossRef]
- Arévalo-Caro, C.; Romero-Sánchez, C.; Garavito-Rodríguez, E. Relation between anti-Porphyromonas gingivalis antibody titers and HLA-DRB1 neutral alleles in individuals with rheumatoid arthritis. Acta Odontol. Scand. 2022, 80, 131–139. [Google Scholar] [CrossRef]
- Bae, S.C.; Lee, Y.H. Association between anti-Porphyromonas gingivalis antibody, anti-citrullinated protein antibodies, and rheumatoid arthritis: A meta-analysis. Z. Rheumatol. 2018, 77, 522–532. [Google Scholar] [CrossRef]
- Okada, M.; Kobayashi, T.; Ito, S.; Yokoyama, T.; Komatsu, Y.; Abe, A.; Murasawa, A.; Yoshie, H. Antibody responses to periodontopathic bacteria in relation to rheumatoid arthritis in Japanese adults. J. Periodontol. 2011, 82, 1433–1441. [Google Scholar] [CrossRef]
- Hitchon, C.A.; Chandad, F.; Ferucci, E.D.; Willemze, A.; Ioan-Facsinay, A.; van der Woude, D.; Markland, J.; Robinson, D.; Elias, B.; Newkirk, M.; et al. Antibodies to Porphyromonas gingivalis are associated with anticitrullinated protein antibodies in patients with rheumatoid arthritis and their relatives. J. Rheumatol. 2010, 37, 1105–1112. [Google Scholar] [CrossRef] [PubMed]
- De Smit, M.; van de Stadt, L.A.; Janssen, K.M.; Doornbos-van der Meer, B.; Vissink, A.; van Winkelhoff, A.J.; Brouwer, E.; Westra, J.; van Schaardenburg, D. Antibodies against Porphyromonas gingivalis in seropositive arthralgia patients do not predict development of rheumatoid arthritis. Ann. Rheum. Dis. 2014, 73, 1277–1279. [Google Scholar] [CrossRef]
- Romero-Sanchez, C.; Rodríguez, C.; Santos-Moreno, P.; Mesa, A.M.; Lafaurie, G.I.; Giraldo, Q.S.; De-Avila, J.; Castillo, D.M.; Duran, M.; Chalem, P.C.; et al. Is the Treatment with Biological or Non-biological DMARDS a Modifier of Periodontal Condition in Patients with Rheumatoid Arthritis? Curr. Rheumatol. Rev. 2017, 13, 139–151. [Google Scholar] [CrossRef] [PubMed]
- Heredia, P.A.M.; Lafaurie, G.I.; Bautista-Molano, W.; Trujillo, T.G.; Chalem-Choueka, P.; Bello-Gualtero, J.M.; Pacheco-Tena, C.; Chila-Moreno, L.; Romero-Sánchez, C. Predictive factors related to the progression of periodontal disease in patients with early rheumatoid arthritis: A cohort study. BMC Oral Health 2019, 19, 240. [Google Scholar] [CrossRef] [PubMed]
- Xiao, L.; Zhang, Q.; Peng, Y.; Wang, D.; Liu, Y. The effect of periodontal bacteria infection on incidence and prognosis of cancer: A systematic review and meta-analysis. Medicine 2020, 99, e19698. [Google Scholar] [CrossRef] [PubMed]
- Jasemi, S.; Erre, G.L.; Cadoni, M.L.; Bo, M.; Sechi, L.A. Humoral Response to Microbial Biomarkers in Rheumatoid Arthritis Patients. J. Clin. Med. 2021, 10, 5153. [Google Scholar] [CrossRef]
- Moen, K.; Brun, J.G.; Madland, T.M.; Tynning, T.; Jonsson, R. Immunoglobulin G and A antibody responses to Bacteroides forsythus and Prevotella intermedia in sera and synovial fluids of arthritis patients. Clin. Diagn. Lab. Immunol. 2003, 10, 1043–1050. [Google Scholar] [PubMed]
- Ingalagi, P.; Bhat, K.G.; Kulkarni, R.D.; Kotrashetti, V.S.; Kumbar, V.; Kugaji, M. Detection and comparison of prevalence of Porphyromonas gingivalis through culture and Real Time-polymerase chain reaction in subgingival plaque samples of chronic periodontitis and healthy individuals. J. Oral Maxillofac. Pathol. 2022, 26, 288. [Google Scholar]
- Simulen, J.S.; Aletaha, D.; McInnes, I.B. Rheumatoid arthritis. Lancet 2016, 388, 2023–2038. [Google Scholar] [CrossRef]
- Li, Y.; Guo, R.; Oduro, P.K.; Sun, T.; Chen, H.; Yi, Y.; Zeng, W.; Wang, Q.; Leng, L.; Yang, L.; et al. The Relationship Between Porphyromonas gingivalis and Rheumatoid Arthritis: A Meta-Analysis. Front. Cell. Infect. Microbiol. 2022, 12, 956417. [Google Scholar] [CrossRef]
- Potempa, J.; Nguyen, K.A. Purification and characterization of gingipains. Curr. Protoc. Protein Sci. 2007, 49, 21.20.1–21.20.27. [Google Scholar] [CrossRef] [PubMed]
- Kharlamova, N.; Jiang, X.; Sherina, N.; Potempa, B.; Israelsson, L.; Quirke, A.M.; Eriksson, K.; Yucel-Lindberg, T.; Venables, P.J.; Potempa, J.; et al. Antibodies to Porphyromonas gingivalis Indicate Interaction Between Oral Infection, Smoking, and Risk Genes in Rheumatoid Arthritis Etiology. Arthritis Rheumatol. 2016, 68, 604–613. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Atienza, E.; Flak, M.B.; Sirr, J.; Paramonov, N.A.; Aduse-Opoku, J.; Pitzalis, C.; Curtis, M.A. The P. gingivalis Autocitrullinome Is Not a Target for ACPA in Early Rheumatoid Arthritis. J. Dent. Res. 2020, 99, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Dye, B.A. Global periodontal disease epidemiology. Periodontol. 2000 2012, 58, 10–25. [Google Scholar] [CrossRef]
- Serrano, C.; Suarez, E. Prevalence of Severe Periodontitis in a Colombian Adult Population. J. Int. Acad. Periodontol. 2019, 21, 53–62. [Google Scholar]



{kind=link}
{kind=link}
| Variable | RA n = 143 | Control n = 112 | p-Value |
|---|---|---|---|
| Age | <0.0001 | ||
| Median (IQR) | 57 (51–61) | 46 (39–53) | |
| Gender F (%) | 0.039 | ||
| Female | 125 (87.4) | 87 (77.7) | |
| Male | 18 (12.6) | 25 (22.3) | |
| BMI F (%) | 0.230 | ||
| Normal | 73 (51.0) | 66 (58.9) | |
| Overweight | 53 (37.5) | 39 (34.8) | |
| Obesity | 17 (11.9) | 7 (6.3) | |
| Habit smoker F (%) | 0.330 | ||
| Yes | 5 (3.5) | 7 (6.3) | |
| No | 138 (96.5) | 105 (93.7) | |
| ACPAs F (%) | <0.0001 | ||
| <20 U | 25 (17.5) | 106 (95.5) | |
| 20–40 U | 5 (3.5) | 5 (4.5) | |
| >40 U | 113(79) | 0 (0) | |
| ESR F (%) | 0.004 | ||
| <20 mm/h | 80 (55.9) | 82 (73.2) | |
| ≥20 mm/h | 63 (44.1) | 30 (26.8) | |
| hsCRP F (%) | <0.0001 | ||
| Normal | 23 (31.1) | 44 (59.5) | |
| >3 mg/L | 17 (23) | 20 (27.0) | |
| >10 mg/L | 34 (46) | 10 (13.5) | |
| RF F (%) | <0.0001 | ||
| <20 IU/mL | 19 (25.7) | 68 (91.9) | |
| 20–59 IU/mL | 19 (25.7) | 6 (8.1) | |
| >59 IU/mL | 36 (48.6) | 0 (0) | |
| DAS28-hsCRP | |||
| Median RIQ | 2.65 (2.2–3.4) | NA | |
| RA activity F (%) | NA | ||
| Without activity | 71 (46.65) | ||
| Low activity | 25 (17.48) | ||
| Moderate activity | 41 (28.67) | ||
| High activity | 6 (4.19) | ||
| Medication F (%) | 112 (100) | <0.0001 | |
| None | 2 (1.4) | ||
| Conventional | 110 (76.9) | ||
| Biological | 31 (21.6) | ||
| Diagnosis time of RA F (%) | NA | ||
| 2–5 years | 10 (7) | ||
| 5–10 years | 64 (45) | ||
| >10 years | 69 (48) |
| Variable | RA n = 143 | Control n = 112 | p-Value |
|---|---|---|---|
| Periodontitis F (%) | 0.106 | ||
| Presence | 119 (83.2) | 84 (75) | |
| Absence | 24 (16.8) | 28 (25) | |
| Severity F (%) | 0.001 | ||
| None | 24 (16.8) | 28 (25) | |
| Low | 1 (0.7) | 18 (16.1) | |
| Mild | 105 (73.4) | 54 (48.2) | |
| Severe | 13 (9.1) | 12 (10.7) | |
| Number of Teeth | <0.0001 | ||
| Median | 20 | 25 | |
| (IQR) | (13–25) | (21–28) | |
| Plaque Index% | 0.023 | ||
| Median | 68 | 52.5 | |
| (IQR) | (35–85) | (35–69) | |
| Gingival Index% | 0.117 | ||
| Median | 50 | 32 | |
| (IQR) | (10–73) | (17.5–63) | |
| Bleeding on probing (%) | 0.381 | ||
| Median | 47 | 40 | |
| (IQR) | (27–63) | (27–54) | |
| Pocket Depth (mm) | <0.0001 | ||
| Median | 4 | 4 | |
| (IQR) | (0–4.2) | (4–4.3) | |
| Pocket Depth (%) | 0.342 | ||
| Median | 25.3 | 24.54 | |
| (IQR) | (23–40) | (10–39.7) | |
| CAL (mm) | 0.0002 | ||
| Median | 2.74 | 2.38 | |
| (IQR) | (2.26–3.39) | (1.94–2.95) | |
| CAL > 5 mm (%) | <0.0001 | ||
| Median | 87 | 51.6 | |
| (IQR) | (60.7–97.7) | (34.6–77.1) | |
| P. gingivalis F (%) | 0.287 | ||
| Presence | 67 (46.9) | 60 (53.6) | |
| Absence | 76 (53.1) | 52 (46.4) | |
| P. gingivalis Log10 | 0.491 | ||
| Median | 0 | 4.14 | |
| (IQR) | (0–6.3) | (0–6.3) | |
| Anti-RgpA Q1 F (%) | <0.0001 | ||
| Positive + | 88 (61.5) | 39 (34.8) | |
| Negative − | 55 (38.4) | 73 (65.2) | |
| Anti-RgpA Q2 F (%) | <0.0001 | ||
| Positive + | 45 (31.5) | 15 (13.4) | |
| Negative − | 98 (68.5) | 97 (86.4) | |
| Anti-PPAD Q1 F (%) | 0.059 | ||
| Positive + | 84 (59) | 53 (42) | |
| Negative − | 59 (41) | 59 (58) | |
| Anti-PPAD Q2 F (%) | 0.236 | ||
| Positive + | 54 (37.7) | 35 (32.3) | |
| Negative − | 89 (62.3) | 77 (77.7) | |
| Anti-RgpAQ1-PPADQ1 | 0.026 | ||
| Positive + | 33 (23.1) | 8 (7.2) | |
| Negative − | 110 (76.9) | 104 (92.8) | |
| Anti-RgpAQ1-PPADQ2 | <0.0001 | ||
| Positive + | 18 (12.5) | 6 (5) | |
| Negative − | 125 (87.4) | 106 (95) |
| Variable | Anti-RgpA Q2 | Anti-RgpA Q1 | Anti-PPAD Q2 | Anti-PPAD Q1 | Anti-PPADQ2RgpA Q1 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Positive | Negative | Positive | Negative | Positive | Negative | Positive | Negative | Positive | Negative | |
| A. RA markers | ||||||||||
| ACPAs F (%) | ||||||||||
| <20 U | 51 (39) | 80 (61) | 23 (18) | 108(82) | 64 (49) | 67 (51) | 39 (30) | 92 (70) | 14 (35) | 117 (55) |
| 20–40 U | 4 (40) | 6 (60) | 2 (20) | 8 (80) | 4 (40) | 6 (60) | 2 (20) | 8 (80) | 1 (25) | 9 (4) |
| >40 U | 71 (63) † | 42 (37) | 35 (31) | 78 (69) | 68 (69) | 45 (31) | 47 (42) | 66 (58) | 25 (62.5) ** | 88 (41) |
| RF F (%) | ||||||||||
| <20 IU/mL | 46 (35) | 84 (65) | 21 (16) | 109 (84) | 63 (48) | 67 (52) | 39 (30) | 91 (70) | 14 (35) | 116 (54) |
| 20–59 IU/mL | 28 (68) | 13 (32) | 16 (39) | 25 (61) | 26 (53) | 15 (37) | 15 (37) | 26 (63) | 10 (25) | 31 (15) |
| >59 IU/mL | 52 (63) ** | 31 (37) | 23 (28) | 60 (72) | 48 (58) | 36 (42) | 34 (41) | 49 (59) | 16 (40) | 67 (31) |
| B. Periodontal markers | ||||||||||
| Gingival Index | ||||||||||
| Median | 47 | 35 | 46 | 36 | 38 | 37 | 37 | 38 | 35 | 38 |
| IQR | (13–68) | (18–63) | (8–65) | (18–64) | (14–66) | (15–66) | (14–64) | (15–64) | (6–64) | (17–65) |
| BoP | ||||||||||
| Median | 47 ** | 40 | 52 | 40 | 43 | 41 | 44 | 41 | 41 | 47 |
| IQR | (27–64) | (23–55) | (23–67) | (26–56) | (22–60) | (27–59) | (21–59) | (26–59) | (26–58) | (20–63) |
| Pocket depth | ||||||||||
| Median | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 |
| IQR | (0–4.2) | (0–4.19) | (0–4.0) | (0–4.16) | (0–4.25) | (0–4.17) | (1–4.38) | (0–2.5) | (0–4.14) | (0–4.0) |
| CAL | ||||||||||
| Median | 2.75 ** | 2.48 | 2.79 ** | 2.52 | 2.7 | 2.6 | 2.6 | 2.7 | 2.6 | 2.8 |
| IQR | (2.3–3.3) | (2–2.9) | (2.1–3.6) | (2–3) | (2.1–3.2) | (2.1–3.2) | (2.1–3.2) | (2.2–3.2) | (2.1–3.1) | (2.3–3.4) |
| Reference | OR Unadjusted | (CI 95%) | OR Adjusted | (CI 95%) | |
|---|---|---|---|---|---|
| Model 1 Dependent Variable | |||||
| RA | Without RA | ||||
| Independent variable | |||||
| ACPAs < 20 U | Reference | 1.0 | 1.0 | ||
| ACPAs > 20 U | 13.7 | 5.1–36.2 ** | 15.21 | 5.2–44.5 ** | |
| RF < 20 UI/mL | Reference | 1.0 | 1.0 | ||
| RF > 20 UI/mL | 10.6 | 4.10–23 ** | 15.58 | 5.0–48.49 ** | |
| Anti-RgpA < Q1 | Reference | 1.0 | 1.0 | ||
| Anti-RgpA > Q1 | 4.09 | 1.20–13.9 * | 8.6 | 1.56–47.8 ** | |
| Model 3 Dependent Variable | |||||
| RA | Without RA | ||||
| Independent variable | |||||
| ACPAs < 20 U | Reference | 1.0 | 1.0 | ||
| ACPAs > 20 U | 13.7 | 5.1–36.2 ** | 14.4 | 5.2–39.9 ** | |
| RF < 20 UI/mL | Reference | 1.0 | 1.0 | ||
| RF > 20 UI/mL | 9.9 | 4.4–25.4 ** | 14.6 | 4.7–45 ** | |
| Anti-RgpA < Q1Anti-PPAD < Q2 | Reference | 1.0 | 1.0 | ||
| Anti-RgpA > Q1Anti-PPAD > Q2 | 6.63 | 1.61–27 * | 9.69 | 1.77–52 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castillo, D.M.; Lafaurie, G.I.; Romero-Sánchez, C.; Delgadillo, N.A.; Castillo, Y.; Bautista-Molano, W.; Pacheco-Tena, C.; Bello-Gualtero, J.M.; Chalem-Choueka, P.; Castellanos, J.E. The Interaction Effect of Anti-RgpA and Anti-PPAD Antibody Titers: An Indicator for Rheumatoid Arthritis Diagnosis. J. Clin. Med. 2023, 12, 3027. https://doi.org/10.3390/jcm12083027
Castillo DM, Lafaurie GI, Romero-Sánchez C, Delgadillo NA, Castillo Y, Bautista-Molano W, Pacheco-Tena C, Bello-Gualtero JM, Chalem-Choueka P, Castellanos JE. The Interaction Effect of Anti-RgpA and Anti-PPAD Antibody Titers: An Indicator for Rheumatoid Arthritis Diagnosis. Journal of Clinical Medicine. 2023; 12(8):3027. https://doi.org/10.3390/jcm12083027
Chicago/Turabian StyleCastillo, Diana Marcela, Gloria Inés Lafaurie, Consuelo Romero-Sánchez, Nathaly Andrea Delgadillo, Yormaris Castillo, Wilson Bautista-Molano, César Pacheco-Tena, Juan Manuel Bello-Gualtero, Philippe Chalem-Choueka, and Jaime E. Castellanos. 2023. "The Interaction Effect of Anti-RgpA and Anti-PPAD Antibody Titers: An Indicator for Rheumatoid Arthritis Diagnosis" Journal of Clinical Medicine 12, no. 8: 3027. https://doi.org/10.3390/jcm12083027